
Abstract
Traditional cardiovascular risk factors have been in the spotlight for coronary artery disease (CAD) management over the past decades. A non-modifiable risk marker is short adult stature. However, a causal role in the etiology of CAD was always questioned, since multiple confounders may also explain the inverse association between height and CAD risk. The assumption that genetic variants affecting height do so without interference of exogenous factors allows for the testing of the association between short stature, that is, genetic markers affecting height, and CAD even without measuring height. Interestingly, these studies suggest a rather multifaceted relationship between the two complex phenotypes. Indeed, investigating 180 height-associated genetic variants in 65,066 patients with CAD and 128,383 healthy controls suggests a causal relationship of short stature and CAD risk. Multiple signaling pathways affecting growth, as well as pleiotropic effects of genetic variants affecting height and lipids, seem to underlie the association between height and CAD risk.
Coronary artery disease (CAD) represents the leading cause of death in industrial nations. Several risk factors, for example, smoking, arterial hypertension, diabetes mellitus Citation[1], and hypercholesterolemia, as well as a positive family history Citation[2] are known to increase its susceptibility Citation[3,4]. Some environmental risk factors can be influenced either by lifestyle or pharmacological interventions, and are thereby often synonymized as modifiable risk factors. On the other hand, the association of a positive family history remained enigmatic until the advent of genome-wide association studies investigating large populations of CAD cases and controls. Those led to the discovery of > 45 common genetic variants genome-wide significantly associated with CAD and myocardial infarction risk Citation[5,6]. Interestingly, only a small portion of the association mediated by these variants was explainable by known risk factors such as arterial hypertension, for example GUCY1A3, or hypercholesterolemia, for example PCSK9, LDLR, or LPA (for a review see Citation[7]). From one point of view, this was the starting point for the identification of novel pathways and mechanisms leading to atherosclerosis. On the other hand, the discovery of genetic variants, for example those associated with hypercholesterolemia, proved the already known pathophysiological context between the risk factor and CAD by genetic means and offered further rationale for respective pharmacological treatment. Matter of fact, new genetic findings from genome-wide association studies can be a starting point for validation or refusal of pathophysiological or epidemiological associations.
An inverse association of height and risk of CAD has been assumed for > 6 decades. As early as 1951, epidemiologic observations rendered this association likely Citation[8]. Human height is known to be heritable Citation[9–11]. In addition, environmental factors such as the socioeconomic background and childhood nutrition influence adult stature Citation[12]. Until now, almost 2000 publications addressed the correlation between human stature and the occurrence of cardiovascular diseases. Taken together, the findings of these in most of the cases observational studies resulted in a burning question: is the link between shorter height and higher risk of CAD causal? Paajanen et al. Citation[13] targeted this topic in a large meta-analysis showing that shorter height is indeed associated with an increased risk of CAD. This systematic review concluded that individuals smaller than 160.5 cm have an almost 1.5 times higher risk of CAD morbidity and mortality compared to those larger than 173.9 cm. A relevant limitation of this study was the comparison of categories, the ‘shortest group’ versus the ‘tallest group’ and – like with most other studies – the inability to exclude confounders.
Mendelian randomization study of height & coronary disease
An option for testing whether there is true association between a trait and a disease is by the Mendelian randomization approach Citation[14]. Human height is a complex and highly polygenic trait with > 180 already known loci influencing its phenotypic variation Citation[15]. These variants have been further studied for association with CAD in a large-scale analysis by Nelson et al. Citation[16], which was published in the New England Journal of Medicine this spring. In this study, 65,066 CAD patients and 128,383 healthy controls were analyzed. The lead SNPs of the 180 loci associated with height identified by Lango Allen et al. were analyzed in the genome-wide association studies of CAD conducted by the CARDIoGRAM Citation[5] and CARDIoGRAMplusC4D consortia Citation[6] regarding their association with CAD. Interestingly, several height-associated SNPs were significantly associated with CAD and 1 SD-decrease (∼6.5 cm) in height led to a 13.5% increase in relative risk of suffering from CAD. In a subgroup analysis investigating only male individuals, the association of height-associated SNPs with CAD was still significant, whereas this was not true in women. In persons with available individual level genetic data, a risk score including the height-associated lead SNPs revealed a 26% decrease in CAD risk of the quartile with the highest number of height-raising lead SNPs compared to the quartile with the lowest number of height-raising SNPs. In an analysis investigating the same SNPs for effects on traditional risk factors, for example hypercholesterolemia, it appeared that approximately 19% of the observed association between height-associated SNPs and CAD was due to association of short stature with these traditional risk factors Citation[16].
