
Abstract
Context
Breast cancer is the most prevalent cancer amongst women but it has the highest survival rates amongst all cancer. Rehabilitation therapy of post-treatment effects from cancer and its treatment is needed to improve functioning and quality of life. This review investigated the range of methods for improving physical, psychosocial, occupational, and social wellbeing in women with breast cancer after receiving breast cancer surgery.
Method
A search for articles published in English between the years 2009 and 2014 was carried out using The Cochrane Database of Systematic Reviews, the Database of Abstracts of Reviews of Effects, PubMed, and ScienceDirect. Search terms included: ‘breast cancer’, ‘breast carcinoma’, ‘surgery’, ‘mastectomy’, ‘lumpectomy’, ‘breast conservation’, ‘axillary lymph node dissection’, ‘rehabilitation’, ‘therapy’, ‘physiotherapy’, ‘occupational therapy’, ‘psychological’, ‘psychosocial’, ‘psychotherapy’, ‘exercise’, ‘physical activity’, ‘cognitive’, ‘occupational’, ‘alternative’, ‘complementary’, and ‘systematic review’.
Study selection
Systematic reviews on the effectiveness of rehabilitation methods in improving post-operative physical, and psychological outcomes for breast cancer were selected. Sixteen articles met all the eligibility criteria and were included in the review.
Data extraction
Included review year, study aim, total number of participants included, and results.
Data synthesis
Evidence for exercise rehabilitation is predominantly in the improvement of shoulder mobility and limb strength. Inconclusive results exist for a range of rehabilitation methods (physical, psycho-education, nutritional, alternative-complementary methods) for addressing the domains of psychosocial, cognitive, and occupational outcomes.
Conclusion
There is good evidence for narrowly-focused exercise rehabilitation in improving physical outcome particularly for shoulder mobility and lymphedema. There were inconclusive results for methods to improve psychosocial, cognitive, and occupational outcomes. There were no reviews on broader performance areas and lifestyle factors to enable effective living after treatment. The review suggests that comprehensiveness and effectiveness of post-operative breast cancer rehabilitation should consider patients’ self-management approaches towards lifestyle redesign, and incorporate health promotion aspects, in light of the fact that breast cancer is now taking the form of a chronic illness with longer survivorship years.
Introduction
Breast cancer incidences ranges from 19.3 per 100,000 women in Eastern Africa to 89.7 per 100,000 women in Western Europe and about 40 per 100,000 in developing countries.Citation1 The 5-year relative survival rates for breast cancer in the US have improved dramatically from 63% in the 1960s to 90% in 2011.Citation2 In Malaysia, the survival rates estimated in 2009 was 43.5%, with Malay, Chinese, and Indians, and Malays having 5-year survival rates of 39.7%, 48.2%, and 47.2% respectively, and the rates have also improved annually. The number of breast cancer survivors has increased dramatically as a result of early detection, better treatment, and various multidisciplinary rehabilitation methods.Citation3,Citation4 However, improved survival rate of breast cancers also comes with numerous side effects from the cancer and its treatment. There is a need for comprehensive rehabilitation methods to address the many impacts of the long-term effects of this treatment, including the less recognized cognitive impairmentsCitation5 to improve survivors’ global functioning.
Surgery is usually conducted with the goal to completely remove breast tumors, either by mastectomy or lumpectomy, and to assess the status of the axillary lymph node, either through sentinel lymph node biopsy (SLNB) or axillary lymph node dissection (ALND).Citation6,Citation7 Often, post-surgery rehabilitation focuses on the more obvious side effects, with pain and physical impairments being reported as the most debilitating complications after surgery. Therefore, commonly reported are upper body symptoms such as shoulder functions, breast/arm swelling (or lymphedema) with deformity, impairment of functionality, physical discomfort and numbness of the skin on upper arm and impaired arm.Citation8–Citation10 Reports from lymphedema studies showed it occurs in 10%–50% of women who underwent ALND and among 5%–20% of women who underwent SLNB.Citation11 Post-operative, long-term pain has also been reported in 12%–50% of women with breast cancer, usually due to nerve injuries during surgery.Citation12
Prevalence of cognitive impairment occurs in 10%–50% of women.Citation7,Citation13 It impacts on daily living performances (activities of daily living, work, and leisure tasks) and the overall quality of life (QoL), but is often ignored, partly because its cause cannot be identified. Furthermore, occupational outcomes, such as time needed to return to work, work absenteeism, and sick leave or employment status is also a concern of breast cancer survivors.Citation14–Citation16 Emotional distress caused by shifts in social support, and fear of recurrence and death has also impacted women’s wellbeing.Citation17,Citation18 However, the rehabilitation is less commonly reported and includes the less obvious psychosocial functioning, including anxiety and depression, and where esthetic deformity or affected body image have been implicated leading to poor coping strategies.Citation19 As such, these after-effects from the post-operative procedures and adjuvant therapies can lead to a compromised QoL.Citation20 Holistic rehabilitation including health-promotion and health-prevention strategies, and via early Occupational therapy involvements is warranted for effective living with breast cancer.
