
Abstract
Background and aims
There is an urgent need to address the role of healthy diet and behaviors promoting health among school adolescents in order to tailor appropriate interventions in Jordanian schools. This study aims to evaluate the reliability and validity of the Arabic version of Students As LifeStyle Activists (SALSA) survey alongside Jordanian adolescents’ attitudes and perceived barriers to healthy eating and physical activity.
Methods
This study uses baseline data from a randomized controlled trial recruiting school students from 29 male and 27 female public high schools that have grades 7 and 8. Cronbach’s alpha and principal components analysis/factor analysis were used to check reliability and validity. Numbers, percentages, and chi square were used to explore healthy diet and physical activities preferences among Jordanian school students and determine gender differences for all evaluated items.
Results
The Arabic version-SALSA survey has acceptable Cronbach’s alpha values (>0.78) for most of its scales. Five scales were derived from the Arabic version-SALSA survey using principal components analysis/factor analysis (factors loading above 0.3). A higher proportion of female students agreed that “healthy food makes you more comfortable” compared to male students (44% vs 36%, P<0.05). Few Jordanian high school students held positive attitudes toward healthy food. This study identified both social and personal barriers to exercise among Jordanian adolescents, including lack of skills for physical activity, easy access and low cost of fast food, scarce opportunities for physical activity, and lack of peers and friends.
Conclusion
Interventions should be tailored to health attitudes and beliefs of Jordanian school students in parallel with improving physical resources and enhancing peer and/or friend support.
Background
NCDs such as cardiovascular diseases are increasingly responsible for the burden of disease in developing countries,Citation1 resulting in a “double burden” of both communicable and NCDs for these countries.Citation1,Citation2 This double burden is especially salient for countries in the WHO Eastern Mediterranean Region,Citation1 including many Arab countries such as Jordan and Egypt. In Jordan, for instance, NCDs are now the leading cause of death, obesity, and diabetes, in which all of them are significant public health problems.Citation3 Analyses of the global disease burden demonstrate that risk factors, such as high blood pressure, physical inactivity, and overweight and obesity, play an increasingly important role in the disease burden in Northern Africa and the Middle East.Citation4 Critically, the NCD burden can be reduced or prevented if certain approaches are adopted.Citation5 Thus, there is a growing interest in interventions to address these issues, and schools are a recognized venue for health promotion.Citation6
School-based health-promoting interventions are increasingly widespread, and have been shown to have beneficial effects, especially on the amount of physical activity during and outside school.Citation7 Such interventions are important for school-aged children, including adolescents, because behaviors and attitudes developed during this time can continue in later life. Previous studies of Arab adolescent lifestyle practices demonstrated that many adolescents have high-calorie/fatty diets and very low levels of physical activity.Citation8–Citation11 A region-wide study found that few adolescents consumed fruits and vegetables as frequently as guidelines recommended.Citation12 Additionally, several barriers to adopting healthy eating and adequate physical activity behaviors by Arab adolescents, including Jordanians,Citation10,Citation11,Citation13 were identified. These barriers include expenses, facilities, accessibility, safety, education, and knowledge. Therefore, programs targeting these barriers to modify healthy lifestyle among this population are urgently needed.
A first step in developing successful interventions to empower adolescents to adopt healthier lifestyles is determining the relevant barriers to these lifestyles, as well as tailor interventions appropriately. While information on the association across different lifestyle behaviors is available for Saudi ArabiaCitation14,Citation15 and Kuwait,Citation16,Citation17 it is scarce in Jordan despite the urgent need. Therefore, the aims of this study are to 1) evaluate the reliability and validity of an Arabic questionnaire evaluating healthy lifestyle behaviors; and 2) assess Jordanian adolescents’ attitudes and perceived barriers to healthy eating and physical activity.
