
Abstract
Whole breast external beam radiotherapy (WBEBRT) is commonly used as an essential arm in the treatment management of women with early-stage breast cancer. Dosimetry planning for conventional WBEBRT typically involves a pair of tangential fields. Advancement in radiation technology and techniques has the potential to improve treatment outcomes with clinically meaningful long-term benefits. However, this advancement must be balanced with safety and improved efficacy. Intensity-modulated radiation therapy (IMRT) is an advanced technique that shows promise in improving the planning process and radiation delivery. Early data on utilizing IMRT for WBEBRT demonstrate more homogenous dose distribution with reduction in organs at risk doses. This translates to toxicities reduction. The two common descriptors for IMRT are forward-planning “fields in field” and inverse planning. Unlike IMRT for other organs, the aim of IMRT for breast planning is to achieve dose homogeneity and not organ conformality. The aim of this paper was to evaluate whether IMRT is ready for prime time based on these three points: 1) workload impact, 2) the clinical impact on the patient’s quality of life, and 3) the appropriateness and applicability to clinical practice.
Introduction
Breast cancer is the most common cancer that occurs in females and the majority of cases are comprised of early-stage disease.Citation1 Breast conserving surgery (BCS), followed by adjuvant radiation therapy (RT), is an essential arm in the treatment management of women with early-stage breast cancer.Citation2 Onitilo et alCitation3 demonstrated that the judicious use of adjuvant RT post-BCS improves survival outcomes compared to radical mastectomy alone.Citation3 Adjuvant RT also halves the recurrence rate thereby significantly improving survival rates.Citation4,Citation5 This translates to more women at risk of developing chronic toxicities associated with their treatment management.
Whole breast external beam radiotherapy (WBEBRT) is associated with acute RT-induced toxicities such as skin desquamation, edema, and pain. This can affect patient’s quality of life (QoL) and also influence their decision regarding the use of BCS with adjuvant RT.Citation6 Hence, the ability to ensure treatment efficacy while reducing toxicities is increasingly important.
Advancement in radiation technology and techniques has the potential to improve treatment outcomes with clinically meaningful long-term benefits.Citation7 However, this advancement must be balanced with safety and improved efficacy. As such, breast RT has progressed from two-dimensional (2D) treatment therapy, based on anatomical landmarks and conventional simulator to three-dimensional (3D) therapy that utilizes computed tomography planning.
Dosimetry planning for conventional WBEBRT typically involves a pair of tangential fields directed to the breast at an angle. The tumor volume or target is the whole ipsilateral breast and the usual field borders are superiorly from the clavicular head to the infra-mammary fold inferiorly and medially from the mid-sternum to the mid-axillary line laterally. A drawback of this technique is the propensity for a more inhomogeneous distribution of the radiation dose due to varying breast shapes and sizes. Due to the conical shape of the breast, the radiation beam must travel through more tissue along the chest wall compared to the nipple areolar complex (NAC) region. This results in significantly higher doses (hot spots) in the NAC region. To improve dose homogeneity throughout the entire breast, wedges as well as additional “fields-in-field” methods may be utilized.Citation8 WBEBRT is often delivered without explicit contouring of the target volume.Citation9
What is intensity-modulated radiation therapy (IMRT)?
Technical advances in radiation oncology rest on the principle of optimizing the therapeutic ratio, that is delivering maximum radiation dose to the target volume while minimizing the dose to the surrounding normal tissues (also known as organs at risk [OAR]), thereby minimizing tissue toxicity. IMRT is an advanced radiation planning and delivery technique that has shown to be able to achieve a greater therapeutic ratio.Citation10,Citation11 However, IMRT has a few disadvantages: planning time is operator dependent and based on the planner’s experience, treatment time is longer, and in most countries, IMRT represents a more expensive treatment. These disadvantages, despite its proven clinical advantage of a greater therapeutic ratio, have resulted in a slow uptake for IMRT, making conventional radiation therapy (CRT) the more popular choice in most centers.Citation12
IMRT is possible due to advances in multileaf collimator (MLC) technology. Within the linear accelerator collimator head lie multiple leaves whose purpose is to shape the beam. By varying the shape of the beam or the speeds at which the MLC leaves travel, the radiation beam is effectively shaped to vary the dose distribution to the target volume.