Description of intervention
Management of long-term side effects of breast cancer treatment is important to improve QoL of breast cancer survivors.Citation21 Optimal rehabilitation includes the inputs from the various health professionals to help remediate and restore the impaired physical, psycho-social, and occupational functioning of women with breast cancer.Citation22 Some of these methods include physical-therapy,Citation23,Citation24 exercise interventions,Citation25,Citation26 psychological therapies such as psycho-education,Citation27,Citation28 occupational therapy,Citation29,Citation30 nutritional rehabilitation,Citation31 alternative rehabilitation such as yoga, music therapy,Citation32,Citation33 and complex rehabilitation.Citation34
Aim
This review aims to examine systematic reviews on the rehabilitation methods for post-operative women with breast cancer, with a view on the comprehensiveness of these methods used, and if they consider breast cancer as a chronic illness. The findings may help inform suitable treatment decisions towards post-operative complications and the after-effects so that survivors can live for indefinite periods, with breast cancer taking a form of chronic illness.
Methods
Search terms
Systematic reviews were searched in four databases, restricted to full-text English language publications, which were published between January 2009 and October 2014, on adult women with breast cancer including The Cochrane Database of Systematic Reviews, the Database of Abstracts of Reviews of Effects, PubMed, and ScienceDirect.
The titles, abstracts, and keywords were searched for the following terms in order to identify the required articles: ‘breast cancer’, ‘breast carcinoma’, ‘surgery’, ‘rehabilitation’, ‘treatment’, ‘therapy’, ‘physical therapy’, ‘occupational therapy’, ‘psychological’, ‘psychosocial’, ‘exercise’, ‘physical activity’, ‘cognitive’, ‘occupational’, ‘alternative’, ‘complementary’, and ‘systematic review’. Search terms were identified by means of the inclusion and exclusion criteria specified in the PICOS (Population, Intervention, Comparator, Outcomes, and Study designs) table (). Boolean operators “AND”, and “OR” and search filter “asterisks (*)” were used together with the search terms to ensure all keyword variations were searched. Grey literature was excluded.
Table 1 PICOS inclusion and exclusion criteria
Selection of reviews
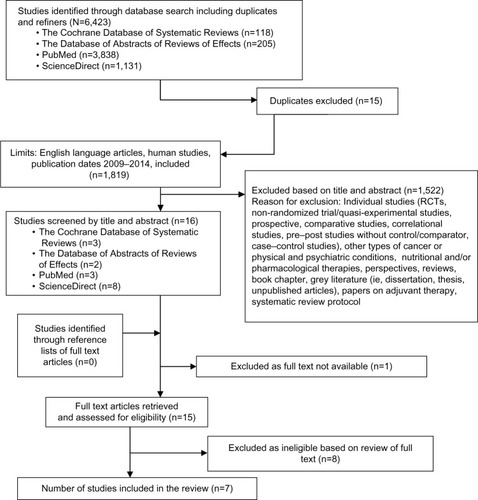
The electronic searches resulted in a number of studies uncovered from each database and was recorded immediately as shown in . The online reference manager (EndNote) was used to remove any duplicates. Reviews were reviewed by one reviewer (ANM) to first assess their eligibility by reading the title and the abstract of each study.
Figure 1 Flow diagram of systematic review process.
Participants
Systematic reviews which include a sample of post-surgery breast cancer adults (aged 18 years and over) were included. Reviews were excluded if the sample had other types of non-breast cancer.
Intervention
Systematic reviews on the effectiveness of single/combined (complex) rehabilitation eg, physical/occupational therapy, exercise, psychological, occupational, cognitive, nutrition, and alternative methods for post-operative breast cancer. The interventions included:
Physical therapy – complex decongestive therapy, manual lymph drainage (MLD), standard physiotherapy, occupational therapy etc.
Physical exercise – home based and instructed exercise.
Psychosocial – cognitive behavior therapy (CBT), psycho-education, etc.
Nutritional – change in dietary habits, dietary regime, etc.
