Abstract
Background
We aimed to evaluate the prognostic significance of the preoperative tumor-marker cancer antigen (CA) 15.3 in Saudi patients with breast cancer and to find out whether any correlation exists between preoperative CA 15.3 and tumor size and nodal status.
Materials and methods
Preoperative blood samples for serum CA 15.3 levels were taken in 112 breast cancer patients who underwent breast-conserving surgery or modified radical mastectomy between February 1988 and August 2008. Serum levels of CA 15.3 below 35 U/mL were considered normal. The correlation between pre- and postoperative CA 15.3 levels with tumor size and nodal status was calculated using Pearson correlative coefficients. Kaplan–Meier curves were used to determine disease-free survival (DFS) according to CA 15.3 groups (<35, 36–100 and above >100 U/mL).
Results
The mean age of the cohort was 47.0 years (range 23–76, standard deviation 10.3). According to menopausal status, 93 patients (83.0%) were premenopausal, and 19 patients (17.0%) were postmenopausal. Mean preoperative CA 15.3 levels were 43.69 U/mL (1.0–209.87). Ten-year DFS rates were 100%, 84%, and 57.7% for CA 15.3 <35 U/mL, 36–100 U/mL, and >100 U/mL, respectively (P = 0.003). Preoperative CA 15.3 levels showed positive correlation with primary tumor size (R = 0.43, R2 = 0.83, P = 0.03) and nodal status (R = 0.59, R2 = 0.28, P < 0.0001), respectively.
Conclusion
Elevated preoperative CA 15.3 above 35 U/mL in Saudi women breast cancer patients showed correlation with primary tumor size and nodal status, and preoperative CA 15.3 level is an independent prognostic factor for DFS. Preoperative serum CA 15.3 levels may be helpful for risk stratification along with other factors.
Introduction
Breast cancer incidence is increasing globally, and the same is reflected in Saudi Arabia. Breast cancer in Saudi Arabia accounts for 26% of all newly diagnosed cancers in Saudi women, with an incidence of 21.6 per 100,000, and the majority of those present at a young age and with advanced TNM staging.Citation1,Citation2
Serum cancer antigen (CA) 15.3 is a carbohydrate antigen that is secreted from breast cancer cells. It has been the most widely used marker in the last two decades in breast cancer patients for neoadjuvant chemotherapy response and prognosis along with other parameters because of its high sensitivity and specificity.Citation3 However, the significance of preoperative CA 15.3 levels is not well known.Citation4 A few studies have supported an association between high preoperative CA 15.3 and tumor burden (advanced tumor and nodal status), and others have not.Citation5,Citation6 Apart from the prognostic significance for response evaluation, the impact of preoperative CA 15.3 on locoregional control (LRC), distant metastatic control (DMC), and disease-free survival (DFS) is also less studied and its significance not known in Middle Eastern patients with breast cancer.Citation7
Our single-institution study aimed to evaluate the prognostic significance of preoperative tumor CA 15.3 in Saudi patients with breast cancer, and also to find out the existence of any correlation of preoperative CA 15.3 with tumor size and nodal status.
Materials and methods
After receiving approval from the institutional ethical review committee board, we took into this study 112 consecutive patients with breast cancer in whom breast-conserving surgery (BCS) or modified radical mastectomy (MRM) was performed between February 1988 and August 2008 in our hospital. Inclusion criteria were (1) histopathologically confirmed breast cancer, (2) T1–T4, N0–N2, (3) and had undergone BCS or MRM with or without adjuvant hormonal chemotherapy and radiotherapy. Exclusion criteria were (1) presence of distant metastasis, (2) neoadjuvant chemotherapy (as our aim was to see the impact of preoperative CA 15.3 levels in chemotherapy-naïve patients at the time of presentation), and (3) inflammatory or inoperable tumors.
Preoperative serum CA 15.3 levels were determined by enzyme linked immunoassay (BioCheck, Foster City, CA, USA) after taking venous blood samples and centrifugation and processing the serum. Normal levels of serum CA 15.3 were considered normal below or equal to 35 U/ml. According to CA 15.3 levels, patients were grouped into three categories (<35, 36–100, and >100 U/mL).
