
Abstract
Patients with triple-negative breast cancer (TNBC) have a considerably less favorable prognosis than those with hormone-positive breast cancers. TNBC patients do not respond to current endocrine treatment and have a 5-year survival prognosis of <30%. The research presented here is intended to fill a void toward the much needed development of improved treatment strategies for metastatic TNBC. The overall goal of this research was to evaluate the effectiveness of reconstituted high-density lipoprotein (rHDL) nanoparticles (NPs) as delivery agents for anti-TNBC drugs. Using lapatinib and valrubicin as components of the rHDL/drug complexes resulted in a significantly better performance of the NP-transported drugs compared with their free (unencapsulated) counterparts. The enhancement of the therapeutic effect and the protection of normal cells (cardiomyocytes) achieved via the rHDL NPs were likely due to the overexpression of the high-density lipoprotein (HDL) (scavenger receptor class B type 1 [SR-B1]) receptor by the TNBC cells.
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Cancer continues to be a major health challenge causing the second highest number of fatalities in the US. Breast cancer (BC) cases may be classified into three major groups, estrogen receptor positive (ER+), estrogen receptor negative (ER−), and human epidermal growth factor receptor 2 positive (HER2+) – either ER- or ER+.Citation1,Citation2 Those BC tumors that do not express any of these molecular biomarkers are termed triple-negative breast cancer (TNBC), a high-grade, highly proliferative, metastatic disease that does not respond to established endocrine therapy.Citation3 Although 15%–20% of all BC cases are of the TNBC subtype, this form of the disease accounts for a disproportionately high number of cancer deaths.Citation3,Citation4 TNBC is frequently associated with a poor prognosis, primarily as the result of recurrence and visceral and brain metastases within the first 5 years of the initial diagnosis.Citation5–Citation8 Although TNBC patients tend to initially respond to chemotherapy, their overall response to treatment is poor in comparison to HER2-positive patients.Citation9 The preferred treatment for women with early-stage or locally advanced TNBC is taxane based or anthracycline regimens because these agents are associated with high rates of complete response.Citation10 Despite their effectiveness against various types of tumors, the use of anthracyclines in chemotherapy is limited due to their intense cardiotoxicity.Citation11 For patients with metastatic disease, sequential single agents or combination therapies have been used; however, no single approach has so far resulted in improved survival.Citation12 Developing multidrug resistance (MDR) by TNBC tumors has been one of the major reasons for unsuccessful chemotherapy.Citation13,Citation14
As an alternative to traditional therapy, nanoparticles (NPs) provide an effective mechanism for drug delivery to malignant cells and tumors by limiting off-target effects that damage healthy tissues.Citation15 NPs are anticipated to increase the therapeutic index of anti-cancer agents by prolonging circulating half-life, increasing drug accumulation in the tumor, and reducing the risk of off-target effects.Citation15 In addition to the above-listed advantages, NPs have been found to be highly effective as drug delivery vehicles by enhancing the efficacy of several drugs via active targeting and thus allowing the drugs to escape efflux pumps associated with drug resistance.Citation16,Citation17
Our laboratory has developed reconstituted high-density lipoprotein (rHDL) NPs for the purpose of improved drug deliveryCitation18–Citation21 to malignant cells and tumors.Citation18–Citation22 High-density lipoproteins (HDLs) are endogenous cholesterol transporters. Their physicochemical properties and targeted delivery of their core components (including drugs) make them ideal transporters of anti-cancer agents.Citation23 The advantages of using rHDL NPs over most of the other drug delivery systems include their small size (>20 nm diameter), long circulation time, biocompatibility,Citation23 absence of immunogenic response, and their capability for tumor-selective delivery of the drug payload. This drug delivery strategy also seems superior to liposomal approaches because of the much smaller size of rHDL NPs and the scavenger receptor class B type 1 (SR-B1) receptor-mediated, tumor-selective delivery of their payload.Citation22
It has been hypothesized that because cancer cells proliferate faster than normal cells, they may have a higher need for cholesterol than normal cells.Citation24 Earlier studies, in fact, revealed that cancer cells show enhanced proliferation in the presence of added HDL.Citation25 One way cancer cells may acquire the excess cholesterol needed for growth is by the overexpression of the HDL receptor or SR-B1.Citation26,Citation27 Most cancer cells studied have been reported to overexpress the SR-B1 protein.Citation22,Citation28 Recently, Yuan et al showed that 54% of malignant breast tumors had a high expression of the SR-B1 receptor. The great majority of the SR-B1-overexpressing tumor samples were obtained from TNBC patients.Citation29 Yuan et alCitation29 also developed a prediction algorithm that indicated a poorer outcome for BC patients whose tumors showed a high expression of the SR-B1 receptor. Using MDA-MB-231 TNBC cells, Danilo et alCitation26 found that migration can be induced by the addition of HDL3 to the culture medium. The studies of Danilo et al also revealed that these effects could be attenuated via the knockdown of SR-B1. These data suggest that SR-B1 is an important factor in malignancy as it promotes the survival and metastatic activity of cancer cells and tumors, including those associated with BC.
