

Abstract
Fecal occult blood (FOB) is a sign of gastrointestinal diseases, such as intestinal ulcers and colorectal cancer. In experimental animal studies, there is no standard method to detect FOB. Here, we present a simple protocol to detect FOB in mice, using the Luminol Reaction Experiment Kit® that was originally designed to detect bloodstains at a crime scene in criminal forensics. To obtain positive control bloody feces, we used an indomethacin-induced intestinal ulcer model in mice. By mixing small pieces of feces with a luminol solution, the fecal solution emitted visible blue–white chemiluminescence in dark field when feces contained hemoglobin. We also established a method for semi-quantification of hemoglobin content in the fecal solution, using a luminometer. This method is simple, quick, economical and semi-quantitative, allowing researchers to detect FOB in experimental mice.
By mixing bloody feces with a luminol solution, the solution emits chemiluminescence. The chemiluminescence is not only seen by the naked eye in dark field but is also measurable by a luminometer for semi-quantification.
Fecal occult blood (FOB) is a sign of gastrointestinal diseases, including ulcers [Citation1] and colorectal cancer [Citation2–4]. Clinically, there are two standard methods to detect FOB: the stool guaiac test is based on the oxidation of guaiac by hydrogen peroxide (H2O2), which is catalyzed by the peroxidase-like activity of hemoglobin (Hb) [Citation5]; while the immunochemical test using anti-human Hb antibodies is more specific and expensive than the guaiac test [Citation2]. For experimental animal studies, however, there is no standard method to detect FOB. Here, we have established a simple method to detect FOB in experimental mice, using the Luminol Reaction Experiment Kit® (Wako Pure Chemical, Osaka, Japan), which has been used in criminal forensics to detect blood at a crime scene. The luminol test is based on the oxidation of the substrate by the peroxidase-like activity of Hb, where the luminol reagents emit visible blue–white chemiluminescence in dark field.
As a positive control, we used a nonsteroidal anti-inflammatory drug-induced intestinal ulcer model in mice [Citation6], where FOB is detectable 4 h after intra-gastric indomethacin administration. The animal experiments were approved by the Institutional Animal Care and Use Committee of Kindai University and performed in accordance with the institutional guidelines. We harvested feces from CD1 mice (Charles River Laboratories Japan, Yokohama, Japan) at different time points following indomethacin administration (6 mg/kg body weight). The luminol solution was prepared by mixing two reagents (luminol and sodium peroxide) in deionized-distilled water (ddH2O), according to the manufacturer’s instruction. Because of the high sensitivity of the luminol solution, we used a dilute solution (fivefold with ddH2O) as a ‘working solution’ for visual detection.
Following addition of the working solution to FOB-positive feces, luminol generated blue–white luminescence (, Supplementary video 1). We also conducted a time-course analysis of FOB following indomethacin administration (). We placed a portion of feces (<1 mg) in a 96-well plate (Thermo Fisher Scientific, MA, USA) at different time points and added 100 μl of the working solution into each well. Blue–white chemiluminescence became detectable at 4 h after the indomethacin administration and luminescence intensity increased thereafter.
(A & B) We induced intestinal ulcer in mice injected with indomethacin, and harvested feces. (A) Feces in a microtube at 0 (con) and 6 h (indo) and (B) a portion of feces in a 96-well plate at different time points (0, 2, 3, 4, 5, 6 and 8 h) following the indomethacin injection. Fecal samples were mixed with a luminol solution and observed in dark field. The blue–white chemiluminescence became detectable at 4 h after the injection: -: negative; ±: dim; +: moderate; and ++: bright. (C) Different amounts of fecal samples from A were placed into a 96-well plate and mixed with 100 μl of a dilute luminol solution. Chemiluminescence intensities were measured by a microplate reader. We calculated the ratios of the chemiluminescence intensities of wells containing different amounts of feces to the chemiluminescence intensity of wells containing a luminol solution alone. Weights of feces containing occult blood positively correlated with the chemiluminescence ratios (r2 = 1.00). (D) We placed 5 μg of fecal samples from B, mixed with the luminol solution, and calculated the chemiluminescence ratios to the chemiluminescence intensity of wells containing feces from untreated mouse (time: 0 h). (E) We placed different amounts of hemoglobin (Hb) in 96-well plates in the absence (‘Hb alone’, open red circles) or the presence (‘Hb + feces’, closed purple circles) of 5 μg of control feces, followed by addition of the luminol solution. The chemiluminescence intensity of the luminol solution alone or with 5 μg of feces was used for the chemiluminescence ratios of ‘Hb alone’ or ‘Hb + feces’, respectively. Both Hb concentrations of ‘Hb alone’ or ‘Hb + feces’ samples positively correlated with the chemiluminescence ratios, although the ratios of the latter samples showed lower chemiluminescence ratios. (F) We placed different amounts of feces from normal mice (1–16 μg/well) into wells containing 50 ng of Hb, followed by addition of the luminol solution. We calculated the chemiluminescence ratios to the chemiluminescence intensity of wells containing 50 ng of Hb without feces. (A–F) We repeated each experiment at least three times.
