
Abstract
Myopia is a common disorder, affecting approximately one-third of the US population and over 90% of the population in some East Asian countries. High amounts of myopia are associated with an increased risk of sight-threatening problems, such as retinal detachment, choroidal degeneration, cataracts, and glaucoma. Slowing the progression of myopia could potentially benefit millions of children in the USA. To date, few strategies used for myopia control have proven to be effective. Treatment options such as undercorrection of myopia, gas permeable contact lenses, and bifocal or multifocal spectacles have all been proven to be ineffective for myopia control, although one recent randomized clinical trial using executive top bifocal spectacles on children with progressive myopia has shown to decrease the progression to nearly half of the control subjects. The most effective methods are the use of orthokeratology contact lenses, soft bifocal contact lenses, and topical pharmaceutical agents such as atropine or pirenzepine. Although none of these modalities are US Food and Drug Administration-approved to slow myopia progression, they have been shown to slow the progression by approximately 50% with few risks. Both orthokeratology and soft bifocal contact lenses have shown to slow myopia progression by slightly less than 50% in most studies. Parents and eye care practitioners should work together to determine which modality may be best suited for a particular child. Topical pharmaceutical agents such as anti-muscarinic eye drops typically lead to light sensitivity and poor near vision. The most effective myopia control is provided by atropine, but is rarely prescribed due to the side effects. Pirenzepine provides myopia control with little light sensitivity and few near-vision problems, but it is not yet commercially available as an eye drop or ointment. Several studies have shown that lower concentrations of atropine slow the progression of myopia control with fewer side effects than 1% atropine. While the progression of myopic refractive error is slowed with lower concentration of atropine, the growth of the eye is not, indicating a potentially reversible form of myopia control that may diminish after discontinuation of the eye drops. This review provides an overview of the myopia control information available in the literature and raises questions that remain unanswered, so that eye care practitioners and parents can potentially learn the methods that may ultimately improve a child’s quality of life or lower the risk of sight-threatening complications.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Myopia, also known as nearsightedness, is caused by an increase in eye length or corneal curvature and this condition causes light from distant objects to focus in front of the retina. Light focused in front of the retina results in blurry vision while looking at far away objects but clear vision while looking at close objects.
Myopia affects approximately one-third of the US population,Citation1 but the prevalence ranges from as low as 3% for Sherpa in NepalCitation2 to over 90% in Taiwan University students.Citation3 In general, the prevalence of myopia is highest in Asian children,Citation4–Citation7 followed by Hispanic, and then black and white children.Citation6,Citation7 Some studies report a greater proportion of myopic females,Citation8–Citation11 but others report a similar prevalence between sexes.Citation12–Citation14 Myopia typically develops at approximately 8 years of age and progresses through 15 or 16 years of age,Citation15,Citation16 and the average rate of progression is approximately 0.50 D (diopter) per year.Citation17–Citation20
Although myopia is a prevalent disease, little is known about the risk factors that lead to the development and progression of myopia. Genetics appear to play a role in determining a child’s refractive error status. The risk of becoming myopic increases with the number of myopic parents,Citation21–Citation23 monozygotic twins have significantly stronger correlation of refractive error than dizygotic twins,Citation24,Citation25 and genetic factors are more responsible for variability in refractive error than environmental factors.Citation26,Citation27 However, no single chromosomal locus has been consistently associated with myopia.Citation28–Citation38 While near work has long been suspected to be a risk factor for myopia, few studies have found a strong correlation with either the onset or progression of myopia.Citation21–Citation23,Citation39–Citation41 However, spending more time outdoors has been shown to decrease the likelihood of becoming myopic,Citation22,Citation42–Citation46 but does not slow down the progression of myopia.Citation41,Citation47 Some schools in Taiwan were randomly assigned to encourage outdoor activities during recess, while other schools maintained their normal routine during recess. In the schools that encouraged more outdoor activities during recess, only 8.4% of children became myopic, compared to 17.7% in the schools that maintained their normal recess activities (P<0.001). However, the myopic children who were encouraged to spend time outdoors during recess progressed in myopia at the same rate as those who maintained their typical recess activities (P=0.18).Citation47
Higher amounts of myopia increase the risk of ocular complications such as glaucoma,Citation48–Citation51 cataracts,Citation52–Citation55 and retinal detachment and atrophy.Citation56–Citation60 Due to these sight-threatening complications and the high worldwide prevalence, research scientists have attempted many methods to reduce the progression of nearsightedness, including undercorrection of myopic refractive error,Citation61,Citation62 bifocal or multifocal spectacles,Citation17,Citation18,Citation63–Citation65 gas permeable contact lenses,Citation19,Citation66 topical pharmaceutical agents,Citation67–Citation73 orthokeratology contact lenses,Citation74–Citation79 and soft bifocal contact lenses.Citation80–Citation83
Undercorrection of Myopia
Myopes read moreCitation84,Citation85 and scholastically perform betterCitation86,Citation87 than emmetropes or hyperopes, so accommodative effort and myopia may be associated. Myopic patients also have a higher accommodative lag than emmetropic patients,Citation88–Citation91 and the lag of accommodation focuses light behind the retina during near work, potentially acting as a putative cue for increased myopia progression. Undercorrection of myopia reduces accommodative effort and accommodative error (lag), and hence is thought to slow myopia progression. In actuality, undercorrecting a child’s refractive error either increasesCitation62 or has no effect on myopia progression,Citation61 and so undercorrection does not slow myopia progression.