Breast cancer pathological specimens
After surgery, breast cancer specimens were fixed in 10% formalin for 12 hours and were examined to evaluate the gross size, histopathological type, grade, presence or absence of lymphovascular invasion, lymph nodes, and retrieved and involved number. Estrogen receptors (ERs), progesterone receptors (PRs), and HER2/neu (human epidermal growth factor receptor 2)-overexpression status underwent immunohistochemical analysis with antibodies against the ERs (Dako, Glostrup, Denmark) and PRs (BioGenex, San Ramon, CA, USA). A cutoff value of 1% for both receptors was considered ER or PR presence, as per institutional protocol. HER2/neu overexpression was checked for immunohistochemical equivocal cases using a HER2 DNA Probe Kit (Abbott Laboratories, Abbott Park, IL, USA) according to the instruction manual. HER2/neu was considered positive when the HER2:CEP17 ratio was 2:1 or higher.
Clinical variables
Additional clinical features, ie, age, menopausal status, associated comorbidities, initial tumor size on physical, mammography and sonography examination, laterality and location of primary tumor, were studied. Surgery was performed using either wide local excision or MRM with axillary lymph-node dissection.
Statistical analysis
The primary end points were frequency preoperative CA 15.3 levels and correlation with tumor size and lymph-node involvement, impact of preoperative CA 15.3 levels on LRC, DMC, and DFS. The mean, median, and mode of preoperative serum CA 15.3 levels were described. The correlation between preoperative CA 15.3 and tumor size/lymph-node involvement was estimated by Pearson correlative coefficients and the Kruskal–Wallis test. The mean differences and limits of agreement corresponding to the 95% confidence interval were analyzed.
The times to last follow-up evaluation, appearance of local relapse, and death were calculated from date of starting treatment. DFS was defined as the duration between the entry date and the date of documented disease reappearance, death from cancer, and/or last follow-up (censored). Overall survival was defined as the duration between the entry date and the date of patient death or last follow-up (censored). Probabilities of LRC, DMC, and DFS were determined with the Kaplan–Meier method. The comparisons for various end points were performed using the log-rank test and Cox proportional hazard analysis. All statistical analyses were performed using PASW statistics 18.0 (IBM, Armonk, NY, USA).
Results
Clinical characteristics
Patients’ clinical and treatment characteristics are shown in . The mean age of cohort was 47.0 years (range 23–76, standard deviation 10.3). According to menopausal status, 93 patients (83.0%) were premenopausal and 19 patients (17.0%) were postmenopausal. Mean body mass index was 31.8 kg/m2 (range 15.7–52.8, standard deviation 7.2). A total of 72 patients (64.3%) had no comorbidities. Common morbidities in 40 patients (35.7%) were hypertension in 14 (12.5%), diabetes in nine (8.0%), and combined hypertension and diabetes in six (5.4%). Family history was positive in 17 patients (15.2%). The majority of the cohort (57 patients, 79.6%) had left-side breast cancer and the outer lower quadrant was a common site of tumor location (50 patients, 45.9%), followed by the upper outer quadrant (30 patients, 27.5%). Elevated preoperative CA 15.3 levels were seen in 96 patients (85.7%), with a mean value of 43.69 U/mL (1.0–209.87).
Table 1 Patient characteristics
Correlation of preoperative CA 15.3 with tumor size and axillary nodal involvement
The clinicopathological characteristics according to preoperative CA 15.3-level groups are shown in . Preoperative serum CA 15.3 levels were correlated with young age, premenopausal status, advanced TNM Classification of Malignant Tumours (TNM) staging, grade 3, and receptor status. Elevated CA 15.3 levels were correlated with triple-negative and HER2/neu status. Correlation of CA 15.3 levels with tumor size and nodal involvement are shown in and . Elevated preoperative CA 15.3 levels were positively correlated with primary tumor size (R = 0.43, R2 = 0.83, P = 0.03) and nodal status (R = 0.59, R2 = 0.28, P < 0.0001).
Figure 1 Correlation between preoperative serum cancer antigen (CA) 15.3 levels and postoperative primary tumor (T) stage.