Types of breast IMRT techniques
The two common descriptors for IMRT are forward-planning “fields in field” (FP FIF) and inverse planning (IP). The aim of IMRT for breast planning is to achieve dose homogeneity and not organ conformality.Citation13
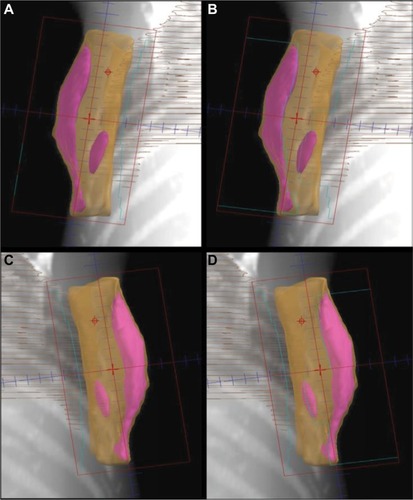
FP FIF IMRT is a technique where limited numbers of MLC segments are determined.Citation14 Beams eye view, when viewed from the radiation beam’s perspective achieved by complex computer algorithm, is utilized to provide a 3D visualization of the isodose distribution from open unmodulated fields (). A limited number of MLC segments with optimal shape and weightings are then determined. These static MLC segments are then delivered sequentially by a step and shoot technique.
Figure 1 Forward-planning “field in field” IMRT technique. A and C demonstrate tangent fields without shielding. B and D demonstrate tangent fields that shielded the volumes receiving ≥110% of the prescribed dose using multileaf collimator.
IP is an IMRT technique that requires contouring of target volumes and OARs.Citation15 This way, a homogenous dose distribution can be achieved and controlled by applying constraints to the target volume and OAR. IP IMRT is often delivered using sliding window dynamic multileaf collimation that allows superior spatial intensity resolution throughout the target volume.Citation15
Both FP FIF and IP IMRT techniques achieve comparable excellent dose distribution.Citation16 The aim of this paper was to evaluate whether IMRT is ready for prime time based on the following three points: 1) workload impact, 2) clinical impact on the patient’s QoL, and 3) appropriateness and applicability to clinical practice.
Workload impact
The efficiency of resources must be ascertained as it impacts the workload and the human resource required. These parameters can be used to compare the impact of CRT and IMRT treatment techniques on resources: 1) time to plan, 2) time to deliver treatment, and 3) time to perform quality assurance (QA).
All planning timings stated in the following excluded contouring timings.
The Cambridge Breast IMRT Trial is a randomized control trial (RCT) comparing 3D or FP FIF IMRT to 2D planning of two-field tangents for 815 randomized patients.Citation17 The median planning time was four times longer for 3D or FP FIF IMRT compared to 2D planning (3D or FP FIF IMRT vs 2D planning: 90 minutes vs 20 minutes). The median treatment time for 3D or FP FIF IMRT compared to 2D tangents was 12.7 minutes and 9.4 minutes, respectively.
Al-Rahbi et alCitation15 compared the planning times of 3D CRT, FP FIF IMRT, and IP IMRT.Citation15 The planning times were 20–30 minutes, 15–20 minutes, and 50–60 minutes, respectively. However, planning times are subjective as it is dependent on dosimetrist’s experience. Treatment delivery timings (inclusive of patient setup) for 3D CRT, FP FIF IMRT, and IP IMRT were 10–15 minutes, 10–15 minutes, and 15–20 minutes, respectively.
A possible explanation of why the planning timings of 3D CRT and IMRT in Al-Rahbi et alCitation15 study is substantially less than the Cambridge Breast IMRT Trial is that breast IMRT planning in the Cambridge Breast IMRT Trial was at its infancy.Citation17 As technology and planning experience matures, planning timings may consequentially be shortened.