Bifocal or multifocal spectacles
A great deal of research has examined the effect of bifocal or multifocal spectacles on myopia progression.Citation17,Citation18,Citation63–Citation65 These glasses allow children to clearly see far away objects through the top portion of the spectacle lens. The bottom portion of the lens contains the reading power, which may control myopia progression by reducing or eliminating the accommodative effort or error associated with myopia.Citation88–Citation91 When compared to single vision lenses, bifocal or multifocal lenses slow the progression of myopia, but the difference in progression rates is typically not clinically meaningful.Citation17,Citation18,Citation64,Citation65 Even myopic children believed to benefit most from bifocal or multifocal spectacle myopia control – those with esophoria (the resting position of the eyes is too close to the nose) and accommodative lag – do not exhibit clinically meaningful slowing of myopia progression.Citation17,Citation65 The most promising method of bifocal spectacle myopia control was reported by Cheng et al.Citation63 They provided executive top bifocal spectacles and base-in prisms to children with progressing myopia and showed that the progression slowed by 51% over 3 years. The base-in prism did not result in additional treatment effect, but it is unknown whether they found a stronger treatment effect than other bifocal or multifocal spectacle myopia control studies because they utilized an executive top bifocal spectacle lens or because they only enrolled progressing myopes, which allowed for better myopia control.Citation63
Gas permeable contact lenses
Alignment-fit gas permeable contact lenses worn during the day slowed myopia progression in early studies, but all those studies suffered from study design issues such as unequal loss to follow-up, enrollment of subjects outside of the expected age of progression, and lack of randomization.Citation92–Citation95 Two more recent randomized clinical trials showed that gas permeable contact lenses do not slow the growth of the eye.Citation19,Citation66 Although Walline et al reported significantly slower myopia progression in the gas permeable contact lens group, they found no difference in the eye growth.Citation19 The treatment effect was mostly due to the differences in corneal curvature at the end of the study. Because corneal curvature changes are temporary, the slowed myopia progression is unlikely to be permanent, so the authors concluded that children should not be fitted with gas permeable contact lenses solely to slow the progression of myopia.Citation19
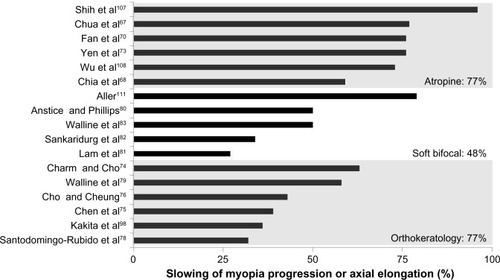
In order to be considered clinically meaningful, a myopia control modality should slow the progression by approximately 50%, according to most myopia control grant applications. Only three modalities are currently considered to be at least close to this level of myopia control: orthokeratology contact lenses, soft bifocal contact lenses, and topical pharmaceutical agents ().
Figure 1 Percent slowing of myopia progression by atropine, soft bifocal, or orthokeratology contact lenses in controlled studies published in the literature.
