
Abstract
Youth and young adults (19–24 years of age) shoulder the burden of sexually transmitted infections accounting for nearly half of all new infections annually. Mobile technology is one way that we have reached this population with safer sex information but challenges exist with the delivery process. The literature between 2010 and 2015 was reviewed for data on safe sex and sexual health information delivered using mobile cell phone devices. A search for relevant databases revealed that 17 articles met our inclusion criteria. Findings suggest that mobile cell phone interventions are an effective mode for delivering safe sex and sexual health information to youth; those at the highest risk may not be able to access cell phones based on availability and cost of the text messages or data plans.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
According to the Centers for Disease Control and Prevention, nearly 19.7 million sexually transmitted infections (STIs) occur each year.Citation1 While preventable, these infections are a major health concern because of the probability that those infected will be reinfected with the same STI or a new one. Youth and young adults (19–24 years of age) account for nearly half of the new infections,Citation1 primarily as a result of risky sexual behaviors. Among high school students surveyed in the 2013 Youth Behavior Surveillance Survey,Citation2 47% reported having had sexual intercourse, 34% had had sexual intercourse during the previous 3 months, and of these 41% did not use a condom the last time they had sex. Additionally, 15% of the youth had had sex with four or more people during their life, and only 22% reported having ever been tested for HIV.
Mobile technology has become a popular option for delivering safer sex interventions for adolescents. According to a Pew Research Center survey, 78% of teens now have a cell phone and almost half (47%) own Smartphones.Citation3 One in four teens (23%) has a tablet computer, and 93% have a computer or have access to one at home. In addition, seven in ten (71%) have access to a laptop or desktop that is shared with family members, making access to social media sites and text messaging a safer sex health promotion option. However, despite the increased use of mobile technology, it remains unclear how effective safer sex education is in reducing sexual risk behaviors. Accordingly, we conducted a review of the literature to examine current practices and recommendations for future use of mobile technology for promoting sexual health and reducing the risk of STIs among youth.
Methods
Studies were included in the review if they: 1) were original reports; 2) pertained to sexual health; 3) used a quantitative or qualitative research design; 4) involved adolescents or had the word adolescent in the title; 5) were published in a peer reviewed journal; and 6) were conducted within the past 5 years. Studies were excluded if published in languages other than English. Based on the National Institutes of Health definition of a childCitation4 and the World Health Organization definition of adolescence, we set the upper age limit of 20 years and the lower age limit of 12 years for adolescence.Citation5 We defined safe sex as the ability to prevent oneself and a sexual partner from contracting an STI or becoming pregnant by using protective devices, such as condoms or dental dams.
The literature review was conducted using PyscInfo, PubMed, CINAHL, Medline, and Cochrane Review databases from 2010 to 2015. The following search terms were used: research, adolescent, safer sex, sexual education, sexuality programs, and mobile technology (text messaging and mobile phones). Reference lists from each article were reviewed for additional citations, and those meeting the inclusion criteria were added. Relevant studies were also uncovered by doing a manual search in journals that published articles on mobile technology and sexual health. A total of 295 abstracts were retrieved and 17 articles met the inclusion criteria (see ). Each study was read and coded according to the study purpose, design, sample, measures, major findings, and limitations. All extracted data were then read, coded, and discussed by the two authors who compared their coding and preliminary findings to confirm the accuracy of their interpretations for each study (Miles and Huberman).Citation6 provides the citations and key components of the studies.
Figure 1 Inclusion/exclusion data.
