
Abstract
Purpose
The aim of this systematic review is to update and synthesize new evidence on BREAST-Q questionnaire’s ability to reflect patient-reported outcomes in women who have undergone breast reconstruction surgery (BRS) following mastectomy.
Methods
PubMed, Science Direct, Google Scholar, Cochrane CENTRAL, and Clincaltrial.gov were searched for relevant studies from January 2009 to September 2021. Any interventional or observational studies that used BREAST-Q to assess patient-reported outcomes in the assessment of BRS following mastectomy were included.
Results
A total of 42 studies were eligible for inclusion in the review. Three were randomized controlled trials and 39 were observational studies. Compared with pre-operative scores, there was an improvement in all BREAST-Q outcome domains following BRS including ‘satisfaction with breasts’, “satisfaction with outcome” “psychosocial”, “physical”, and “sexual wellbeing”. Sexual well-being had the lowest BREAST-Q score both pre-and post-operatively (37.8–80.0 and 39.0–78.0, respectively). Autologous BRS reports higher satisfaction and overall wellbeing compared to implant-based BRS. BREAST-Q has a higher and narrow internal consistency of 0.81 to 0.96 compared with other patient-reported outcome measures (PROMs; EORTC-QLQ, FACT-B, BR-23, BCTOS). The BREAST-Q questionnaire is the only PROM which allows patients to reflect on their care, surgical outcomes, and satisfaction collectively.
Conclusion
This review highlights the fact that BREAST-Q can effectively and reliably measure satisfaction and wellbeing of breast cancer patients after BRS. Comparatively, sexual wellbeing shows poorer outcomes following BRS and more longitudinal studies are necessary to understand the basis for these findings. Compared to other PROMs, BREAST-Q is reliable and specific to breast cancer surgery. Overall, BREAST-Q can help clinicians improve their quality of service, understand patient experiences, and may be used as an auditing tool for surgical outcomes.
Introduction
Breast cancer is the most prevalent type of cancer globally. In 2020 alone 2.3 million women were diagnosed with breast cancer worldwide, and 7.8 million women are currently living with it.Citation1 Over 30% of these women undergo a single mastectomy,Citation2,Citation3 or prophylactic double mastectomy.Citation4 For many, the loss of one or both breasts is devastating, and breast reconstruction surgery (BRS) can improve outcomes for these patients.Citation5,Citation6 Over 40% of women who undergo mastectomy opt for a BRS.Citation7
Surgical management strategies for breast cancer may involve mastectomy, breast conservative surgery, BRS, and other reconstructive methods.Citation8–Citation10 Age, body habitus, co‐morbidities, previous surgeries, and other neo-adjuvant treatment influence the surgical method of choice.Citation11,Citation12 Many of the women opting for BRS are often eligible for more than one type of breast reconstruction, therefore the timing of reconstruction, use of autologous tissue versus implants, short-versus long-term outcomes, and financial implications are all factors a patient may contemplate.Citation9
Patient-reported outcomes (PROs) have become increasingly important in health care and assess the perception of health, quality of life (QoL), and functional status after treatment.Citation13 In cosmetic/reconstructive surgery, this is particularly important as the aim of the intervention is often to improve appearance, function, mental health, and QoL.Citation13 These tools can also help patients become informed, form realistic expectations, communicate with the surgical team, and gain greater satisfaction from the decision-making process.Citation14,Citation15
Patient-reported outcome measures (PROMs) are tools used to quantify PROs, often in the form of self-completed questionnaires.Citation16 The BREAST-Q is a PROM used to assess the unique outcomes of breast surgery patients.Citation17 Developed in 2009, BREAST-Q is made up of three procedure-specific modules: augmentation, reduction, and reconstruction.Citation18 The questionnaire examines outcomes commonly reported as important to women who have undergone a reconstructive procedure for breast cancer as well as health-related quality of life (HRQoL), psychosocial, physical, and sexual well-being, and satisfaction scales.Citation17 Since its development, BREAST-Q has been an effective measure for a spectrum of breast cancer surgeries.Citation19,Citation20
While several studies have used the BREAST-Q to assess the outcomes of patients undergoing breast surgeries for breast cancer, only one comprehensive systematic review exists on PROMs assessed by BREAST-Q which is now outdated and had heterogeneous results.Citation19 Hence, our review aims to update and synthesize new evidence on BREAST-Q’s ability to reflect PROs in women who have undergone BRS following mastectomy. This review will address the following questions:
To what extent has BREAST-Q evaluated PROM amongst patients who have undergone BRS?
What were the outcome parameters used for BREAST-Q?
How does BREAST-Q compare to other available PROMs?
Is BREAST-Q an effective tool for measuring PROMs in BRS?
Methods
Search Strategy
This review adhered to the Preferred Reporting in Systematic Review & Meta-Analysis (PRISMA) guidelines and was listed retrospectively on the PROSPERO International Prospective Register of Systematic Review (CRD42021278102).Citation21 PubMed, Google Scholar, Science Direct, Cochrane CENTRAL, and trial registries (http://clinicialtrials.gov/) were searched for relevant studies published from January 1st, 2009 to September 30th, 2021. The search terms included: (“mastectomy” OR “breast removal surgery”) AND (“breast reconstructive surgery” OR “BRS”) AND (“BREAST-Q” OR “BREAST-Q questionnaire”). Furthermore, the references of selected articles were manually searched for relevant articles. After a screening of titles and abstracts, full-text reports were assessed for eligibility.
