
Abstract
Background
Interprofessional education is considered as one of the approaches in educating learners in the health system that increases interprofessional collaboration and improves the quality of patient care.
Purpose
This study sought to design an interprofessional continuing education model.
Methods
This study was conducted in three stages. In the first stage, a systematic review of literature and search of databases were conducted to identify the common models of interprofessional continuing education and to extract the elements used in these models. In the second stage, specialists in interprofessional continuing education were interviewed in relation to the features of elements derived from the first stage. In the third stage, the model of interprofessional continuing education was designed using the results of the first and second stages.
Results
Seven models were obtained. Five themes, including the subject of interprofessional continuing education, objectives, content, learning strategy, and evaluation strategies, were extracted from them. Specialists stated interprofessional collaboration, needs of community and learners, focus on patient, using interactive teaching methods, and feedback as the main features of these five themes.
Conclusion
The results of this study showed that providing a framework and model regulated in interprofessional continuing education programs can help design these programs.
Introduction
According to the World Health Organization (WHO’s) definition, interprofessional education is the method in which two or more groups of students or learners of different professionals of health system are trained to provide health services, prevention, treatment, rehabilitation, disease improvement, and promotion of health with the important objective of creating an interaction and participation among them in a specific period and place.Citation1–Citation4 An interprofessional team is composed of professionals in various health sciences who have knowledge, attitudes, skills and special capabilities in the form of a team with a common objective based on clients’ needs and their specialties are applied for patient’s objectives in an effective and constructive relationship.Citation5 Specialization of health care and increasing advancement in its technology add to the complexities of health services delivery more than ever and make provision of safe and favorable treatment based on community depending on the participation of members of various medical professions in interprofessional teams. The fact is that members of these teams are rarely trained. In addition, they come from various disciplines and have different educational programs and, in principle, are less able to work in teams.Citation6–Citation8 Teamwork is very important for patient safety. Particularly when the members of a team know their responsibilities well, they make fewer mistakes than others. In so doing, they need to be trained together to understand their role in the team. It seems that the solution to this problem is interprofessional education.Citation9
Currently, continuing education programs are planned based on professional needs. Research has shown that continuing education programs that are tailored to a particular profession cannot empower provider with the challenges they face in the workplace.Citation10,Citation11 Therefore, there is a weak evidence of effective strategies such as teamwork in solving the challenges of treatment in the country.Citation12 In the context of interprofessional education programs in Iran, research on interprofessional education has expanded; however, it has not so far reached the level of application at the university level and educational centers.Citation13 In this regard, interprofessional executive model in health sciences was designed at the university level according to the available contexts in the educational system of Iran in 2014 by Vafadar et al. This model provides an appropriate framework for the development of morality and the evolution of human and professional identities among the health system’s students to provide a basis for patients.Citation14 Irajpour examined the status of medical education in the country in terms of preparation for interprofessional education, cooperative learning, and the required capacities.Citation12 The results of the study highlighted the favorable conditions and readiness for the development of interprofessional education programs in medical education of the country.Citation12 However, in recent years, the attitude and readiness of students in the country’s medical education have been investigated in the field of development of interprofessional education using Readiness for Interprofessional Learning Scale (RIPLS).Citation15,Citation16 The results indicated the positive attitude of the majority of medical students toward the necessity to use this educational approach and its outcomes for improving the provision of health services to clients and promoting the quality of interactions among staff in the health system.Citation17–Citation19
Despite few decades of the emergence and growth of interprofessional education in the field of health, this approach is still unknown for many professors and educational planners due to inadequate knowledge and poor evidence. Currently, interprofessional education research is increasing in Iran’s educational system.Citation20 In 2011, Yamani et al developed a diabetic patient care program based on interprofessional education. Thirty-four doctors and nurses received the necessary training through a 3-day workshop. The questionnaire was used to evaluate the Team Climate Inventory Questionnaire and Diabetes Questionnaire, which were administered pre- and posttest. The findings of the study assessed the quality of care provided for diabetics and improved knowledge and practice of learners positively.Citation21
An interprofessional education post-registration model was designed by Ontario in 2009. This model was programmed in three stages: getting started; gaining mastery and continuous mastery at each stage; and teaching, learning, and evaluation of methods to assess the learners.Citation22 Designing and evaluating a new model of interprofessional education were done with an emphasis on the use of asthma drugs in 2014 by Bosnic-Anticevich. In this study, three models of continuing education including face-to-face education, e-learning, and a new interprofessional education model were implemented.Citation23 In order to develop interprofessional education and improve continuing education of the health community, it is necessary to provide a suitable model for the country’s cultural and educational context and its implementation to achieve the abovementioned objectives. Using an implementation model will pave the way for achieving these goals. To this end, this study sought to design an interprofessional continuing education model.