Con: Control; Hb: Hemoglobin; Indo: Indomethacin.
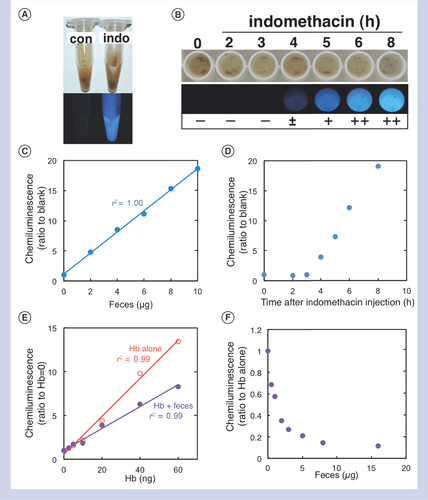
To apply the luminol reaction for estimation of Hb concentrations in feces, we determined the range of fecal sample weights applicable for the luminol reaction. We prepared a FOB-positive fecal solution (1 mg/ml) with ddH2O, centrifuged it at 8000 × g for 2 min, and the supernatant was used for assay. We placed 1–10 μl of the solution in 96-well plates, added 100 μl of the 500-fold dilute luminol solution, and measured its chemiluminescence signals using a microplate reader (ARVO; Perkin Elmer, MA, USA). In the range of 1 to 10 μg feces/reaction, we obtained excellent linearity between chemiluminescence signals and fecal amounts (), while fecal amounts higher than 40 μg decreased chemiluminescence signals (data not shown). Although the absolute chemiluminescence signal of the luminol solution differed in each assay, the ratio to the background chemiluminescence signal was stable (data not shown). Thus, we can obtain reproducible results by using the ratio to the background chemiluminescence (blank wells containing the luminol solution alone).
To determine whether the chemiluminescence signals could reflect the results of the above visual detection method, we used the same samples of and detected FOB by the chemiluminescence signals. We prepared fecal sample solutions (1 mg/ml) at different time points, placed 5 μg of feces in 96-well plates, and measured their chemiluminescence signals. The signals became detectable 4 h after indomethacin administration and increased thereafter (). Thus, the chemiluminescence results were similar to the results observed by the visual detection.
Next, we quantified the Hb concentrations in feces, using Hb standard solutions derived from normal murine blood (Hb concentration was determined by Hematology Analyzer XT-1800; Sysmex Corporation, Hyogo, Japan). In the range of 1–60 ng/well, Hb concentration curves showed excellent linearity with chemiluminescence ratios (); the detection limit was 1 ng Hb/well, while Hb concentrations higher than 60 ng/well reached a plateau (data not shown).
Since feces themselves have been shown to affect the chemiluminescence [Citation7], we measured the chemiluminescence signals of wells containing 50 ng of Hb in the presence of different amounts of feces from normal mice (0–16 μg of feces/well). The addition of feces decreased the signals; in the presence of 5 μg of feces, the signal decreased to 20% of that of a control well containing 50 ng of Hb alone (). The signals in the presence of 5 μg of feces/well provided the most reproducible results among different fecal amounts tested.
Lastly, we attempted to estimate the Hb concentrations in feces. We calculated the chemiluminescence ratios of wells containing different amounts of Hb in the presence of 5 μg of feces from control mice (). Although the presence of feces decreased the ratios (and signals, data not shown) compared with those of wells containing no feces (‘Hb alone’), their Hb concentrations curves showed excellent linearity with chemiluminescence ratios (r2 = 0.99).
We have established two simple protocols to detect FOB by visual observation or chemiluminescence measurement (). We propose a scoring system for FOB, which can be used in either protocol. For practical use, there are three tips for obtaining reproducible results as follows: first, the absolute value of chemiluminescence of the luminol solution can differ in each experiment; one needs to either set up wells containing 5 μg of a control fecal sample from normal mice to calculate the chemiluminescence ratios, or freeze and store all fecal samples so that all samples can be analyzed simultaneously in a single experiment. Second, the chemiluminescence decreases rapidly once the luminol reaction is initiated (Supplementary video 2); the chemiluminescence needs to be measured immediately following addition of the luminol solution. Third, several compounds affect the luminol reaction [Citation8]. In our study, contamination with low levels of phosphate-buffered saline (PBS) and murine urine decreased the luminol reaction, while contamination with bleach (sodium hypochlorite, Wako Pure Chemical) and H2O2 increased the reaction: 50% and 99% decreases by 1 μl of PBS and normal urine/100 μl reaction, respectively; sixfold and fourfold increases by 1 μl of 100-times diluted sodium hypochlorite and 1 μl of 3% H2O2 solution/100 μl reaction, respectively. In summary, our FOB detection method is simple, quick, economical and semi-quantitative, allowing researchers to detect FOB in experimental mice. It would be interesting to compare this method to other methods, such as the guaiac test and the immunochemical test in the future.