Orthokeratology contact lenses
Orthokeratology contact lenses are worn overnight to flatten the central cornea and temporarily reduce the amount of myopia. Orthokeratology contact lenses provide clear vision without the need for vision correction during the day, and they also reduce myopic progression ().Citation74–Citation79,Citation96–Citation98 These contact lenses are thought to slow myopia progression optically. Light that focuses in front of the retina (myopic blur) acts as a putative signal to slow the eye growth. Orthokeratology contact lenses correct central refractive error while leaving peripheral myopic blur, which acts as a putative cue to slow the progression of myopia.Citation98–Citation100 Because these contact lenses are worn overnight, they are associated with an increased risk of microbial keratitis, which may be as high as wearing soft contact lenses overnight.Citation101
Table 1 Axial elongation of orthokeratology contact lens wearers compared to controls
Orthokeratology contact lenses slow axial length growth compared to single vision gas permeable contact lenses,Citation96 single vision soft contact lenses,Citation79 and single vision spectacles.Citation74–Citation76,Citation97,Citation98,Citation102 The first randomized clinical trial of orthokeratology myopia control demonstrated significantly slower mean (± standard deviation) axial elongation in children wearing orthokeratology lenses (0.36±0.24 mm) than children wearing single vision spectacles (0.63±0.26 mm, P<0.01).Citation76
Soft bifocal contact lenses
Soft bifocal contact lenses are typically worn by patients 40 years old or older to provide clearer vision while reading. Soft bifocal contact lenses with a center distance design (reading portion outside the central contact lens) also slow myopic progression by creating myopic defocus in the periphery,Citation103 which acts as a putative signal to slow the eye growth. However, these lenses are worn during the day and fitted more commonly than orthokeratology contact lenses. Several nonrandomized, controlled clinical trials have shown the myopia control benefit of soft bifocal contact lenses.Citation80–Citation83 Overall, soft bifocal contact lenses slow the progression of myopia in children by nearly 50%, which is similar to orthokeratology contact lenses ().
Table 2 Changes in refractive error with soft bifocal contact lenses compared to single vision contact lens wearers
Topical pharmaceutical agents
Topical pharmaceutical methods to control myopic progression in children are anti-muscarinic eye drops that are used in routine eye care to dilate the pupil and reduce or eliminate accommodation. Atropine is a broad spectrum anti-muscarinic agent and side effects include temporary sensitivity to light and unclear vision at near. Pirenzepine affects only M1 anti-muscarinic receptors, which are less concentrated in the iris and ciliary body, and hence does not dilate the pupil or reduce accommodation as much as atropine.
Although the specific myopia control mechanism of anti-muscarinic agents is unknown, studies show both pirenzepine and atropine are very effective at reducing myopic eye growth in children ().Citation70,Citation71,Citation73,Citation104–Citation108 However, atropine is rarely prescribed due to the side effects, and pirenzepine is not approved by the US Food and Drug Administration (FDA) for myopia control, nor is it commercially available.
Table 3 Effects of pharmaceutical agents on myopia progression compared to control groups
Lower concentrations of atropine may provide clinically meaningful myopia control while minimizing side effects.Citation68,Citation69,Citation71,Citation107 Chia et al randomly assigned myopic children to 0.5%, 0.1%, and 0.01% atropine eye drops.Citation68 Over 2 years, myopia progressed −0.30±0.60 D for the 0.5% group, −0.38±0.60 D for the 0.1% group, and −0.49±0.63 D for the 0.01% groups. All were significantly slower than the historical placebo control group. There was no difference between the groups in terms of best-corrected distance visual acuity, but the subjects with higher concentration of atropine had worse near visual acuity while wearing correction for distance vision. Subjects in this investigation were told that if they had trouble reading at near, they could request for reading glasses to help them see more clearly; 70% of children on 0.5% atropine, 61% of children on 0.1% atropine, and only 6% of children on 0.01% atropine requested the glasses to improve near vision.Citation68 Although myopic progression was slowed by the lower concentration of eye drops, axial elongation of the eye was not.Citation69 This result is puzzling and suggests that the myopia control may be due to changes in crystalline lens curvatures secondary to reduced tonic accommodation while the eyes are at rest. In fact, 1 year after discontinuation of the various concentrations of atropine eye drops, the most effective myopia control was provided by 0.01% atropine,Citation69 presumably because the accommodative tonus returned to normal, negating the stronger myopia control effect due primarily to changes in tonic accommodation. In a separate study, 0.025% atropine was found to reduce the onset of myopia from 54% to 21% (P=0.016).Citation110
The most effective myopia control was provided by topical pharmaceutical agents, but they are rarely prescribed due to the side effects. While lower concentrations provide clinically meaningful myopia control, the mechanism may be at least partially due to temporary changes in tonic accommodation and may not lead to permanent decreases in myopia progression.