IMRT planning has evolved from FP FIF IMRT to hybrid IMRT. Several studies have demonstrated that hybrid IMRT achieved comparable dosimetric outcomes as FP FIF IMRT with comparable treatment planning time.Citation18–Citation21
Descovich et alCitation18 compared a hybrid direct aperture optimized (hDAO) IP IMRT to FP FIF IMRT for WBE-BRT.Citation18 Both hDAO IP IMRT and FP FIF IMRT utilized two tangential beam directions. hDAO IP IMRT plans were inversely optimized and utilized two open fields with eight segments in two tangential beam directions. Both plans achieved comparable breast coverage and OAR sparing. hDAO IP IMRT plans outperformed FP FIF IMRT plans in terms of reduction of breast volume receiving 105% of prescribed dose in the hDAO IP IMRT than in the FP FIF IMRT plans: 25% vs 63% (p = 0.008) for small, 22% vs 57% (p = 0.005) for medium, and 28% vs 53% (p = 0.005) for large breasts. Lumpectomy coverage was marginally better for hDAO IP IMRT compared to FP FIF IMRT (92.4% vs 90.9%). The planning time for hDAO IP IMRT plans was substantially shorter compared to FP FIF IMRT (60–90 minutes vs 20–30 minutes).
Farace et alCitation19 similarly compared tangential and non-tangential beam arrangements for hybrid IP IMRT plans utilizing a semi-automated method and a plan optimization volume set as a target objective during IP.Citation19 The tangential beam arrangement was a four-field technique (two conventional open plus two IP IMRT tangents), and the non-tangential beam arrangement was a six-field technique where two non-tangential (anterior-oblique) IP IMRT beams were added. All dosimetric goals were met; the dosimetry was similar between the tangential and non-tangential beam arrangements and the average planning time was 10 minutes. Both studies demonstrated that the merits of utilizing hybrid IP IMRT lie in its largely automated process while achieving a comparable plan quality to FP FIF IMRT yet reducing planning time, reducing manual process during planning as well as dependence on dosimetrist’s expertise. The limited monitor units (MU) contribution from IP IMRT beams allowed QA to be less taxing compared to full IP IMRT.Citation19 An added advantage of utilizing hybrid IP IMRT is the use of open fields as a main radiation source as this makes planned dosimetry less sensitive to changes in breast shape and setup inaccuracies.Citation22
Overall, utilizing IMRT, regardless of the technique used, lengthens the treatment planning time and QA time required. However, the outcome is a plan with better dosimetry and a more homogenous distribution.
Clinical impact on patient’s QoL
Side effects due to RT affect multiple dimensions of QoL. They cause pain, emotional distress, and affect day-to-day functioning.Citation23 RCTs of FP FIF IMRT vs conventional tangents for breast cancer demonstrated that plans with improved dosimetry correlate with reduced skin toxicities that directly affect cosmesis, pain, and QoL.Citation10,Citation24–Citation26
The Royal Marsden trial is a prospective RCT that compared the 2D standard tangents of FP FIF IMRT.Citation25 Three hundred and six women were randomized into FP FIF IMRT (test arm) or 2D standard tangents (control arm) after BCS. All were prescribed WBEBRT with 50 Gy followed by 10 Gy electron boost. The endpoints included breast cosmesis, pain, and QoL. This trial found that greater normal tissue changes were correlated to increasing breast size and distortion of breast shape post-surgery, which resulted in greater dose inhomogeneity. However, dose homogeneity was improved with FP FIF IMRT. 2D standard tangents had greater dose inhomogeneity with a larger proportion of dose exceeding 110% compared to FP FIF IMRT technique. This was found to correlate with a higher incidence of late adverse events for 2D standard tangents compared to FP FIF IMRT technique.
When comparing the proportion of patients showing changes in breast appearance at 1, 2, and 5 years after randomization by maximum dose absorbed by breast, there was a significant difference in the type of breast changes with the absence or presence of doses exceeding 105%. Sections of breast exceeding 105% dose were 1.9 times (95% confidence interval [CI] 1.3–2.9, p = 0.002) more likely to have breast changes than sections not exceeding 105% dose. After adjusting for the 2D standard tangents, the absence or presence of doses >105% and its correlation to breast change remained significant (p = 0.030) with odds ratio (OR) of 2.6 (95% CI 1.1–6.0). However, the significant treatment effect, that is dependent on the technique used, disappeared. This validates the rationale for correlating the statistical difference in incidence of the endpoints of the two techniques to dosimetry. It also validates the relationship between dosimetry and treatment effects and demonstrates that the more the changes, the longer the follow-up. The results favor FP FIF IMRT.