Alternative – yoga, music therapy, acupuncture, etc.
Complex – combined interventions eg, counseling and exercise.
Types of studies
All published systematic reviews in the English language, on rehabilitation programs (for a combination of dysfunctions) were selected. The programs could have been physical or exercise or psychological or cognitive or occupational or nutritional or alternative or complex rehabilitation. There were no restrictions on the type of systematic review, ie, systematic reviews of randomized controlled trials (RCTs), uncontrolled trials, non-randomized studies, qualitative, etc, provided that the aim of the study was to investigate the effects of either single or combinational rehabilitation methods/programs for post-operative patients with breast cancer. Systematic reviews were excluded if they focused on one narrow aspect or just one modality (eg, just specifically arm lymphedema as the outcome) and/or if there is less than four studies in the review paper, or it utilized less than three databases to search for individual studies.
Outcome measures
Systematic reviews on the physical, cognitive, occupational, and psychological outcomes in post-operative breast cancer patients were included:
Physical outcomes – shoulder mobility, lymphedema, wound healing, fatigue, etc.
Psychological outcomes – QoL, anxiety, depression, mood, and stress.
Cognitive outcomes – memory, attentiveness, “chemo-brain”, etc.
Occupational outcomes – return to work, absenteeism, etc.
Lifestyle redesign – preventive and health promotion methods.
Eligibility criteria
The present systematic review included published systematic review articles in the English language between the years 2009 and 2014. Unpublished reviews (grey literatures) were not included in the review. Inclusion criteria were kept relatively broad to ensure comprehensiveness in assessing the various rehabilitation methods reviewed in previous systematic reviews.
Data extraction and synthesis of results
Reviews were selected based on inclusion and exclusion criteria as depicted in the flow diagram (). All relevant reviews accessed were followed-up to establish inclusion. The information extracted included data from the data extraction table () guided by a previous systematic review of reviews.Citation35 The data were extracted by one researcher (ANM) which was guided, assessed, and reviewed by a senior researcher (SYL). It was expected that there would be heterogeneity in the outcomes measured.
Risk of bias in individual studies
Methodological quality of included systematic reviews was independently rated according to the “assessment of multiple systematic reviews” (AMSTAR) tool.Citation36 Responses of the AMSTAR tool are ‘yes’, ‘no’, ‘can’t answer’, or ‘not applicable’, with yes being rated as ‘1’, and ‘no’, ‘can’t answer’, or ‘not applicable’ rated as ‘0’. Based on this scale, reviews were rated as ‘low’, ‘moderate’ or ‘high’ quality. The domains identified in the 11-item tool are presented in .
Table 2 A 11-item “assessment of multiple systematic reviews” (AMSTAR) for assessing systematic reviews
Results
Study selection
is the flow chart of the systematic review process from four databases (Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, PubMed, and ScienceDirect), which yielded seven full-text systematic reviews,Citation7,Citation22,Citation37–Citation41 and excluded eight full-text reviews.Citation8,Citation42–Citation48 Reasons for the exclusion of reviews are stated in the screening inclusion and exclusion table ().
shows the AMSTAR tool for assessing methodological quality or rigor of each review included. Based on the AMSTAR tool, three out of the seven reviews reported were of good methodological quality,Citation22,Citation37,Citation38 with three RCTs of medium quality,Citation7,Citation39,Citation40 and one review of low quality.Citation41 All but one systematic reviewCitation41 had ensured at least two independent researchers had been involved in data extraction, or at least one researcher had checked the other’s work. All, but one reviewCitation7 had ensured a comprehensive literature search (ie, a search strategy using more than two databases and one supplementary strategy that uses review of references in individual studies). Only one systematic reviewCitation38 had searched for and attained unpublished or grey literature. Three reviewsCitation22,Citation37,Citation38 had ensured a list of included and excluded studies, with reasons for inclusion and exclusion provided. Methodological quality assessments of included studies were measured in all, but one review.Citation41 However, only two reviewsCitation38,Citation40 had considered the methodological quality of each individual study in carrying out a conclusion or recommendation of rehabilitation methods. All, but two reviewsCitation7,Citation41 had assessed heterogeneity of included studies reviewed. Publication bias was assessed. In two reviewsCitation38,Citation39 publication bias could not be assessed since the number of included studies was less than 20.
Table 3 AMSTAR (assessment of multiple systematic reviews) checklist
Characteristics of included reviews
A summary of the review is presented in , outlining its year of publication, aim, search strategy used, inclusion and exclusion criteria, number and design of included studies in each review, total number and age of participants, and outcomes measured.