Conclusion
Of all the methods studied to slow the progression of myopia, topical pharmaceutical agents, orthokeratology contact lenses, and soft bifocal contact lenses were found to be the most effective, commercially available modalities. However, none of them is approved by the FDA to slow the progression of myopia. Topical pharmaceuticals are not used frequently due to the side effects, primarily photophobia and reduced near vision and accommodation, but there is potential for myopia control with fewer side effects using lower concentrations. Orthokeratology contact lenses and soft bifocal contact lenses slow the myopic progression of myopia in a similar manner, so the best modality should be determined by the eye care practitioner and parent, based on the lifestyle of the specific child. Bifocal and multifocal spectacles is statistically significant in slowing the myopia progression, but do not provide a clinically meaningful effect; however, the latest randomized clinical trial using executive top bifocal spectacles on progressing myopes exhibited a clinically meaningful slowing of myopia progression. Undercorrection of myopia and gas permeable contact lenses were not found to slow the progression of myopia in children.
Although we have answered many questions about slowing of myopia progression in children, many questions remain to be answered. For example, will soft bifocal contact lenses with the reading portion in the center of the contact lenses also slow myopia progression? Will the implementation of both optical (soft bifocal or orthokeratology contact lenses) and pharmacologic (atropine) myopia control methods provide better myopia control than either one alone? Can we permanently reduce the risk of myopia onset using these myopia control methods? What happens to myopia progression once the myopia control modalities are discontinued? Far more research needs to be conducted to answer these important questions so that we can optimize eye care for children and potentially prevent or maintain lower amount of myopia, which may reduce the risk of sight-threatening complications.
Disclosure
The authors report no conflicts of interest in this work.
References
- VitaleSEllweinLCotchMFFerrisFL3rdSperdutoRPrevalence of refractive error in the United States, 1999–2004Arch Ophthalmol200812681111111918695106
- GarnerLFOwensHKinnearRFFrithMJPrevalence of myopia in Sherpa and Tibetan children in NepalOptom Vis Sci199976528228510375242
- WangTJChiangTHWangTHLinLLShihYFChanges of the ocular refraction among freshmen in National Taiwan University between 1988 and 2005Eye (Lond)20092351168116918551136
- IpJMHuynhSCRobaeiDEthnic differences in refraction and ocular biometry in a population-based sample of 11–15-year-old Australian childrenEye (Lond)200822564965617277756
- IpJMHuynhSCRobaeiDEthnic differences in the impact of parental myopia: findings from a population-based study of 12-year-old Australian childrenInvest Ophthalmol Vis Sci20074862520252817525179
- KleinsteinRNJonesLAHullettSRefractive error and ethnicity in childrenArch Ophthalmol200312181141114712912692
- VooILeeDAOelrichFOPrevalences of ocular conditions among Hispanic, white, Asian, and black immigrant students examined by the UCLA Mobile Eye ClinicJ Am Optom Assoc19986942552619585665
- Bar DayanYLevinAMoradYThe changing prevalence of myopia in young adults: a 13-year series of population-based prevalence surveysInvest Ophthalmol Vis Sci20054682760276516043848
- DandonaRDandonaLSrinivasMRefractive error in children in a rural population in IndiaInvest Ophthalmol Vis Sci200243361562211867575
- HashemiHFotouhiAMohammadKThe age- and gender-specific prevalences of refractive errors in Tehran: the Tehran Eye StudyOphthalmic Epidemiol200411321322515370553
- HeMHuangWZhengYHuangLEllweinLBRefractive error and visual impairment in school children in rural southern ChinaOphthalmology2007114237438217123622