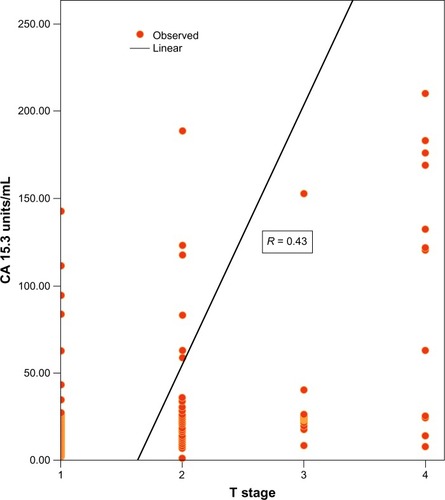
Figure 2 Correlation between preoperative serum cancer antigen (CA) 15.3 levels and postoperative axillary nodal (N) status.
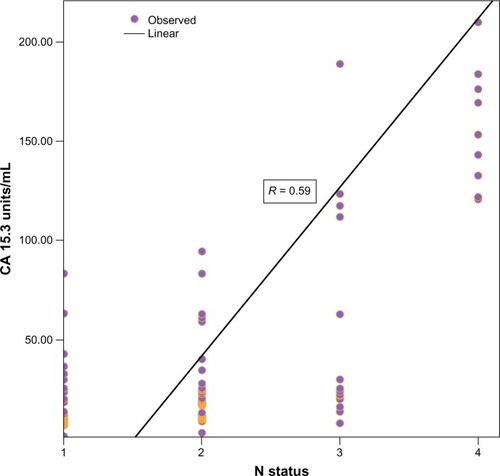
Table 2 Clinicopathological characteristics according to serum cancer antigen (CA) 15.3 groups
Locoregional recurrence, distant control, and overall survival
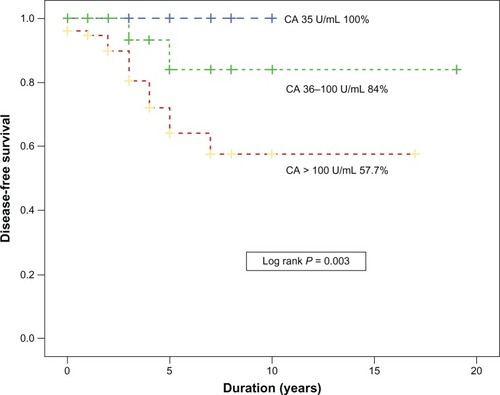
Ten locoregional recurrences (LRRs; 8.93%) were seen among 112 breast cancer patients. Four (40%) LRRs occurred at the scar site, and six LRRs (60%) were seen in the ipsilateral axilla and supraclavicular regions. The median time of LRR was 3.6 years (range 2.73–5.1). The 10-year actual LRC rate was 86.4%. Distant metastases were documented in 29 patients at 10 years, with 10 actual DMC rates averaging 63% (95% confidence interval 57%–79.0%). Ten-year DFS rates were 100%, 84%, 57.7% in CA 15.3 <35 U/mL, 36–100 U/mL, and >100 U/mL, respectively (P = 0.003). In preoperative CA 15.3 groups, there was no difference between LRRs; however, CA 15.3 above 35 U/mL had worse DMC and DFS rates ().
Figure 3 Disease-free survival according to cancer antigen (CA) 15.3-level groups.
Cox proportional analysis of clinical and histopathological prognostic factors in our cohort showed four prognostic factors influencing the LRRs: (1) age less than 45 years, (2) premenopausal status, (3) presence of lymphovascular invasion, and (4) no adjuvant radiotherapy (). For DMC, in addition to age less than 45 years, premenopausal status, and breast cancer subtypes, elevated preoperative CA 15.3 levels were found to be an independent prognostic factor ( and ).