Table 4 Characteristics of systematic reviews on rehabilitation methods after breast cancer surgery
Description of methods
The selected systematic reviews vary considerably in terms of the designs of the studies included, type of rehabilitation methods, and search strategy (databases used, publication years and language restriction, and search terms) (). Five out of the seven systematic reviews were RCTs.Citation22,Citation37–Citation40 One review included both controlled and uncontrolled quantitative trials.Citation41 Another study included qualitative studies only.Citation7 Three reviews had specifically investigated physical rehabilitation methods: two papers were on the efficacy of various types of exercise,Citation37,Citation38 whilst one was on weight training exercises.Citation39 One review investigated psychosocial interventions,Citation40 another the efficacy of occupational rehabilitation on women with breast cancer,Citation41 and one explored cognitive functioning.Citation7 Only the review by Juvet et alCitation22 covered a holistic range of rehabilitation methods – physical activity rehabilitation, psychosocial rehabilitation, nutritional rehabilitation, complementary or alternative rehabilitation (ie, yoga, music therapy, etc), and complex (psycho-education plus counseling) rehabilitation for women after breast cancer.Citation22
For each of the resulted review, we had searched in more than one database for individual studies (refer to ). Restriction of publication years and language varied across the seven reviews. Chan et alCitation37 included published articles between the years 2000 and 2009. Paramanandam and RobertsCitation39 restricted review to articles dated between 2001 and 2012, Fors et alCitation40 included published articles between the years 1999 and 2008, Hoving et alCitation41 included articles between the years of 1970 and 2007, Juvet et alCitation22 included published articles up until 2008, and Selamat et alCitation7 included articles restricted to those published from 2002 to 2014. One reviewCitation38 included both published and unpublished literature until 2008. Three reviewsCitation7,Citation37,Citation39 restricted articles to the English language only. One reviewCitation38 did not have any language restrictions. Three reviewsCitation22,Citation40,Citation41 did not specify language restrictions. All reviews specified the various search terms used.
Description of participants
The total number of participants was specified in all seven reviews. The age of participants was specified in three reviewsCitation37–Citation39 only. Details of the total number and age of participants are provided in . All but three reviewsCitation38,Citation39,Citation41 specified exclusion criteria for participants. Chan et alCitation37 excluded reviews which included male participants.
Description of outcomes
Physical, psychosocial, occupational, and cognitive outcomes varied. Amongst the physical outcomes assessed were: upper body symptoms (ie, shoulder function, arm movement, limb strength),Citation37,Citation38 risk or incidence of secondary lymphedema,Citation37–Citation39 fatigue,Citation40 pain,Citation38 seroma formation,Citation38 wound drainage,Citation38 physical fitness (ie, body mass index [BMI], body composition),Citation22,Citation39 and adherence to exercise.Citation38 Amongst the psychosocial outcomes were QoL,Citation38–Citation40 mood, health behavior, and social function.Citation40 Occupational outcomes included return to work, absenteeism, work disability, sick leave or employment status measured by only one systematic review.Citation41 Cognitive outcomes include perception of “chemo-brain”, coping strategies towards cognitive dysfunction, and self-management as breast cancer survivor. Only one reviewCitation22 had attempted to look at somatic, psychological, and social outcomes as a comprehensive whole.
Findings
Effects on physical outcomes
shows the results of the effects of various rehabilitation methods on physical outcomes. Five reviews had investigated the effects of rehabilitation for physical outcomes, with adequate methodological quality: three reviews were rated as having high methodological quality,Citation22,Citation37,Citation38 and two were rated as having medium quality.Citation39,Citation40
Table 5 Results of studies on rehabilitation methods on physical outcomes
Exercise rehabilitation showed significant improvement in shoulder movement – irrespective of type or time period of implementationCitation37 but, early exercise was found to be more effective than delayed exercise.Citation38 Paramanandam and RobertsCitation39 found that gradual intensity weight training, with slow progression, improved upper and lower limb strength. More importantly, exercise did not increase risk or change in the incidence rate of lymphedemaCitation22,Citation37–Citation39 and complex decongestive therapy decreased the incidence of lymphedema as compared to standard physiotherapy.Citation22 The benefits of exercise were well reported. Early exercise (versus delayed) also helps wound healing by increasing the wound drainage volume.Citation38 There were inconclusive results for exercise interventions on BMI.Citation22,Citation39 With fatigue management, psycho-education had a significant short-term benefit,Citation40 but not cognitive behavioral therapy.Citation22,Citation40 With hot flashes, complementary rehabilitation (acupuncture, yoga, art therapy, or relaxation training) did not show conclusive evidence.Citation22 Overall, the physical rehabilitation seems to focus on shoulder range of motion, fatigue, body weight, wound, and hot flashes amongst the wide range of after-effects from breast cancer and its treatment.