Methods
This study was conducted in three stages. In the first stage, the systematic review of literature was done to identify models common in interprofessional education and to identify the constituent elements in each model.
First, the search for literature was started with the keyword of interprofessional continuing education. Other words were used to combine with the original word using “AND” and “OR”. These terms included interprofessional education models, interprofessional continuing education models, interprofessional education postgraduation models, and interprofessional education post-licensure models.
Advanced search was done based on title, summary, and keywords in English in years from 1990 to 2015. The results were simultaneously transferred to EndNote software. Given the accessibility to different databases and the coverage of the available studies in this field, the search was conducted in several specialized databases of health science studies including Science Direct, PubMed, Eric, Cochrane Library, Ovid, and Google Scholar. Search strategy is shown in . The titles and abstracts of the obtained articles were examined in relation to the research question. Then, the irrelevant articles were excluded based on the inclusion and exclusion criteria, and the relevant articles were entered into the qualitative assessment process. Based on the components derived from these articles, the features of this component were explained by experts.
Table 1 Search strategy
The following criteria were used to identify papers of interprofessional education models post-registration in order to develop the detailed case studies:
All case studies should be considered examples of models interprofessional education post-registration or continuing interprofessional education
All participants are health professionals
The purpose of continuing interprofessional educations is expressed
Articles that were editorial report, bulletin, commentary, book review, and introductory report and articles whose purpose was not specified and the attendees were not health professionals were excluded from the study.
In the second stage, interviews with experts in continuing education and interprofessional education were conducted. Before the interview, e-mails were sent to the experts, and written informed consent and the time of the interview were obtained. Ethical approval was granted by Isfahan University of Medical Sciences. Since the adaptation of the interprofessional education model to health education is an important part of modeling design, the study of the sociocultural and social context of educational approaches to health science and, in particular, recognition of the experiences of continuing education officials are of particular importance in designing the model. At this stage, based on the components derived from these papers, the characteristics that these components have to offer in interprofessional training are explained by specialists through semi-structured interviews. Considering that the patterns of continuing interprofessional education patterns are the most basic part of the model. In order to analyze the articles, first, the article’s description on executive search methodology was reviewed repeatedly to obtain a general understanding of the subject. The text was read by line. Then, by repeated and frequent comparisons between them, the codes that were the most frequent in the texts were explained and combined, and descriptive themes were identified.
In the third stage, the interprofessional continuing education model was designed. The draft of this model was presented to a group of interprofessional education experts, and the applied model was finalized based on the results of their comments and corrective suggestions.
Results
Seven models were obtained from the findings of the first stage in interprofessional continuing education ().Citation22–Citation24,Citation25–Citation28 These models were studied repeatedly, and five constructs were extracted out of them.
Table 2 Continuing interprofessional education models
Subject
The first structure that came from interprofessional education models was the subject of interprofessional education, which included articles on health, hygiene, care, treatment, and education. From the point of view of specialists, the title or subject of interprofessional education should have the features of interprofessional collaboration, teamwork, and patient centeredness. According to the theory of adult education, the subject of continuing education and interprofessional education programs should be the needs of the learners and should be achieved through the needs assessment of learners to be effective on the attitude and knowledge of learners.
Objectives
The second construct obtained from the models is the goals of interprofessional education. The studies identified the objectives of interprofessional education programs, interprofessional communication, recognition of the role and responsibilities of other professionals in the team, and mutual respect in the team. Professionals outlined the characteristics of interprofessional education goals such as relevance to continuing education, practice, participating professions, and audiences. The objectives should also be based on the need of the learner, patient, professions, and community.
Content
Professional commonalities should be considered in the formulation of the content. Professors of the professions involved in the program should participate in content development. It should be learner-based, profession-based, and patient-based care and cover all educational goals. Adult education should be problem centered and function oriented, rather than content centered.
Learning strategies
The interactive-based, learner-based, and problem-based learning methods (seminars, workshops, group discussions) are among the most widely used ones in studies. From the experts’ point of view, teaching methods should be learner based, create learning synergy, share experiences, and be implemented in formative-summative method.