Study Selection and Outcomes
Inclusion criteria:
Primary research published in peer-reviewed journals including experimental such as randomized control trials (RCTs) and non-randomized trials, and observational such as cohort and case–control studies;
Studies with a target population included women with primary breast cancer who had mastectomy, or women who had prophylactic mastectomy. No restrictions were placed on age, type, and stage of breast cancer;
Studies reporting outcomes of any type of BRS following mastectomy;
Studies reporting outcomes using BREAST-Q.
Exclusion criteria:
Studies not published in English language:
Reviews, pre-prints, case reports, conference proceedings, conference abstracts, and letters or editorial opinions.
Studies on breast cancer in general without specific reference to BRS.
Studies that did not use BREAST-Q questionnaire as a PROM, or did not fully report BREAST-Q satisfaction or health-related quality of life outcomes.
Data Collection and Extraction
Titles and abstracts of studies identified during the search were imported into Endnote X9 (https://endote.com) for preliminary screening. Full texts of potentially relevant papers were further screened using the eligibility criteria. These were done by two independent reviewers (IS and GB), and any disparity in either selecting eligible articles or assessing findings between the two reviewers was resolved through consultation with a third reviewer (NS). The following data were extracted from each included article into a pre-structured data collection sheet: year of publication, the country where the study was done, sample size, average age, the type of BRS, follow-up period, outcomes measured by BREAST-Q (such as reliability, and responsiveness), and average BREAST-Q scores.
Quality Assessment
The methodological quality of each study will be assessed using the Cochrane Systematic Review RCT risk of bias assessment tool 2 (RoB 2) for RCTs,Citation22,Citation23 and Joanna Briggs Institute (JBI) Critical Appraisal Checklist for observational studies.Citation24 The RoB 2 tool addresses the following biases: random sequence generation, bias due to deviations from intended interventions, bias due to incomplete outcome data, bias in measurement of the outcome, and selective reporting. The items were assessed as “low risk”, “high risk”, or “some concerns”. The JBI is a reliable and valid tool used to assess the methodological quality of observational cross-sectional studies. The checklist consists of eight questions, with 4 possible answers: ‘yes’, “no”, “unclear”, and “not applicable”. A final question on whether to include, exclude, or seek further information on the study gives the overall judgement of the reviewer on that study. Disagreements were resolved through discussion with a third reviewer.
Data Synthesis
Data extracted from included articles were analyzed and combined in a narrative synthesis. Information from the studies were coded based on their methodologies and findings. These were then organized into subheadings and descriptive categories. Tables and charts were used to present the results. Through study screening, there was a wide variation of BRS types evident in literature, therefore a meta-analysis would show significant heterogeneity and ungeneralizable results.
Results
Study Characteristics
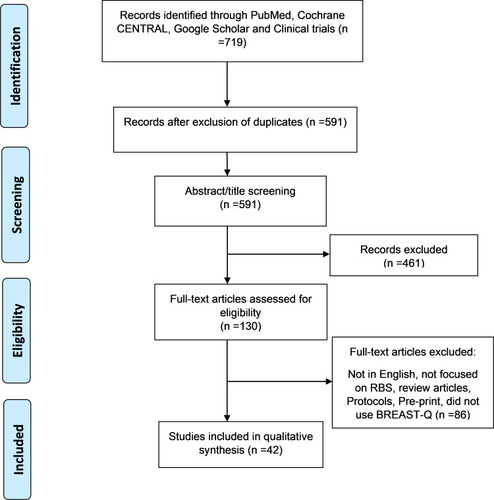
A total of 719 studies were identified from the literature search, and 43 met the eligibility criteria (). All included studies identified their target population as patients who had a therapeutic or prophylactic mastectomy for breast cancer. The sample sizes ranged from 22 to 2048. Nineteen studies reported on implant-based BRS, 9 reported on autologous BRS, and 15 reported on both. One study did not include the type of procedure carried out on subjects. Most studies were conducted in the United States (13), with other countries being Italy (7), United States and Canada (4), Canada only (3), Netherlands (4), Germany (3), Mexico (1), Portugal (1), India (1), Australia (1), Denmark (1), United Kingdom (1) and Czech Republic (1). Studies were published between 2009 and 2021. Only three studies used a randomized controlled study design, while others used an observational design. Fifteen studies were of retrospective design while 28 were of prospective design. The average age ranged from 43.3 to 67 years, and the average follow-up duration at the time of administration of BREAST-Q tool ranged from 1 month to 6.5 years ().
Table 1 Characteristics of Included Studies
Figure 1 PRISMA flow diagram of selected studies.
Patient Reported Outcomes Using BREAST-Q
All studies used the breast reconstruction module of the BREAST-Q tool and aimed to assess the satisfaction and/or QoL of participants after BRS following mastectomy. All but one study reported the respondents’ BREAST-Q scores on “satisfaction with breast” and “satisfaction with outcome” were reported by 31 studies. Wellbeing, psychosocial wellbeing, sexual wellbeing, and physical wellbeing (chest and upper body) were reported by 39, 39, and 37 studies, respectively. Thirteen studies assessed satisfaction with information, surgeon, medical team, and administrative staff domains, respectively.
On the BREAST-Q tool, the scoring for each domain ranges from 0, signifying the least possible level of satisfaction or wellbeing, to 100, signifying the highest. The average scores on satisfaction with breast domain ranged from 39.5 to 75.8 pre-operatively and 51.1–82.0 post-operatively while satisfaction with overall outcome ranged from 56.3 to 89. Average psychosocial well-being scores ranged from 54.3 to 77.9 on pre-operative assessment and 63.0–94.0 on post-operative assessment. Sexual well-being had the lowest average scores in all the studies, ranging from 37.8 to 80.0 on pre-operative assessment and 39.0–78.0 on post-operative assessment. Physical well-being (chest and upper body) had average scores ranging from 57.8 to 81.4 at baseline and 53.2–83.0 post-operatively. The studies also reported high satisfaction rates with medical care. Average scores for satisfaction with information ranged from 53.5 to 89, satisfaction with the surgeon, 83.2–100.0, Satisfaction with the medical team, 78.0–100.0, and satisfaction with the administrative team, 81.5–100.0.