- AtteboKIversRQMitchellPRefractive errors in an older population: the Blue Mountains Eye StudyOphthalmology199910661066107210366072
- JunghansBMCrewtherSGPrevalence of myopia among primary school children in eastern SydneyClin Exp Optom200386533934514558856
- KatzJTielschJMSommerAPrevalence and risk factors for refractive errors in an adult inner city populationInvest Ophthalmol Vis Sci19973823343409040465
- GossDACoxVDTrends in the change of clinical refractive error in myopesJ Am Optom Assoc19855686086134031351
- ThornFGwiazdaJHeldRMyopia progression is specified by a double exponential growth functionOptom Vis Sci200582428629715829846
- FulkGWCyertLAParkerDEA randomized trial of the effect of single-vision vs bifocal lenses on myopia progression in children with esophoriaOptom Vis Sci200077839540110966065
- GwiazdaJHymanLHusseinMA randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in childrenInvest Ophthalmol Vis Sci20034441492150012657584
- WallineJJJonesLAMuttiDOZadnikKA randomized trial of the effects of rigid contact lenses on myopia progressionArch Ophthalmol2004122121760176615596577
- WallineJJJonesLASinnottLRandomized trial of the effect of contact lens wear on self-perception in childrenOptom Vis Sci200986322223219214129
- SawSMShankarATanSBA cohort study of incident myopia in Singaporean childrenInvest Ophthalmol Vis Sci20064751839184416638989
- JonesLASinnottLTMuttiDOMitchellGLMoeschbergerMLZadnikKParental history of myopia, sports and outdoor activities, and future myopiaInvest Ophthalmol Vis Sci20074883524353217652719
- MuttiDOMitchellGLMoeschbergerMLJonesLAZadnikKParental myopia, near work, school achievement, and children’s refractive errorInvest Ophthalmol Vis Sci200243123633364012454029
- DiraniMChamberlainMShekarSNHeritability of refractive error and ocular biometrics: the Genes in Myopia (GEM) twin studyInvest Ophthalmol Vis Sci200647114756476117065484
- HeMHurYMZhangJDingXHuangWWangDShared genetic determinant of axial length, anterior chamber depth, and angle opening distance: the Guangzhou Twin Eye StudyInvest Ophthalmol Vis Sci200849114790479418586876
- HammondCJSniederHGilbertCESpectorTDGenes and environment in refractive error: the twin eye studyInvest Ophthalmol Vis Sci20014261232123611328732
- LyhneNSjolieAKKyvikKOGreenAThe importance of genes and environment for ocular refraction and its determiners: a population based study among 20–45 year old twinsBr J Ophthalmol200185121470147611734523
- ChenCYStankovichJScurrahKJLinkage replication of the MYP12 locus in common myopiaInvest Ophthalmol Vis Sci200748104433443917898262
- CinerEIbayGWojciechowskiRGenome-wide scan of African-American and white families for linkage to myopiaAm J Ophthalmol20091473512517.e219026404
- CinerEWojciechowskiRIbayGBailey-WilsonJEStambolianDGenomewide scan of ocular refraction in African-American families shows significant linkage to chromosome 7p15Genet Epidemiol200832545446318293391
- HammondCJAndrewTMakYTSpectorTDA susceptibility locus for myopia in the normal population is linked to the PAX6 gene region on chromosome 11: a genomewide scan of dizygotic twinsAm J Hum Genet200475229430415307048
- KleinAPDuggalPLeeKEKleinRBailey-WilsonJEKleinBEConfirmation of linkage to ocular refraction on chromosome 22q and identification of a novel linkage region on 1qArch Ophthalmol20071251808517210856
- MuttiDOCooperMEO’BrienSCandidate gene and locus analysis of myopiaMol Vis2007131012101917653045
- MuttiDOSeminaEMarazitaMCooperMMurrayJCZadnikKGenetic loci for pathological myopia are not associated with juvenile myopiaAm J Med Genet. 120021124355360
- SchacheMRichardsonAJMitchellPGenetic association of refractive error and axial length with 15q14 but not 15q25 in the Blue Mountains Eye Study cohortOphthalmology2013120229229723131718
