
Abstract
Primary breast lymphoma is a rare disease and accounts for 0.5% of cases of breast cancer. Most primary breast lymphomas develop from B cells, and the involvement of T cells is rare. Anaplastic large cell lymphoma (ALCL) is a recently discovered T-cell lymphoma associated with breast implants. Only a few cases have been reported to date. It is believed that the incidence of ALCL is increasing because of the increasing number of breast implants. The clinical presentation is variable and can manifest as a palpable mass in the breast or armpit, breast pain, or capsular contracture. Because of the rarity of the disease and the lack of knowledge to date, clinical diagnosis is often delayed, with consequent delays in treatment. The cause and pathogenesis have not been fully elucidated, and there are no evidence-based guidelines for diagnosis, treatment, or follow-up of this disease. We present a review of cases of patients with silicone breast implants, including ALCL, a rare type of breast cancer that is still under study, and silicone-induced granuloma of breast implant capsule and its differential diagnosis, and discuss if a silicone-induced granuloma of breast implant capsule could be the precursor of the disease.
Keywords:
Introduction
Breast cancer is the most common cancer among women and is considered the leading cause of cancer mortality among women in Brazil. More than 95% of cases of breast cancer are carcinomas. Other malignant tumors may occasionally develop in breast tissues, including sarcomas, secondary metastases, and lymphomas.Citation1
Primary breast lymphoma
Primary breast lymphomas (PBLs) are rare neoplasms, representing approximately 0.5% of the cases of breast cancers and 2% of the cases of extranodal lymphomas.Citation2 PBLs originate from periductal and perilobular lymphoid tissues of the breast and may be related to lymphoid tissues associated with mucous membranes.Citation3 Most PBLs are derived from B cells, and tumors with T-cell phenotypes are rare (less than 6% cases).Citation4 The average age at onset of PBL is 57 years.Citation5
The clinical and radiological manifestations of PBL are indistinguishable from those of other breast tumors. Therefore, immunohistochemistry is fundamental for the diagnosis of these tumors.Citation4
These tumors are usually single, painless, and well-defined and have an elastic consistency.
The diagnostic criteria originally defined for PBL continue to serve as the standard definition of the disease,Citation6 which include the following:
An initial site of disease presentation in the breasts;
The absence of a previous history of lymphoma;
The absence of disseminated disease at diagnosis;
An association between the lymphoma and breast tissue on histopathological examination;
An association between the axillary lymph nodes involvement with breast lymphoma.
Anaplastic large cell lymphoma (ALCL)
Anaplastic large cell lymphoma (ALCL) is a rare subtype of non-Hodgkin lymphoma of T cells; it represents approximately 3% of cases of non-Hodgkin lymphoma.Citation7
Most of the described cases (81%) correspond to ALCL and involve the presence of CD30+ and the absence of the ALK gene.Citation8
ALCL CD30+ occurs as a result of the activation and abnormal proliferation of T lymphocytes; it may present in cutaneous or systemic forms. The expression of the ALK gene allows the classification of ALCL into two subtypes, which help determine prognosis. The morphological and cytological characteristics of ALCL associated with breast implants are similar to those of systemic ALK-negative ALCL; however, the latter has a poor prognosis, whereas breast implant-associated ALK-negative ALCL is typically an indolent disease with a much better prognosis.Citation9
The interest in ALCL has been motivated by reports of cases of PBLs associated with saline and silicone implants. These cases usually involve surgical findings, and the diagnosis before surgery is unknown.Citation10–Citation12
The first case of ALCL associated with breast implants was described in 1997 by Keech and Creech.Citation13 In 2011, the United States Food and Drug Administration issued a statement confirming 60 cases of ALCL associated with prosthesis.Citation14 Since then, the number of cases of ALCL has increased, presumably due to the growing number of breast implants and the greater knowledge of the disease pathology.
The reported incidence of ALCL is one case per 500,000 women with breast implants. The age at onset varies between 34 and 59 years, with an average of 46 years. The disease develops within approximately 3–7 years, with a mean of 5 years after mammoplasty.Citation11
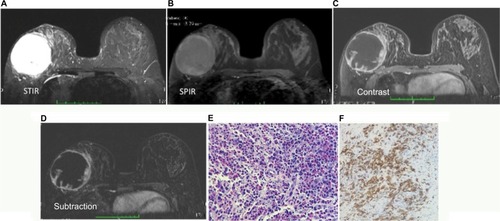
ALCL affects the fibrous capsule around the implant, rarely appears as a solid mass and does not involve the breast parenchyma.Citation9,Citation15 The initial presentation in most patients includes seroma without spontaneous resolution, capsular contracture, or peri-implant massesCitation8 ().
