
Abstract
Reverse mentoring is a relatively contemporary concept that relies on the reversal of the traditional roles of mentor and mentee and the abolition of the mentorship model as an apprenticeship or hierarchy. Typically, a younger specialist takes on the role of mentor and an older, more experienced specialist the role of mentee. Reverse mentoring is founded in learning and social theories of mentorship and has been practically applied in information technology, business and education fields. However, there is a role for reverse mentoring in medical education and the health sciences, particularly with the inclusion of new technologies in a changing health landscape, and the emphasis on interdisciplinary teamwork and improved workplace culture. Further investigation and analysis of reverse mentoring is warranted, with a particular focus on the implementation of the reverse mentor model in the field of medical education and the health sciences. To assist those considering implementation of mentorship programs in their workplace, this article provides an overview of recent literature, with suggested applications of “reverse mentoring” in the medical education context.
Introduction
The term “mentorship” is derived from ancient times, first mentioned in Homer’s “Odyssey”. When the King of Ithaca, Odysseus, went to fight in the Trojan War, he entrusted the care of his kingdom and family to Mentor.Citation1 Mentor provided guidance, counsel and support to Telemachus, Odysseus’ son. Although mentorship is a concept that has long existed, it has only recently been formalized as playing a role crucial to both personal and professional development in medical education.Citation2 A variety of definitions of mentorship exist, reflecting the varied contexts in which mentoring is utilized. It is generally accepted, however, that mentorship relies on 1) reciprocity of the mentee–mentor relationship, 2) developmental benefits for the mentee’s career or work, and the mentor’s learning partnership and 3) consistent communication between the mentor and mentee.Citation3
Traditionally, mentorship is considered a process where the mentor, an experienced person, guides the mentee in developing the knowledge and skills required in their professional development. This core concept of mentoring is applicable to a diversity of organizational contexts. Numerous styles of mentoring exist and extend from the classical model to cascading mentoring, group mentoring, network mentoring, spot mentoring and virtual mentoring.Citation1,Citation4 Most workplaces use traditional models of mentoring aimed at facilitating learning and development of the mentee.Citation5 With the advent of information technology (IT), followed by the engagement of millennials in the workplace, however, the potential in cross-generational mentorship is increasingly being recognized. This paper provides an overview of the recent literature to assist those considering implementation of mentoring programs in their workplace. In particular, we provide a focus on the new mentoring style of “reverse mentoring” and consider this in the context of medical education.
Reverse mentoring
Reverse mentoring relies on the reversal of the traditional roles of mentor and mentee and the abolition of the mentorship model as an apprenticeship or hierarchy.Citation4 Ziegler expands the definition of reverse mentoring, outlining the “reciprocal and temporally stable relationship between a less experienced mentor providing specific expert knowledge and a more experienced mentee who wants to gain this knowledge”.Citation5 The mentor fulfills the traditional role of advice-giver, providing new insight regarding ideas or concepts to the mentee.Citation6 Crucially, as outlined by Zauchner-Studnicka, reverse mentoring “aims at both the development of the mentors and the mentees”.Citation4
There are unique characteristics of the reverse mentoring relationship.Citation7 First, the partner status of both parties is different from conventional mentoring roles; a more junior specialist takes on the role of mentor and a generally older, more experienced specialist the role of mentee.Citation7 The mentor provides advice to the mentee, and the mentee gives the mentor a new insight to stimulate growth and reflection in the mentor.Citation6 Importantly, the reverse mentoring relationship is characterized by a commitment to a shared goal of mutual learning and collaboration.Citation6 The exchange of knowledge shifts away from the traditional longitudinal mentoring relationship to a focus on learning from the mentor’s specific technical or content expertise.Citation7 This final characteristic of reverse mentoring reflects its origins in learning and social theories of mentorship. The typical characteristics and benefits of reverse mentoring are summarized in .