BREAST-Q Response Rate
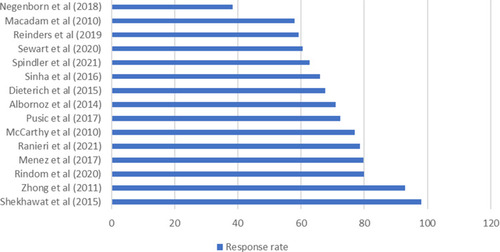
Of the 42 studies, only 15 reported the response rate for completion of the BREAST-Q questionnaire, which ranged from 38.4% to 98% ().
Figure 2 Response rate for completion of BREAST-Q questionnaire (%).
Comparison Between Different BRS Types
Most studies compared PROs between different types of BRS. Comparisons were based on timing (immediate versus delayed),Citation25–Citation27 type (implant-based versus autologous),Citation28–Citation37 type of flap used (deep inferior epigastric perforators [DIEP], transverse rectus abdominis myocutaneous [TRAM], latissimus dorsi [LD] flaps),Citation38–Citation40 type of Implant/tissue expanders used (acellular dermal matrices [ADM], silicone expanders, saline expanders),Citation41–Citation44 placement of implant (pre-pectoral versus sub-pectoral),Citation45,Citation46 number of stages (single stage versus multiple stages),Citation25–Citation27,Citation45 weight (normal weight, overweight, obese),Citation47 and age (less than 60 versus over 60, less than 65 versus over 65).Citation39,Citation48
Autologous vs Implant-Based BRS
In nearly all studies that compared PROs between autologous and implant-based BRS, autologous BRS had better outcomes comparatively.Citation28–Citation37 shows the average BREAST-Q scores for the HRQoL subscales between autologous and implant-based BRS. In all domains, autologous BRS had higher post-operative scores compared to implant-based.
Table 2 Average BREAST-Q Score for Different Breast Reconstruction Surgeries Across Included Studies. Each Domain Ranges from 0, Signifying the Least Possible Level of Satisfaction or Wellbeing, to 100, Signifying the Highest (0–100 Range in Each Domain)
Type of Flaps and Implants Used
Only two studies in this review compared the PROs following autologous BRS with different flap types. Rindom et al compared the PROs between BRS with a latissimus dorsi (LD) flap and a thoracodorsal artery perforator flap, while Ludolph et al compared the PROs between DIEP and TRAM.Citation38,Citation39 These two studies found no significant difference between the two groups in respect to all satisfaction and HRQoL domains, as both groups reported high satisfaction rates.Citation38,Citation39 Similarly, two studies compared the use of saline and silicone implants. Both found that silicone implants showed better PROs compared to saline implants.Citation44,Citation49 Sorkin et al found no difference between the use of ADM and non-ADM tissue expanders the PROs of patients.Citation42
Single-Stage versus Multiple-Stage BRS
Negenborn et al and Qureshi et al found no significant differences in all BREAST-Q domains between patients who underwent one-stage BRS and those who underwent two-stages implant BRS using tissue expanders.Citation25,Citation50 Another study found no significant difference in the PROs of patients in both direct-to-implant (DTI) group and tissue expander groups, except in sexual wellbeing, where the DTI group fared better.Citation27
BREAST-Q versus Other PROMs
The BREAST-Q tool was compared with five other HRQoL PROM questionnaires (). BREAST-Q covers a wide range of domains compared with other PROMs and is the only tool that assesses individuals’ satisfaction with care received. While all tools generally reported good internal consistency/reliability with Rasch analysis, a statistical tool that assesses psychometric properties, BREAST-Q had a narrower range of reliability (0.81–0.96, compared to 0.69–0.9.0 and 0.46–0.91 as seen with EORTC QLQ 30 and BR-23 respectively) and is considered psychometrically robust.Citation17,Citation51,Citation52 The test re-test reproducibility of BREAST-Q ranges from 0.73 to 0.96.Citation17 Only the BREAST-Q reconstruction module is specific to HRQoL after BRS following mastectomy.
Table 3 Comparison of BREAST-Q Questionnaire with Other Patient-Reported Outcome Questionnaires
Methodological Quality of Studies
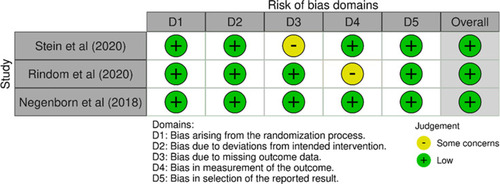
Of the included studies, only 3 were RCTs, and all had low risk of bias (). The JBI Critical Appraisal Checklist was used to assess the methodological quality of the observational studies. All studies were of high quality and were therefore included in the review.
Figure 3 Risk of bias assessment for included RCTs.
Discussion
The BREAST-Q questionnaire is a validated tool for evaluating PROs in patients undergoing BRS following mastectomy. Generally, BRS using either autologous or implant-based methods resulted in greater satisfaction and HRQoL. This review also found that autologous BRS had better PROs than implant-based BRS in all BREAST-Q domains. No statistical differences were noticed between the different types of flaps studied, however patients with silicone implants had better BREAST-Q scores indicating greater satisfaction and HRQoL. Patients that underwent one-staged and two-staged breast reconstructions fared similarly.