Figure 1 A 57-year-old patient with asymmetric enlargement of the right breast and clinical signs of capsular contracture.
Abbreviations: MRI, magnetic resonance imaging; ST1R, short-TI inversion recovery; SPIR, spectral presaturation with inversion recovery; ALCL, anaplastic large cell lymphoma.
The mechanism involved in the development of lymphoma is uncertain,Citation11 and its pathogenesis is currently under investigation. However, the mechanism may involve an immune response induced by the silicone or polyurethane material in the implant, which may cause an immune overreaction and induce monoclonal neoplasia with activated T lymphocytes. Other postulated mechanisms involve an indirect reaction mediated by cytokines and toxic damage induced by silicone.Citation16
Microscopic leakage of silicone from the interior of the prosthesis into the intracapsular area has been described even in cases in which implants are not ruptured. In the case of saline or silicone implants, the capsules may be responsible for chronic local inflammation with T-cell activation and clonal expansion.Citation11
Silicone-induced granuloma of breast implant capsule (SIGBIC)
The SIGBIC is probably a resultant of an autoimmune/inflammatory syndrome induced by silicone (ASIA syndrome). The association between autoimmunity and silicon exposure, similar to that causing the ALCL, may result in the following scenario:
Silicone leaks from the interior of a normal implant into the intracapsular space;
Silicon-containing particles are captured by macrophages, resulting in entrapment within lysosomes;
These macrophages are activated, resulting in the production of cytokines, for example, interleukin-1b, reactive oxygen species, and reactive nitrogen species;
Apoptosis of macrophages result in the release of silicon-containing particles that can be taken up once again by other macrophages.
Exposure to silicon-containing particles also leads to a massive production of interleukin-17, resulting in an influx of neutrophils that are activated and produce reactive oxygen species and release of myeloid granular enzymes such as myeloperoxidase. Additionally, if there is a capsular disruption, silicon-containing particles are transported to the regional lymph nodes, resulting in a pronounced adjuvant effect. Silica particles induce a type-2 inflammatory response characterized by increase in IgE and IgG1 and chronic activation of T cells, possibly because negative regulators of T cells are dysfunctional in combination with dysfunction of regulatory T cells. It is known that silicones may undergo oxidization to silica and that silicon-containing gel induces an adjuvant effect.Citation17
Searching the bibliographic databases online on the web, no reference was found to silicone-induced granuloma in intact breast implants. As seen above, the pathophysiology of ALCL is very similar to that of SIGBIC, where the only difference would be monoclonal neoplasia induced by activation of T lymphocytes. Because they are very rare entities, new studies need to be performed to determine whether ALCL is an evolution of SIGBIC. We also believe that SIGBIC should be underdiagnosed in clinical practice due to its benign course.
Diagnosis
Clinical examination
Clinically, ALCL may present as seroma without spontaneous resolution, capsular contracture, or peri-implant masses,Citation8 while SIGBIC may present as a mass. The conditions usually have an indolent course and excellent prognosis, with a good response to excision of the fibrous capsule and removal of the implant. In contrast, cases that involve the presence of masses can be more aggressive and can have poor prognoses.Citation15
Image diagnosis
The image features of ALCL and SIGBIC will be similar, although ALCL could present as fluid fill within the intracapsular space, while SIGBIC is most often present as an intracapsular mass. It is important to emphasize that the implant should be intact, without signals of visible ruptures by imaging methods.
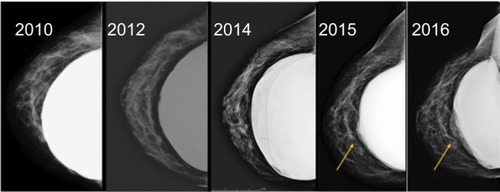
Mammography is usually the first clinical examination conducted (). However, in patients with capsular contracture, their performance may be difficult due to the breast stiffness. Patients must complete a consent form for the examination owing to the risk of rupture by compression of the device.
Figure 2 A 53-year-old patient at the breast screening program.
Abbreviation: BI-RADS, breast imaging reporting and data system.