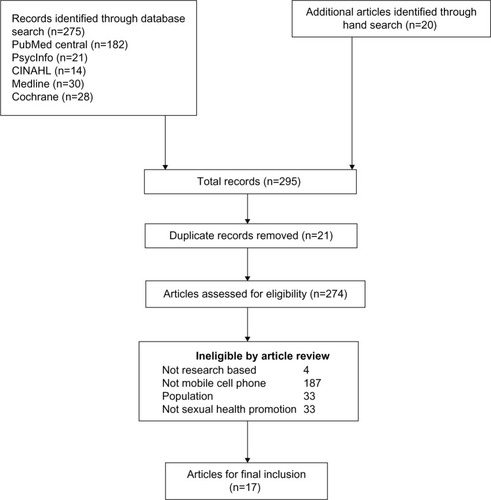
Table 1 Review of the literature
Results
Study designs
Ten of the 17 studies used quantitative methods. Four studies were longitudinal with repeated measuresCitation7–Citation10 and the other quantitative studies used descriptive or cross-sectional designs.Citation11–Citation14 One study was a randomized trial;Citation8 the others were a one-group pre-/posttest designCitation7 and a nonrandomized control group design.Citation9 Three studies used mixed methods,Citation15–Citation17 one was constructed in AfricaCitation18 and the others used qualitative designs, with interviews or focus groups.Citation19–Citation22 Intervention lengths varied from 4 weeksCitation16,Citation17 to 3 months.Citation7,Citation9,Citation10 Text messaging or mobile cell phone follow-up periods ranged from posttest,Citation16,Citation17 weekly,Citation7,Citation9 3 monthsCitation9,Citation11,Citation22 to 24 monthsCitation8; most studies were formative or pilot studies, and used validated measures to assess intervention outcomes. All studies used self-reported data with the exception of two; one used STI biomarkers in addition to self-reported dataCitation11 and the other used early pregnancy tests in addition to self-reported data.Citation8 Sample sizes varied from eleven to 1,738 participants. Four studies discussed theories used to guide development of the text messages/interventions.Citation10,Citation15,Citation16,Citation22 These theories included empowerment theory, social capital theory, theory of reasoned action, health belief model,Citation10,Citation22 youth asset developmental theory,Citation16 and ADAPT-ITT model.Citation15 The text-messaging dosage varied among interventions from one message per day,Citation7,Citation11 weekly,Citation20 three per weekCitation9,Citation10 to eleven per week.Citation17 Mobile cell phone counseling calls occurred once weekly.Citation8 Only one study discussed analysis of an HIV-prevention website enhanced for mobile cell phone text-messaging delivery.Citation23 Over a 14-month time period, the website had a total of 2,125 unique visitors from 61 different countries. Another study discussed data from a sexual health text message service designed for youth to determine the type of confidential questions asked by participants.Citation13
Delivery process
Several studies identified challenges involved in the development of text messages for mobile cell phone delivery. In one study, participants noted that some of the text-messaging abbreviations were not helpful.Citation15 Further, areas of inaccuracy and confusion were found. For example, one teen was unsure whether mosquitoes could transmit HIV even after the correct information was provided. Whenever teens got the answer wrong, they felt they should be able to text a facilitator to clarify why the response was wrong. In another study, participants felt that the initial text messages blamed or stigmatized the African-American community and recommended that messages be geared to the young black population.Citation22 Participants also noted that messages should be factual, respectful, and humorous. One suggested format was starting with humor, then finishing with a fact. Participants in one study found that a mobile phone application (app) was difficult to read and use, was not tailored to the intended population, and raised privacy issues.Citation17
Technical problems also presented challenges.Citation15,Citation17 In one study, the research team identified errors in the message delivery process as well as equipment problems, including failure of the short messaging service to send the message at the specified time, inability to receive text messages, and failure to respond to the messages as the result of a lost or damaged cell phone.Citation15 All of the problems were corrected, however. In the same study, problems in downloading videos or viewing URL links were found to be challenges. The researchers noted, however, that including a tech facilitator on the research team who could quickly correct problems reduced frustration and dropout rates.Citation15 In one study, the researchers found that they had to replace a participant’s phone, which had been stolen, and had to turn off two cell phones when teens went over their allocated minutes before the end of the month.Citation17 In another study, some teens lost or damaged their phones or were out of contact for an extended period of time resulting in considerable variability in participation rates.Citation8
The cost of delivering text-messaging interventions was also a challenge and in two studies, mobile cell phones were given to participants to offset costs.Citation15,Citation17 However, given current unlimited text-messaging plan, this is no longer a major barrier to adoption of text-messaging interventions. In the Teen Outreach Program, the buddy system was used. Teens with a mobile phone shared their phone or read the messages to a peer (their buddy) who did not have access to a mobile phone. This process did not work uniformly with some teens deleting messages before their buddy could read them.Citation16 In another study, the mobile phone incentive diminished as the low cost of prepaid cell phones became readily available and many of the teens purchased their own personal cell phone by the end of the study.Citation17
Lack of longitudinal studies
Only two of the studies reported outcomes beyond the 3-month follow-upCitation9,Citation10 and only one included 24-month follow-up.Citation8 Thus, only short-term effects of mobile cell phone interventions have been reported. Juzang et alCitation9 found significant changes in three key outcomes: higher condom use, increased sexual health awareness, and increased monogamy postintervention. In another study, HIV knowledge, attitudes toward condom use, and perceived HIV risk increased while HIV risk behaviors decreased at 3-month follow-up.Citation7
Privacy issues
In two studies, adolescents identified issues of privacy and lack of anonymity as possible challenges in delivering text messages/mobile cell phone interventions.Citation17,Citation21 In one study, no participants said that they would feel embarrassed if someone viewed their messages and 90% were unconcerned if their parents saw their messages.Citation21 However, they did say that privacy could be compromised, which could make a situation uncomfortable for a teen. In another study, privacy was a consideration with the use of a mobile cell phone safe sex app since participants felt that the research team could see what they were doing with the phones.Citation17
Need for tailored messages
In a follow-up to a mobile cell phone app study, Schnall et alCitation7 found that adolescents 13–18 years of age viewed the app as hard to understand and complicated to use, and thus felt that the app was not tailored to adolescents. This finding is consistent with the conclusion of Selkie et alCitation21 that sexual health resources must be written in clear, understandable language and tailored to adolescents. In addition, Wright et alCitation22 found that their adolescent participants wanted mobile cell phone text messages about STIs, including HIV/AIDS, to be factual and specific to them.