Methods
Design and participants
This analysis is part of a larger study evaluating a school-based, peer-led healthy lifestyle intervention. This analysis uses the baseline data from a randomized controlled trial of the intervention. A multistage stratified sampling technique was used to ensure equal representation of socioeconomic status (including monthly income and level of education) – by school district – and both sexes. After stratification for school district and gender, a total of 6 male and 6 female schools (all Jordanian schools are split by sex) were randomly selected using opaque, sealed envelopes from 29 male and 27 female public high schools that have grades 7 and 8 (56 is the entire number of public high schools that met the inclusion criteria in the 3 districts), in Northern Jordan. Within selected schools, the entire seventh and eighth grade classes were invited to participate. Students were eligible to participate if they were physically and cognitively capable of completing the self-reporting survey and were free of major diseases that could affect their responses such as diabetes, hypertension, and cardiovascular diseases.Citation18,Citation19
Ethical considerations
Approval for the study was obtained from the Human Research Ethics Committees at the Ministry of Education, relevant educational school districts, and Jordan University of Science and Technology in Jordan. The students and parents were provided with detailed information about the study. Subsequently, written informed consent and assent were voluntarily obtained from eligible parents and students, respectively, prior to participation. The study was carried out in accordance with the principles of the Declaration of Helsinki.
Instruments
The SALSA surveyCitation20 was used to determine adolescents’ attitudes, practices, and perceived barriers toward healthy eating and physical activity. The SALSA survey is part of a peer-led educational program originally developed in Sydney, Australia.Citation20 Before implementing the survey in Jordan, it was translated into Arabic and back translated again into English by a professional translator but has not been validated in Arabic-speaking populations or in Australia. The survey, a classroom activity, is self-administered by students in 15 minutes and facilitated by two research assistants and a volunteer school teacher. For the purposes of the current study, students from the 12 schools completed a total of 66 items. The item responses were “yes”/“no”; and 4-to-5 point Likert scale answers depending on the question itself.
Statistical analyses
Reliability
Cronbach’s alpha was used to assess reliability. Coefficients above 0.8 were interpreted as indicative of high reliability.Citation21 The five scales were determined based on the relevance of the items to each other and the experts’ opinions.
Validity
As we did not have prior hypotheses about the dimensionality of the Arabic version of SALSA, we used PCA to identify and extract factors in the data. We then rotated the factors using Varimax rotation with Kaiser Normalization. We used 0.30 as a cutoff value for factor loading. All analyses, including PCA and Cronbach’s alpha, were performed using SPSS v21.0 (SPSS Inc., Chicago, IL, USA) and SAS software (v 9.4, Cary, NC, USA). Data are presented as numbers and percentages. The chi-squared test was used to determine gender differences for all evaluated items. P-values of <0.05 were considered statistically significant.
Results
As illustrated in , a total of 791 students participated in the study from 12 public high schools. Participants were mostly female (N=475, 60%), and aged between 13 and 15 years (60% were 14 years of age).
Table 1 Participants’ demographical characteristics (N=791)
Results of the reliability analysis
All scales got desirable values of Cronbach’s alpha, above 0.7, except two scales. Those two scales obtaining low Cronbach’s alpha values are eating behaviors (0.05) and food preferences (0.30) ().
Table 2 The reliability coefficients for each of the five scales of Arabic version of Students As LifeStyle Activists
Results of validity analysis
We divided the SALSA survey into smaller scales based on their related questions resulting in five scales. Then, we addressed each scale alone, showing how many factors each scale has.
Eating behaviors scale
This scale has nine items prior to PCA. As illustrated in , two items do not load above 0.3 on this scale, so we removed the following two items: How many times you eat useless meals per week? How many cups of water do you drink usually (one cup =052 mL)? Then, we iterated the analysis until we got two factors. The first factor has four items (How many times you eat breakfast per week? How many times you eat junk food during watching TV? How many cups of carbonated beverages do you usually drink? How many times per week do you eat fast food, such as McDonalds, Hungry Jacks, Pizza Hut, Chinese, or Asian takeaway?). The second factor has three items (How much share of the fruits do you eat per week? How much share of the vegetables do you eat per week? How many cups of fruit juice do you drink a day: one cup =052 mL?).