The present study was aimed to evaluate the use of rHDL-mediated drug delivery that takes advantage of the SR-B1 gateway to TNBC cells and tumors.Citation30 This “Trojan Horse” strategyCitation18 has proven effective for a number of malignant cells;Citation18–Citation21 therefore, it is anticipated to provide a foundation for the development of novel therapeutic approaches for TNBC.
Materials and methods
Cell culture and chemicals
MDA-MB-231 (TNBC) and H9C2 (cardiomyocyte cells; ATCC, Manassas, VA, USA) were grown in 75 cm2 flasks containing Dulbecco’s Modified Eagle Medium (DMEM) high-glucose media with phenol red (Thermo Fisher Scientific, Waltham, MA, USA) supplemented with 10% fetal bovine serum (FBS; HyClone, Logan, UT, USA) incubated at 37°C in a humidified incubator at 5% CO2. Stock solutions of valrubicin (China Kouting Group Ltd., Shenzhen, China) at 50 mg/mL and lapatinib at 25 mg/mL (Selleck Chemicals, Houston, TX, USA) were prepared in dimethyl sulfoxide (DMSO) and kept at −20°C.
Preparation of drug containing rHDL NPs
A mixture of egg yolk phosphatidylcholine (PC; 7.5 mg/mL), free cholesterol (FC; 0.175 mg/mL), and cholesteryl oleate (CE; 0.075 mg/mL) was pipetted into a glass vial from respective stocks in chloroform, and the chloroform was subsequently evaporated under nitrogen gas to form a thin film inside the vial. The drugs (lapatinib or valrubicin) were added at a concentration of 1 mg/mL to the lipids, followed by 30 µL DMSO and apo A-I (2.5 mg/mL; MCLAB, San Francisco, CA, USA), and mixed thoroughly by vortexing. To this mixture, 7 mg/mL sodium cholate was added (from a stock of 100 mg/mL), and the preparation was made up to a final volume of 1 mL by adding a buffer solution (10 mM Tris, 0.1 M KCl, 1 mM EDTA, pH 8.0). The sample was then frozen at −80°C overnight. Subsequently, the NP preparation was lyophilized, redissolved in water, and dialyzed against 2 L of phosphate-buffered saline (PBS) for 48 hours. After dialysis, the preparations were centrifuged at 3300 ×g for 1 minute, and the supernatant was collected. The NP preparation was then syringe filtered through a 0.45 µm pore filter (EMD Millipore, Billerica, MA, USA). The preparations were kept at 4°C until used.
Determination of drug entrapment efficiency (DEE)
Entrapment efficiency was determined as reported previously.Citation20 Briefly, entrapment efficiency was determined by measuring the amount of initial (before dialysis) and final (after filtration) drug concentrations. In a 96-well plate, series of dilutions of rHDL–valrubicin NPs and rHDL–lapatinib NPs were prepared using PBS with 1% triton, and the absorbance was read at 490 nm. rHDL–lapatinib NPs were mixed with PBS in the presence of 1% Triton X-100, and the absorbance was read at 490 or 362 nm for valrubicin and lapatinib, respectively. The respective drug concentrations were extrapolated using a standard graph for each drug.
Preparation of rHDL/H-cholesteryl oleate complex
A mixture of egg yolk PC in chloroform with labeled cholesterol oleate and CE was prepared with a molar ratio of apo A-1:FC:CE:PC = 1:5:1.3:1.15. Chloroform was evaporated from PC, CE, and CE under nitrogen gas to a thin film and rehydrated in 60 µL DMSO for a 2 mL preparation. To this mix, apo A-I (2.5 mg/mL) and 140 µL sodium cholate (from a stock of 100 mM) were added with sodium cholate buffer (10 mM Tris, 0.1 M KCl, and 1 mM EDTA, pH 8.0) to make a volume of 2 mL. The cholate/lipid/protein mixture was then frozen in the −80°C freezer overnight. Preparations were then dialyzed for 48 hours against 2 L of PBS, with three buffer changes during the first 6 hours. After dialysis, the preparations were centrifuged at 3300 ×g for 1 minute and kept at 4°C until used.
Determination of chemical composition of the rHDL NPs
Pierce BCA protein assay kit (Thermo Fisher Scientific) was used to determine protein concentration. The amounts of cholesterol and phospholipid contained in the NPs were determined by respective enzymatic reagent kits (cholesterol E and phospholipid C; Wako Chemicals, Richmond, VA, USA) using microtiter plate assays as per manufacturer’s suggestions. All assays were read on the PowerWave 340 microplate reader (BioTek Instruments, Winooski, VT, USA) at the appropriate wavelength.