Effects on non-physical related outcomes
shows the effects of rehabilitation methods on less obvious psychological, occupational, and cognitive outcomes. Of the five reviews, the methodological quality of the three reviews was rated as high quality,Citation22,Citation37,Citation38 and two reviewsCitation39,Citation40 were rated as medium quality.
Table 6 Results of studies on rehabilitation methods on psychosocial, occupational, and cognitive outcomes
QoL was assessed in three reviewsCitation22,Citation39,Citation40 as an outcome of exercise rehabilitation,Citation22,Citation39 CBT,Citation40 and psycho-educationCitation22,Citation40 albeit with inconclusive results. One reviewCitation22 found inconclusive results on the benefit of both complementary and complex decongestive therapy on QoL. Health behaviors and social function and coping were assessed in two reviewsCitation22,Citation40 with inconclusive results. There were inconclusive results of social and emotional support interventions in two reviews.Citation22,Citation40 Mood outcomes such as anxiety, event related distress, and depression assessed in two reviewsCitation22,Citation40 found that psycho-education, CBT, and social and emotional support interventions yield inconclusive results towards improving mood. There was some evidence that complementary intervention after primary breast cancer treatment was found to have a small effect on mood outcomes.Citation22
Rehabilitation methods for cognitive outcomes
Cognitive outcomes were measured in one review only.Citation7 Psychosocial interventions and practical reminders were adequate coping strategies towards cognitive dysfunction but the meta-ethnography review also found cultural differences in coping strategies, such as Asian women being more likely to use complementary medicine like medicinal herbs, to improve cognitive functioning.
Rehabilitation methods on occupational outcomes
There were inconclusive outcomes with occupational rehabilitationCitation41 – whether rehabilitation consisting of counseling or exercise would indeed decrease time needed to return to work in breast cancer survivors. However, the review showed that the extensiveness of the surgical procedures correlates with the length of time needed to return to work.
Discussion
An over-emphasis on physical dysfunction
Effectiveness of rehabilitation methods on physical, psychosocial, cognitive, and occupational outcomes vary according to numerous type/s of rehabilitation methods used. Reviews investigating physical outcomes dominate the literatures. There were relatively less systematic reviews on cognitive outcomes and occupational outcomes, both were reviewed by Selamat et alCitation7 and Hoving et alCitation41 respectively and both suggests a lack of work and acknowledgment by health professionals and survivors in this area of cognitive impairment. Exercise was found to be effective in improving shoulder mobility, limb strength, and wound healing, although it was found to be inconclusive for fatigue and body composition (ie, BMI) management, and lymphedema. In fact with the common fatigue post operation, more work is needed as there were inconclusive findings for psycho-education, CBT, and social-emotional rehabilitation for fatigue management. There were also inconclusive results for the efficacy of complementary rehabilitation (acupuncture, yoga, art therapy, or relaxation training) on hot flashes.
Overall, exercise seems to be the one rehabilitation method to improve the narrow physical outcomes eg, for shoulder mobility, and irrespective of the type of exercise implemented. The benefit of broader exercise such as exercise for lifestyle redesign for a preventive stance against cancer recurrence and for better QoL, needs more research. There are some studies, both quantitative and qualitativeCitation49,Citation50 which have highlighted barriers to exercise 5 years after diagnosis of breast cancer and uncovered many expressed psychological barriers (eg, low motivation, dislike of gym), environmental barriers (eg, employment-priority, low access to facilities, interfering seasonal weather, traffic congestion to get to the gym), and lack of time. As such, studies are also needed on interventions to overcome these barriers to exercise and to ensure adherence to exercise regimes to gain its benefit on cancer recurrences and for better quality of living during the survivorship phases.
A lack of evidence for non-physical rehabilitation methods
Reviews showed inconclusive results were found for the efficacy of rehabilitation methods using psycho-education, CBT, social-emotional support, complementary-alternative methods towards improving health behaviors and/or QoL. In general, the review of the reviews also found inconclusive results on social functioning, coping, and mood outcomes. However, complementary intervention may have a small effect on mood outcomes. Nevertheless, the studies are largely heterogeneous in terms of type, length, and components of rehabilitation methods which make the comparisons rather difficult to carry out.