Visual detection (A) and chemiluminescence measurement (B). (A) Visual detection: (1) Add a luminol dilute solution (dilute the original solution fivefold with deionized-distilled water [ddH2O]) to pooled feces in a microtube (left) or a piece of feces taken by a toothpick in a white 96-well plate (right); and (2) observe them in dark field. In the presence of blood, blue–white chemiluminescence is visible. (B) Chemiluminescence measurement: (1) Prepare fecal solutions with ddH2O (1 mg/ml) in a microtube; (2) vortex and centrifuge the tube for 2 min; (3) transfer 5 μl of the solution (containing 5 μg of feces) in a 96-well plate; (4) add 100 μl of a luminol dilute solution (diluted 500-fold with ddH2O) to each well; and (5) measure the chemiluminescence signal by a luminometer immediately. (C) Fecal blood scores based on the two luminol protocols. To calculate the chemiluminescence ratios, it is recommended to store the control fecal solution (1 mg/ml) derived from normal mice. Hb concentrations have been estimated by comparing with the results of feces mixed with standard Hb solutions.
ddH20: Deionized-distilled water; Hb: Hemoglobin.
![Figure 2. Schematic illustration of two protocols for detecting fecal occult blood by the luminol reaction.Visual detection (A) and chemiluminescence measurement (B). (A) Visual detection: (1) Add a luminol dilute solution (dilute the original solution fivefold with deionized-distilled water [ddH2O]) to pooled feces in a microtube (left) or a piece of feces taken by a toothpick in a white 96-well plate (right); and (2) observe them in dark field. In the presence of blood, blue–white chemiluminescence is visible. (B) Chemiluminescence measurement: (1) Prepare fecal solutions with ddH2O (1 mg/ml) in a microtube; (2) vortex and centrifuge the tube for 2 min; (3) transfer 5 μl of the solution (containing 5 μg of feces) in a 96-well plate; (4) add 100 μl of a luminol dilute solution (diluted 500-fold with ddH2O) to each well; and (5) measure the chemiluminescence signal by a luminometer immediately. (C) Fecal blood scores based on the two luminol protocols. To calculate the chemiluminescence ratios, it is recommended to store the control fecal solution (1 mg/ml) derived from normal mice. Hb concentrations have been estimated by comparing with the results of feces mixed with standard Hb solutions.ddH20: Deionized-distilled water; Hb: Hemoglobin.](/cms/asset/4e632788-c26f-4ea0-81b3-b81dc152ec23/ibtn_a_12360545_f0002.jpg)
Author contributions
Study concept and design: A-MP and IT; experiments: A-MP; drafting the manuscript: A-MP and IT; obtaining fundings: A-MP and IT.
BioTechniQues
Download MS Word (47.6 KB)Additional file 1
Download QuickTime Video (1.2 MB)Additional file 1
Download QuickTime Video (10.2 MB)Acknowledgments
We thank Mitsugu Fujita, Fumitaka Sato and Seiichi Omura for valuable discussion, and Namie Sakiyama for excellent technical assistance.
Financial competing interests disclosure
This work was supported by grants from the National Institute of General Medical Sciences COBRE Grant (P30-GM110703, I Tsunoda), the Japan Society for the Promotion of Science (JSPS, Grant-in-Aid for Scientific Research [B]-MEXT KAKENHI Grant #15K08975 [A-M Park], Grants-in-Aid for Scientific Research-KAKENHI, 16H07356 [I Tsunoda]) and Novartis Pharma Research Grants 2017 (A-M Park, I Tsunoda). This paper is subject to the NIH Public Access Policy. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.tandfonline.com/doi/suppl/10.2144/btn-2018-0017
Additional information
Funding
References
- Kobayashi Y , WatabeH, YamadaAet al. Impact of fecal occult blood on obscure gastrointestinal bleeding: observational study. World J. Gastroenterol.21(1), 326–332 (2015).
- Federici A , Giorgi RossiP, BorgiaP, BartolozziF, FarchiS, GausticchiG. The immunochemical faecal occult blood test leads to higher compliance than the guaiac for colorectal cancer screening programmes: a cluster randomized controlled trial. J. Med. Screen.12(2), 83–88 (2005).
- Levin B , LiebermanDA, McFarlandBet al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology134(5), 1570–1595 (2008).
- Hewitson P , GlasziouP, IrwigL, TowlerB, WatsonE. Screening for colorectal cancer using the faecal occult blood test, Hemoccult. Cochrane Database Syst. Rev. (1), CD001216 (2007).
- Rozen P , LeviZ, HazaziRet al. Quantitative colonoscopic evaluation of relative efficiencies of an immunochemical faecal occult blood test and a sensitive guaiac test for detecting significant colorectal neoplasms. Aliment. Pharmacol. Ther.29(4), 450–457 (2009).
- Stadnicki A , ColmanRW. Experimental models of inflammatory bowel disease. Arch. Immunol. Ther. Exp. (Warsz).51(3), 149–155 (2003).
- Weber K , MikulovicV. The luminescence of luminol XI (Yugoslavia). Arhiv. Higijenu rada, Zagreb. (English translated version is available from US Department of the Army, #AD839542) (1959).
- Marquette CA , BlumLJ. Applications of the luminol chemiluminescent reaction in analytical chemistry. Anal. Bioanal. Chem.385(3), 546–554 (2006).