Alongside subjective outcomes, patient satisfaction is an indicator of surgical success and predicts psychosocial health following BRS. Within the included studies, average BREAST-Q scores for “satisfaction with breasts” domain ranged from 39.5 to 75.8 pre-operatively and increased to 51.1–82.0 post-operatively which can be attributed to a favorable change in body image. In contrast, satisfaction amongst patients who underwent mastectomy without BRS was poorer, with women being unhappy with their breasts and surgical scar despite the cancer being successfully treated.Citation53,Citation54 Duggal et al found that over three-quarters of their participants opting for BRS had body image as their motivating factor.Citation55 These BREAST-Q scores and supporting findings suggest BRS should be indicated for patients who house concerns about body image, or hope to improve body image following mastectomy.
The reviewed literature suggests BREAST-Q can indicate which BRS will yield greatest outcomes in satisfaction ( and ). All types of BRS yielded improvements with breast satisfaction following surgery and continued to improve over time except for Stein et al and Negenborn et al, who notably used ADM alongside tissue expanders/implant BRS.Citation41,Citation50 In these surgeries, lower satisfaction with breast/s, overall outcome, physical and sexual wellbeing outcomes following BRS were observed.Citation41,Citation50 A possible explanation for these findings is that ADM is associated with higher post-operative complications including seroma, infections, and red breast syndrome which may affect patient QoL and satisfaction.Citation41,Citation50,Citation56,Citation57 Another factor that worsened BREAST-Q scores was radiotherapy, which is also associated with higher rates of complications in autologous and implant-based BRS.Citation33,Citation58,Citation59 Knowing the difference in complication rates in these BRS cohorts would better explain the low level of satisfaction observed.
Physical and psychosocial wellbeing following BRS was assessed in most of the included studies and showed overall improvement. An exception to this was Rowland et al who found patients undergoing mastectomy with and without reconstruction showed declined physical wellbeing, but this was equal when compared with women undergoing lumpectomy.Citation60 Another domain, sexual wellbeing, generally decreased following mastectomy compared with pre-operative BREAST-Q scores, and after BRS there was reportedly worsened to minimal improvements.Citation41,Citation42,Citation61 Overall, sexual wellbeing fared the least compared to all other domains which can be explained by the psychological effects of breast cancer surgery which can include anxiety, depression, and a feeling of loss of femininity.Citation62 Moreover, pain and discomfort in the months following surgery may impact the pursuit or desire for sexual activity. In the latter case, patient sexual well-being should improve following complete healing which could take up to a year or more.Citation63 Future longitudinal studies are needed to define the etiology of this domain because if decreased sexual wellbeing is due to mental health, this defines an opportunity to address it with a health professional.
The BREAST-Q questionnaire also allows patients to reflect on their relationship with the surgeon, the information that they received, and the care provided by the administrative staff.Citation17 Although most studies did not assess this domain, the ones that did show patients had high levels of satisfaction with the care that they received. More studies should focus on this PRO because these measures can be used to monitor and improve quality of care by surgeons and hospitals, and for auditing by health governance. Satisfaction with care has also been known to influence other outcome domains such as “satisfaction with breasts” and physical wellbeing including HRQoL. In future, this PRO should be focused upon more and be viewed as a potentially valuable tool for measuring quality of care.Citation64
The BREAST-Q questionnaire was designed to measure outcomes which should be examined in BRS.Citation65,Citation66 When examined by Rasch analysis, BREAST-Q has a high narrow internal consistency and test–retest reproducibility.Citation17,Citation51,Citation52 This strongly supports that it is valid and reliable tool for its purpose. Other PROMs used in assessing HRQoL in breast cancer patients are equally reliable but have wide reported range. In contrast to these questionnaires, BREAST-Q is also specific to BRS and is the only tool to accurately assess patient satisfaction with care ().Citation67,Citation68 Chen et al reported BREAST-Q as one of the best tools for assessing HRQoL in breast cancer patients, stating that it was able to address surgery-specific issues, unlike other PROMs.Citation69 In support, the International Consortium for Health Outcomes Measurement endorsed BREAST-Q for breast cancer patients, highlighting its approval by healthcare governing bodies for assessing oncoplastic BRS outcomes.Citation70
The current systematic review achieved its aims to examine the current evidence about BREAST-Q for management of post-mastectomy BRS and was able to compare it with the other PROMs (). Furthermore, the current study adopted a well-structured search strategy, followed the PRISMA guidelines and utilized manual searches to identify most eligible studies, and only included studies that were of good methodological quality. Despite these benefits, this study has several limitations. Firstly, the BREAST-Q tool collects self-reported data which can be unreliable; however, for subjective outcomes self-reported data are an accepted measure of choice.71 Secondly, the level of heterogeneity in BRS procedures prevented the performance of a meta-analysis and pooled analysis. Lastly, there was diversity amongst the geographic origin of included studies which may have introduced sociocultural factors. The impact of these would need to be statistically explored in meta-analysis, however the heterogeneity between studies made a meta-analysis unsuitable.
Conclusion
This review highlights that BREAST-Q can effectively and reliably measure satisfaction and HRQoL of breast cancer patients after BRS. Comparatively, sexual wellbeing shows poorer outcomes following BRS and more longitudinal studies are necessary to understand the basis for these findings. Overall, BREAST-Q can help clinicians improve their quality of service, understand patient experiences, and may be used as an auditing tool for surgical outcomes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest to disclose.
References
- World Health Organization. Breast cancer [Internet]; 2020 [cited September5, 2021.]. Available from: https://www.who.int/news-room/fact-sheets/detail/breast-cancer. Accessed November29, 2021.