Particle diameter measurements
rHDL/valrubicin and rHDL/lapatinib NP size estimations were performed using dynamic light scattering (DLS) carried out using a Nanotrac system (Microtrac Inc., Montgomeryville, PA, USA) as per manufacturer’s instructions. rHDL/lapatinib NP size was also established by transmission electron microscopy (TEM). Following dialysis in a volatile buffer (0.125 M ammonium acetate, 2.6 mM ammonium carbonate, 0.26 mM EDTA, pH 7.4), the isolated rHDL samples were negatively stained with 2% sodium phosphotungstate, pH 7.2, and placed on formvar/carbon-coated 200 mesh nickel grid support films (Ted Pella Inc., Redding, CA, USA) as previously described.19 The particles were visualized using a magnification of 50,000 on a Zeiss 910 transmission electron microscope (Carl Zeiss, Thornwood, NY, USA).
Determination of IC50 by cytotoxicity assay
The impact of valrubicin and lapatinib on the viability of normal and cancer cells was estimated using the cell counting kit-8 (CCK-8; Dojindo Molecular Technologies, Gathesburg, MD, USA). H9C2 and MDA-MB-231 cells (6000 cells/well) were seeded into 96-well microtiter plates and incubated at 37°C in 5% CO2 atmosphere overnight. Free drug formulations were diluted in serum-free media to yield the concentrations (2–8 µM). After incubation, 10 µL of a tetrazolium salt, 2-(2-methoxy-4-nitrophenyl)-3-(4-nitrophenyl)-5-(2,4-disulfophenyl)-2H-tetrazolium (WST-8; monosodium salt), stock solution was added to all wells. The reagent was thoroughly mixed. After a 3-hour incubation period, the absorbance at 450 nm was read using a PowerWave 340 microplate reader. There were four replicates for each concentration. Each experiment was repeated at least three times.
Flow cytometry analysis of SR-B1 expression
A total of 750,000 cells were plated and cultured in a 100 mm Petri dish. Cells were collected and washed with 1× PBS twice, followed by a wash with staining buffer (1× PBS, 2% FBS, 0.1% sodium azide). Next, cells were seeded in a 96 round-bottom plate at 1 × 106 cells/well. Cells were blocked with anti-goat serum for 30 minutes at room temperature and then treated with 1:50 dilution of SR-B1 rabbit-anti-human monoclonal antibody (Abcam, Cambridge, MA, USA) in staining buffer for 30 minutes at room temperature. Cells were then washed in staining buffer for two times, followed by incubation with the secondary goat anti-rabbit Alexa Fluor 488-conjugated antibody at 1:2000 dilution for 30 minutes in the dark. Cells were pelleted and washed in staining buffer. Cells were acquired using the Cytomics FC 500 Cytometer and analyzed by CXP2.1 software (Beckman Coulter, Brea, CA, USA).
Confocal microscopy
MDA-MB-231 cells (7.5 × 104/well) were seeded onto poly-lysine-coated 12 mm coverslips (Corning Inc., Corning, NY, USA) in a six-well plate (Thermo Fisher Scientific) and incubated overnight at 37°C in an atmosphere of 5% CO2. Cells were pretreated with 0.05 mg/mL of the block lipid transporter-1 (BLT-1; Sigma-Aldrich, St. Louis, MO, USA) or SR-B1 antibody (1:50 dilution) for 30 minutes. After pretreatment, the cells were treated with rHDL–valrubicin (8 µM) or free valrubicin at 8 µM concentration and incubated at 37°C with serum-free media for 3 hours. Cells were then washed three times with PBS containing 1% FBS. The coverslip (with the attached MDA-MB-231 cells) was removed from the six-well plate and mounted on microscope slides with 4,6-Diamidino-2-phenylindole, dihydrochloride (DAPI) antifade mounting serum (Molecular Probes, Eugene, OR, USA). The Zeiss LSM 510 microscope was used to obtain the confocal image of the cells at 40× magnification, at excitation/emission wavelengths of 488/518 nm for SR-B1, 488/561 nm for valrubicin, 405/461 nm for DAPI, and 650/668 nm for actin phalloidin.