Box 1 Typical characteristics and benefits of reverse mentoring
Theoretical underpinnings of reverse mentoring
Mentorship occurs as part of different theoretical frameworks that help guide the way it is developed and implemented. As outlined by Dominguez and Hager, traditional concepts of mentoring arise from three primary theoretical frameworks: developmental, learning and social theories.Citation8 Reverse mentoring, as a classical form of mentoring, arises more from social and learning theories of mentorship than developmental theory.Citation4,Citation8
Developmental theory
Developmental theories of mentorship reflect an inherent hierarchic relationship between mentee and mentor within succeeding phases of an individual’s development.Citation4,Citation9 The mentor provides practical support during a mentee’s developmental transitions with effective mentoring relying on matching of academic and occupational strategies. The value is predominantly in the mentee’s personal growth. Examples of the application of developmental theory include peer-to-peer student mentoringCitation10 and junior-senior faculty mentoring relationships.Citation11
Learning theory
There are a multitude of learning theories relating to mentorship. The concept of mentorship as a learning partnership is a common foundation for adult learning (andragogy), behaviorist, cognitivist and constructivist theories as well as transformative, action and social learning theories. Within learning theories of mentorship, the mentor becomes a facilitator for a mentee’s personal progress.Citation12 Andragogy theory emphasizes the facilitator role of the mentor, where both the mentor and mentee engage in a mutual learning process through self-reflection and critical discussion of past experiences and social roles.Citation13 Similarly, transformative learning theory advocates for active discussion and critical thinking between mentor and mentee to change perspectives on work and identity.Citation14 The process of mutual development is also seen in social learning theory, which focuses on the process of learning through imitation. Taken together, learning theories of mentorship emphasize the role of the mentee as an active co-constructor of development.Citation8 The basis of reverse mentoring therefore arises from the notion of an involved and contributory mentee.
Social theory
Social theories of mentorship shift the focus from dyadic relationships to a networking perspective with mutual benefits. Social theories of mentorship include socialization, human/social capital, social exchange and social network theories, as well as communities of practice.Citation8 Within these theories, the mentee is an active contributor to the mentor relationship. In particular, social exchange theory and communities of practice emphasize the importance of information and knowledge exchange within the relationship. Social exchange theory suggests that a successful mentorship relationship arises when there is a clear cost-benefit to both parties, based on the possession of valued characteristics.Citation15 The concept of communities of practice regards mentorship as a knowledge network where mentoring is more a partnership than apprenticeship.Citation16 Mentees enter multiple communities with their own set of skills and knowledge, which allow them to contribute as a mentor in one field and learn as a novice in another.Citation17 Within the educational field, students can bring up-to-date knowledge to the community,Citation18 while senior colleagues provide traditional guidance with respect to community roles.Citation19 The construction of mentorship in this way reflects the core foundation of reverse mentoring.
Practical applications of reverse mentoring
The origins of reverse mentoring lie in business and IT sectors and reflect the need for employees to stay current in the workplace.Citation20 It is particularly utilized in the IT industry where younger generations can advise on the latest in technological advancements.Citation21 Reverse mentoring is not limited, however, to fields of IT or business. There are examples of the concept in education,Citation6 economic theories, language skills and innovative ideas.Citation22 It has become “best practice” for several large corporations including Dell,Citation23 Procter and GambleCitation24 and Time Warner.Citation25 It can be particularly useful in workplaces that are frequently exposed to the rapid transformation of technology, including social media, such as the public relations industry.Citation26
Differences within these contextual arrangements relate to the formulation of the mentor–mentee relationship. In the IT industry, the younger specialist (mentor) provides his or her experience with a new technology to the older mentee, in line with the mission of traditional mentoring relationships. Reverse mentoring in education is less strictly defined and relies more on a duality of roles; learning is a two-way street or “boomerang”.Citation6 Reverse mentoring in education is therefore not limited to a younger–older interaction.Citation27 With a focus on specific, content-driven relationships it is important to recognize that reverse mentoring is differentiated from the scenario where a specialist approaches a more junior colleague for assistance with a single issue. There is an established relationship characterized by the mutual exchange of knowledge that continues beyond the static episode. provides examples of features that differentiate reverse mentoring from traditional mentoring.