Credible information
Trust in the information and having someone qualified to respond to questions were found to be challenges in four studies.Citation9,Citation15–Citation17 Participants in one study felt that knowing a person was qualified to answer their questions was important in accessing information using mobile cell phones.Citation21 In another study, the participants unanimously agreed that they should be able to text questions to their facilitator.Citation15 In one study, trained staff members from the Adolescent Pregnancy Prevention Campaign provided medically accurate responses to text messages within 24 hours: typical responses occurred within 3–4 hours.Citation16 The cost of having a staff member to answer individual questions may be an issue for community-based agencies. Yet, youth want an immediate answer to a sexual health question that arises.Citation7,Citation21 Automatic standard responses may not always provide an appropriate response or one detailed enough to answer the question.
Impact of age on study outcomes
In one study, the way text messages were perceived varied depending on the age of the participants. Cornelius et alCitation7 found that age was a primary factor in change in outcome variables. They found greater increases in knowledge, attitudes toward condom use and perceived HIV risk, and more reduction in HIV risk behaviors among older participants (16–18 years of age) than younger participants (13–15 years of age). The reason why text messages did not resonant among younger participants was unclear. However, the younger participants did report less sexual activity than the older teens, which could explain why the messages did not resonate with them.
Adaptation to other countries: limited access
Adaptation of mobile cell phone-based interventions to other countries has presented challenges. One of the concerns with technology-based interventions is that we may not reach those who are at the highest risk, partly because of economics and access to services and technology. With low mobile cell phone ownership rates among adolescents in Uganda, only 51% of the participants in one study indicated that they were somewhat or extremely likely to access HIV/AIDS information via text.Citation18 Interest in accessing this information was associated with owning a cell phone. Thus, those at the highest risk may not be able to access cell phones because of the cost of the phone or text messages or data plans.
Use of health care providers
Only one study identified ways in which health care providers can use a text-messaging service to connect with youth. France examined how a school nurse used text messages to provide students access to her health promotion services.Citation12 The challenges with this approach involved administrative time and costs in managing and recording text messages. Advantages to the approach included the fact that it enhanced health services at the school and involved youth by empowering them to become knowledgeable about their sexual health. However, the approach was limited to students who owned or had access to a cell phone. Those without a cell phone did not have access to the services.
Discussion
Only 17 published articles were found that examined use of mobile cell technology and sexual health. The majority of the articles were descriptive studies that reported text messaging as the primary mode of sending or receiving sexual health information. Only four articles provided findings from a longitudinal study, and these findings were limited to 3–24 months. One study used a one-group design, one was a randomized trial, and one used a nonrandomized control group design.
Our review nonetheless suggests that mobile cell phone interventions are an effective mode for delivering safe sex and sexual health information to youth. However, while studies have demonstrated the potential of delivering sexual health information via mobile technology, there is still much to be learned about optimizing this intervention channel. More randomized controlled trials are needed to examine longitudinal effects and varying doses of text messages. Further, one studyCitation7 has identified possible differential effects of text messaging depending on age. The younger teens in this study also reported less sexual activity than the older teens, which may explain why the messages did not resonate with younger teens. Therefore, it is important to know the population for whom messages are developed: not all messages can be applied to everyone.
Teens want an immediate response to a text message. Automation may be appropriate in many situations, but there are times when a question or the response is not in the database or repository of a sexual health program. It is a challenge to provide real-time responses from staff, but this maybe the only way to be able to provide an answer to every question that may be texted to a sexual health program. Programs such as HookupCitation20 and BrdsNBzCitation13 have found success in providing text-automated responses to messages but data are limited on the long-term effectiveness of these programs.