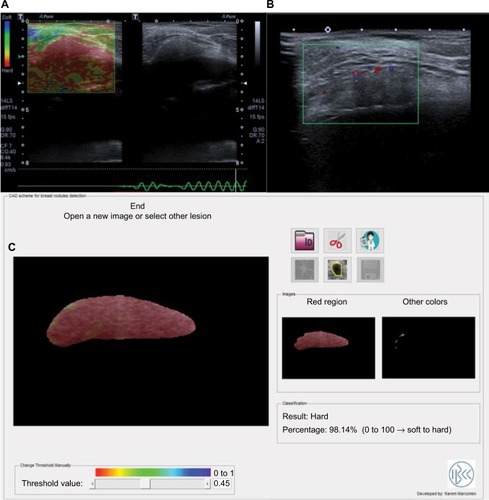
Ultrasound is the second most common examination and is usually interpreted in conjunction with the mammogram. Ultrasound may be used to guide punctures or biopsies; one of its advantages is its low cost. ALCL findings are often not very specific. Approximately two-thirds of patients present fluid collection around the implant, which is observed in the images, and one-third are characterized by the presence of masses ().
Figure 3 The same 53-year-old patient noted in the earlier figure underwent ultrasound scan that shows (A) a hard mass at the elastography, (B) with high vascularity at the color Doppler scan, and (C) when processing a CAD software of the lesion, the result shows a mass composed essentially of hard tissue, 98.14% of hard tissue.
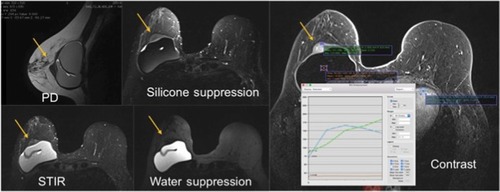
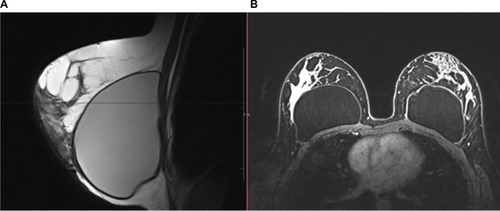
Magnetic resonance imaging (MRI) has the best sensitivity for the assessment of suspected cases of lymphoma and evaluation of the integrity of the implant. For these reasons, MRI is widely used in clinical practice ().
Figure 4 MRI of the same 53-year-old patient noted in the earlier figures.
Abbreviations: PD, proton density; ST1R, short T1 inversion recovery; MRI, MRI, magnetic resonance imaging.
Cytological/anatomopathological diagnosis
Diagnosis can be made by cytology of the seroma or biopsy of the capsule.Citation5 In cases of recurrent seroma that develop approximately 6 months or more after mammoplasty, cytological examination of the aspirate is recommended because the lymphoma cells are found in seroma around the implant, in the fibrous capsule or within a peri-implant mass.Citation8,Citation18 Typically, there is no invasion, other than the fibrous capsule, into the breast parenchymaCitation18 ().
Figure 5 Specimen of core needle biopsy of the lesion shows a rigid lesion.
Abbreviation: SIGBIC, silicone-induced granuloma of breast implant capsule.
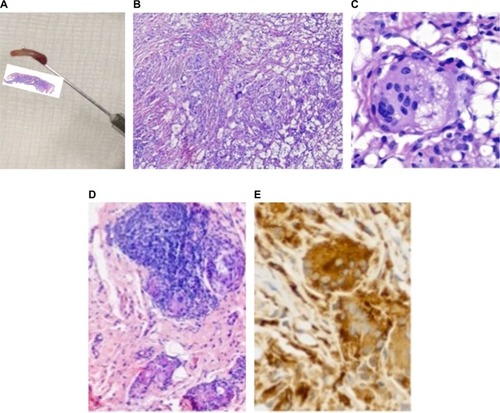
The differential diagnosis between ALCL and SIGBIC is made essentially by the presence of anaplastic monoclonal T cell at optic microscopy, enhanced by CD30+ and CD3 immunostain.
Differential diagnosis
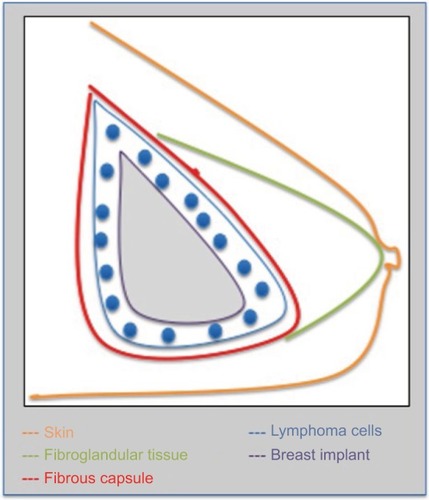
No masses should be present in the virtual space between the fibrous capsule and the breast implant. If present, these masses limit the differential diagnosis of ALCL and SIGBIC ().
Figure 6 Schematic representation of the location of ALCL and SIGBIC.
The main differential diagnosis includes the presence of seroma, capsular contracture, late hematoma, and late inflammatory/infectious processes.