Table 1 Examples of features that differentiate reverse mentoring from traditional mentoring
There is a lack of research in the field of health sciences, including academic medicine, relating to reverse mentoring. The benefits of traditional mentoring for mentors have been reported previously.Citation2,Citation28 A pilot study by Cotugna and Vickery outlined the benefits of reverse mentoring amongst dietitian students assigned older professionals with limited experience in accessing the internet.Citation29 There is a strong argument for further empiric research in the field of reverse mentoring within the health sciences. Like education, clinical and academic fields of the health sciences are less clearly defined by a younger–older dynamic. However, in traditional forms of mentoring, it is suggested that for both academic and clinical mentoring relationships, the mentor should be one career stage above a mentee in order to provide the mentee with appropriate research and professional guidance.Citation30
Attributes and behaviors of the mentee and mentor in reverse mentoring
The unique structure and purpose of the reverse mentoring relationship require a re-evaluation of the attributes and behaviors required by the mentee and mentor. and below outline the qualities required for successful reverse mentorship.
Table 2 Attributes and behaviors of effective mentors in reverse mentoring
Table 3 Attributes and behaviors of effective mentees in reverse mentoring
Is there a role for reverse mentoring in medicine and health education?
The concept of reverse mentoring is particularly relevant within medical education and the health sciences. For example, the flipped classroom and social media for learning are growing within medical education.Citation31 The key to enhancing student engagement may be in learning from millennials and gaining skills from early career staff. In particular, the advent of new technologies, including e-learning modules, apps, podcasts and online forums, and electronic databases places more junior colleagues at the forefront of an advancing healthcare landscape. Traditional pillars of healthcare are being re-written with the inclusion of new technologies that change the understanding of information exchange as well as core concepts of privacy. For example, the transition to online health records highlights the need for more experienced specialists to be up to date with new technologies in order to access patient information, prescribe medications and communicate with other clinicians. Less experienced clinicians have a role to play in teaching understanding of these technological developments.
The role of early career clinicians in the reverse mentoring relationship is not limited to the field of technology, however. As outlined by Robinson, junior health professionals can help to drive a workplace culture where “concerns can be raised and learning thrives”.Citation32 Trainees and junior health professionals can provide new perspectives on issues such as clinician health and well-being and exemplify a non-discriminatory approach to patients. In this way, reverse mentoring can assist with the breakdown of the traditionally regimented and hierarchical structure of medicine.Citation33 In particular, reverse mentoring between senior clinicians and more junior staff from ethnic minority backgrounds can aid in the breakdown of cultural biases and stereotypes, improving diversity.Citation32 At a societal level, early career staff can enter debate and provide insight into the changing role of healthcare within communities.
Additionally, there is a current emphasis on interdisciplinary teamwork. With increasingly complex healthcare systems, members of the health service delivery team need to collaborate more closely with each other to improve patient safety.Citation34 Reverse mentoring has the potential to provide a useful means to learn about aspects of others’ professions without placing an additional burden on senior clinical staff. Early career staff (resident medical officers, junior physiotherapists, speech therapists, pharmacists and dentists) can provide relevant insights into the organizational structure and learning models of their particular fields and the knowledge, skills and values that are held within their professions. Within medical education, staff usually work across multiple institutions, including hospitals, research centers and universities – here, reverse mentoring affords the opportunity for early career staff, who may have more time, to provide unique insights into other domains.
Reverse mentoring in medical education may also be useful in career transitions across these domains. For example, senior clinicians, who are experts in their medical field, may move into teaching and research roles within medical education. The millennials already working in medical education may provide a closer connection to current trends in the field, have more time, and have a greater enthusiasm than the more experienced medical educationalists. In some regards, reverse mentorship emphasizes the need for continual professional development, where one identifies the gaps in their own knowledge, and seeks to improve specific knowledge and skills.