- HardingC, PompeiF, BurmistrovD, WilsonR. Use of mastectomy for overdiagnosed breast cancer in the United States: analysis of the SEER 9 cancer registries. J Cancer Epidemiol. 2019;2019:e5072506.
- DragunAE, HuangB, TuckerTC, SpanosWJ. Increasing mastectomy rates among all age groups for early stage breast cancer: a 10-year study of surgical choice. Breast J. 2012;18(4):318–325.22607016
- DragunAE, PanJ, RileyEC, et al. Increasing use of elective mastectomy and contralateral prophylactic surgery among breast conservation candidates: a 14-year report from a comprehensive cancer center. Am J Clin Oncol. 2013;36(4):375–380.22643566
- HeidariM, ShahbaziS, GhodusiM. Evaluation of body esteem and mental health in patients with breast cancer after mastectomy. J Midlife Health. 2015;6(4):173.26903758
- ArroyoJMG, LópezMLD. Psychological problems derived from mastectomy: a qualitative study. Int J Surg Oncol. 2011;4(2011):e132461.
- IlonzoN, TsangA, TsantesS, EstabrookA, ThuMAM. Breast reconstruction after mastectomy: a ten-year analysis of trends and immediate postoperative outcomes. Breast. 2017;32:7–12.27988412
- BellavanceEC, KesmodelSB. Decision-making in the surgical treatment of breast cancer: factors influencing women’s choices for mastectomy and breast conserving surgery. Front Oncol. 2016;29(6):74.
- SunCS, CantorSB, ReeceGP, FingeretMC, CrosbyMA, MarkeyMK. Helping patients make choices about breast reconstruction: a decision analysis approach. Plast Reconstr Surg. 2014;134(4):597–608.25357022
- FingeretMC, NipomnickSW, CrosbyMA, ReeceGP. Developing a theoretical framework to illustrate associations among patient satisfaction, body image and quality of life for women undergoing breast reconstruction. Cancer Treat Rev. 2013;39(6):673–681.23380309
- CutressRI. Oncoplastic breast reconstruction: guidelines for best practice [Internet]. In: RainsburyD, WillettA, editors. British Association of Plastic Reconstructive and Aesthetic Surgeons; 2012: 68.[cited September 5, 2021]: Available from: https://eprints.soton.ac.uk/345578/. Accessed November29, 2021.
- SchmaussD, MachensH-G, HarderY. Breast reconstruction after mastectomy. Front Surg. 2015;2:71.26835456
- WeldringT, SmithSMS. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv Insights. 2013;4(6):61–68.
- LipscombJ, GotayCC, SnyderCF. Patient-reported outcomes in cancer: a review of recent research and policy initiatives. CA Cancer J Clin. 2007;57(5):278–300.17855485
- CanoSJ, KlassenA, PusicAL. The science behind quality-of-life measurement: a primer for plastic surgeons. Plast Reconstr Surg. 2009;123(3):98e–106e.19116542
- BlackN. Patient reported outcome measures could help transform healthcare. BMJ. 2013;28(346):f167.
- PusicAL, KlassenAF, ScottAM, KlokJA, CordeiroPG, CanoSJ. Development of a new patient-reported outcome measure for breast surgery: the BREAST-Q. Plast Reconstr Surg. 2009;124(2):345–353.19644246
- PusicAL, ChenCM, CanoS, et al. Measuring quality of life in cosmetic and reconstructive breast surgery: a systematic review of patient-reported outcomes instruments. Plast Reconstr Surg. 2007;120(4):823–837.17805107
- LiuL, BranfordO, MehiganS. BREAST-Q measurement of the patient perspective in oncoplastic breast surgery: a systematic review. Plast Reconstr Surg Glob Open. 2018;6(8):e1904.30254830
- DeanNR, CrittendenT. A five-year experience of measuring clinical effectiveness in a breast reconstruction service using the BREAST-Q patient reported outcomes measure: a cohort study. J Plast Reconstr Aesthet Surg. 2016;69(11):1469–1477.27639422
- PageMJ, McKenzieJE, BossuytPM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;29(372):n71.
- HigginsJP, SavovićJ, PageMJ, ElbersRG, SterneJA. Assessing risk of bias in a randomized trial. In: Cochrane Handbook for Systematic Reviews of Interventions [Internet]. John Wiley & Sons, Ltd; 2019: 205–228. [cited May 4, 2021]. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/9781119536604.ch8. Accessed November29, 2021.
- McGuinnessLA, HigginsJPT. Risk‐of‐bias VISualization (robvis): an R package and Shiny web app for visualizing risk‐of‐bias assessments. Res Syn Meth. 2021;12(1):55–61.
- MunnZ, MoolaS, LisyK, RiitanoD, TufanaruC. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int J Evid Based Health. 2015;13:147–153.
