
Abstract
Purpose
Successful prosthodontic rehabilitation involves making many interrelated clinical decisions which have an impact on each other. Self-directed computer-based training has been shown to be a very useful tool to develop synthetic and analytical problem-solving skills among students. Thus, a computer-based case study and treatment planning (CSTP) software program was developed which would allow students to work through the process of comprehensive, multidisciplinary treatment planning for patients in a structured and logical manner. The present study was aimed at assessing the effect of this CSTP software on the clinical judgment of dental students while planning prosthodontic rehabilitation and to assess the students’ perceptions about using the program for its intended use.
Methods
A CSTP software program was developed and validated. The impact of this program on the clinical decision making skills of dental graduates was evaluated by real life patient encounters, using a modified and validated mini-CEX. Students’ perceptions about the program were obtained by a pre-validated feedback questionnaire.
Results
The faculty assessment scores of clinical judgment improved significantly after the use of this program. The majority of students felt it was an informative, useful, and innovative way of learning and they strongly felt that they had learnt the logical progression of planning, the insight into decision making, and the need for flexibility in treatment planning after using this program.
Conclusion
CSTP software was well received by the students. There was significant improvement in students’ clinical judgment after using this program. It should thus be envisaged fundamentally as an adjunct to conventional teaching techniques to improve students’ decision making skills and confidence.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Quality decision making is essential for planning prosthodontic rehabilitation. Many prosthetic treatment options are available today depending on patients’ choice and operators’ skills. Decision making involves making many timely and interrelated clinical decisions. Theoretical concepts are taught to the students during their curriculum but managing patients in clinical practice requires the application of that knowledge and a critical thinking ability. There are very few training tools available to help teach students diagnosis and treatment options of discrete conditions and treatment sequencing once a decision has been made.
Self-directed computer-based training has been shown to be a very useful tool to learn synthetic and analytical problem-solving skills to apply factual knowledge to real life, complex patient management.Citation1–Citation4
A survey conducted among the faculty of our institute indicated a perceived lack of competency of dental students to devise a comprehensive treatment plan for prosthodontic rehabilitation cases, and as a result the quality of patient care is often affected. One of the reasons cited was lack of exposure to a variety of clinical cases during I-IV Bachelor of Dental Surgery tenure. An inability of conventional teaching techniques to provide information on a generic framework to formulate a custom prosthodontic rehabilitation plan for a particular clinical situation was also mentioned as another possible factor.
Thus, the present study aimed to develop a computer-based case study and treatment planning (CSTP) software program which will expose dental students to a variety of clinical situations requiring prosthodontic rehabilitation using tooth and/or implant supported removable or fixed prostheses. Furthermore, it aimed to seek their perceptions about the said software and evaluate its effect on clinical judgment while planning prosthodontic rehabilitation.
Material and methods
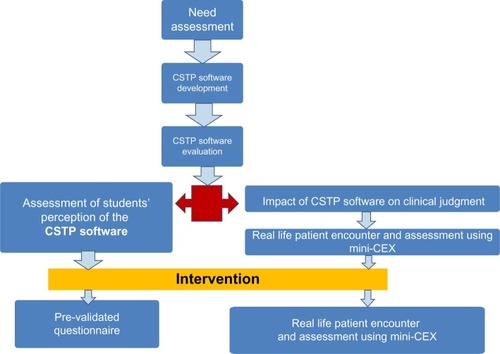
This is a cross sectional pre- and post-test investigation. The flowchart of methodological sequence followed is depicted in .
Figure 1 Flowchart of methodology.
Software development
CSTP software was developed entitled “Case assisted Learning in Prosthodontics-Prosthodontic Rehabilitation of the Partially and Completely Edentulous Adult” constituting 50 case scenarios adapted from real life situations which had been peer-reviewed.
Selection of cases
The cases were real life patients who were completely and partially edentulous requiring prosthodontic rehabilitation using tooth and/or implant supported removable and/or fixed prostheses. Cases with acquired maxillary and mandibular defects were also included. A special emphasis was given to select cases which required interdisciplinary planning namely, pre-prosthetic treatments by endodontics, periodontal therapy, surgery, and other specialized procedures. The intent was to train the students to make interdisciplinary clinical decisions and to follow the correct sequencing of the treatment.
Design of the software
The first phase was the provision of information about the real life patient in the form of clinical photographs, X-rays, reports of investigations, etc. In the second stage the request for some action from the respondent was sought, ie, to devise a treatment plan for that particular case using the structured template provided (including pre-prosthetic treatment, treatment sequencing, detailed design of the prosthesis, maintenance, and prognosis of the case), so as to guide them in the decision making processes. At the third stage, a standard treatment plan for that particular case, which was entered into the software program beforehand, was displayed along with the treatment plan submitted by the student for that case so that the student could compare, analyze, and learn from his/her mistakes.