Introducing reverse mentoring in medical education
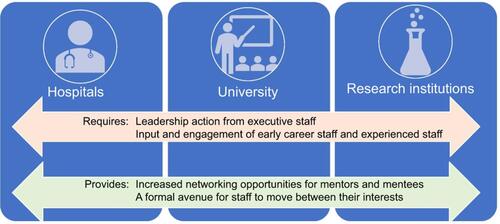
The authors (a neurology advanced trainee (AC), two educationalists (AB and CVD) and a pediatric respiratory consultant (CM) all experienced in working across the university and hospital sectors) posit that given the increased use of IT in medical education, there is a place for reverse mentoring in medical education and the health sciences. Often there is a lack of formal relationship between hospital, university and research institutions. Engagement in a reverse mentoring program provides a formal avenue for staff to move between their interests. The development of such a program requires communication and cooperation between senior leaders of all institutions, as well as leadership and input from early career staff to establish a program that functions across institutions, as outlined in .
Figure 1 Flowchart illustrating the activities and input required for a reverse mentorship program.
Benefits of reverse mentoring
The benefits of mentorship are widespread and have been evaluated specifically in the field of health sciences.Citation35 In particular, mentorship is linked to significant mentee benefits, including facilitating specialty choice, career advancement,Citation36 as well as productivity.Citation37 The presence of a mentor is associated with higher reports of career satisfaction.Citation38 Mentoring, in its traditional sense, also holds benefits for the mentor. Through discussion and collaboration, mentors are given the opportunity to share their wisdom and experience, leading to a sense of personal fulfillment and a renewed sense of awareness of their own professional skills and workplace practices.Citation2 Similarly, a reverse mentoring relationship holds benefits for both parties.
Benefits for mentors
For a less experienced employee in the role of mentor, the benefits relate predominantly to the development of professional skills, improved organizational culture through the opening of communication lines, and enhanced clinical and academic opportunities due to the exchange of new knowledge. The opportunity to work closely with a more experienced colleague facilitates the development of skills necessary to be a good mentor.Citation30 The mentor can develop his or her professional skills in tandem with the provision of a new set of ideas or knowledge to the mentee. The exchange of ideas can aid in the development of cross-generational leadership, important in a changing healthcare landscape.Citation39 Thus, a portion of the knowledge sharing provided by mentees fulfills the traditional concept of mentorship.Citation7 Indeed, Lee et al propose that mentees have an obligation to “return on investment”.Citation30 In the case of reverse mentoring, the return on investment includes the sharing of experience and “role modeling”Citation40 the professional skills necessary for the development of less experienced colleagues. For example, within medicine, role modeling by clinicians plays a key role in shaping trainees’ and students’ professional competencies, values and attitudes.Citation41 In the reverse mentorship relationship, clinical skills and knowledge, teaching skills and personal qualities are areas that may be exhibited by the more experienced mentee, and emulated by the less experienced mentor.
For less experienced mentors, the opportunity to engage in a relationship that is more partnership than apprenticeship facilitates open communication. In the traditionally hierarchical field of health sciences, discussion and exchange of ideas can contribute to a mentor’s feeling of empowerment and job satisfaction. Previous studies in traditional mentorship in clinical medicine describe junior employees being afraid to approach a senior colleague about mentorship.Citation36 The abrogation of traditional learner-teacher models can facilitate an improved organizational culture and workplace.Citation7 The mentor may feel more like a peer than a junior colleague, an important motivator for millennial employees.Citation42 Carrying this forward, reverse mentoring can extend mentors social capital, improving access to the resources of others.Citation43
The engagement of reverse mentors may guide research selection and involvement in new directions. In traditional mentoring relationships, the mentor acts as a “sponsor” for the mentee.Citation40 As a sponsor, the mentor gives and shares opportunities in research and provides constructive critique to guide maturity in the research product.Citation44 In contrast, reverse mentors, armed with new knowledge at the forefront of innovation, may play a more partisan role in the development of ideas.Citation7 In turn, this can drive a more collaborative and productive mentoring relationship in the field of education and research. summarizes the potential benefits for mentors in reverse mentoring.
Table 4 Potential benefits for mentors in reverse mentoring
Table 5 Potential benefits for mentees in reverse mentoring
Benefits for mentees
The more experienced mentee in a reverse mentoring relationship stands to gain benefits, predominantly an exposure to the newest content or technical skills, as well as an enhancement of existing leadership skillsCitation7 and renewed enthusiasm.Citation40
It has long been accepted that mentoring is a “two-way street”.Citation2,Citation40,Citation47 A more experienced mentee stands to gain tangible benefits from a successful reverse mentorship. These include improved research outputCitation40 and the inclusion of new ideas in the mentee’s work.Citation30 Mentees may also gain insight into other fields within the healthcare spectrum.Citation2 In an era dominated by advances in IT, mentees can also benefit from a renewed understanding of practical skills in clinical medicine, particularly the increasing role of e-medicine and online learning tools.