For less recognized problems faced by survivors of breast cancer, qualitative research identified “chemo-brain”, and attitudinal changes towards work.Citation7,Citation51 Psycho-social rehabilitation and practical reminders were strategies proposed to improve cognitive function despite variations due to cultural differences. With occupational rehabilitation, inconclusive results were found on whether exercise or counseling rehabilitation would decrease time needed to return to work in women with breast cancer.Citation41 Qualitative findings from focus groups of multi-ethnic survivors have highlighted several barriers such as fear of environmental hazards, high job-demand, intrusive thoughts and family over-protectiveness,Citation30 as well as other socio-demographic factors eg, education, range of treatment received, strenuous physical work, fatigue, and psychological factors such as negative mood.Citation52 Future occupational studies should investigate the breadth and depth of rehabilitation methods (eg, work stamina, tolerance, psychological factors for facilitating work re-entry, work accommodations such as flexibility towards work hours etc) for enabling post-operation survivors to return to work in a design that has a control or comparison group (ie, other types of interventions, wait-list, etc).
A need for more comprehensive methods to enable living for indefinite period
Overall, the lack of evidence for non-physical rehabilitation methods highlight the lack of research work that extend beyond the rehabilitation methods for physical after-effects. The gradual acknowledgment that breast cancer is taking a form of chronic illnessCitation53 is not proportionate to the current rehabilitation methods which suggest an overall management of breast cancer as an acute/fatal condition. Amongst the important implications of this current review is that rehabilitation for women with breast cancer should be comprehensive (ie, broader rather than eg, narrowly focused on upper limb function) and proactive (rather than reactive). This stance is a better preparation of breast cancer survivors to live indefinitely with the condition and to empower them to re-engage in lifestyle modification and/or lifestyle redesign,Citation54 in order to address ill-health, and improve their wellbeing, lifespan, and QoL. The specific, but predominantly performance component rehabilitation, such as improving shoulder mobility, is effective but not sufficient to enable or inform survivors to live the best they can for the remainder of their life span. The lack of emphasis on patient self-management and occupational redesign towards a healthier lifestyle suggests a dire lack of focus on these broader aspects of life. This also showed a lack of appreciation that breast cancer is evolving into a form of chronic disease requiring a brand new platform to support its increasing numbers of survivors.
Limitations
The main limitation of this systematic review on systematic reviews is the difficulty to synthesize because of the heterogeneous nature of the methodology of each review. There were varying inclusion-exclusion criteria, different outcome measures, which leads to difficulties extracting and synthesizing the data.
Conclusion
In conclusion, the current rehabilitation methods tend to focus narrowly on performance components (particularly on physical impairments or dysfunctions). The review found evidence that exercise rehabilitation methods improves physical outcome post operation, although, inconclusive results exist on rehabilitation methods to improve the non-physical sequelae such as psychosocial, cognitive, occupational, and broader lifestyle performance factors. Clearly missing are the rehabilitation methods to enable survivors to redesign their lifestyle in tandem with living with a breast cancer condition that is taking a form of chronic disease. This calls for health prevention and illness prevention lifestyle strategies to i) control cancer recurrence and ii) to promote better QoL during the indefinite period of survivorship. With the overwhelming strong evidence that cancer risk is affected by lifestyle, future studies with higher methodological rigor should be conducted on health promotion strategies to enable healthy lifestyle.
Supplementary materials
Table S1 Screening inclusion/exclusion table
Table S2 Search strategy
Disclosure
The authors declare no conflict of interest.
Acknowledgments
English language checked by Dr Gail Boniface, Cardiff University, United Kingdom.