- QureshiAA, OdomEB, ParikhRP, MyckatynTM, TenenbaumMM. Patient-reported outcomes of aesthetics and satisfaction in immediate breast reconstruction after nipple-sparing mastectomy with implants and fat grafting. Aesthet Surg J. 2017;37(9):999–1008.28379284
- CasellaD, Di TarantoG, OnestiMG, GrecoM, RibuffoD. A retrospective comparative analysis of risk factors and outcomes in direct-to-implant and two-stages pre-pectoral breast reconstruction: BMI and radiotherapy as new selection criteria of patients. Eur J Surg Oncol. 2019;45(8):1357–1363.30827802
- SrinivasaDR, GarveyPB, QiJ, et al. Direct-to-Implant versus two-stage tissue expander/implant reconstruction: 2-year risks and patient-reported outcomes from a prospective, multicenter study. Plast Reconstr Surg. 2017;140(5):869–877.29068918
- BennettKG, QiJ, KimHM, et al. Association of fat grafting with patient-reported outcomes in postmastectomy breast reconstruction. JAMA Surg. 2017;152(10):944–950.28658472
- DavisGB, LangJE, PericM, et al. Breast reconstruction satisfaction rates at a large county hospital. Ann Plast Surg. 2014;72:S61–5.24691306
- PirroO, MestakO, VindigniV, et al. Comparison of patient-reported outcomes after implant versus autologous tissue breast reconstruction using the BREAST-Q. Plast Reconstr Surg Glob Open. 2017;5(1):e1217.28203513
- KliftoKM, AravindP, MajorM, et al. Differences between breast cancer reconstruction and institutionally established normative data using the BREAST-Q reconstruction module: a comparative study. Plast Reconstr Surg. 2020;145(6):1371–1379.32459767
- SantosaKB, QiJ, KimHM, HamillJB, PusicAL, WilkinsEG. Effect of patient age on outcomes in breast reconstruction: results from a multicenter prospective study. J Am Coll Surg. 2016;223(6):745–754.27806906
- ReindersFCJ, Young-AfatDA, BatenburgMCT, et al. Higher reconstruction failure and less patient-reported satisfaction after post mastectomy radiotherapy with immediate implant-based breast reconstruction compared to immediate autologous breast reconstruction. Breast Cancer. 2020;27(3):435–444.31858435
- SantosaKB, QiJ, KimHM, HamillJB, WilkinsEG, PusicAL. Long-term patient-reported outcomes in postmastectomy breast reconstruction. JAMA Surg. 2018;153(10):891–899.29926096
- KlementKA, HijjawiJB, LoGiudiceJA, AlghoulM, Omesiete-AdejareP. Microsurgical breast reconstruction in the obese: a better option than tissue expander/implant reconstruction? Plast. Reconstr Surg. 2019;144(3):539–546.
- Martinez-LópezJC, García-EspinozaJA, Flores-SotoD, et al. Patient satisfaction index and quality of life measurement with Breast-Q after breast reconstruction in a plastic surgery center in Mexico. J Biosci Med. 2021;9(6):94–105.
- BritoÍM, FernandesA, AndresenC, BarbosaR, RibeiroM, Valença-FilipeR. Patient satisfaction with breast reconstruction: how much do timing and surgical technique matter? Eur. J Plast Surg. 2020;43(6):809–818.
- RindomMB, GunnarssonGL, LautrupMD, et al. Good health-related quality-of-life and high patient-reported satisfaction after delayed breast reconstruction with pedicled flaps from the back. J Plast Reconstr Aesthet Surg. 2021;74(8):1752–1757.33676866
- LudolphI, HorchRE, HarlanderM, et al. Is there a rationale for autologous breast reconstruction in older patients? A retrospective single center analysis of quality of life, complications and comorbidities after DIEP or ms-TRAM flap using the BREAST-Q. Breast J. 2015;21(6):588–595.26400037
- ZhongT, McCarthyC, MinS, et al. Patient satisfaction and health-related quality of life after autologous tissue breast reconstruction: a prospective analysis of early postoperative outcomes. Cancer. 2012;118(6):1701–1709.22025176
- SteinMJ, ArnaoutA, LichtensteinJB, et al. A comparison of patient-reported outcomes between Alloderm and Dermacell in immediate alloplastic breast reconstruction: a randomized control trial. J Plast Reconstr Aesthet Surg. 2021;74(1):41–47.32893151
- SorkinM, QiJ, KimHM, et al. Acellular dermal matrix in immediate expander/implant breast reconstruction: a multicenter assessment of risks and benefits. Plast Reconstr Surg. 2017;140(6):1091–1100.28806288
- CasellaD, Di TarantoG, MarcascianoM, et al. Nipple-sparing bilateral prophylactic mastectomy and immediate reconstruction with TiLoop® Bra mesh in BRCA1/2 mutation carriers: a prospective study of long-term and patient reported outcomes using the BREAST-Q. Breast. 2018;39:8–13.29455110
- MacadamSA, HoAL, CookEF Jr, LennoxPA, PusicAL. Patient satisfaction and health-related quality of life following breast reconstruction: patient-reported outcomes among saline and silicone implant recipients. Plast Reconstr Surg. 2010;125(3):761–771.20009795
- CaputoGG, ZingarettiN, KiprianidisI, et al. Quality of Life and early functional evaluation in direct-to-implant breast reconstruction after mastectomy: a comparative study between prepectoral versus dual-plane reconstruction. Clin Breast Cancer. 2021;21(4):344–351.33308993
- GhilliM, MarinielloMD, CamilleriV, et al. PROMs in post-mastectomy care: patient self-reports (BREAST-QTM) as a powerful instrument to personalize medical services. Eur J Surg Oncol. 2020;46(6):1034–1040.31812290
- SinhaS, RuskinO, D’AngeloA, McCombeD, MorrisonWA, WebbA. Are overweight and obese patients who receive autologous free-flap breast reconstruction satisfied with their postoperative outcome? A single-centre study. J Plast Reconstr Aesthet Surg. 2016;69(1):30–36.26481926