Statistical analysis
All experimental data were obtained by calculating the mean value derived from five independent measurements. p-values were calculated at a 95% confidence interval and were considered statistically significant when <0.05. Differences in cell viability IC50 values were evaluated using the GraphPad Prism software (GraphPad Software Inc., La Jolla, CA, USA). The unpaired two-tailed Student’s t-test was used to determine the significance of IC50 values between cell viability tests. Cell survival data were expressed as mean ± standard deviation. The paired Student’s t-test was used to assess the difference in the radioactivity uptake by MBA study for assessing SR-B1 functionality. ImageJ software (Wayne Rasband, National Institutes of Health, Bethesda, MD, USA) was used to determine the fluorescence intensity of the confocal images. Fluorescence intensity was displayed as corrected total cell fluorescence (CTCF). The Student’s t-test was used to compare the differences in fluorescence intensity in valrubicin–rHDL-treated TNBC cells vs free valrubicin treatment.
Results
Characterization of the valrubicin containing rHDL NPs
Valrubicin was incorporated into rHDL NPs using the procedure described earlier. The overall chemical composition of the rHDL–valrubicin NPs showed that the percentage of protein, phospholipid, cholesterol, and drug was 28.36%, 60.77%, 1.14%, and 9.72%, respectively (). The percentage chemical composition of these particles resembled that of native circulating HDL.Citation20 Data from DLS demonstrated that the formulation was reasonably homogeneous with the majority of the NPs showing an average diameter of 48.1 ± 6.1 nm (). These observations confirmed earlier findings regarding the size of the NPsCitation20 and were observed to be within the acceptable range for NPs to penetrate the tumor microenvironment.Citation31 The analysis of surface properties of rHDL–valrubicin NPs exhibited zeta potential of −6.43 ± 2.6 ().
Figure 1 Particle size measurement by DLS and TEM.
Abbreviations: rHDL, reconstituted high-density lipoprotein; NP, nanoparticle; DLS, dynamic light scattering; TEM, transmission electron microscopy.
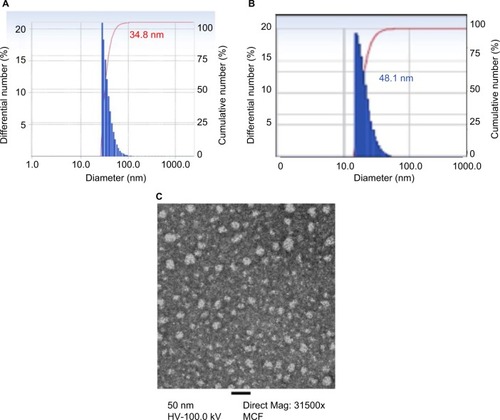
Table 1 Chemical composition of the lapatinib containing rHDL NPs
Characterization of lapatinib containing rHDL NPs
The chemical composition of the lapatinib containing rHDL NPs is shown in and . The NP components were determined by respective analyses as described in the “Materials and methods” section. The relative drug incorporation (19% for lapatinib) is one of the highest observed in our experience with several drug payloads.Citation19–Citation21 The lapatinib–rHDL NPs were found to have a mean diameter of 34.8 ± 3.6 nm, assessed via DLS (), and a zeta potential of −8.8 ± 2.6 mV. Not surprisingly, the molecular diameter of the lapatinib-containing rHDL NPs was found to be considerably smaller (<20 nm; ) when examined by TEM compared to the value yielded via DLS measurements (). We have consistently observed this trend with our rHDL NPs.
Assessment of the cytotoxicity of valrubicin and lapatinib formulations
To determine the effectiveness of valrubicin and lapatinib as free drugs vs drugs containing rHDL NPs, cell viability assays were performed. Because anthracyclines are known to be cardiotoxic, the impact of the valrubicin formulations on cardiomyocytes (H9C2) was also assessed. Untreated cells were used as controls. The cell viability was determined over a 72-hour period using a CCK-8 kit as described in the “Materials and methods” section. The results of the cell viability assays for the free (unencapsulated) and the rHDL–valrubicin-treated TNBC (MB-MDA23) cells are shown in . The regression lines () and the calculated IC50 values () indicate that the rHDL/valrubicin formulation is more toxic toward TNBC cells than the free drug. Accordingly, the IC50 value for rHDL–valrubicin vs valrubicin was 2.3 ± 0.14 µM and 3.45 ± 0.19 µM, respectively. Similar assays performed with the H9C2 (cardiomyocyte) cell line () gave rise to an exactly opposite trend (). Here, the free drug was considerably more effective in killing the cells (IC50 = 4.39 ± 0.39 µM) than the rHDL–valrubicin formulation (IC50=7.53 ± 0.10 µM).
Figure 2 Assessment of (A) the impact of free valrubicin vs valrubicin incorporated into rHDL NPs on MDA-MB-231 (TNBC) cells and (B) cytotoxicity of free lapatinib vs rHDL–lapatinib against TNBC cells.