Evaluation strategies
Evaluation is one of the most difficult and complex parts of interprofessional education model. The patient is the center of the professional system, and the health outcomes will be affected by the performance of the interprofessional team, whereas the learner is the center of the educational system, whose consequences are affected by the educational process.
In the articles reviewed, the most important instruments used in evaluation were knowledge, attitude, and practice questionnaires, RIPLS questionnaire, interviews with experts, and feedback from families and patients. Experts said that evaluation should be based on goals. It should also be based on evidence-based and patient-center.
Development of continuing interprofessional education model
From the findings of the first and second stages, the continuing interprofessional education model was developed in three stages: design, implementation, and evaluation ().
Figure 1 The model designed for continuing interprofessional education.
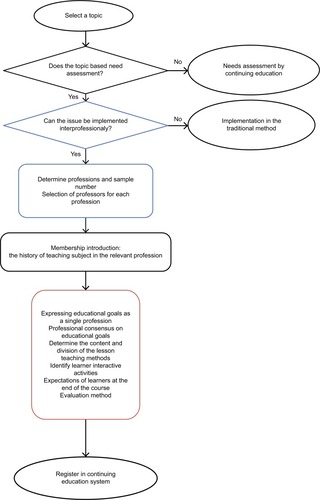
At the design stage, first, the needs assessment is done by the Continuing Education Center, and the subject of the program is selected based on the needs assessment. Then a panel of experts is formed on whether the selected topic has the ability to run interprofessional education. If it cannot be implemented using an interprofessional approach, it will be implemented in a traditional method. If it can be implemented using an interprofessional approach, it will be selected in the same panel of participating professionals and professors.
In the second session of the panel, the professors of each profession are introduced and then the common learning objectives among the professions, the common content, teaching methods, interactive activities, and assessment of the learners are identified.
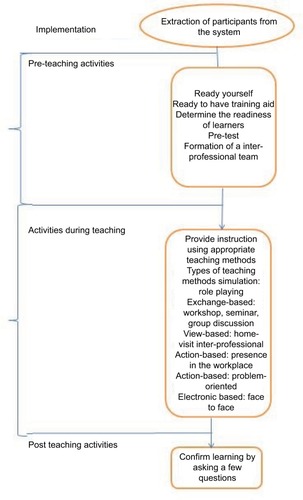
The implementation phase is divided into three sections: pre-teaching activities, while-teaching activities, and post-teaching activities.
At the stage of pre-teaching activities, the characteristics of learners and their readiness for implementation of interprofessional education are determined using the RIPLS questionnaire. Also, a pretest related to the curriculum is implemented.
At the stage of teaching activities, learning methods that suit the interprofessional training are used. During the post-teaching activities, the materials are collected, and the learning is fixed through questions and answers.
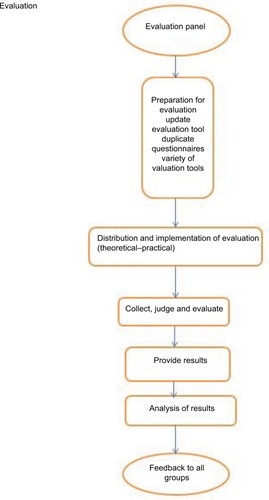
Evaluation stage
At this stage, questionnaires and other evaluation tools are kept ready. The determined evaluation methods appropriate to the program and objectives are used. The results are collected, judged, and analyzed. At the end of the report, the results are presented, and the feedback is given to all groups.
Discussion
The results of this study showed that providing a framework and model for continuing interprofessional education programs can help design these programs.
The basis of this design was the implementation of continuing education programs based on the interprofessional training. The characteristic of this model, which distinguishes it from other patterns, is the step-by-step explanation of the implementation of the interprofessional continuing education program.
The designed model in Ontario has been developed in three stages of the start-up phase, the stage of excellence and continuous mastery, and emphasized the learning and evaluation methods in three stages. In other articles, the interprofessional training program has not been designed and implemented on the basis of interactions between the professions. The model we have designed is also applicable to all educational systems in other countries, and its implementation stages are clear. There are resistances to implementing interprofessional training programs. Planning and coordinating the implementation of these programs is hard. The differences in the culture of every individual and conflicts of interest are the basis of these resistances.
The lack of formal and academic experience in interprofessional continuing education and the lack of familiarity with respect to interprofessional training among the continuing education officials were the limitations of this paper.