The Canadian Phase III multicenter trial is another prospective RCT with a similar design and prescription. However, this trial included and stratified all breast sizes – small, medium, and large.Citation26
The trial arm was FP FIF IMRT, and the control arm was standard conventional tangents. Endpoints were acute skin reaction, pain, and QoL. The Canadian trial demonstrated that FP FIF IMRT significantly improved dosimetry. This correlated to a lower proportion of patients experiencing moist desquamation (FP FIF IMRT vs standard treatment: 31.2% vs 47.8%, p = 0.002). In a multivariate analysis, smaller breast sizes (p < 0.001) and the use of FP FIF IMRT (p = 0.030) were significantly associated with a decreased risk of moist desquamation. Although the use of FP FIF IMRT did not correlate with pain and QoL, the presence of moist desquamation significantly correlated with pain (p = 0.002) and a reduced QoL (p = 0.003). Updated results on QoL showed that the benefits of IMRT was greatest in older women.Citation27
The Cambridge IMRT trial is a RCT of FP FIF IMRT vs 2D standard tangents for early breast cancer.Citation17 A total of 815 women with inhomogeneity exceeding 107% were randomized. This trial demonstrated that dosimetry for all breast sizes benefits from FP FIF IMRT. In the 5-year follow-up following the Cambridge trial, toxicities such as overall cosmesis, breast shrinkage, and telangiectasia were compared between both arms.Citation28 Univariate analysis reported that FP FIF IMRT arm had fewer suboptimal cosmesis (OR, 0.68; 95% CI 0.48–0.96; p = 0.027) and skin telangiectasia (OR, 0.58; 95% CI 0.36–0.92; p = 0.021). Although breast shrinkage was similar in both arms, the benefit of FP FIF IMRT for overall cosmesis (p = 0.038) and skin telangiectasia (p = 0.031) was significant. These results demonstrate that improved dose homogeneity with simple FP FIF IMRT correlates with a risk reduction of skin telangiectasia and superior overall cosmesis.
To date, there are no RCTs comparing IP IMRT with 3D CRT. However, two separate comparative dosimetric studies – which generated two plans, 3D CRT and IP IMRT, for each computed tomography data set – demonstrated that IP IMRT resulted in superior dose conformity with a larger volume receiving low dose.Citation29,Citation30 Hence, it could be expected that IP IMRT can reduce toxicities and improve overall cosmesis.
Appropriateness and applicability to clinical practice
To ascertain the appropriateness and applicability of breast IMRT as standard clinical practice, the following points should be duly considered ().
Table 1 Summary of the points of comparison between CRT and IMRT
The planning objectives for CRT and IMRT are similar as 95% of the prescribed dose should cover 100% of the target volume and OAR constraints for both techniques must be respected. However, IMRT is more complex as deliberate attempts must be made to reduce dose homogeneity and lower the maximum dose.Citation15,Citation16
In terms of MUs, Al-Rahbi et alCitation15 demonstrated that IP IMRT technique required more MUs compared to 3D CRT and FP FIF IMRT techniques.Citation15 The number of MUs for the FP FIF IMRT technique was four times lesser than that for the IP IMRT technique (293 MU vs 1160 MU), whereas those for the 3D CRT technique was three times lesser (443 MU vs 1160 MU). The number of MU for 3D CRT was higher than that for the FP FIF IMRT technique (443 MU vs 293 MU) because of the use of wedges in the 3D CRT technique. A separate study comparing forward and inverse planning methods demonstrated that IP IMRT required the most number of MUs, as per the following results: CRT using physical wedges: 278 ± 15; CRT using dynamic wedges: 235 ± 10; FP FIF IMRT: 227 ± 9; and IP IMRT: 437 ± 84.Citation31 This inevitably increased treatment time.Citation15,Citation31 Other implications such as higher machine leakage and whole body dose may increase the risk of radiation-induced secondary malignancy.Citation15,Citation31