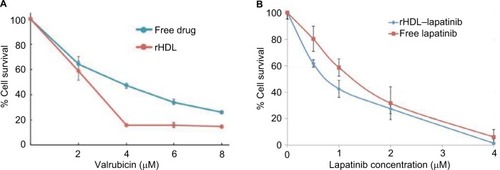
Figure 3 Assessment of the impact of (A) free valrubicin vs valrubicin incorporated into rHDL NPs on H9C2 (cardiomyocyte) cells and (B) free lapatinib vs lapatinib incorporated into rHDL NPs on H9C2 (cardiomyocyte) cells.
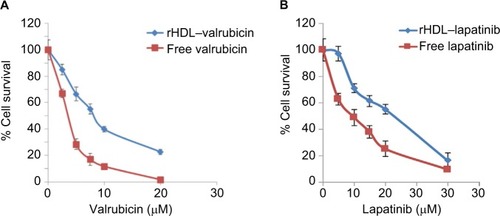
Table 2 Cytotoxicity of valrubicin vs rHDL–valrubicin against TNBC cells (MB-MDA231) and cardiomyocytes (H9C2)
The broadening of the therapeutic window due to the incorporation of valrubicin into rHDL NPs was calculated using the formula shown as follows:
This formula yields the following relationship:
Accordingly, the therapeutic enhancement of valrubicin against TNBC cells resulting from the incorporation of the drug into rHDL NPs was ~2.5 fold. These findings indicate potential benefits for TNBC chemotherapy by limiting or avoiding off-target toxicity of the anti-cancer agent due to formulating it with rHDL.
Cytotoxicity of lapatinib against TNBC (MDA-MB-231) cells
The cytotoxicity studies involving lapatinib were conducted in a manner similar to those with valrubicin (). The data shown in indicate that the rHDL–lapatinib NPs are more effective against TNBC cells (IC50 = 0.78 ± 0.04 µM) than the free drug (IC50 = 1.40 ± 0.59 µM). When the rHDL–lapatinib formulation was used against H9C2 cells, the free lapatinib had IC50 values that were less than half (9.68 ± 3.4) than those of rHDL–lapatinib (>20 nM) as shown in . Overall, the rHDL–lapatanib formulation had a protective effect against cardiomyocytes as indicated in . When the abovementioned formula Equation(2)(2) was applied to calculate the expanding of the therapeutic window via formulating lapatinib with rHDL NPs, the therapeutic enhancement was estimated to be approximately fourfold for rHDL–lapatinib vs free lapatinib.
Table 3 Cytotoxicity of lapatinib vs. rHDL–lapatinib against TNBC cells (MDA-MB-231) and cardiomyocytes (H9C2)
Role of the SR-B1 receptor in delivering anti-cancer agents to TNBC cells
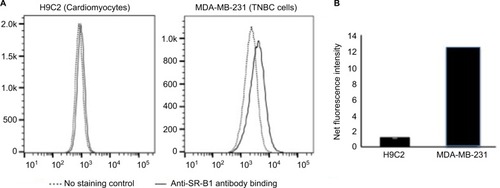
Northern blot analyses of cancer cell lines revealed that the TNBC cells (MDA-MB-231) showed a high expression of the SR-B1 receptor.Citation22 However, because mRNA levels do not always correlate strictly with expressed protein levels and protein function, therefore, flow cytometry was used to determine the SR-B1 protein expression levels in TNBC and cells (MDA-MB-231) and a cardiomyocyte cell line (H9C2; ). In , the dotted line represents the level of autofluorescence that the cells emit naturally, while the solid line represents the mean fluorescence intensity, indicating the level of SR-B1 protein expression by the respective cells. The amount of SR-B1 protein can be estimated by assessing the shift in fluorescence intensity (to the right). In , the cardiomyocytes show almost no shift in fluorescence intensity, while the MDA-MB-231 cell line does show a significantly higher shift (t = 17.26; p < 0.01), indicating that the TNBC cell line, unlike the cardiomyocytes, robustly expresses the SR-B1 protein.
Figure 4 Flow cytometry analysis of SR-B1 expression in malignant vs normal cells.
Abbreviations: SR-B1, scavenger receptor class B type 1; TNBC, triple-negative breast cancer.
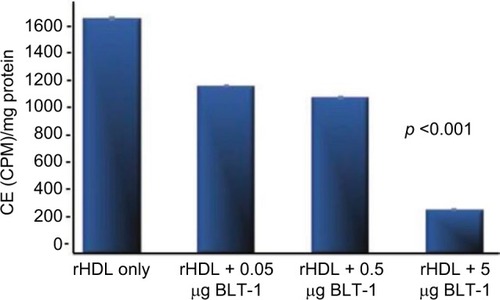
To further validate the role of the SR-B1 as a gateway for anti-cancer drug delivery to TNBC cells, the functional capabilities of this receptor were assessed. 3H-cholesteryl oleate was incorporated into rHDL NPs, as described in the “Materials and methods” section. MDA-MB-231 cells were incubated with the radioactively labeled rHDL NPs in the presence and absence of an SR-B1 inhibitor (BLT-1). The findings show a nearly complete inhibition of the cholesteryl oleate uptake by the MDA–MB-231 cells in the presence of the highest concentration of BLT-1, apparently blocking the function of the SR-B1 receptor ().