Students can choose any case and after submission their response for that particular case is stored in the software for reference.
Selection of subjects
The study design involves a single group in which pre- and post-testing was carried out. After approval from Vidya Shikshan Prasarak Mandal’s (VSPM) Academy of Higher Education ethics committee, universal sampling technique was adopted.
In our university, students enter into a one year rotating internship after passing their four year Bachelor of Dental Surgery course during which they are posted in each discipline for a stipulated period. This is the time when they are actively involved in the diagnosis and treatment planning for all patients who report to the prosthetic department. Thus, during the present investigation, all 60 interns posted at the Department of Prosthodontics at our institute during the period of one year (August 2011–July 2012) were asked to undertake all 50 cases. Consent to participate was obtained from the interns who used the software.
Software evaluation
The evaluation of the intervention was carried out according to Kirkpatrick’s level 2b which assesses learners’ reaction, modification of attitudes and perceptions as well as acquisition of knowledge and skills.Citation5
Evaluation of the impact of this program on clinical judgment
Evaluation was done using mini-CEX (American Board of Internal Medicine [ABIM]) format.Citation6 It has been validated for use in medicine and was chosen because assessment of students can be done in a structured manner by giving scores. Although all seven competencies (interviewing skills, examination skills, counseling skills, clinical judgment, organization/efficiency, professionalism, and overall clinical competence) were observed and scored, only “clinical judgment” was taken into account for analysis. It includes selecting the appropriate investigation, interpreting findings, and selecting proper treatment for a particular case. The scores range from 1–3 (unsatisfactory), 4–6 (satisfactory), and 7–9 (superior).
Pre-intervention real life clinical encounters with patients requiring extensive prosthodontic rehabilitation were planned for the students. They were asked to examine, diagnose, and plan the treatment while one trained faculty member recorded the details using mini-CEX format. Scores were recorded. Feedback was not given prior to the use of CSTP software as it might have created biased results. All students were asked to go through and submit the treatment plan for all the cases in the CSTP program. Post-intervention, students were again subjected to real life clinical encounters with patients requiring extensive prosthodontic rehabilitation and their clinical judgment was scored using mini-CEX. They were asked to examine, diagnose, and plan the treatment while one trained faculty member recorded the details using mini-CEX format. Scores for clinical judgment were recorded.
Evaluation of students’ perception about the software
Evaluation was done by a prevalidated feedback questionnaire with a total of seven questions of which three were close-ended.
The primary research question was: “Is the use of CSTP software associated with change in clinical judgment of dental students while planning prosthodontic rehabilitation?” The null hypothesis was that the use of the CSTP software does not affect the clinical judgment of dental students (P-value 0.05).
Results
The faculty assessment scores of clinical judgment using mini-CEX before and after the use of CSTP software are depicted in and . The mean scores before the intervention were 3.6 (standard deviation [SD] ±1.94). Mean scores post-intervention were 6.32 (SD ±1.92). Statistical analysis was done using chi-square test. The values were χ2=14.4, P=0.0001. Thus, the improvement in scores was statistically significant after using the program (P<0.001). Thus, the null hypothesis was rejected. It shows that the CSTP software has improved the clinical judgment of students for planning prosthodontic rehabilitation.
Figure 2 Impact of CSTP software on clinical judgment scores of students.
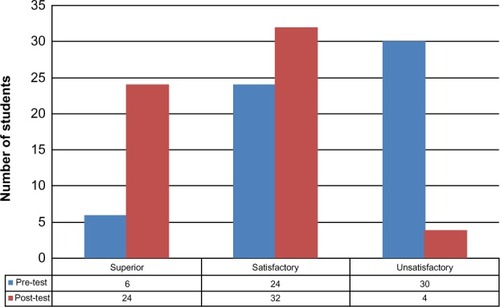
Table 1 Mini-CEX scores for clinical judgment
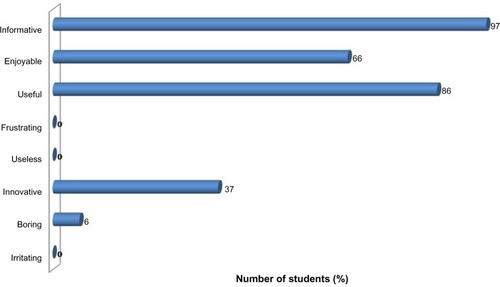
Students’ perceptions about the program as evaluated by a feedback questionnaire are depicted in and . The analysis indicated that 86% of students felt that it was easy to navigate the program, 100% of students felt the program enhanced their existing knowledge about the subject, 90% of students felt that the program increased their confidence in planning prosthodontic rehabilitation, and only 6% said that they would prefer lectures instead of this program. Ninety-seven percent of students felt the program was informative, 86% were of the opinion that it was useful, 66% mentioned that it was enjoyable, and only 2% found it boring. Eighty-six percent of students agreed that conventional teaching techniques do not provide adequate training to plan prosthodontic rehabilitation but 13% disagreed with this statement. Ninety percent of students agreed that this program should be used along with conventional teaching techniques regularly.