The literature reports that IMRT requires longer planning time and advanced planning skills.Citation32 Smith et alCitation32 found that CRT required a mean time of 15 minutes compared to 60–90 minutes required by FP FIF IMRT, while Al-Rahbi et alCitation15 reported an average time of 20–30 minutes, 15–20 minutes, and 45–60 minutes for 3D CRT, FP FIF IMRT, and IP IMRT, respectively. It is interesting to note that the planning time for FP FIF IMRT is quartered in Al-Rahbi et al’sCitation15 study. This might be attributed to the fact that as technology matures, the time taken for planning is shortened as the planning system becomes more powerful. Also, compared to 3D CRT and FP FIF IMRT, IP IMRT requires patient-specific QA measurements.Citation15 This additional QA time must be taken into account when measuring the total workload per plan. Compared to the IP IMRT and 3D CRT plans, the higher-quality FP FIF IMRT plans are likely to be generated in a shorter time without requiring a high level of planning ability.Citation15
An earlier concern with breast IMRT is its susceptibility to intrafraction movement during treatment and breast shape changes due to the interplay between MLC and respiratory motion during treatment and the breast shape, respectively.Citation33 However, it is interesting to note that both an early study by George et alCitation33 and a separate study by Jain et alCitation34 demonstrated no statistically significant differences between the planned and expected dose distributions in any phase of the respiratory cycle during treatment suggesting that breast deformity and intrafraction movement have limited impact.Citation33,Citation34
Another advantage of IMRT is that a simultaneous integrated boost dose (SIB) can be delivered simultaneously compared to the widely used sequential electron boost. Improvements in skin sparing, cosmesis, and dose conformality are expected. This is especially useful for deep-seated boost volumes. Total dose and dose per fraction to OAR are also decreased. This also shortens the overall treatment time for patients and reduces planning workload. However, SIB can only be achieved with IP IMRT.Citation35,Citation36
Discussion
IMRT is gaining widespread acceptance across many centers. Resource limitation is a concern that may hinder the adoption of IMRT. Hence, selecting the planning technique is often a trade-off among four factors: 1) plan quality; 2) time, expertise, and effort to generate a plan; 3) need for QA; and 4) beam on time. As early-stage breast cancer makes up the bulk of patient proportion in a typical radiotherapy center, any increase in treatment complexity will affect resource allocation. A systematic review by Chen et alCitation37 found a relative risk of 1.11 (95%CI 1.04–1.19) of local recurrence per month of waiting time for postoperative RT for breast cancer.Citation37 Thus, it could be inferred that treatment delay as a result of more complex planning techniques could pose a risk for patients.
This is especially relevant to IP IMRT as it requires physics QA of the MU calculation, deliverability, and linear accelerator (linacs), which adds a strain to physics resources and may limit linacs that can be used for these treatments too.
Although the literature suggests that IMRT allows the rational use of current resources with a slight increase in planning expertise, it remains unlikely that every patient requires IMRT, both IP and FP FIF. This necessitates the judicious selection of breast cancer patients who would most benefit from IMRT. This may help mitigate the impact on clinic resources.
Conclusion
The merit of breast IMRT is well documented. However, the routine application of breast IMRT has to be wisely considered. Conventional tangent for WBEBRT remains simple and effective. Advanced technology such as IMRT, albeit with homogeneity and toxicity benefits, may further strain the health care system already fraught with limited clinical resources and time constraints. This is especially relevant for breast RT that represents a substantial portion of a typical radiation oncology center.
The definition of IMRT for breast remains ambiguous. It is imperative that a clear distinction should be made between FP FIF IMRT and IP IMRT. The distinct difference is that FP FIF IMRT, although popularly termed IMRT, should be more accurately defined “field in field” 3D CRT (FIF 3D CRT). These two different descriptors essentially refer to the same technique that shares the same goal of achieving dose homogeneity within the breast to reduce skin toxicities, thereby preserving or improving cosmesis. The secondary goal is for better OAR sparing especially for the heart in left breast cancer patients.