Figure 5 Radioactive CE uptake from rHDL in the presence of a chemical inhibitor BLT-1 by MDA-MB-231 cells (n = 4/dose).
Confocal microscopy studies for the validation of the SR-B1 drug delivery model
To investigate the rHDL drug delivery mechanism, further confocal images were taken of rHDL–valrubicin-treated MDA-MB-231 cells vs free drug-treated cells. Before taking confocal images of treated MDA-MB-231 cells, a confocal image of the untreated cell line was taken as a control (data not shown). Here, the cells were stained for F-actin (magenta). The image demonstrates the epithelial-to-mesenchymal transition (EMT), a spindle-like shape of the cells. An image of MDA-MB-231 cells after being treated with the free drug (valrubicin) and the rHDL–valrubicin preparation (8 µM) for a 3-hour period is depicted in . The fluorescent intensity of the cells was measured using the ImageJ software. The fluorescence intensity is a measure of the amount of drug that has entered the cell. There was a significantly higher fluorescence intensity observed in the rHDL-treated cells than in the cells treated with the free drug (t = 3.45, p < 0.05), indicating that significantly more drug accumulated within the cell when treated with rHDL–valrubicin vs those treated with the free drug.
Figure 6 Confocal microscopey images of valrubicin treated MDA-MB-231 cells.
Abbreviations: rHDL, reconstituted high-density lipoprotein; CTCF, corrected total cell fluorescence.

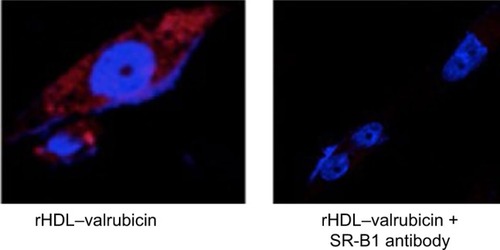
To investigate that the rHDL NPs are specifically interacting with the SR-B1 receptor, a chemical inhibitor of the receptor, BLT-1, was used. Subsequently, the cells were also treated with rHDL–valrubicin () or the free drug () at 8 µM concentration. After 3 hours, the cells were washed, and confocal images were taken. The data in show that the capacity of the rHDL–valrubicin-treated cells for drug uptake was significantly reduced in the presence of the BLT-1 inhibitor (p < 0.01). depicts the inhibition-free valrubicin uptake by MDA-MB-231 cells in the presence of the BLT-1 inhibitor. The data show () that the BLT-1 (SR-B1) inhibitor had little or no effect on the uptake of free (unencapsulated) valrubicin by the MDA-MB-231 cells, as indicated by the absence of a significant decrease in fluorescence intensity. The data in provide further support for the receptor-mediated (SR-B1) mechanism of treatment options for TNBC are limited and often lead to inadequate response and low survival rates.Citation34 In addition, the chemotherapeutic agents currently in use present with substantial off-target effects therefore, detract from the potential benefits of therapy.Citation35,Citation36 NPs have provided the valrubicin uptake from rHDL–valrubicin as the SR-B1 antibody appears to completely block the valrubicin uptake by the MDA-MB-231 cells. These results confirm our earlier findingsCitation18–Citation22 that the drug delivery via rHDL NPs is indeed facilitated by the SR-B1 receptor.
Figure 7 Confocal microscopy images of MDA-MB 231 treated with rHDL-valrubicin in presence of BLT-1.
Abbreviations: rHDL, reconstituted high-density lipoprotein; NP, nanoparticle; SR-B1, scavenger receptor class B type 1; BLT-1, block lipid transporter-1; CTCF, corrected total cell fluorescence.
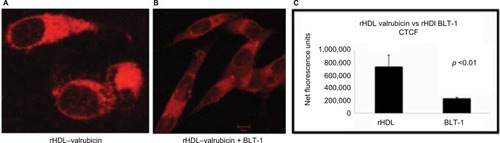
Figure 8 Confocal microscopy images of MDA-MB 231 treated with free valrubicin in presence of BLT-1.
Abbreviation: BLT-1, block lipid transporter-1.
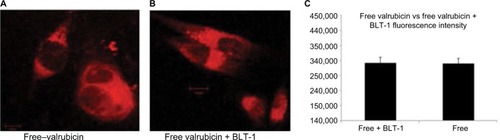
Figure 9 Confocal microscopey images (A and B) of rHDL–valrubicin uptake by MDA-MB-231 cells following pretreatment with an SR-B1 antibody. Magnification ×40.