References
- FerlayJShinHRBrayFFormanDMathersCParkinDMEstimates of worldwide burden of cancer in 2008: GLOBOCAN 2008Int J Cancer2010127122893291721351269
- cancer.org [homepage on the Internet]American Cancer Society Cancer Facts and Figures 2012AtlantaAmerican Cancer Society Available from: http://www.cancer.org/research/cancerfactsfigures/cancerfactsfigures/cancer-facts-figures-2012Accessed January 31, 2015
- MarínÁPSánchezARArranzEEAuñónPZBarónMGAdjuvant chemotherapy for breast cancer and cognitive impairmentSouth Med J2009102992993419668023
- MeadeEDowlingMEarly breast cancer: diagnosis, treatment and survivorshipBr J Nurs20122117S4S823123699
- SelamatMHLohSYMackenzieLVardyJChemobrain Experienced by Breast Cancer Survivors: A Meta-Ethnography Study Investigating Research and Care ImplicationsPloS One201499e10800225259847
- VeronesiUCascinelliNMarianiLTwenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancerN Engl J Med2002347161227123212393819
- FisherBAndersonSBryantJTwenty-year follow-up of a ran-domized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancerN Engl J Med2002347161233124112393820
- ChungCLeeSHwangSParkESystematic Review of Exercise Effects on Health Outcomes in Women with Breast CancerAsian Nurs Res (Korean Soc Nurs Sci)20137314915925030253
- HayesSCJohanssonKStoutNLUpper-body morbidity after breast cancer: incidence and evidence for evaluation, prevention, and management within a prospective surveillance model of careCancer20121188 Suppl2237224922488698
- BosompraKAshikagaTObrienPJNelsonLSkellyJSwelling, numbness, pain, and their relationship to arm function among breast cancer survivors: a disablement process model perspectiveBreast J20028633834812390356
- KimTGiulianoAELymanGHLymphatic mapping and sentinel lymph node biopsy in early-stage breast carcinomaCancer2006106141616329134
- RietmanJSDijkstraPUHoekstraHJLate morbidity after treatment of breast cancer in relation to daily activities and quality of life: a systematic reviewEur J Surgical Oncol2003293229238
- WefelJSLenziRTheriaultRBuzdarAUCruickshankSMeyersCA‘Chemobrain’ in breast carcinoma?: a prologueCancer2004101346647515274059
- BradleyCJBednarekHLNeumarkDBreast cancer survival, work, and earningsJ Health Econ200221575777912349881
- BradleyCJNeumarkDBednarekHLSchenkMShort-term effects of breast cancer on labor market attachment: results from a longitudinal studyJ Health Econs2005241137160
- TaskilaTMartikainenRHietanenPLindbohmMLComparative study of work ability between cancer survivors and their referentsEur J Cancer200743591492017314041
- MorrowGRRoscoeJAHickokJTAndrewsPLMattesonSNausea and emesis: evidence for a biobehavioral perspectiveSupport Care Cancer20021029610511862499
- SpencerSMLehmanJMWyningsCConcerns about breast cancer and relations to psychosocial well-being in a multiethnic sample of early-stage patientsHealth Psychol199918215916810194051
- van’t SpijkerATrijsburgRWDuivenvoordenHPsychological sequelae of cancer diagnosis: a meta-analytic review of 58 studies after 1980Psychosom Med19975932802939178339
- FuMRChenCMHaberJGuthAAAxelrodDThe effect of providing information about lymphedema on the cognitive and symptom outcomes of breast cancer survivorsAnn Surg Oncol20101771847185320140528
- InagakiMYoshikawaEMatsuokaYSmaller regional volumes of brain gray and white matter demonstrated in breast cancer survivors exposed to adjuvant chemotherapyCancer2007109114615617131349
- JuvetLKElvsaasILeivsethGRehabilitation of breast cancer patientsNorwegian Knowledge Centre for the Health Services20092
- Torres LacombaMYuste SánchezMJZapico GoñiÁEffectiveness of early physiotherapy to prevent lympho-edema after surgery for breast cancer: randomised, single blinded, clinical trialBMJ2010340b539620068255
- BeurskensCHvan UdenCJStrobbeLJOostendorpRAWobbesTThe efficacy of physiotherapy upon shoulder function following axillary dissection in breast cancer, a randomized controlled studyBMC Cancer20077166
- SchmitzKHAhmedRLTroxelAWeight lifting in women with breast-cancer–related lymphedemaN Engl J Med2009361766467319675330
- CourneyaKSSegalRJMackeyJREffects of aerobic and resistance exercise in breast cancer patients receiving adjuvant chemotherapy: a multicenter randomized controlled trialJ Clin Oncol200725284396440417785708
- AntoniMHLechnerSCKaziAHow stress management improves quality of life after treatment for breast cancerJ Consult Clin Psychol20067461143115217154743
- ColemanAETulmanLSamarelNThe effect of telephone social support and education on adaptation to breast cancer during the year following diagnosisOncol Nurs Forum200532482282915990911