There is a cost for delivering mobile cell phone messages or interventions. Participants and staff must have working equipment and unlimited text messaging and data plans. Those most at risk may not have cell phones and may not be able to access safe sex messages; therefore, alterative means for delivering safer sex messages must be found. Further, lost or damaged equipment remains a challenge and research staff may need to provide phones on loan to reduce dropout rates in studies.
Recommendations
Excessive use of text messaging affects adolescent social development negatively.Citation24 It would be interesting to do a longitudinal study to see whether text messaging drops off when social skills develop. Case scenarios could be developed to see how participants interact with others, measuring eye contact, word fillers, and body language against their text-messaging rates.Citation24
Currently, text messaging is an acceptable form of receiving sexual health information among adolescents, but in this review, we found no studies with follow-up beyond 24 months. Future studies should examine participant attrition, plans for improving retention, and message boosting to encourage maintenance of behavior change. In one studyCitation7 the researchers sent text-messaging boosters to augment a face-to-face intervention, and this enhanced effects. We must also begin to investigate other sources of sexual health communication. Currently, social media networks are being examined as potential sexual health information sources among adolescents. Platforms deploying multiple technologies may be particularly successful. For example, with a social media intervention that uses multiple sites, youth only need to log into one site. Given the long interval between mobile cell phone intervention development and dissemination, it is also important to assess not only the current user population but also potential future populations.
Sexual health interventions should go where the population goes. Real time interventions will have the greatest impact. As newer types of media become increasingly available and used by adolescents, it may be important to study different types of cell phone interactions and their associations with sensation seeking and impulsivity.
The lack of theory-based interventions found in this review may reflect the current focus on clinical care rather than on preventive health behavior change. However, interventions built on theory may have the greatest potential to change behavior and empower youth with the skills to practice abstinence or safe sex behaviors. Further, as technologies continue to develop, assessments should be performed prior to launching a program using new technology to ensure that the technology platform is still relevant to the target audience. New technology should augment, not replace existing resources.
Only one studyCitation23 reviewed here identified dissemination of a mobile safe sex information via a website. The website augmented information from an intervention and demonstrated one method of broad dissemination of safe sex information for adolescents. This website had a global impact, reaching unique users in 61 different countries. Future research should further examine the global impact of text-messaging interventions with participants in different countries.
More research is also needed to examine technology-based sexual communications among youth, since these have implications for adolescents’ safe sex decision-making. Timing, quality, length, and commitment of relationships should be examined with the mobile cell phone communication process. In addition, parent–child mobile cell phone-based interventions may improve adolescents’ safe sex decision-making since parents have been identified as a factor in the delay of their child’s sexual debut.
Further, we need to examine sexting behaviors across geographic regions by format (photo, text) and medium (cell phone, email, etc) and relationships to sexual activities. Future research should also examine parents’ perceptions of their child’s cell phone use and compare this with the child’s actual self-reported usage for sexual risks. Since sexting has been identified as a prelude to sexual intercourse, parents and health care providers should begin discussions of technology use with teens to identify possible sexual risks. Finally, research is needed to find out what youth do with the information that they use on text-generated sites (such as Hookup and SexInfo) and the extent in which the information is found helpful.
One strength of this review is the multiple strategy search process used. Further, the time frame was limited to the last 5 years, providing the most recent studies on this topic. The limitations of the review include the fact that many of the studies reviewed were pilot or exploratory studies with small purposive samples limiting generalizability of the findings. In addition, the review was limited by having only one article from Africa, where rates of HIV infection are the highest in the world.
Conclusion
This systematic review provides useful information on the impact of technology on the delivery of safe sex information to youth. Additional research is needed to identify the most effective approaches to using mobile cell phones as a vehicle for providing sexual health information to youth. There remain challenges, however, in the delivery of mobile cell phone safe sex interventions. One challenge is that young participants may not own a cell phone or have access to one. Another is that we do not know about the long-term effectiveness of mobile phone sexual health interventions. Further, messages must be tailored to the targeted population who need to be involved with the research planning from the ground up. Technical problems must be identified early and corrected as soon as possible to prevent attrition; this may require the constant presence of a technology specialist with the project. Finally, some text messages or data plans may incur a cost, which could be a barrier to implementation.
Disclosure
The authors report no conflicts of interest in this work.