Figure 3 Students’ perceptions about the CSTP software, part I.
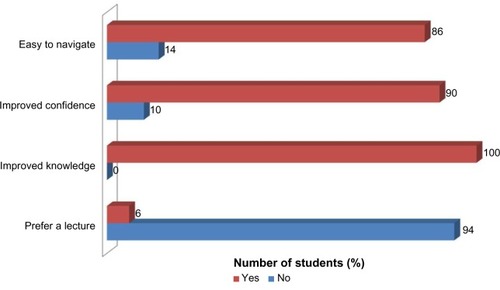
Figure 4 Students’ perceptions about the CSTP software, part II.
In response to the open-ended question “What was the main thing you learnt?” most answers referred to the logical progression of planning, the insight into decision making and the need for flexibility in planning treatment.
The best things about the program were perceived to be the concept and self-paced nature of the learning process, as well as the screen design and layout. Students also described the program in their own words as “interesting”, “innovative”, and “relevant”.
The study was supplemented by a focus group discussion. The program was described by the students as a computerized treatment planning guide in which they could devise a structured treatment plan in a standardized manner. The themes that emerged from the focus groups revealed students’ agreement that a CSTP software program is helpful both for learning clinical application of theoretical knowledge and clinical judgment. They also expressed a need for self-directed learning. One common demand was that there should be human feedback at some stage. In conclusion, the overall attitude of dental students was positive toward CSTP software.
Discussion
A book can never provide or teach active dental therapy planning. To facilitate this kind of learning, real patients and training are required. When a case is presented in a book, all the learning material is presented linearly, frequently together with a subsequent solution to the case. Often the book begins from an already given topic with a description of a patient record and status of the cases. This principle is also frequently used in lectures wherein the student is usually told the solution without any interaction with the teacher or content.Citation1,Citation2
Crespo et alCitation3 examined the reasoning skills of “expert” dentists and found them to be qualitatively different from those of “beginner” and “competent” clinicians. They have proposed that such skills could be taught, concluding that students’ clinical experience would be enhanced by exposing them to as wide a variety of cases as possible. They suggested that case-based scenarios could be utilized to inculcate an understanding of the processes of clinical decision making. Since clinical time in pre-doctoral dental curricula is constrained, students can be exposed to only a limited sample of the entire array of clinical conditions. Case-based teaching may provide a means to ease these constraints. Foster et alCitation4 in their study on Dental Students’ Attitudes towards the Design of a Computer-Based Treatment Planning Tool concluded that it could be a significant instructional tool for the development and practice of cognitive skills relevant to treatment planning through a library of structured patient cases of increasing complexity. They also stated that it is desirable that a CSTP tool should be developed in such a way that it will allow online, after-hours access to a library of planned and unplanned patient cases.
In the present curriculum students perform certain pre-decided clinical procedures for all disciplines during their clinical posting individually. However, they are not asked to treat all problems of a patient as a whole. So their critical thinking and problem solving ability is not fully developed. When these students enter into one year of compulsory rotating internship, they find it difficult to plan complex prosthodontic rehabilitation for patients who report to OPD (outpatient department) of the department. Taking into account the limitations of the curriculum, time and paucity of clinical case material, computerized learning seemed to be an excellent alternative to train students for planning prosthodontic rehabilitation. Hence, the present program developed by us follows the concept given by Foster et alCitation4 which allows students to work through the process of comprehensive, multidisciplinary treatment planning for patients in a structured and logical manner. The first phase is the provision of information about the patient, the second, the request for some action from the respondent, the third, the feedback to the respondent. The case scenarios in this program enable the students to visualize the clinical situation and analyze it critically. Also, a structured format helps them to plan and sequence treatment steps logically. An attempt has been made to record a variety of cases requiring all types of prostheses namely, complete denture, removable and fixed partial denture, full mouth rehabilitation, implant supported prosthesis, maxillofacial prosthesis, and so on.