Table 3 Factor analysis of the eating behaviors scale
Food preferences scale
This scale has nine items prior to PCA. The item of “I rarely eat vegetables and fruits at home?” does not load above 0.3, so we removed it, resulting in two factors. As illustrated in , the first factor has four items (I avoid eating fries and chips? Do you have opinion about the food, which is bought to the house? Do you choose what you eat at home? Do you have opinion about the meals that are bought to the house?). The second factor has four items (Do you use fast food and carbonated beverages equally? I cannot eat fruits and vegetables due to their high cost? Do you choose what you eat for lunch? Do you bring some fruits and vegetables to school?).
Table 4 Factor analysis of the food preferences scale
Thoughts of eating scale
This scale has 12 items prior to PCA. The item of “Do you think that healthy food help you to build muscle?” does not load above 0.3, so we removed it. Then, after iterating the analysis, we found the item of “Do you think that healthy food help you to have more energy?” does not load above 0.3, so we removed it as well. Eventually, we got two factors, as illustrated in . The first factor has six items (Do you think that healthy food help you to set a good example for your friends? Do you think that healthy food help you to increase the fame? Do you think that healthy food help you to perform better in sports? Do you think that healthy food help you save money? Do you think that healthy food help you to improve the outward appearance? Do you think that healthy food help you to achieve good scores in school?). The second factor has four items (Do you think that healthy food help you lose weight? Do you think that healthy food help you to concentrate and think better? Do you think that healthy food help you to gain weight? Do you think that healthy food help you feeling better?).
Table 5 Factor analysis of the thoughts of eating scale
Play and exercises scale
This scale has 19 items prior to PCA. The item of “During the week, how many times you play sports of various kinds (such as walking to school or jogging, aerobics, basketball, volleyball, jumping rope, football … etc.)?” does not load above 0.3, so we removed it. Then, we iterated the analysis with four factors as a cutoff for the number of factors. However, we did not reach the simple structure of factor analysis, so we fixed the number of factors into 3. We found that two items do not load above 0.3 (Do you agree that there is a close space I can go to it in order to exercise? And do your parents believe that going to/coming back from school is safe?). Thus, we removed them and iterated the analysis. However, we did not reach the simple structure with three factors, so we iterated the analysis with two factors. We found that two items do not load above 0.3; these are: Do you think that playing sport is difficult if there is no one train with you? And do you think that it is difficult to play sport because you prefer not to sweat or increase your body temperature? Thus, we removed these items and iterated the analysis, to get a two-factor scale, as illustrated in .
Table 6 Factor analysis of the play sport and exercise scale
The first factor has 11 items (Do you think that you are not good at sports, and this makes the sport difficult for you? Do you think that the lack of sufficient power make your training difficult? Do you think that full awareness of your body shape and fitness level makes your sport training difficult? Do you think that having to wear sports clothes makes it difficult for you to play sport? Do you think that you not preferring to play or train makes difficult for you to do regular sport? Do you think that if your parents do not want to play sport with you make it difficult for your practice? Do you think the fact that you do not want to get any injuries makes the sport difficult? Do you think that if others scoff at your performance level it will make your practice difficult? Do you think that not having access to suitable places to play and have fun will make your practice difficult? Do you think that the lack of playgrounds makes your practice difficult? Do you think that your friends not practicing any kind of physical exercise will make your practice difficult?).
The second factor has three items (During the school day, how much time do you spend watching TV before and after school? How do you go to and from school [you can choose more than one answer]? In the school day, how much time do you spend using a computer or Facebook before and after school?).