- SchacheMRichardsonAJPertileKKDiraniMScurrahKBairdPNGenetic mapping of myopia susceptibility lociInvest Ophthalmol Vis Sci200748114924492917962440
- WojciechowskiRStambolianDCinerEIbayGHolmesTNBailey-WilsonJEGenomewide linkage scans for ocular refraction and meta-analysis of four populations in the Myopia Family StudyInvest Ophthalmol Vis Sci20095052024203219151385
- ZhuGHewittAWRuddleJBGenetic dissection of myopia: evidence for linkage of ocular axial length to chromosome 5qOphthalmology2008115610531057.e2
- RichlerABearJCRefraction, nearwork and education. A population study in NewfoundlandActa Ophthalmol (Copenh)19805834684787415832
- AngleJWissmannDAThe epidemiology of myopiaAm J Epidemiol198011122202287355884
- Jones-JordanLASinnottLTCotterSATime outdoors, visual activity, and myopia progression in juvenile-onset myopesInvest Ophthalmol Vis Sci201253117169717522977132
- DiraniMTongLGazzardGOutdoor activity and myopia in Singapore teenage childrenBr J Ophthalmol2009938997100019211608
- GuggenheimJANorthstoneKMcMahonGTime outdoors and physical activity as predictors of incident myopia in childhood: a prospective cohort studyInvest Ophthalmol Vis Sci20125362856286522491403
- Jones-JordanLASinnottLTGrahamNDThe contributions of near work and outdoor activity to the correlation between siblings in the Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error (CLEERE) StudyInvest Ophthalmol Vis Sci201455106333633925205866
- LinZVasudevanBJhanjiVNear work, outdoor activity, and their association with refractive errorOptom Vis Sci201491437638224637483
- RoseKAMorganIGIpJOutdoor activity reduces the prevalence of myopia in childrenOphthalmology200811581279128518294691
- WuPCTsaiCLWuHLYangYHKuoHKOutdoor activity during class recess reduces myopia onset and progression in school childrenOphthalmology201312051080108523462271
- MitchellPHourihanFSandbachJWangJJThe relationship between glaucoma and myopia: the Blue Mountains Eye StudyOphthalmology1999106102010201510519600
- PonteFGiuffreGGiammancoRDardanoniGRisk factors of ocular hypertension and glaucoma. The Casteldaccia Eye StudyDoc Ophthalmol19948532032107924848
- YoshidaMOkadaEMizukiNAge-specific prevalence of open-angle glaucoma and its relationship to refraction among more than 60,000 asymptomatic Japanese subjectsJ Clin Epidemiol200154111151115811675167
- WongTYKleinBEKleinRKnudtsonMLeeKERefractive errors, intraocular pressure, and glaucoma in a white populationOphthalmology200310121121712511368
- LimRMitchellPCummingRGRefractive associations with cataract: the Blue Mountains Eye StudyInvest Ophthalmol Vis Sci199940123021302610549667
- McCartyCAMukeshBNFuCLTaylorHRThe epidemiology of cataract in AustraliaAm J Ophthalmol1999128444646510577586
- WongTYKleinBEKleinRTomanySCLeeKERefractive errors and incident cataracts: the Beaver Dam Eye StudyInvest Ophthalmol Vis Sci20014271449145411381046
- YounanCMitchellPCummingRGRochtchinaEWangJJMyopia and incident cataract and cataract surgery: the Blue Mountains Eye StudyInvest Ophthalmol Vis Sci200243123625363212454028
- CurtinBThe Myopias: Basic Science and Clinical ManagementPhiladelphia, PAHarper and Row, Publishers, Inc1985
- KarlinDBCurtinBJPeripheral chorioretinal lesions and axial length of the myopic eyeAm J Ophthalmol19768156256351275043
- PierroLCamesascaFIMischiMBrancatoRPeripheral retinal changes and axial myopiaRetina199212112171565864
- CelorioJMPruettRCPrevalence of lattice degeneration and its relation to axial length in severe myopiaAm J Ophthalmol1991111120231985485
- Risk factors for idiopathic rhegmatogenous retinal detachment. The Eye Disease Case-Control Study GroupAm J Epidemiol199313777497578484366
- AdlerDMillodotMThe possible effect of undercorrection on myopic progression in childrenClin Exp Optom200689531532116907670
- ChungKMohidinNO’LearyDJUndercorrection of myopia enhances rather than inhibits myopia progressionVision Res200242222555255912445849