Overall, the investigated 180 loci only explain ∼10% of the variation in stature Citation[15]. It is also important to mention that none of the 180 analyzed loci had been previously linked to CAD. However, the major advantage of this genetic approach was the exclusion of social status, smoking, and nutrition, that is, exogenous confounders, which allowed identifying a primary relationship between short stature and risk of CAD.
Pathophysiological explanation attempts
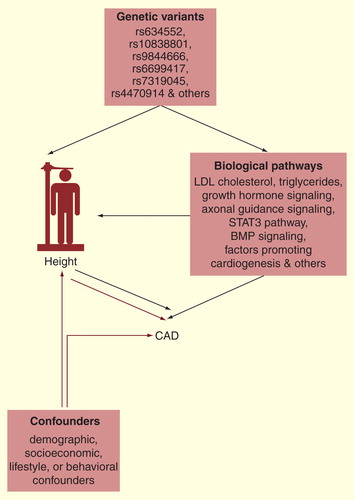
Breaking the previously mentioned findings down to a pathophysiological level, several hypotheses may be considered. One simple theory presumes shorter people to suffer from coronary stenosis at younger age due to a smaller vessel diameter. However, if so, women should be at higher risk regarding their overall shorter height and their smaller size of coronary arteries Citation[17], which is not the case as women develop CAD later in life than men Citation[18,19]. Regarding traditional cardiovascular risk factors, an association was detected for some height SNPs with LDL-cholesterol and triglycerides, rendering a disadvantage lipid profile as potential intermediate phenotype between height and CAD likely. However, this has only partially influenced the association of height and CAD in the genetic analysis Citation[16]. Other functional links between height SNPs and CAD risk may involve pathways modulated by respective SNPs that already had revealed a link to CAD risk in functional studies . Bearing in mind that none of the height-associated variants was significantly associated with CAD in the first place, it becomes obvious that the sum of small effects on height may be the most important link explaining the association with CAD risk. A potential mechanism that immediately links a shorter stature and coronary physiology relates to pulse valve reflection and a more pronounced augmentation of coronary pressure. It can be hypothesized that at a given velocity of the forward traveling pulse wave (and its reflection) the time until it reappears in the ascending aorta is shorter in a shorter person. This may augment coronary pressure in late systole with resulting coronary hypertension and atherosclerosis at an earlier point in time. However, the pathophysiological implications of this analysis might be too complicated to be fully understood just from the current state of scientific knowledge. A possible explanation could be the concept of shared pathways leading to larger height as well as increased risk of CAD; however, it is also possible that larger height influences lifestyle thereby modifying CAD risk Citation[16].
Figure 1. Complexity of short stature and increased risk of coronary artery disease. Modified from NEJM, Nelson et al., Genetically Determined Height and Coronary Artery Disease, 372(17):1608-18 Copyright © (2015) Massachusetts Medical Society. Reprinted with permission.
Future prospects
A major advantage of genetic analyses in large populations besides looking at traditional risk factors is the identification of novel biological mechanisms and signaling cascades, which may contribute to disease development and progression. Detailed pathway analyses uncovered the association of height with growth factors like BMP and TGF-β, which are known to influence vascular function and cardiac development Citation[16]. Future studies will help to understand those correlations more deeply and hopefully identify new targets for prevention and therapy. Additionally, future studies will help to clarify the predictive power of including height as a factor in risk-assessment strategies.
Nevertheless, as the socioeconomic level including healthcare and living standards hopefully continues to rise in western countries, it becomes more difficult to identify environmental risk factors influencing adult height. Among Europeans, nutrition with ‘high-quality’ proteins, for example fish and milk, versus ‘lower-quality’ proteins like wheat has been identified as the main external factor influencing adult stature Citation[20]. Further surveys on lifestyle including daily sugar or fat intake as well as overweight in young adults are desired to identify the ultimate recipe for growth.