For more experienced mentees, engagement in reverse mentoring can cultivate existing leadership skills, enhancing communication across generations in the workplace.Citation7 Mentees stand to gain improved social capital through increased intra-organizational support and knowledge exchange. Additionally, Tobin argues that the gain of “youthful energy” from an engaged and contributory young person is a “major benefit” of mentorship.Citation40 Talented, albeit less experienced, mentors can bring new ideas and renewed enthusiasm to a mentee’s existing work.Citation30 This may renew interest in a more experienced mentee’s personal career. The potential benefits for mentees in reverse mentoring are summarized in .
Disadvantages of reverse mentoring
The disadvantages of reverse mentoring lie in the foundation of the construct. The mentor as a younger or less experienced contributor to the relationship may be plagued by a lack of confidence and experience. This reflects a traditional imbalance in the concepts of power and may be exacerbated by the overlapping roles between mentor and mentee in a reverse mentorship.
In traditional concepts of mentorship, there is an inherent imbalance of power between mentee and mentor which is well recognized,Citation36,Citation45 particularly in the traditionally hierarchical fields of academic and clinical medicine. Reverse mentoring aims to eliminate these traditional roles by elevating the less experienced colleague to the role of mentor. By contributing new and innovative knowledge to the relationship, the mentor’s status is raised, and the mentor and mentee are considered equals and learn from each other.Citation45 However, the mentor may lack prior experience in the role of mentor,Citation2 limiting his or her ability to fulfill this role adequately. Where mentors lack confidence in their interaction, information exchange is curtailed.Citation45 In order to overcome this potential limitation, reverse mentoring relationships must be characterized by mutuality,Citation7 reciprocity and mutual respect.Citation37
The view of reverse mentorship as a community of practice, characterized by the sharing of knowledge, can lead to a lack of clarity in the role of the mentor and mentee.Citation2 Overlapping roles can blur the boundaries of the traditional mentor–mentee exchange.Citation46 Traditional mentoring relationships have typically advocated for self-identification of mentors by mentees, rather than the formal assigning of mentors.Citation47 There is a lack of literature regarding the most useful way to assign roles in a reverse mentoring relationship, and whether the engagement of mentors and mentees would also benefit from self-identification.
Conclusion
The importance of mentoring in medical education and the health sciences is well documented. However, as outlined by Sambunjak et al, there is an absence of experimental research about mentorship, particularly with regards to theoretical and conceptual perspectives on mentorship.Citation44 Sheri et al advocate for further longitudinal reviews of mentoring efficacy.Citation28 In particular, the relatively contemporary concept of reverse mentoring stands to benefit from further research. In a changing healthcare and medical education landscape, the role of junior colleagues as mentors will increase, particularly with the advent of concepts such as electronic health data and online platforms, and as improved interactions within the workplace and across disciplines are emphasized. More senior colleagues can benefit from their junior colleagues’ enhanced understanding of these concepts and involvement in new research. There has been some exploration of these benefits in the IT, business and educational literature. Further investigation and analysis of reverse mentoring in the field of medical education and health sciences is warranted. Research should focus on the role of the mentor and content of mentorship, including the assigning of mentors, as well as adverse outcomes of mentorship.
Disclosure
The authors report no conflicts of interest in this work.
References
- Roberts A. The origins of the term mentor. Hist Educ Soc Bull. 1999;64:313–329.
- Burgess A, van Diggele C, Mellis C. Mentorship in the health professions: a review. Clin Teach. 2018;14:1–6.
- Haggard DL, Dougherty D, Turban P, Wilbanks JE. Who is a mentor? A review of evolving definitions and implications for research. J Manage. 2011;37:280–304. doi:10.1177/0149206310386227
- Zauchner-Studnicka SA. A model for reverse-mentoring in education. Int Scholarly Sci Res Innovation. 2017;11(3):551–558.