- ChengDWooGCDrobeBSchmidKLEffect of bifocal and prismatic bifocal spectacles on myopia progression in children: three-year results of a randomized clinical trialJAMA Ophthalmol2014132325826424435660
- BerntsenDASinnottLTMuttiDOZadnikKA randomized trial using progressive addition lenses to evaluate theories of myopia progression in children with a high lag of accommodationInvest Ophthalmol Vis Sci201253264064922205604
- Correction of Myopia Evaluation Trial 2 Study Group for the Pediatric Eye Disease Investigator GroupProgressive-addition lenses versus single-vision lenses for slowing progression of myopia in children with high accommodative lag and near esophoriaInvest Ophthalmol Vis Sci20115252749275721282579
- KatzJScheinODLevyBA randomized trial of rigid gas permeable contact lenses to reduce progression of children’s myopiaAm J Ophthalmol20031361829012834674
- ChuaWHBalakrishnanVChanYHAtropine for the treatment of childhood myopiaOphthalmology2006113122285229116996612
- ChiaAChuaWHCheungYBAtropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2)Ophthalmology2012119234735421963266
- ChiaAChuaWHWenLFongAGoonYYTanDAtropine for the treatment of childhood myopia: changes after stopping atropine 0.01%, 0.1% and 0.5%Am J Ophthalmol20141572451457.e124315293
- FanDSLamDSChanCKFanAHCheungEYRaoSKTopical atropine in retarding myopic progression and axial length growth in children with moderate to severe myopia: a pilot studyJpn J Ophthalmol2007511273317295137
- LeeJJFangPCYangIHPrevention of myopia progression with 0.05% atropine solutionJ Ocul Pharmacol Ther2006221414616503774
- TongLHuangXLKohALZhangXTanDTChuaWHAtropine for the treatment of childhood myopia: effect on myopia progression after cessation of atropineOphthalmology2009116357257919167081
- YenMYLiuJHKaoSCShiaoCHComparison of the effect of atropine and cyclopentolate on myopiaAnn Ophthalmol19892151801821872742290
- CharmJChoPHigh myopia-partial reduction ortho-k: a 2-year randomized studyOptom Vis Sci201390653053923645372
- ChenCCheungSWChoPMyopia control using toric orthokeratology (TO-SEE study)Invest Ophthalmol Vis Sci201354106510651724003088
- ChoPCheungSWRetardation of myopia in Orthokeratology (ROMIO) study: a 2-year randomized clinical trialInvest Ophthalmol Vis Sci201253117077708522969068
- ChoPCheungSWEdwardsMThe longitudinal orthokeratology research in children (LORIC) in Hong Kong: a pilot study on refractive changes and myopic controlCurr Eye Res2005301718015875367
- Santodomingo-RubidoJVilla-CollarCGilmartinBGutierrez-OrtegaRMyopia control with orthokeratology contact lenses in spain (MCOS): refractive and biometric changesInvest Ophthalmol Vis Sci20125385060506522729437
- WallineJJJonesLASinnottLTCorneal reshaping and myopia progressionBr J Ophthalmol20099391181118519416935
- AnsticeNSPhillipsJREffect of dual-focus soft contact lens wear on axial myopia progression in childrenOphthalmology201111861152116121276616
- LamCSTangWCTseDYTangYYToCHDefocus Incorporated Soft Contact (DISC) lens slows myopia progression in Hong Kong Chinese schoolchildren: a 2-year randomised clinical trialBr J Ophthalmol2014981404524169657
- SankaridurgPHoldenBSmithE3rdDecrease in rate of myopia progression with a contact lens designed to reduce relative peripheral hyperopia: one-year resultsInvest Ophthalmol Vis Sci201152139362936722039230
- WallineJJGreinerKLMcVeyMEJones-JordanLAMultifocal contact lens myopia controlOptom Vis Sci201390111207121424061152
- GrishamJDSimonsHDRefractive error and the reading process: a literature analysisJ Am Optom Assoc198657144553512675
- GrosvenorTAre visual anomalies related to reading ability?J Am Optom Assoc1977484510517301532
- WilliamsSMSandersonGFShareDLSilvaPARefractive error, IQ and reading ability: a longitudinal study from age seven to 11Dev Med Child Neurol19883067357423234604