Until then, those already dusting off the torture rack should keep in mind that taller individuals face an increased risk compared to shorter people for other cardiovascular diseases, for example, pulmonary embolism and aortic rupture Citation[21].
Conclusion
The association between genetically assigned adult height and risk for CAD illustrates the complexity of genetic predisposition in CAD. Risk prediction models could help to identify individuals at high risk but we need to keep in mind that adult stature only accounts for a small portion of CAD risk. Therefore, taller people do not get a free ride for an unhealthy lifestyle.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
- Ross S, Gerstein HC, Eikelboom J, et al. Mendelian randomization analysis supports the causal role of dysglycaemia and diabetes in the risk of coronary artery disease. Eur Heart J 2015;36(23):1454-62
- Otaki Y, Gransar H, Berman DS, et al. Impact of family history of coronary artery disease in young individuals (from the CONFIRM registry). Am J Cardiol 2013;111(8):1081-6
- Wilson PW, D’Agostino RB, Levy D, et al. Prediction of coronary heart disease using risk factor categories. Circulation 1998;97(18):1837-47
- Myers RH, Kiely DK, Cupples LA, Kannel WB. Parental history is an independent risk factor for coronary artery disease: the Framingham Study. Am Heart J 1990;120(4):963-9
- Schunkert H, Konig IR, Kathiresan S, et al. Large-scale association analysis identifies 13 new susceptibility loci for coronary artery disease. Nat Genet 2011;43(4):333-8
- Consortium CAD, Deloukas P, Kanoni S, et al. Large-scale association analysis identifies new risk loci for coronary artery disease. Nat Genet 2013;45(1):25-33
- Kessler T, Erdmann J, Schunkert H. Genetics of coronary artery disease and myocardial infarction–2013. Curr Cardiol Rep 2013;15(6):368
- Gertler MM, Garn SM, White PD. Young candidates for coronary heart disease. J Am Med Assoc 1951;147(7):621-5
- Silventoinen K, Sammalisto S, Perola M, et al. Heritability of adult body height: a comparative study of twin cohorts in eight countries. Twin Res 2003;6(5):399-408
- Visscher PM, Medland SE, Ferreira MAR, et al. Assumption-free estimation of heritability from genome-wide identity-by-descent sharing between full siblings. PLoS Genet 2006;2(3):e41
- Yang J, Benyamin B, McEvoy BP, et al. Common SNPs explain a large proportion of the heritability for human height. Nat Genet 2010;42(7):565-9
- Silventoinen K. Determinants of variation in adult body height. J Biosoc Sci 2003;35(2):263-85
- Paajanen TA, Oksala NK, Kuukasjarvi P, Karhunen PJ. Short stature is associated with coronary heart disease: a systematic review of the literature and a meta-analysis. Eur Heart J 2010;31(14):1802-9
- Jansen H, Samani NJ, Schunkert H. Mendelian randomization studies in coronary artery disease. Eur Heart J 2014;35(29):1917-24
- Lango Allen H, Estrada K, Lettre G, et al. Hundreds of variants clustered in genomic loci and biological pathways affect human height. Nature 2010;467(7317):832-8
- Nelson CP, Hamby SE, Saleheen D, et al. Genetically determined height and coronary artery disease. N Engl J Med 2015;372(17):1608-18
- Dickerson JA, Nagaraja HN, Raman SV. Gender-related differences in coronary artery dimensions: a volumetric analysis. Clin Cardiol 2010;33(2):E44-9
- Hochman JS, Tamis JE, Thompson TD, et al. Sex, clinical presentation, and outcome in patients with acute coronary syndromes. Global Use of Strategies to Open Occluded Coronary Arteries in Acute Coronary Syndromes IIb Investigators. N Engl J Med 1999;341(4):226-32
- Leening MJG, Ferket BS, Steyerberg EW, et al. Sex differences in lifetime risk and first manifestation of cardiovascular disease: prospective population based cohort study. Bmj 2014;349:g5992
- Grasgruber P, Cacek J, Kalina T, Sebera M. The role of nutrition and genetics as key determinants of the positive height trend. Econ Hum Biol 2014;15:81-100
- Emerging Risk Factors C. Adult height and the risk of cause-specific death and vascular morbidity in 1 million people: individual participant meta-analysis. Int J Epidemiol 2012;41(5):1419-33