- Ziegler A. Mentoring: konzeptionelle Grundlagen und Wirkamkeitsanalyse. In: Stöger H, Ziegler A, Schimke D, editors. Mentoring: Theoretische Hintergrunde, empirische Befunde and praktische Anwendungen. Lengerich: Pabst Science Publishers; 2009:7–30.
- Augustiniene A, Ciuciulkiene N. Reverse mentoring as a facilitating factor for the development of a beginning teacher’s self-authorship process. Soc Sci. 2013;3(81):73–84.
- Marcinkus Murphy W. Reverse mentoring at work: fostering cross-generational learning and developing millennial leaders. Hum Resour Manage. 2012;51(4):549–574. doi:10.1002/hrm.21489
- Dominguez N, Hager M. Mentoring frameworks: synthesis and critique. Int J Mentor Coach Educ. 2013;2(3):171–188. doi:10.1108/IJMCE-03-2013-0014
- Levinson D. The Seasons of a Man’s Life. New York, NY: Random House; 1978.
- Darwin A, Palmer E. Mentoring circles in higher education. High Educ Res Dev. 2009;28(2):125–136.
- Haynes R, Petrosko J. An investigation of mentoring and socialization among law faculty. Mentor Tutoring. 2009;17(1):41–52. doi:10.1080/13611260802658520
- Zachary L, Fischler L. The Mentee’s Guide: Making Mentoring Work for You. San Francisco, CA: Jossey-Bass; 2009.
- Marquardt M, Waddill D. The power of learning in action learning: a conceptual analysis of how the five schools for adult learning theories are incorporated within the practice of action learning. Action Learn. 2004;1(2):185–202. doi:10.1080/1476733042000264146
- Clutterbuck D. Mentor competences: a field perspective. In: Clutterbuck D, Lane G, editors. The Situational Mentor. Burlington, VT: Gower; 2004:42–56.
- Allen T, Cobb J, Danger S. Inservice teachers mentoring aspiring teachers. Mentor Tutoring. 2003;11(2):177–182. doi:10.1080/13611260306854
- Wenger E. Communities of Practice: Learning, Meaning and Identity. Cambridge: Cambridge University Press; 1999.
- Baker VL, Lattuca LR. Developmental networks and learning: toward an interdisciplinary perspective on identity development during doctoral study. Stud High Educ. 2010;35(7):807–827. doi:10.1080/03075070903501887
- Lave J, Wenger E. Situated Learning: Legitimate Peripheral Participation. Cambridge: Cambridge University Press; 1991.
- Kram K. Phases of the mentor relationship. Acad Manage J. 1983;26(4):608–625.
- Perry L. Who’s mentoring whom?: be a mentor – you might learn something. Public Relat Tactics. 2009;16(11):7.
- Prensky M. Digital Natives, Digital Immigrants. Horiz. NCB University Press. 2001;9(5):1–6.
- Giddens D, Phillips R Reverse Mentoring: finding a new way of working while discovering Web 2.0. ALIA National Library and Information Technicians Conference; September; 2009; Adelaide Convention Centre, Adelaide, South Australia, Australia.
- Harvey M, Buckley MR. Assessing the ‘conventional wisdoms’ of management for the 21st century organization. Organ Dyn. 2002;30:368–378. doi:10.1016/S0090-2616(02)00062-1
- Greengard S. Moving forward with reverse mentoring. Workforce. 2002;81(3):15.
- Hewlett SA, Sherbin L, Sumberg K. How Gen Y and boomers will reshape your agenda. Harv Bus Rev. 2009;8(7/8):71–76.
- Hays B, Swanson DJ. Prevalence and success of reverse mentoring in public relations. Pubic Relat J. 2011;5(4):1–18.
- Dickinson K, Jankot T, Gracon H. Technical Report: Sun Mentoring: 1996–2009. Menlo Park, California: Sun Microsystems; 2009.