References
- Centers for Disease Control and Prevention (CDC)CDC fact sheet: Incidence, prevalence of sexually transmitted diseases in the United States Published February 2013. Available from: http://www.cdc.gov/std/stats/sti-estimates-fact-sheet-feb-2013.pdfAccessed September 22, 2015
- Centers for Disease Control and Prevention2015Youth behavior surveillance survey Published May 15, 2015. Available from: http://www.cdc.gov/healthyyouth/data/yrbs/index.htmAccessed September 22, 2015
- Pew Research CenterTeens and technology 2013 Published March 13, 2013. Available from: http://www.pewinternet.org/files/old-media/Files/Reports/2013/PIP_TeensandTechnology2013.pdfAccessed September 22, 2015
- National Institutes of HealthFrequently asked questions Published March 17, 1999. Available from: http://grants.nih.gov/grants/funding/children/pol_children_qa.htmAccessed September 22, 2015
- World Health OrganizationAdolescent health Published 2015. Available from: http://www.who.int/topics/adolescent_health/en/Accessed September 22, 2015
- MilesMHubermanAQualitative Data Analysis2nd edThousand Oaks CASage1994
- CorneliusJBDmochowskiJBoyerCLawrenceJSStLightfootMMooreMText messaging enhanced HIV interventions for African American adolescents: a feasibility studyJ Assoc Nurses AIDS Care201224325636723122907
- KatzKSRodanMMilliganRTanSCourtneyL2011Efficacy of a randomized cell phone-based counseling intervention in postponing subsequent pregnancy among teen mothersMatern Child Health J15Suppl 1S42S5321809218
- JuzangIFortuneTBlackSWrightEBullSA pilot programme using mobile phones for HIV preventionJ Telemed Telecare201117315015321270049
- FortuneTWrightEJuzangIBullSRecruitment, enrollment, and retention of young black men for HIV prevention research: experiences from the 411 for Safe Text ProjectContem Clin Trials201031151156
- BuhiERKlinkenbergerNHughesSBluntHDRietmeijerCTeens’ use of digital technologies and preferences for receiving STD prevention and sexual health promotion messages: implications for the next generation of intervention initiativesSex Trans Dis20134015254
- FranceJUsing texts to increase access to school nursesNurs Times201411013181924757937
- WilloughbyJFJacksonKCan you get pregnant when u r in the pool? Young people’s information seeking from a sexual health text lineSex Ed201313196106
- WhiteleyLBBrownLKSwensonAfrican American adolescents and new media: associations with HIV/STI risk behavior and psychosocial variablesEthn Dis201121221622221749027
- CorneliusJBCatoMLawrenceJSStBoyerCBLightfootMDevelopment and pretesting multimedia HIV-prevention text messages for mobile cell phone deliveryJ Assoc Nurs AIDS Care2011225407413
- DevineSBullSDreisbachSShlayJEnhancing a teen pregnancy prevention program with text messaging: Engaging minority youth to develop TOP® Plus TextJ Adolesc Health2014543S78S8324560081
- SchnallROkoniewskiATiaseVLowARodriguezMKaplanSUsing text messaging to assess adolescents’ health information needs: an ecological momentary assessmentJ Med Internet Res2013153116
- MitchellKJBullSKiwanukaJYbarraMLCell phone usage among adolescents in Uganda: acceptability for relaying health informationHealth Educ Res201126577078121536715
- CorneliusJBLawrenceJSStHowardJCAdolescents’ perceptions of a mobile cell phone text messaging-enhanced intervention and development of a mobile cell phone-based HIV prevention interventionJ Spec Pediatr Nurs201217616922188273
- PerryRCKayekjianKCBraunRACantuMSheoranBChungPJAdolescents’ perspectives on the use of a text messaging service for preventive sexual health promotionJ Adolesc Health201251322022522921131
- SelkieEMBensonMMorenoMAdolescents’ views regarding uses of social networking websites and text messaging for adolescent sexual health educationAm J Health Educ201142420521222229150
- WrightEFortuneTJuzangIBullSText messaging for HIV prevention with young Black men: formative research and campaign developmentAIDS Care201123553454121287416
- CorneliusJBCatoMGTothJLBardPMMooreMWWhiteAFollowing the trail of an HIV-prevention web site enhanced for mobile cell phone text messaging deliveryJ Assoc Nurses AIDS Care201223325525921550826
- LaBodeVText messaging: one step forward for phone companies, one leap backward for adolescenceInt J Adolesc Med Health2011231657121721366