Seroma is one of the complications associated with breast implants. It consists of an exudate between the fibrous capsule and the implant that is typically reabsorbed spontaneously. The complication is considered late when its clinical manifestation occurs more than 12 months after the procedure. In general, most of the seromas described in the literature are associated with Biocell textured implants, which favor the development of double capsules.Citation19 Double capsules usually occur when there is detachment of the fibrous capsule from the surface of the implant, forming a local seroma/hematoma. After resorption, a new, second, capsule is formed.
Capsular contracture results from the proliferation of fibrous scar tissues in the adjacent fibrous capsule; these tissues compress and deform the implant. This complication may be due to infection, hematoma, or seromaCitation20 (). Its clinical scoring follows the classification of Baker and includes the following four grades:
Grade I: soft breast, with normal visual appearance;
Grade II: slight stiffening of the breast, with normal visual appearance;
Grade III: hardening of the breast, with abnormal visual appearance (deformity); and
Grade IV: hardened breast, with pain and significant visual deformity.
Figure 7 A 43-year-old patient with thickening and discomfort in the left breast.
Abbreviation: PD, proton density.
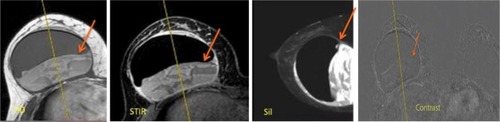
Late hematoma originates from medium-sized arteries located in the implant capsule. Chronic bleeding of these arteries is caused by microfractures in the fibrous capsule. Because of the rigidity of the prosthesis, the retraction of the damaged vessel is limited, which favors new bleedingCitation21 ().
Figure 8 A 48-year-old patient with pain and enlargement on the right breast.
Abbreviations: PD, proton density; ST1R, Short T1 inversion recovery; Sil, silicone; MRI, magnetic resonance imaging.
Late infection can occur after cosmetic surgeries such as breast augmentation, in which 2.9% of patients present infection in the surgical bed; among those affected, 1.7% cases are acute, and 0.8% cases are late. These rates are higher in patients undergoing mastectomy and reconstruction because of the complexity of the procedures and range between 1% and 53%. The onset of late infection may vary from a few months to several years and is different between saline implants (onset within 8 weeks, with an average of 4 weeks) and silicone implants (onset within 24 weeks, with an average of 8 weeks). Late infections are caused by the colonization of prostheses secondary to blood bacteremia. The microorganisms involved are gram-positive and gram-negative bacteria. Coagulase-negative staphylococci and Propionibacterium acnes are the most common strains. The diagnosis is made by liquid culture of the material obtained by fine-needle aspiration, and empirical treatment with vancomycin should be conducted with antibiotics until the results of antibiogram susceptibility testing become available, based on the high number of infections due to β-lactam resistant pathogens, among which are methicillin-resistant Staphylococcus aureus and coagulase-negative staphylococciCitation22 ().
Figure 9 A 35-year-old patient with signs of fluid collection in the right breast 7 years after implantation.
Abbreviation: MRI, magnetic resonance imaging.

The main differential diagnoses are not correlated with the presence of masses with anomalous enhancement on MRI. Therefore, the injection of a paramagnetic agent (gadolinium) is essential in MRI examinations of breast implants to determine if the diagnosis of ALCL or SIGBIC should be discarded because of the consequences of late diagnosis. Without the use of contrast media, it is not possible to evaluate the presence of solid masses in the hematoma.
We suppose that SIGBIC is subdiagnosed at the clinical practice due to some factors: lack of information about the implant status at the surgery for the pathologist, and most often the material of capsulotomy is not sent for histological examination. We believe it could be a precursor of the ALCL because both have the same physiopathogeny.
Treatment
The treatment proposed for ALCL and SIGBIC is almost the same: removal of the prosthesis and fibrous capsule. Chemotherapy or adjuvant radiotherapy is not indicated in cases confined to the capsule for ALCL.Citation23 Despite the poor prognosis of ALK-negative ALCL, the primary cases with silicone implants appear to have an indolent course, with good response to treatment and better disease-free survival.Citation8 The reported rate of cure is higher than 90%. Cases with clinical presentation of solid masses are often more aggressive; in such instances, secondary therapy, such as chemotherapy and radiation, is recommended.Citation23,Citation24
Conclusion
Although ALCL and SIGBIC are rare, knowledge about these diseases is essential in patients subjected to diagnostic MRI for the assessment of breast implants because treatment is simple and involves the removal of the prosthesis and the capsule around the prosthesis. Therefore, a contrast agent should be used for the evaluation of breast implants on MRI to ensure that a diagnosis is made before the surgery for prosthesis replacement is performed because of the complications reported for ALCL.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
The authors are grateful to:
Marcelo L Balancin, MD, from Diagnostika – Patologia Cirúrgica e Citologia, who provided us the histopathologic images of the SIGBIC;
Raquel Civolani Marques Fernandes, MD, PhD, from FEMME – Laboratório da Mulher, who provided us the histopathologic images of the ALCL.