- Sheri K, Too JYJ, Chuah EEL, Toh YP, Mason S, Krishna LKR. A scoping review of mentor training programs in medicine between 1990 and 2017. Med Educ Online. 2019;24:1555435. doi:10.1080/10872981.2018.1555435
- Cotunga N, Vickery C. Reverse mentoring: a twist to teaching technology. J Am Diet Assoc. 1998;98(10):1166. doi:10.1016/S0002-8223(98)00270-3
- Lee JM, Anzai YA, Langlotz CP. Mentoring the mentors: aligning mentor and mentee expectations. Acad Radiol. 2006;13:556–561. doi:10.1016/j.acra.2006.01.050
- Stacey E, Gerbic P. Success factors for blended learning. In: Atkinson R, McBeath C, editors. Ascilite: Hello! Where are You in the Landscape of Educational Technology? Proceedings. Ascilite, Burwood, Victoria: Deakin University; 2008:964–968.
- Robinson A. Sixty seconds on … reverse mentoring. Br Med J. 2018;363:k4887. doi:10.1136/bmj.k4029
- Waljee JF, Chopra V, Saint S. Mentoring millennials. J Am Med Assoc. 2018;319:1547–1548. doi:10.1001/jama.2018.3804
- Buring SM, Bhushan A, Brazeau G, Conway S, Hansen L, Westberg S. Keys to successful implementation of interprofessional education: learning location, faculty development, and curricular themes. Am J Pharm Educ. 2009;73(4):60. doi:10.5688/aj730460
- Feldman MD, Arean PA, Marshall SJ, Lovett M, O’Sullivan P. Does mentoring matter: results from a survey of faculty mentees at a large health sciences university. Med Educ Online. 2010;15:1. doi:10.3402/meo.v15i0.5063
- Ramanan RA, Taylor WC, Davis RB, Phillips RS. Mentoring matters: mentoring and career preparation in internal residency training. J Gen Intern Med. 2006;21(4):340–345. doi:10.1111/j.1525-1497.2006.00346.x
- Straus SE, Johnson MO, Marquez C, Feldman MD. Characteristics of successful and failed mentoring relationships: a qualitative study across two academic health centers. Acad Med. 2013;88(1):82–89. doi:10.1097/ACM.0b013e31827647a0
- Palepu A, Friedman RH, Barnett RC, et al. Junior faculty members’ mentoring relationships and their professional development in medical schools. Acad Med. 1998;73(3):318–323. doi:10.1097/00001888-199803000-00021
- Powell SK. Case managers’ retirement: what has reverse mentoring got to do with it? Prof Case Manag. 2013;18(6):271–272. doi:10.1097/NCM.0b013e3182a7a553
- Tobin MJ. Mentoring: seven roles and some specifics. Am J Respir Crit Care Med. 2004;170:114–117. doi:10.1164/rccm.2405004
- Burgess A, Goulston K, Oates K. Role modelling of clinical tutors: a focus group study among medical students. BMC Med Educ. 2015;15(17):1–9. doi:10.1186/s12909-015-0303-8
- Trunk P What Gen Y really wants. Time Magazine; [ Published July, 2007]. Available from: http://www.time.com/time/magazine/article/0,9171,1640395,00.html. Accessed March, 2019.
- Hezlett SA, Gibson SK. Linking mentorship and social capital: implications for career and organization development. Adv Dev Hum Resour. 2007;9:384–411. doi:10.1177/1523422307304102
- Sambunjak D, Straus SE, Marusic A. Mentoring in academic medicine: a systematic review. J Am Med Assoc. 2006;296(9):1103–1115. doi:10.1001/jama.296.9.1103
- Cooke KJ, Patt DA, Prabhu RS. The road of mentorship. Am Soc Clin Oncol Educ Book. 2017;37:788–792. doi:10.1200/EDBK_175193
- Macleod S. The challenge of providing mentorship in primary care. J Postgrad Med. 2007;83(979):317–319. doi:10.1136/pgmj.2006.054155
- Straus SE, Chatur F, Taylor M. Issues in the mentor-mentee relationship in academic medicine: a qualitative study. Acad Med. 2009;84(1):135–139. doi:10.1097/ACM.0b013e31819301ab