- SongD, SlaterK, PapsdorfM, et al. Autologous breast reconstruction in women older than 65 years versus women younger than 65 years: a multi-center analysis. Ann of Plast Surg. 2016;76(2):155–163.26637165
- McCarthyCM, KlassenAF, CanoSJ, et al. Patient satisfaction with postmastectomy breast reconstruction: a comparison of saline and silicone implants. Cancer. 2010;116(24):5584–5591.21136577
- NegenbornVL, DikmansREG, BoumanM-B, WilschutJA, MullenderMG, SalzbergCA. Patient-reported outcomes after ADM-assisted implant-based breast reconstruction: a cross-sectional study. Plast Reconstr Surg Glob Open. 2018;6(2):e1654.29616167
- CanoSJ, KlassenAF, ScottAM, CordeiroPG, PusicAL. The BREAST-Q: further validation in independent clinical samples. Plast Reconstr Surg. 2012;129(2):293–302.22286412
- FuzesiS, CanoSJ, KlassenAF, AtishaD, PusicAL. Validation of the electronic version of the BREAST-Q in the army of women study. Breast. 2017;33:44–49.28279888
- AnagnostopoulosF, MyrgianniS. Body image of Greek breast cancer patients treated with mastectomy or breast conserving surgery. J Clin Psychol Med Settings. 2009;16(4):311–321.19701698
- KoçanS, GürsoyA. Body image of women with breast cancer after mastectomy: a qualitative research. J Breast Health. 2016;12(4):145–150.28331752
- DuggalCS, MetcalfeD, SackeyfioR, CarlsonGW, LoskenA. Patient motivations for choosing postmastectomy breast reconstruction. Ann Plast Surg. 2013;70(5):574–580.23542859
- ChunYS, VermaK, RosenH, et al. Implant-based breast reconstruction using acellular dermal matrix and the risk of postoperative complications. Plast Reconstr Surg. 2010;125(2):429–436.20124828
- DikmansREG, NegenbornVL, BoumanM-B, et al. Two-stage implant-based breast reconstruction compared with immediate one-stage implant-based breast reconstruction augmented with an acellular dermal matrix: an open-label, Phase 4, multicentre, randomised, controlled trial. The Lancet Oncol. 2017;18(2):251–258.28012977
- AlbornozCR, MatrosE, McCarthyCM, et al. Implant breast reconstruction and radiation: a multicenter analysis of long-term health-related quality of life and satisfaction. Ann Surg Oncol. 2014;21(7):2159–2164.24740825
- KoppikerCB, NoorAU, DixitS, et al. Implant-based breast reconstruction with autologous lower dermal sling and radiation therapy outcomes. Indian J Surg. 2019;81(6):543–551.
- RowlandJH, DesmondKA, MeyerowitzBE, BelinTR, WyattGE, GanzPA. Role of breast reconstructive surgery in physical and emotional outcomes among breast cancer survivors. J Natl Cancer Inst. 2000;92(17):1422–1429.10974078
- NegenbornVL, Young-AfatDA, DikmansREG, et al. Quality of life and patient satisfaction after one-stage implant-based breast reconstruction with an acellular dermal matrix versus two-stage breast reconstruction (BRIOS): primary outcome of a randomised, controlled trial. The Lancet Oncol. 2018;19(9):1205–1214.30104147
- GilbertE, EmileeG, UssherJM, PerzJ. Sexuality after breast cancer: a review. Maturitas. 2010;66(4):397–407.20439140
- SpectorDJ, MayerDK, KnaflK, PusicA. Women’s recovery experiences after breast cancer reconstruction surgery. J of Psychosoc Oncol. 2011;29(6):664–676.22035539
- O’ConnellR, DiMiccoR, KhabraK, et al. Initial experience of the BREAST-Q breast-conserving therapy module. Breast Cancer Res Treat. 2016;160(1):79–89.27637781
- DaviesC, HolcombeC, SkillmanJ, et al. Protocol: protocol for a mixed-method study to inform the feasibility of undertaking a large-scale multicentre study comparing the clinical and patient-reported outcomes of oncoplastic breast conservation as an alternative to mastectomy with or without immediate breast reconstruction in women unsuitable for standard breast-conserving surgery (the ANTHEM Feasibility Study). BMJ Open. 2021;11:4.
- PotterS, HolcombeC, WardJA, et al. Development of a core outcome set for research and audit studies in reconstructive breast surgery. Br J Surg. 2015;102(11):1360–1371.26179938
- JaenssonM, DahlbergK, NilssonU. Factors influencing day surgery patients’ quality of postoperative recovery and satisfaction with recovery: a narrative review. Perioperative Med. 2019;8(1):3.
- BerningV, LaupheimerM, NüblingM, HeideggerT. Influence of quality of recovery on patient satisfaction with anaesthesia and surgery: a prospective observational cohort study. Anaesthesia. 2017;72(9):1088–1096.28510285
- ChenCM, CanoSJ, KlassenAF, et al. Measuring quality of life in oncologic breast surgery: a systematic review of patient-reported outcome measures: quality of life in breast surgery. Breast J. 2010;16(6):587–597.21070435
- OngWL, SchouwenburgMG, van BommelACM, et al. A standard set of value-based patient-centered outcomes for breast cancer: the International Consortium for Health Outcomes Measurement (ICHOM) Initiative. JAMA Oncol. 2017;3(5):677–685.28033439
- LucasRE. Reevaluating the strengths and weaknesses of self- report measures of subjective well-being. In: E. Diener, S. Oishi, & L. Tay (Eds.). Handbook of Well-Being. Salt Lake City, UT: DEF publishers; 2018:12. doi: nobascholar.com
- RanieriJ, FiascaF, GuerraF, PerilliE, MatteiA, Di GiacomoD. Examining the post-operative well-being of women who underwent mammoplasty: a cross-sectional study. Front Psychiatry. 2021;29(12):645102.