- LohSYYipCHPackerTQuekKFSelf-management pilot study on women with breast cancer: lessons learnt in MalaysiaAsian Pac J Cancer Prev20101151293129921198280
- TanFLLohSYSuTVelooVWNgLLReturn to work in multi-ethnic breast cancer survivors-a qualitative inquiryAsian Pac J Cancer Prev201213115791579723317258
- BlackburnGLWangKADietary fat reduction and breast cancer outcome: results from the Women’s Intervention Nutrition Study (WINS)Am J Clin Nutr2007863s878s88118265482
- ZhouKLiXLiJA clinical randomized controlled trial of music therapy and progressive muscle relaxation training in female breast cancer patients after radical mastectomy: Results on depression, anxiety and length of hospital stayEur J Oncol Nurs2014pii:S1462-3889(14)00106-9
- BanerjeeBVadirajHSRamAEffects of an integrated yoga program in modulating psychological stress and radiation-induced geno-toxic stress in breast cancer patients undergoing radiotherapyIntegr Cancer Ther20076324225017761637
- Demark-WahnefriedWCaseLDBlackwellKResults of a diet/exercise feasibility trial to prevent adverse body composition change in breast cancer patients on adjuvant chemotherapyClin Breast Cancer200881707918501061
- SmithVDevaneDBegleyCMClarkeMHigginsSA systematic review and quality assessment of systematic reviews of randomised trials of interventions for preventing and treating preterm birthEur J Obstet Gynecol Reprod Biol2009142131118996637
- SheaBJGrimshawJMWellsGADevelopment of AMSTAR: a measurement tool to assess the methodological quality of systematic reviewsBMC Med Res Methodol200771017302989
- ChanDNLuiLYSoWKEffectiveness of exercise programmes on shoulder mobility and lymphoedema after axillary lymph node dissection for breast cancer: systematic reviewJ Adv Nurs2010661902191420626480
- McNeelyMLCampbellKOspinaMExercise interventions for upper-limb dysfunction due to breast cancer treatmentCochrane Database Syst Rev20106CD00521120556760
- ParamanandamVSRobertsDWeight training is not harmful for women with breast cancer-related lymphoedema: a systematic reviewJ Physiother201460313614325086730
- ForsEABertheussenGFThuneIPsychosocial interventions as part of breast cancer rehabilitation programs? Results from a systematic reviewPsychooncology201120990991820821803
- HovingJLBroekhuizenMLAFrings-DresenMHReturn to work of breast cancer survivors: a systematic review of intervention studiesBMC Cancer20099111719383123
- E LimaMTE LimaJGde AndradeMFBergmannALow-level laser therapy in secondary lymphedema after breast cancer: systematic reviewLasers Med Sci20142931289129523192573
- HuangTWTsengSHLinCCEffects of manual lymphatic drainage on breast cancer-related lymphedema: a systematic review and meta-analysis of randomized controlled trialsWorld J Surg Oncol2013111523347817
- JohannsenMFarverIBeckNZachariaeRThe efficacy of psychosocial intervention for pain in breast cancer patients and survivors: a systematic review and meta-analysisBreast Cancer Res Treat2013138367569023553565
- KhanFAmatyaBNgLDemetriosMZhangNYTurner-StokesLMultidisciplinary rehabilitation for follow-up of women treated for breast cancerCochrane Database Syst Rev201212CD00955323235677
- MarkesMExercise for Women Receiving Adjuvant Therapy of Breast-Cancer: A Systematic Review. [doctoral dissertation]Technical University of BerlinBerlin, Germany2011
- MoseleyALPillerNBCaratiCJThe effect of gentle arm exercise and deep breathing on secondary arm lymphedemaLymphology200538313614516353491
- ShamleyDRBarkerKSimoniteVBeardshawADelayed versus immediate exercises following surgery for breast cancer: a systematic reviewBreast Cancer Res Treat200590326327115830140
- HefferonKMurphyHMcLeodJMutrieNCampbellAUnderstanding barriers to exercise implementation 5-year post-breast cancer diagnosis: a large-scale qualitative studyHealth Educ Res201328584385623969632
- LohSYChewSLQuekKFPhysical activity engagement after breast cancer: Advancing the health of survivorsHealth20135838846
- KennedyFHaslamCMunirFPryceJReturning to work following cancer: a qualitative exploratory study into the experience of returning to work following cancerEur J Cancer Care (Engl)2007161172517227349
- IslamTDahluiMMajidHAFactors associated with return to work of breast cancer survivors: a systematic reviewBMC Public Health201414Suppl 3S825437351
- LohSYYipCHBreast cancer as a chronic illness: implications for rehabilitation and medical educationJournal of the University of Malaya Medical Centre200692311
- LeeJELohSYPhysical Activity and Quality of Life of Cancer Survivors: A Lack of Focus for Lifestyle RedesignAsian Pac J Cancer Prev20131442551255523725173