References
- inca.gov.br [homepage on the internet]Rio de JajeiroINCA- Ministério da Saúdec1996-2016 Available from: http://www2.inca.gov.br/wps/wcm/connect/tiposdecancer/site/home/mamaAccessed October 27, 2016
- JoksMMysliwiecKLewadoskiKPrimary breast lymphoma – a review of the literature and report of three casesArch Med Sci201171273322291729
- MirandaRNLinLTalwalkarSSAnaplastic large cell lymphoma involving the breast: a clinicopathologic study of 6 cases and review of the literatureArch Pathol Lab Med20091331383139019722744
- Jeanneret-SozziWTaghianAEpelbaumRPrimary breast lymphoma: Patient profile, outcome and prognostic factorsBMC Cancer20088869318380889
- BinmahfouzASteinkeKA case report of breast implantassociated anaplastic large cell lymphoma: The good, the bad, and the uglyInt J Case Rep Images201678537541
- WisemanCLiaoKTPrimary lymphoma of the breastCancer197229170517124555557
- JarjisRDHansenLBMatzenSHThe non-specific symptoms of breast implant-associated anaplastic large cell lymphoma resulting in delayed diagnosis: a case-based reviewJPRAS Open2015614
- ScheligaAAReinertTSantosALStefanoffCGLinfoma primário da mama: apresentação clínica e características histopatológicas e molecularesRevista Brasileira de Oncologia Clínica201287987 Portuguese
- XuJWeiSBreast implant – associated anaplastic large cell lymphomaArch Pathol Lab Med2014138684284624878027
- SahooSRosenPPFeddersenRMAnaplastic large cell lymphoma arising in a silicone breast implant capsule: a case report and review of the literatureArch Pathol Lab Med20031273e115e11812653596
- RodenACMaconWRKeeneyGLSeroma-associated primary anaplastic large-cell lymphoma adjacent to breast implants: an indolent T-cell lymphoproliferative disorderMod Pathol200821445546318223553
- OlackBGuptaRBrooksGSAnaplastic large cell lymphoma arising in a saline breast implant capsule after tissue expander breast reconstructionAnn Plast Surg2007591565717589261
- KeechJACreechBJAnaplastic T-cell lymphoma in proximity to a saline-filled breast implantPlast Reconstr Surg19971005545559252643
- KimBPredmoreZSMattkeSvan BusumKGidengilCABreast implant-associated anaplastic large cell lymphoma: update results from a structured expert consulation processPlast Reconstr Surg Glob Open201531e29625674377
- ClemensMWMirandaRNComing of age: Breast implantassociated anapestic large cell lymphoma after 18 years of investigationClin Plast Surg20154260561326408447
- fda.gov [homepage on the internet]Silver SpringU.S. Food and Drug Administration [Updated January 26, 2011]. Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm241090.htmAccessed October 27, 2016
- Cohen TervaertJWKappelRMSilicone implant incompatibility syndrome (SIIS): a frequent cause of ASIA (Shoenfeld’s syndrome)Immunol Res2013562–329329823576058
- ThompsonPALadeSWebsterHRyanGPrinceHMEffusion-associated anaplastic large cell lymphoma of the breast: time for it to be defined as a distinct clinicopathological entityHaematologica201095111977197920801901
- SpearSLRottmanSJGlicksmanCBownMAl-AttarALate seromas after breast implants: theory and practicePlast Reconstr Surg2012130242343522495216
- fda.gov [homepage on the internet]Silver SpringU.S. Food and Drug Administration [Updated August 13, 2013]. Available from: http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ImplantsandProsthetics/BreastImplants/ucm064348.htmAccessed October 27, 2016
- PetersWFornasierVHowarthDLate unilateral hematoma after breast augmentationPlast Surg (Oakv)2014221182125152642
- RubinoCBrongoSPagliaraDInfections in breast implants: a review with a focus on developing countriesJ Infect Dev Ctries2014891089109525212072
- KimBRothCYoungVLAnaplastic large cell lymphoma and breast implants: results from a structured expert consultation processPlast Reconstr Surg2011128362963921502904
- TalwalkarSSMirandaRNValbuenaJRLymphomas involving the breast: a study of 106 cases comparing localized and disseminated neoplasmsAm J Surg Pathol2008321299130918636016