Encouragement scale
This scale has 17 items prior to PCA, 4 factors were determined immediately as a simple structure. As illustrated in , the first factor has six items (Does your dad encour age you to watch TV and play video games and computers? Do your friends encourage you to play by telling you that you are good at exercise and sports? Does your teacher encourage you to exercise? Does your mother encourage you to exercise? Do your friends ask you to walk or ride a bike with them? Does your teacher encourage you by telling you that you play well and exercise?). The second factor has five items (Do your friends encourage you to play and exercise with you? Does your dad encourage you by telling you that you play well and exercise? Does your mother encourage you to watch TV and play with video games and computers? Does your dad encourage you to exercise? Does your mother encourage you to play and exercises with you?) The third factor has three items (Do your friends encourage you to exercise? Does your dad encourage you to play and exercise with you? Does your mother encourage you by telling you that you play well and exercise?). The same number of items was obtained for the fourth factor (Does your dad ask you to walk or ride a bike with him? Does your teacher encourage you to play and exercises with you? Does your friends encourage you to watch TV and play with video games and computers?).
Table 7 Factor analysis of the encouragement scale
Attitudes regarding healthy food
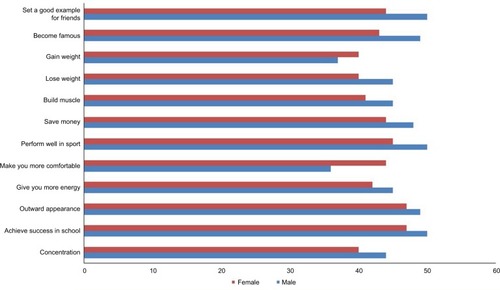
Regardless of gender, most students did not view healthy food in a positive light (). For nearly all items, male students were more likely to endorse positive statements about healthy food than female students, although these differences were not significant (). There was one major exception: a higher proportion of female students agreed that “healthy food makes you feel better”, and this difference was statistically significant (44% vs 36%, P<0.05). Slightly fewer male students (37%) than female students (40%) agreed that healthy food helped you gain weight, but this difference was not statistically significant. The proportion of female students agreeing with the statements about healthy food was <50% for all items. For male students, 50% agreed that healthy food helped them achieve success in school, perform well in sport, and set a good example for friends. However, for the remaining nine items, <50% of male students agreed ().
Figure 1 Attitudes toward healthy food, by sex: % agreeing with statements about healthy food.
Exercise barriers and facilitators
In terms of exercise facilitators, a minority of students agreed that they had access to nearby places to exercise (44%) and that their parents agreed that they had a safe route to school (40%) (). Interestingly, less than half of the students (35%) reported that access to places to play was a problem, and again a minority (39%) of students reported familial barriers. The most frequently endorsed barriers were the lack of someone to train with (62%) and a lack of desire to sweat (61%). For both of these barriers, a significant gender difference was identified, with higher proportions of male students endorsing these statements compared to female students ().
Table 8 Exercise barriers and facilitators, overall and by sex: N (%) students endorsing statements
Gender differences were also seen for other barriers, and in general higher proportions of male students were more likely to agree that barriers existed. The exception was lack of access to places to play, where a slightly higher proportion of female students (35%) reported this as a barrier compared to male students (34%) ().
Discussion
The results from this study indicate several areas in which healthy lifestyle interventions can be targeted. First, relatively few students held positive attitudes toward healthy food. Second, students identified both social and personal barriers to exercise that can be targeted in interventions. These barriers were more frequently reported for male students, suggesting that additional emphases in these areas can be included in interventions delivered at male schools.
In terms of the SALSA survey, most scales had reasonable reliability except low values of eating behaviors (0.05) and food preferences (0.30). Those low values are referred to variances in the nature of questions from asking about drinking water, tea, and juice to eating vegetables and fruits pertaining to validity, five scales (eating behaviors, food preferences, thoughts of eating, play and exercises, and encouraging scales) derived from SALSA survey entail items loading above 0.3 on their scales, in which these items are correlated well with each of them. This is considered the first preliminary factor analysis conducted for SALSA survey since its inception in Australia.
Few Jordanian high school students held positive attitudes toward healthy food. Students also reported several barriers to exercise, with some barriers more salient for male than female students.