Both patients and physicians alike can be misled that IP IMRT is superior to FP FIF IMRT, which is essentially FIF 3D CRT. The medical literature does not support this. While IP IMRT provides superior outcomes for other sites, IP IMRT for breast RT is not routinely advantageous compared to FIF 3D CRT. However, IP IMRT can be a useful tool for women with atypical anatomy such as severe pectus excavatum.Citation38 Although IMRT for early-stage breast cancer is ready for prime time, incorporating IP IMRT as standard practice is not recommended as it does not always improve dose homogeneity or patient outcomes. Rather, the judicious selection of each technique’s dosimetric advantage and treatment efficacy should be matched with the patient’s characteristics.
Disclosure
The authors report no funding sources and no conflicts of interest in this work.
References
- WHOFact Sheets by Cancer Available from: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspxAccessed April 12, 2016
- American Cancer SocietyRadiation for Breast Cancer2016 Available from: http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-treating-radiationAccessed November 7, 2016
- OnitiloAAEngelJMStankowskiRVDoiSASurvival comparisons for breast conserving surgery and mastectomy revisited: community experience and the role of radiation therapyClin Med Res2015132657325487237
- DarbySMcGalePCorreaCEarly Breast Cancer Trialists’ Collaborative Group (EBCTCG)Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trialsLancet201137898041707171622019144
- KanapuruBErshlerWBHesdorfferCJemalAYatesJWLong-term survival of older breast cancer patients: population-based estimates over three decadesBreast Cancer Res Treat2012134285385722710707
- FisherJScottCStevensRRandomized phase III study comparing best supportive care to biafine as a prophylactic agent for radiation-induced skin toxicity for women undergoing breast irradiation: radiation therapy oncology group (RTOG) 97-13Int J Radiat Oncol Biol Phys20004851307131011121627
- KronTChuaBRadiotherapy for breast cancer: how can it benefit from advancing technology?Euro Med J201428390
- StefanovskiZSmichkoskaSPetrovaDLazarovaEAdvantages of the technique with segmented fields for tangential breast irradiation20167578 Available from: https://inis.iaea.org/search/search.aspx?orig_q=RN:45026292Accessed April 13, 2016
- Afkhami-ArdakaniMEsfahaniMNourollahiYAshuri-TaziyaniYHagh-ParastMAssessment of the effect of breast size on dose distribution for 3D and conventional methods with TLD dosimetry in breast phantoms2015 Available from: http://fbt.tums.ac.ir/index.php/fbt/article/view/39/36Accessed November 8, 2016
- HarsoliaAKestinLGrillsIIntensity-modulated radiotherapy results in significant decrease in clinical toxicities compared with conventional wedge-based breast radiotherapyInt J Radiat Oncol Biol Phys20076851375138017544598
- ViciniFASharpeMKestinLOptimizing breast cancer treatment efficacy with intensity-modulated radiotherapyInt J Radiat Oncol Biol Phys20025451336134412459355
- WangEHMougalianSSSoulosPRAdoption of intensity modulated radiation therapy for early-stage breast cancer from 2004 through 2011Int J Radiat Oncol Biol Phys201591230331125442334
- McCormickBHuntMIntensity-modulated radiation therapy for breast: is it for everyone?Semin Radiat Oncol2011211515421134654
- OzyigitGCurrent role of modern radiotherapy techniques in the management of breast cancerWorld J Clin Oncol20145342543925114857
- Al-RahbiZSAl MandhariZRavichandranRDosimetric comparison of intensity modulated radiotherapy isocentric field plans and field in field (FIF) forward plans in the treatment of breast cancerJ Med Phys2013381222923531607
- NguyenSCaoFRamaseshanRTemplate-based breast IMRT planning for increased workload efficiencyRadiat Oncol201386723514439
- BarnettGCWilkinsonJMoodyAMA randomised controlled trial of forward-planned radiotherapy (IMRT) for early breast cancer: baseline characteristics and dosimetry resultsRadiother Oncol2009921344119375808