- SimonsHDGasslerPAVision anomalies and reading skill: a meta-analysis of the literatureAm J Optom Physiol Opt198865118939043252737
- MuttiDOMitchellGLHayesJRAccommodative lag before and after the onset of myopiaInvest Ophthalmol Vis Sci200647383784616505015
- NakatsukaCHasebeSNonakaFOhtsukiHAccommodative lag under habitual seeing conditions: comparison between myopic and emmetropic childrenJap J Ophthalmol200549318919415944822
- GwiazdaJBauerJThornFHeldRA dynamic relationship between myopia and blur-driven accommodation in school-aged childrenVision Res1995359129913047610590
- GwiazdaJThornFBauerJHeldRMyopic children show insufficient accommodative response to blurInvest Ophthalmol Vis Sci19933436906948449687
- KellerJMyopia control with RGPs in childrenCont Lens Spect1996114548
- KhooCYChongJRajanUA 3-year study on the effect of RGP contact lenses on myopic childrenSingapore Med J199940423023710487074
- PerriginJPerriginDQuinteroSGrosvenorTSilicone-acrylate contact lenses for myopia control: 3-year resultsOptom Vis Sci199067107647692247299
- StoneJThe possible influence of contact lenses on myopiaBr J Physiol Opt1976313891141052437
- SwarbrickHAAlharbiAWattKLumEKangPMyopia control during orthokeratology lens wear in children using a novel study designOphthalmology2015122362063025439432
- HiraokaTKakitaTOkamotoFTakahashiHOshikaTLong-term effect of overnight orthokeratology on axial length elongation in childhood myopia: a 5-year follow-up studyInvest Ophthalmol Vis Sci20125373913391922577080
- KakitaTHiraokaTOshikaTInfluence of overnight orthokeratology on axial elongation in childhood myopiaInvest Ophthalmol Vis Sci20115252170217421212181
- SmithELHungLFHarwerthRSEffects of optically induced blur on the refractive status of young monkeysVision Res19943432933018160365
- TroiloDWallmanJThe regulation of eye growth and refractive state: an experimental study of emmetropizationVision Res1991317–8123712501891815
- BullimoreMASinnottLTJones-JordanLAThe risk of microbial keratitis with overnight corneal reshaping lensesOptom Vis Sci201390993794423892491
- Santodomingo-RubidoJVilla-CollarCGilmartinBGutierrez-OrtegaRMyopia control with orthokeratology contact lenses in Spain: refractive and biometric changesInvest Ophthalmol Vis Sci20125385060506522729437
- TicakAWallineJJPeripheral optics with bifocal soft and corneal reshaping contact lensesOptom Vis Sci20139013823222924
- SiatkowskiRMCotterSMillerJMSafety and efficacy of 2% pirenzepine ophthalmic gel in children with myopia: a 1-year, multicenter, double-masked, placebo-controlled parallel studyArch Ophthalmol2004122111667167415534128
- SiatkowskiRMCotterSACrockettRSTwo-year multicenter, randomized, double-masked, placebo-controlled, parallel safety and efficacy study of 2% pirenzepine ophthalmic gel in children with myopiaJ AAPOS200812433233918359651
- TanDTLamDSChuaWHShu-PingDFCrockettRSAsian Pirenzepine Study GOne-year multicenter, double-masked, placebo-controlled, parallel safety and efficacy study of 2% pirenzepine ophthalmic gel in children with myopiaOphthalmology20051121849115629825
- ShihYFChenCHChouACHoTCLinLLHungPTEffects of different concentrations of atropine on controlling myopia in myopic childrenJ Ocul Pharmacol Ther1999151859010048351
- WuPCYangYHFangPCThe long-term results of using low-concentration atropine eye drops for controlling myopia progression in schoolchildrenJ Ocul Pharmacol Ther201127546146621815829
- WuPCYangYHFangPCThe long-term results of using low-concentration atropine eye drops for controlling myopia progression in schoolchildrenJ Ocul Pharmacol Ther201127546146621815829
- FangPCChungMYYuHJWuPCPrevention of myopia onset with 0.025% atropine in premyopic childrenJ Ocul Pharmacol Ther201026434134520698798
- AllerTWildsoetCResults of a one-year prospective clinical trial (CONTROL) of the use of bifocal soft contact lenses to control myopia progressionOphthalmic Physiol Opt20062689