These findings have some consistency with findings from other studies in Arab countries. For example, few gender-specific differences for barriers to healthy eating were identified for Kuwaiti university students, whereas such differences were found for barriers to physical activity.Citation22 Interestingly, Musaiger et al found these barriers to be more salient for female students than male students; for example, higher proportions of female students reported access to affordable places to be active and lack of skills for activity as barriers compared to male students. In a seven-country study of Arab adolescents, including Jordanian adolescents, aged 15–18, lack of enjoyment of and motivation for eating healthy foods was a barrier.Citation22 In this study, Jordanian adolescents also reported concern about lack of skills for physical activity as a barrier. Interestingly, higher proportions of Jordanian adolescents reported access to places to exercise as a barrier in Musaiger et al’s studyCitation22 than in our study (49% reporting it as “important” or “somewhat important” in that study, vs 35% in this study). One possible explanation for this difference is the different age groups, as the adolescents in Musaiger et al’s studyCitation22 were older. Another possibility is regional difference: data for this study were collected from a city in Northern Jordan, whereas Musaiger et al collected data from an unspecified “major city” in Jordan. Musaiger et alCitation22 also found that lack of information and motivation for healthy eating were significant barriers. Although our study did not evaluate this explicitly, it may be that lack of information around healthy food is a factor in students’ relative absence of positive attitudes regarding healthy eating. Regardless, the findings from the current study suggest that health-promoting interventions should target beliefs about healthy food and work to address personal and social barriers to exercise. The approach for addressing some of these barriers may need to be gender-specific.
Furthermore, obesity in children and youth has been associated with multifaceted barriers to adopt healthy eating and adequate physical activityCitation13,Citation23 including cultural norms, neighborhood characteristics, and school environment, and these can significantly differ among various settings.Citation24,Citation25 In the current study, participating students reported several barriers to healthy eating and physical activity with some of them having already been identified in the literature. For example, literature has identified several barriers to healthy eating, including easy access and low cost of fast food,Citation26–Citation29 which is not the case for healthy food.Citation30–Citation32 Adolescents’ attitude toward healthy food can significantly impact their eating behaviorsCitation30,Citation33,Citation34 including lack of funding to provide healthy food,Citation27 availability of unhealthy food at school,Citation29 insufficient food brought from home,Citation33,Citation35 and peer pressure such as teasing and stigma.Citation27,Citation29,Citation36,Citation37 School students tend to choose their food preferences and eating behaviors based on their parents’ preferences and beliefs. Consistent with the literature, the current study identified several barriers to regular exercise including school’s scarce physical activity opportunitiesCitation36,Citation38–Citation40 and lack of peer and parental supportCitation41,Citation42 can negatively impact adolescents’ attitude toward physical activity. Parents reported lack of time or motivation to exercise with their children.Citation43–Citation45 Interestingly, one of the barriers to regular exercise, as reported by students in the current study, was having nobody to exercise with, which could imply peers and friends. In Arab countries, the main barriers to healthy diet were lack of information related to healthy nutrition, motivation, and time to prepare or eat healthy foods due to school commitments.Citation22 These barriers were similar for physical activity as well.Citation22 In fact, Arab countries, including Jordan, have high availability of unhealthy food and low level of physical activity promoting high intake and low expenditure.Citation22
Conclusion
The Arabic version of SALSA survey is reliable and valid to determine attitudes and perceived barriers to healthy eating and physical activity in Jordanian adolescents. Positive attitudes and beliefs of healthy eating and adequate physical activity in Jordanian adolescents should be enriched through providing health education in school classes, improving schools’ facilities tailored to exercises performance, and enhancing sharing motivations and feelings about exercises among peers/friends in schools.
Ethics approval and consent to participate
Approval for the study was obtained from the Human Research Ethics Committees at the Ministry of Education, relevant educational school districts, and Jordan University of Science and Technology in Jordan. The study was carried out in accordance with the principles of the Declaration of Helsinki.
Author contributions
SS developed the original questionnaire and advised on the study. All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Abbreviations
| NCDs | = | noncommunicable diseases |
| PCA | = | principal components analysis |
| SALSA | = | Students As LifeStyle Activists |
| WHO | = | World Health Organization |
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Disclosure
The authors report no conflicts of interest in this work.