- DescovichMFowbleBBevanASchechterNParkCXiaPComparison between hybrid direct aperture optimized intensity-modulated radiotherapy and forward planning intensity-modulated radiotherapy for whole breast irradiationInt J Radiat Oncol Biol Phys2010761919919395189
- FaracePZuccaSSollaIPlanning hybrid intensity modulated radiation therapy for whole-breast irradiationInt J Radiat Oncol Biol Phys2012841e115e12222543199
- FongABromleyRBeatMVienDDineleyJMorganGDosimetric comparison of intensity modulated radiotherapy techniques and standard wedged tangents for whole breast radiotherapyJ Med Imaging Radiat Oncol2009531929919453534
- MayoCSUrieMMFitzgeraldTJHybrid IMRT plans—concurrently treating conventional and IMRT beams for improved breast irradiation and reduced planning timeInt J Radiat Oncol Biol Phys200561392293215708276
- van MourikAvan KranenSden HollanderSSonkeJJvan HerkMvan Vliet-VroegindeweijCEffects of setup errors and shape changes on breast radiotherapyInt J Radiat Oncol Biol Phys20117951557156420933341
- SchnurJBOuelletteSCDilorenzoTAGreenSMontgomeryGHA qualitative analysis of acute skin toxicity among breast cancer radiotherapy patientsPsychooncology201120326026820238306
- BarnettGCWilkinsonJSMoodyAMRandomized controlled trial of forward-planned intensity modulated radiotherapy for early breast cancer: interim results at 2 yearsInt J Radiat Oncol Biol Phys201282271572321345620
- DonovanEBleakleyNDenholmEBreast Technology GroupRandomised trial of standard 2D radiotherapy (RT) versus intensity modulated radiotherapy (IMRT) in patients prescribed breast radiotherapyRadiother Oncol200782325426417224195
- PignolJPOlivottoIRakovitchEA multicenter randomized trial of breast intensity-modulated radiation therapy to reduce acute radiation dermatitisJ Clin Oncol200826132085209218285602
- MukeshMBQianWWilkinsonJSPatient reported outcome measures (PROMs) following forward planned field-in field IMRT: results from the Cambridge Breast IMRT trialRadiother Oncol2014111227027524746570
- MukeshMBBarnettGCWilkinsonJSRandomized controlled trial of intensity-modulated radiotherapy for early breast cancer: 5-year results confirm superior overall cosmesisJ Clin Oncol201331364488449524043742
- HaciislamogluEColakFCanyilmazEDosimetric comparison of left-sided whole-breast irradiation with 3DCRT, forward-planned IMRT, inverse-planned IMRT, helical tomotherapy, and volumetric arc therapyPhys Med201531436036725733372
- SmallKKellyCBeldham-CollinsRGebskiVWhole breast and excision cavity radiotherapy plan comparison: conformal radiotherapy with sequential boost versus intensity-modulated radiation therapy with a simultaneously integrated boostJ Med Radiat Sci2013601162426229603
- Al-RahbiZSRavichandranRBinukumarJPDavisCASatyapalNAl-MandhariZA dosimetric comparison of radiotherapy techniques in the treatment of carcinoma of breastJ Cancer Ther20134111017
- SmithWMenonGWolfeNPloquinNTrotterTPudneyDIMRT for the breast: a comparison of tangential planning techniquesPhys Med Biol20105541231124120124651
- GeorgeRKeallPJKiniVRQuantifying the effect of intrafraction motion during breast IMRT planning and dose deliveryMed Phys200330455256212722807
- JainPMarchantTGreenMInter-fraction motion and dosimetric consequences during breast intensity-modulated radiotherapy (IMRT)Radiother Oncol2009901939819012980
- AlfordSLPrassasGNVogelesangCRLeggettHJHamiltonCSAdjuvant breast radiotherapy using a simultaneous integrated boost: clinical and dosimetric perspectivesJ Med Imaging Radiat Oncol201357222222923551785
- AskoxylakisVJensenADHäfnerMFSimultaneous integrated boost for adjuvant treatment of breast cancer—intensity modulated vs. conventional radiotherapy: the IMRT-MC2 trialBMC Cancer20111124921676232
- ChenZKingWPearceyRKerbaMMackillopWThe relationship between waiting time for radiotherapy and clinical outcomes: a systematic review of the literatureRadiother Oncol200887131618160158
- TehBSLuHHSobremonteSThe potential use of intensity modulated radiotherapy (IMRT) in women with pectus excavatum desiring breast-conserving therapyBreast J20017423323911678800