Conclusion
The most important feature of this template is the transparency of the steps and step-by-step description in three stages of design implementation and evaluation. It is suggested that interprofessional training programs should be conducted not solely for theoretical training but should also be implemented in the clinical setting according to this model.
Acknowledgments
This study is supported by the Department of Medical Education, Medical Education Research Center at Isfahan University of Medical Sciences, as part of a thesis.
Disclosure
The authors report no conflicts of interest in this work.
References
- GilbertJHYanJHoffmanSJA WHO report: framework for action on interprofessional education and collaborative practiceJ Allied Health201039Suppl 119619721174039
- WHOInterprofessional education case studyHuman Resources for Health Observer2014
- BakerPGFramework for Action on Interprofessional Education and Collaborative PracticeGeneva, Switzerland2010
- IrajporAAlaviMSetting up a virtual network of cooperation between education and professional developmentIJME201313119991000
- BarrHInterprofessional Education: Yesterday, Today and TomorrowHigher Education Academy, LTSN Health Sciences and Practice Subject Centre. CAIPE2002
- IrajpourAAlaviMIzadikhahASituation analysis and designing an interprofessional curriculum for palliative care of the cancer patientsIJME2015141210471056
- YanJGilbertJHoffmanSWHO Study Group on interprofessional education and collaborative practiceJ Interprof Care2007216587589
- YildirimADomacSInterprofessional Education Model for the Health and Life Science Faculties
- LapkinSLevett-JonesTGilliganCA systematic review of the effectiveness of interprofessional education in health professional programsNurse Educ Today20133329010222196075
- MasoomiRYamaniNA review on interprofessional education in health professionals’ trainingIJME201211912311240
- ThistlethwaiteJEInterprofessional education: implications and development for medical educationEducación Médica20151616873
- IrajpourAInter-professional education: a reflection on education of health disciplinesIJME2011104452463
- VafadarZVanakiZEbadiAInter-professional education: the necessity for ethical growth in health domainJ Med Educ Dev2014931834
- VafadarZVanakiZdesign a practical interprofessional education model in the health sciences [doctoral thesis]2015
- ReidRBruceDAllstaffKMcLernonDValidating the Readiness for Interprofessional Learning Scale (RIPLS) in the postgraduate context: are health care professionals ready for IPL?Med Educ200640541542216635120
- AminiBBigdeliSShiraziMMirshahvaladSMValidity and reliability of the “Readiness for Interprofessional Learning Scale (RIPLS)” in Iranian contextJ Payavard Salamat20161015158
- IrajpourAAlaviMReadiness of postgraduate students of Isfahan University of Medical Sciences for inter professional learningIJME201211910501056
- VafadarZVanakiZEbadiAThe readiness of postgraduate health sciences students for interprofessional education in IranGlob J Health Sci20157419025946930
- DalooeiRJMoonaghiHKYamaniNIrajpoorARSaadatyarFSInterprofessional education: the strategy to improve health careRes Med Educ2015715462
- VafadarZVanakiZEbadiAInterprofessional education; a response to health system challengesIJME2014142148164
- YamaniNAsgarimoqadamMHaghaniFAlavijehAQThe effect of interprofessional education on interprofessional performance and diabetes care knowledge of health care teams at the level one of health service providingAdv Biomed Res2014315325221756
- MedvesJSaxe-BraithwaiteMAylwardDInterprofessional Education Curricula Models for Health Care Providers in Ontario2009
- Bosnic-AnticevichSZStuartMMacksonJDevelopment and evaluation of an innovative model of interprofessional education focused on asthma medication useBMC Med Educ20141417224708800
- BonwellPBParsonsPLBestAMHiseSAn interprofessional educational approach to oral health care in the geriatric populationGerontol Geriatr Educ201435218219924131421
- LundonKShupakRReevesSSchneiderRMcIlroyJHThe Advanced Clinician Practitioner in Arthritis Care program: an interprofessional model for transfer of knowledge for advanced practice practitionersJ Interprof Care200923219820019085269
- TonerJAFergusonKDSokalRDContinuing interprofessional education in geriatrics and gerontology in medically underserved areasJ Contin Educ Health Profs2009293157160
- GoodingHCZinielSTouloumtzisCCase-based teaching for interprofessional postgraduate trainees in adolescent healthJ Adolesc Health201658556757227107910
- VillarrealDRestrepoMIHealyJA model for increasing palliative care in the intensive care unit: enhancing interprofessional consultation rates and communicationJ Pain Symptom Manage201142567667922045372