References
- World Health OrganizationChapter 2: The Double Burden: Emerging Epidemics and Persistent ProblemsWorld Health Report1999 Available from: http://www.who.int/whr/1999/en/Accessed 15 March 2018
- BoutayebABoutayebSThe burden of non communicable diseases in developing countriesInt J Equity Health200541215651987
- Al-NsourMZindahMBelbeisiAHadaddinRBrownDWWalkeHPrevalence of selected chronic, noncommunicable disease risk factors in Jordan: results of the 2007 Jordan behavioral risk factor surveillance surveyPrev Chronic Dis20129E2522172192
- LimSSVosTFlaxmanADA comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the global burden of Disease Study 2010Lancet201238098592224226023245609
- BaldwinWThe burden of non-communicable diseases in the developing worldAgency for Healthcare Research and Quality: Population Health: Behavioral and Social Science Insights2015 Available from: https://www.ahrq.gov/professionals/education/curriculum-tools/population-health/baldwin.htmlAccessed March 15, 2018
- CDCMMWR: Recommendations and Reports1996Guidelines for School Health Programs to Promote Lifelong Healthy Eating Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/00042446.htmAccessed January 4, 2019
- vander PloegKAMaximovaKMcGavockJDavisWVeugelersPDo school-based physical activity interventions increase or reduce inequalities in health?Soc Sci Med2014112808724820223
- Al-HaifiARAl-FayezMAAl-AthariBIRelative contribution of physical activity, sedentary behaviors, and dietary habits to the prevalence of obesity among Kuwaiti adolescentsFood Nutr Bull201334161323767276
- Al-KloubMIAl-HassanMAFroelicherESPredictors of obesity in school-aged Jordanian adolescentsInt J Nurs Pract201016439720649672
- HamaidehSHAl-KhateebRYAl-RawashdehABOverweight and obesity and their correlates among Jordanian adolescentsJ Nurs Scholarsh201042438739421091621
- Abu-MweisSSTayyemRFBawadiHAMusaigerAOAl-HazzaaHMEating habits, physical activity, and sedentary behaviors of Jordanian adolescents’ residents of AmmanMediterr J Nutr Metab2014716774
- Al AniMFAl SubhiLKBoseSConsumption of fruits and vegetables among adolescents: a multi-national comparison of eleven countries in the Eastern Mediterranean regionBr J Nutr201611561092109926817392
- Institute of Medicine (US) Committee on Prevention of Obesity in Children and YouthKoplanJPLivermanCTKraakVIPreventing Childhood Obesity: Health in the BalanceWashington DCNational Academies Press (US)2005
- Al-HazzaaHMAbahussainNAAl-SobayelHIQahwajiDMMusaigerAOLifestyle factors associated with overweight and obesity among Saudi adolescentsBMC Public Health201212135422591544
- Al-HazzaaHMAbahussainNAAl-SobayelHIQahwajiDMMusaigerAOPhysical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and regionInt J Behav Nutr Phys Act20118114022188825
- MusaigerAOAl-KandariFIAl-MannaiMPerceived barriers to weight maintenance among university students in Kuwait: the role of gender and obesityEnviron Health Prev Med201419320721424402439
- AllafiAAl-HaifiARAl-FayezMAPhysical activity, sedentary behaviours and dietary habits among Kuwaiti adolescents: gender differencesPublic Health Nutr20141792045205223987909
- FleissPMAn Analysis of Bias Regarding Circumcision in American Medical Literature Male and Female CircumcisionBoston, MASpringer1999379402
- CohenJStatistical Power Analysis for the Behavioral Sciences2nd edHillsdale, NJErlbaum1998
- ShahSPatching van der SluijsCLaglevaMA partnership for health – working with schools to promote healthy lifestyleAust Fam Physician20114012101122146334
- PolitDBeckCNursing Research: Generating and Assessing Evidence for Nursing Practice9th edPhiladelphia, PAWolters Kluwer Health/Lipppincott Williams and Wilkins2012
- MusaigerAOAl-MannaiMTayyemRPerceived barriers to healthy eating and physical activity among adolescents in seven Arab countries: a cross-cultural studySci World J201320131111