Discussion
While the current average 5-year survival rate for BC patients is 89.2%,Citation32 the 5-year survival prognosis for patients with metastatic TNBC is <30%.Citation5 This unusually low survival impacts African-American women disproportionately as ~50% of African American women with BC at the age of 40 years or younger present with the TNBC type.Citation33 Current promising alternatives to traditional therapy by enhancing the therapeutic index and an improved antitumor effect.Citation18–Citation22 The rHDL NPs loaded with chemotherapeutic agents appear to have highly desirable characteristics needed for improved TNBC chemotherapy.Citation15 These include the following:
the relatively small size of the rHDL NPs could be a major therapeutic advantage vs conventional drug carriers (including liposomes) as smaller particles are anticipated to penetrate the tumor environment more successfully;Citation31
extended circulation time, due to the ability to avoid the mononuclear phagocyte system that clears the most of the nanoparticulate foreign bodies from the blood; and
tumor-selective targeted drug deliveryCitation18 (see in the following section).
The rHDL NPs loaded with chemotherapeutic agents thus appear to have highly desirable characteristics needed for improved TNBC chemotherapy.
During this study, two drugs (valrubicin and lapatinib) were evaluated regarding their potential contributions to TNBC therapy. These studies show that the rHDL NPs facilitate active targeting of both drugs via the SR-B1 receptor that is overexpressed by most cancer cells and tumors (including those involved with TNBC).Citation22 These studies have also shown that tumor-selective delivery of the anti-cancer drug payload of the rHDL NPs via the SR-B1 receptor is feasible as evidenced by the uptake of radioactive cholesteryl esters by TNBC cells () and confocal microscopy experiments (–).
Regarding the receptor-mediated drug delivery, the cytosolic targeting of anti-cancer agentsCitation37 could be another major advantage of the rHDL transport system because rHDL NPs may have the ability to deliver their payload directly to the cytoplasm and thus avoid the drug resistance pump mechanisms located in the cell membrane. Taken together, these findings show that the MDA-MB31 cells acquire drugs from rHDL NPs via a targeted, receptor-mediated mechanism,Citation30 validating the proposed approach to serve as a potentially enhanced therapy for TNBC. The rHDL NPs are expected to resist opsonization and subsequent sequestering of the NPs by the reticuloendothelial system, one of the current barriers to effective chemotherapy.
At the same time, these particles showed protective effect against cardiomyocytes due to their limited SR-B1 expression. This observation suggests reduction or elimination of cardiac side effects when drugs are encapsulated in rHDL NPs during therapy.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
This research was supported by the Cancer Prevention and Research Institute of Texas (DP150091); Wheels for Wellness, Fort Worth, TX, USA; and the Rutledge Foundation.
References
- World Health OrganizationStewartBWildCWorld Cancer Report 20142014 Available from https://www.iarc.fr/en/media-centre/pr/2014/pdfs/pr224_E.pdfAccessed December 12, 2014
- MilesDRecent advances in systemic therapy. When HER2 is not the target: advances in treatment of HER2-negative metastatic breast cancerBreast Cancer Res200911420819744307
- RakhaEAReis-FilhoJSEllisIOBasal-like breast cancer: a critical reviewJ Clin Oncol200826152568258118487574
- CleatorSHellerWCoombesRCTriple-negative breast cancer: therapeutic optionsLancet Oncol20078323524417329194
- LiedtkeCMazouniCHessKRResponse to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancerJ Clin Oncol20082681275128118250347
- BosPDZhangXHNadalCGenes that mediate breast cancer metastasis to the brainNature200945972491005100919421193
- HudisCAGianniLTriple-negative breast cancer: an unmet medical needOncologist201116suppl 1111
- ManciniPAngeloniARisiEOrsiCMeziSStandard of care and promising new agents for triple negative metastatic breast cancerCancers (Basel)201464187223
- LehmannBDBauerJAChenXIdentification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapiesJ Clin Invest201112172750276721633166
- SchettiniFGiulianoMDe PlacidoSArpinoGNab-paclitaxel for the treatment of triple-negative breast cancer: rationale, clinical data and future perspectivesCancer Treat Rev20165012914127665540