- AllenRJ, SobtiN, PatelAR, et al. Laterality and patient-reported outcomes following autologous breast reconstruction with free abdominal tissue: an 8-year examination of BREAST-Q data. Plast Reconstr Surg. 2020;146(5):964–975.33141527
- KoslowS, PharmerLA, ScottAM, et al. Long-term patient-reported satisfaction after contralateral prophylactic mastectomy and implant reconstruction. Ann Surg Oncol. 2013;20(11):3422–3429.23720070
- MénezT, MichotA, TamburinoS, WeigertR, PinsolleV. Multicenter evaluation of quality of life and patient satisfaction after breast reconstruction, a long-term retrospective study. Ann Chir Plast Esthét Elsevier. 2017;63(2):126–133.
- RazzanoS, MarongiuF, WadeR, FigusA. Optimizing DIEP flap Insetting for immediate unilateral breast reconstruction: a prospective cohort study of patient-reported aesthetic outcomes. Plast Reconstr Surg. 2019;143(2):261e–70e.
- HuES, PusicAL, WaljeeJF, et al. Patient-reported aesthetic satisfaction with breast reconstruction during the long-term survivorship period. Plast Reconstr Surg. 2009;124(1):1–8.19568038
- PusicAL, MatrosE, FineN, et al. Patient-reported outcomes 1 year after immediate breast reconstruction: results of the mastectomy reconstruction outcomes consortium study. J Clin Oncol. 2017;35(22):2499–2506.28346808
- ShekhawatL, BusheriL, DixitS, PatelC, DharU, KoppikerC. Patient-reported outcomes following breast reconstruction surgery and therapeutic mammoplasty: prospective evaluation 1-year post-surgery with BREAST-Q questionnaire. Indian J Surg Oncol. 2015;6(4):356–362.27065661
- DieterichM, AngresJ, StubertJ, StachsA, ReimerT, GerberB. Patient-reported outcomes in implant-based breast reconstruction alone or in combination with a titanium-coated polypropylene mesh – a detailed analysis of the BREAST-Q and overview of the literature. Geburtshilfe Frauenheilkd. 2015;75(7):692–701.26257406
- SewartE, TurnerNL, ConroyEJ, et al. Patient-reported outcomes of immediate implant-based breast reconstruction with and without biological or synthetic mesh. BJS Open. 2021;5(1):zraa063.33609398
- EltahirY, BosmaE, TeixeiraN, WerkerPMN, de BockGH. Satisfaction with cosmetic outcomes of breast reconstruction: investigations into the correlation between the patients’ Breast-Q outcome and the judgment of panels. JPRAS Open. 2020;12(24):60–70.
- OchoaO, Garza IIIR, PisanoS, et al. Prospective longitudinal patient-reported satisfaction and health-related quality of life following DIEP flap breast reconstruction: relationship with body mass index. Plast Reconstr Surg. 2019;143(6):1589–1600.30907803
- SpindlerN, EbelF, BriestS, WallochnyS, LangerS. Quality of life after bilateral risk-reducing mastectomy and simultaneous reconstruction using pre-pectoral silicone implants. Patient Prefer Adherence. 2021;13(15):741–750.
- TanML, IdrisDB, TeoLW, et al. Validation of EORTC QLQ-C30 and QLQ-BR23 questionnaires in the measurement of quality of life of breast cancer patients in Singapore. Asia Pac J Oncol Nurs. 2014;1(1):22–32.27981079
- OuZ, TangY, FuJ, DoucetteJ, MurimiIB. PCN482 patient-reported outcome measures in breast cancer: a systematic review of EORTC QLQ-C30, FACT-B, and EORTC QLQ-BR23 development and validation. Value in Health. 2019;22:S530.
- NguyenJ, PopovicM, ChowE, et al. EORTC QLQ-BR23 and FACT-B for the assessment of quality of life in patients with breast cancer: a literature review. J Comp Eff Res. 2015;4(2):157–166.25825844
- MontazeriA, HarirchiI, VahdaniM, et al. The EORTC Breast Cancer-Specific Quality of Life Questionnaire (EORTC QLQ-BR23): translation and Validation study of the Iranian Version. Qual Life Res. 2000;9(2):177–184.10983481
- Ashing-GiwaK, RosalesM. A cross-cultural validation of patient-reported outcomes measures: a study of breast cancers survivors. Qual Life Res. 2013;22(2):295–308.22367682
- Ashing-GiwaKT, PadillaGV, TejeroJS, KimJ. Breast cancer survivorship in a multiethnic sample: challenges in recruitment and measurement. Cancer. 2004;101(3):450–465.15274058
- RamadhantyZ, YarsoK, ProbandariA. Construct validity and reliability of Indonesian Version of RAND SF-36 quality of life questionnaire in breast cancer patients. Indonesian J Cancer. 2019;13:55.
- HahnEA, SegawaE, KaiserK, CellaD, SmithBD. Validation of the Functional Assessment of Cancer Therapy-Breast (FACT-B) quality of life instrument. JCO. 2015;33(15_suppl):e17753–e17753.
- BradyMJ, CellaDF, MoF, et al. Reliability and validity of the Functional Assessment of Cancer Therapy-Breast quality-of-life instrument. J Clin Oncol. 1997;15(3):974–986.9060536
- BellaO, CocchiaraR, de LucaA, et al. Functional Assessment of Cancer Therapy Questionnaire for Breast Cancer (FACT-B+4): Italian version validation. Clin Ter. 2018;169:e151–4.30151547
- KrishnanL, StantonAL, CollinsCA, ListonVE, JewellWR. Form or function? Part 2 objective cosmetic and functional correlates of quality of life in women treated with breast-conserving surgical procedures and radiotherapy . Cancer. 2001;91(12):2282–2287.11413516