- LeviJSegalLMThomasKSt LaurentRLangARayburnJF as in fat: how obesity threatens America’s future2012 Available from: http://health-equity.lib.umd.edu/3975/1/F_as_in_Fat-_How_Obesity_Threatens_America%E2%80%99s_Future_2012.pdfAccessed March 12, 2019
- JonesLWellsKStrategies for academic and clinician engagement in community-participatory partnered researchJAMA2007297440741017244838
- WallersteinNDuranBCommunity-based participatory research contributions to intervention research: the intersection of science and practice to improve health equityAm J Public Health2010100Suppl 1S40S4620147663
- CrollJKNeumark-SztainerDStoryMHealthy eating: what does it mean to adolescents?J Nutr Educ200133419319811953240
- CullenKWWatsonKZakeriIImprovements in middle school student dietary intake after implementation of the Texas public school nutrition policyAm J Public Health200898111111718048778
- DrewnowskiASpecterSEPoverty and obesity: the role of energy density and energy costsAm J Clin Nutr200479161614684391
- GohYYBogartLMSipple-AsherBKUsing community-based participatory research to identify potential interventions to overcome barriers to adolescents’ healthy eating and physical activityJ Behav Med200932549150219544091
- HarrisonKMarskeALNutritional content of foods advertised during the television programs children watch mostAm J Public Health20059591568157416118368
- McKinleyMCLowisCRobsonPJIt’s good to talk: children’s views on food and nutritionEur J Clin Nutr200559454255115714214
- MonsivaisPDrewnowskiAThe rising cost of low-energy-density foodsJ Am Diet Assoc2007107122071207618060892
- EvansWDRenaudJMFinkelsteinEKamerowDBBrownDSChanging perceptions of the childhood obesity epidemicAm J Health Behav200630216717616533101
- ShepherdJHardenAReesRYoung people and healthy eating: a systematic review of research on barriers and facilitatorsHealth Educ Res200621223925716251223
- CrollJKNeumark-SztainerDStoryMWallMPerryCHarnackLAdolescents involved in weight-related and power team sports have better eating patterns and nutrient intakes than non-sport-involved adolescentsJ Am Diet Assoc2006106570971716647329
- BauerKWPatelAProkopLAAustinSBSwimming upstream: faculty and staff members from urban middle schools in low-income communities describe their experience implementing nutrition and physical activity initiativesPrev Chronic Dis200632A3716539778
- NollenNLBefortCASnowPDaleyCMEllerbeckEFAhluwaliaJSThe school food environment and adolescent obesity: qualitative insights from high school principals and food service personnelInt J Behav Nutr Phys Act2007411817511873
- HohepaMSchofieldGKoltGSPhysical activity: what do high school students think?J Adolesc Health200639332833616919793
- KubikMYLytleLFulkersonJAFruits, vegetables, and football: findings from focus groups with alternative high school students regarding eating and physical activityJ Adolesc Health200536649450015901514
- YoungDRFeltonGMGrieserMPolicies and opportunities for physical activity in middle school environmentsJ Sch Health2007771414717212759
- BauerKWYangYWAustinSB“How can we stay healthy when you’re throwing all of this in front of us?” Findings from focus groups and interviews in middle schools on environmental influences on nutrition and physical activityHealth Educ Behav2004311344614768656
- MabryIRYoungDRCooperLAMeyersTJoffeADugganAKPhysical activity attitudes of African American and white adolescent girlsAmbul Pediatr20033631231614616044
- Gordon-LarsenPNelsonMPagePPopkinBInequality in the built environment underlies key health disparities in physical activity and obesityPediatrics2006117241742416452361
- HarrisonKMarskeALNutritional content of foods advertised during the television programs children watch mostAm J Public Health20059591568157416118368
- HeskethKWatersEGreenJSalmonLWilliamsJHealthy eating, activity and obesity prevention: a qualitative study of parent and child perceptions in AustraliaHealth Promot Int2005201192615668217