Similar programs have been evaluated previously regarding students’ perceptions,Citation4,Citation7–Citation11 however, impact on clinical judgment has not been reported. Thus, in the present study it was deemed necessary to evaluate any change in the students’ clinical judgment after using CSTP software.
Selecting a standardized assessment tool for clinical judgment was the most critical aspect of this study as it is very difficult to measure clinical decision making skills or clinical judgment objectively. The only assessment tool which rates clinical judgment is mini-CEX. It is a method for assessing clinical performance in the workplace developed by the American Board of Internal Medicine (ABIM). It has seven competency domains including overall clinical competency, a nine point rating scale, and has been shown to be valid, reliable, feasible, and acceptable and fair assessment in postgraduate and undergraduate practice in the USA.Citation6 It was used in the present investigation as it is a standardized assessment tool which can also be used to give feedback to the students during the course of the study. The assessment was done only in OPD set-up and focus areas were data gathering, diagnosis, and treatment planning. The complexity of cases ranged from medium to high. Scores of “clinical judgment” were recorded and compared pre- and post-intervention, ie, using the CSTP software.
Users’ reactions were positive as to clinical applicability, design, and ease of use of the program. There was definitive acquisition of knowledge and clinical judgment of dental students reflected by improved scores on mini-CEX. Although the exact same intervention has not been previously reported in the literature, the results of the present investigation are in accordance with Lechner et alCitation12 who developed a computer-aided learning program for teaching principles of removable partial denture design which was also very well received by students.
This study has a few limitations such as: in order to evaluate the CSTP software more effectively, more cases should be included in the software. Also, the evaluation should be done for a bigger number of students and over a long period of time.
In future, there is a need to evaluate long-term effects of using this program (Kirkpatrick’s level 3 and 4) for students as well as patient care. This software can also be evaluated as an assessment tool.
Conclusion
Computerized CSTP software was well received by the students. There was significant improvement in students’ clinical judgment after using this program.
It should thus be envisaged fundamentally as an adjunct to conventional teaching techniques to improve students’ clinical judgment and confidence. Also, it must be evaluated over an extended period of time to assess the effect on overall quality of patient care at the institute.
Acknowledgments
Dr Avinash Supe, Director of FAIMER regional Institute at GSMC Mumbai for his critical analysis of this investigation and Dr Usha Radke, Dean of VSPM’s Dental College and Research Centre, Nagpur for supporting this investigation.
Disclosure
The authors report no conflicts of interest in this work. The software development project was partially funded by the Teacher’s Scholarship Grant from Maharashtra University of Health Sciences at Nashik.
References
- SchittekMMattheosNLyonHCAttströmRComputer assisted learning. A reviewEur J Dent Educ2001539310011520331
- DugasMBatschkusMMLyonHCJrMr Lewis on the Web – how to convert learning resources for Intranet technologyMed Educ1999331424610211276
- CrespoKETorresJERecioMEReasoning process characteristics in the diagnostic skills of beginner, competent and expert dentistsJ Dent Educ200468121235124415576812
- FosterLKnoxKRungAMattheosNDental students’ attitudes toward the design of a computer-based treatment planning toolJ Dent Educ201175111434144222058392
- YardleySDornanTKirkpatrick’s levels and education ‘evidence’Medical Education2012469710622150201
- NorciniJJBlankLLArnoldGKKimballHRThe mini-CEX (clinical evaluation exercise): A preliminary InvestigationAnn Intern Med1995123107951997574198
- KumarVGadbury-AmyotCCCase-based and team-based learning model in prosthodontic and maxillofacial radiologyJ Dent Educ201276333033722383601
- TaoLTangYZhuMYZhuYQApplication of case-based learning in clinical practice of dental studentsShanghai Kou Qiang Yi Xue2011202209212 Article in Chinese21566876
- LechnerSKThomasGABradshawMLechnerKMPlanning oral rehabilitation: case-based computer assisted learning in clinical dentistryBr Dent J2001191315215611523888
- LoweCIWrightJLBearnDRComputer-aided Learning (CAL): an effective way to teach the Index of Orthodontic Treatment Need (IOTN)?J Orthod200128430731111709597
- LechnerSKLechnerKMThomasGAEvaluation of a computer-aided learning program in removable partial denture framework designingJ Prosthodont19998210010510740508
- LechnerSKThomasGABradshawMAn interactive multimedia solution to learning removable partial denture designJ Prosthodont1998731771829807101