- HagiwaraHSunadaYMechanism of taxane neurotoxicityBreast Cancer2004111828514718798
- ZhangJFLiuJWangYZhangBNovel therapeutic strategies for patients with triple-negative breast cancerOnco Targets Ther201696519652827799799
- LeeESNaKBaeYHDoxorubicin loaded pH-sensitive polymeric micelles for reversal of resistant MCF-7 tumorJ Control Release2005103240541815763623
- PatelNRRathiAMongaytDTorchilinVPReversal of multidrug resistance by co-delivery of tariquidar (XR9576) and paclitaxel using long-circulating liposomesInt J Pharm2011416129629921703341
- JohnsonRSabnisNMcConathyWJLackoAGThe potential role of nanotechnology in therapeutic approaches for triple negative breast cancerPharmaceutics20135235337024244833
- GuoYHeWYangSZhaoDLiZLuanYCo-delivery of docetaxel and verapamil by reduction-sensitive PEG-PLGA-SS-DTX conjugate micelles to reverse the multi-drug resistance of breast cancerColloids Surf B Biointerfaces201715111912727988472
- ZhangYLeonardMShuYOvercoming tamoxifen resistance of human breast cancer by targeted gene silencing using multifunctional prank nanoparticlesACS Nano201711133534627966906
- LackoANairMParanjapeSMooberryLMcConathyWTrojan horse meets magic bullet to spawn a novel, highly effective drug delivery modelChemotherapy200652417117316691026
- McConathyWJNairMParanjapeSMooberryLLackoAGEvaluation of synthetic/reconstituted high density lipoproteins (rHDL) as delivery vehicles for paclitaxelAnticancer Drugs200819218318818176115
- SabnisNANairMIsraelMMcConathyWJLackoAGEnhanced solubility and functionality of valrubicin (AD-32) against cancer cells upon encapsulation into biocompatible nanoparticlesInt J Nanomedicine2012797598322393294
- SabnisNPratapSAkopovaIBowmanWPLackoAGPre-clinical evaluation of rHDL encapsulated retinoid for the treatment of neuroblastomaFront Pediatr Oncol20131110
- ShahzadMMMangalaLSHanHDTargeted delivery of small interfering RNA using reconstituted high-density lipoprotein nanoparticlesNeoplasia201113430931921472135
- KuaiRLiDChenYEMoonJJSchwendemanAHigh-density lipo-proteins: nature’s multifunctional nanoparticlesACS Nano20161033015304126889958
- CruzPMMoHMcConathyWJSabnisNLackoAGThe role of cholesterol metabolism and cholesterol transport in carcinogenesis: a review of scientific findings, relevant to future cancer therapeuticsFront Pharmacol201341723346057
- GospodarowiczDLuiGMGonzalezRHigh-density lipoproteins and the proliferation of human tumor cells maintained on extracellular matrix-coated dishes and exposed to defined mediumCancer Res1982429370437137049362
- DaniloCGuiterrez-PajaresJMaineriMScavenger receptor class B type 1 regulates cellular cholesterol metabolism and cell signaling associated with breast cancer developmentBreast Cancer Res2013155R8724060386
- WadsackCHirschmuglBHammerAScavenger receptor class B, type I on non-malignant and malignant human epithelial cells mediates cholesteryl ester-uptake from high density lipoproteinsInt J Biochem Cell Biol200335444145412565706
- LackoAGNairMParanjapeSJohnsonSMcConathyWJHigh density lipoprotein complexes as delivery vehicles for anticancer drugsAnticancer Res20022242045204912174882
- YuanBWuCWangXHigh scavenger receptor class B type 1 expression is related to tumor aggressiveness and poor prognosis in breast cancerTumor Biol201537318
- MooberryLKNairMParanjapeSMcConathyWJLackoAGReceptor mediated uptake of paclitaxel from a synthetic high density lipoprotein nanocarrierJ Drug Target2010181535819637935
- JiangWKimBRutkaJChanWNanoparticle-mediated cellular response is size dependentNat Nanotechnol20083314515018654486
- National Cancer Institute [webpage on the Internet]SEER Fact Sheet: Female Breast Cancer2013 Available from: www.seer.cancer.gov/statfacts/html/breast.htmlAccessed April 3, 2016
- DietzeECSistrunkCMiranda-CarboniGO’ReganRSeewaldtVLTriple-negative breast cancer in African-American women: disparities versus biologyNat Rev Cancer201515424825425673085
- WabhaHAEl-HadaadHACurrent approaches in treatment of triple-negative breast cancerCancer Biol Med201512210611626175926
- RobinsonPKasembeliMBharadwajUEngineerNEckolsKTTweardyDJSubstance P receptor signaling mediates doxorubicin-induced cardiomyocyte apoptosis and triple-negative breast cancer chemoresistanceBiomed Res Int20162016195927026981525
- AndersCKAbramsonVTanTDentRThe evolution of triple-negative breast cancer: from biology to novel therapeuticsAm Soc Clin Oncol Educ Book201635344227249684
- ZhangZCaoWJinHBiomimetic nanocarrier for direct cytosolic drug deliveryAngew Chem Int Ed Engl200948489171917519876988