Table 3 Cox regression (multivariate) analysis of prognostic factors for locoregional recurrence in breast cancer
Table 4 Cox regression (multivariate) analysis of prognostic factors for distant metastasis in breast cancer
Table 5 Cox regression (multivariate) analysis of prognostic factors for disease-free survival in breast cancer
Discussion
Correlation of preoperative serum CA 15.3 levels with primary tumor size and nodal status and its prognostic significance on DMC and DFS in patients with breast cancer has been demonstrated in Western dataCitation5,Citation8; however, the impact of preoperative CA 15.3 levels in Middle Eastern women with breast cancer has not been well studied.Citation8–Citation10 In our region, women with breast cancer present at a young age, mostly premenopausal, and with advanced TNM stage and high HER2/neu expression (32.2%), which are well-known prognostic factors for tumor and nodal stage in breast cancer. Similar findings were seen in our small cohort, and we confirmed the correlation of elevated preoperative CA 15.3 with young age, premenopausal status, advanced TNM staging, histological grade, and basal and HER2/neu-type receptors, and also confirmed preoperative CA 15.3 levels as independent prognostic factors for DMC and DFS, similar to Western data.Citation11,Citation12
Potential strengths of our study were complete data of preoperative serum CA 15.3 in all patients and a long follow-up period, and possible limitations of our study were that (1) we did not take postoperative blood samples for serum CA 15.3 levels, (2) ours was a small cohort, and (3) patients receiving neoadjuvant chemotherapy were excluded, as our aim was to see the impact of preoperative CA 15.3 on DFS in neoadjuvant chemotherapy-naïve patients. Bottini et al have reported that serum CA 15.3 levels did not substantially change after neoadjuvant chemotherapy, despite the high response rate obtained after surgery.Citation13
In conclusion, our data in patients with breast cancer suggest that elevated preoperative CA15.3 levels are associated with advanced TNM staging, histological grade, and basal and HER2/neu-receptor status, and thus a high risk of recurrence locally or at distant sites. We found preoperative CA 15.3 level an independent prognostic factor for DFS. Although the American Society of Clinical Oncology panel does not recommend therapeutic decisions be based on preoperative serum CA 15.3, we recommend the incorporation of routine preoperative CA 15.3 levels in our patients based on the aforementioned studies, and such patients with elevated preoperative serum CA 15.3 levels may benefit from aggressive treatment. However, larger prospective trials are required to predict the significance of preoperative serum CA 15.3 levels on LRC, DMC, and DFS in breast cancer patients.
Disclosure
The authors report no conflicts of interest in this work.
References
- Saudi Arabia Cancer Incidence and Survival Report 2007 [webpage on the Internet]Saudi ArabiaSaudi Cancer Registry2007 Available from: http://ghdx.healthmetricsandevaluation.org/record/saudi-arabia-cancer-incidence-and-survival-report-2007Accessed July 2, 2013
- IbrahimEMZeeneldinAASadiqBBEzzatAAThe present and the future of breast cancer burden in the Kingdom of Saudi ArabiaMed Oncol20082538739318317955
- MiyaTWatanabeTAdachiIAnalysis of cytosol CA15-13, carcinoembryonic antigen, and estrogen and progesterone receptors in breast cancer tissuesJpn J Cancer Res1992831711771555999
- DuffyMJCatherineDRachelKHigh preoperative CA 15.3 concentrations predict adverse outcome in node-negative and node-positive breast cancer: study of 600 patients with histologically confirmed breast cancerClin Chem20045055956314726467
- SandriMTSalvaticiMBotteriEPrognostic role of CA15.3 in 7942 patients with operable breast cancerBreast Cancer Res Treat201213231732622065291
- LumachiFBrandesAAErmaniMBrunoGBoccagniPSensitivity of serum tumor markers CEA and CA 15-13 in breast cancer recurrences and correlation with different prognostic factorsAnticancer Res2000204751475511205212
- GünczlerPOgrisEMacaSDanmayrETumor markers in breast cancer: on the diagnostic value of serum determinations in clinical freedom from tumor and manifest diseaseOnkologie198912209214 German2685686
- MolinaRAugéJMEscuderoJMEvaluation of tumor markers (HER-2/neu oncoprotein, CEA and CA 15.3) in patients with locoregional breast cancer: prognostic valueTumour Biol20103117118020361287
- BahramiAMortazavizadehMRYazdiMFChamaniMSerial tumour markers serum carcinoembryonic antigen and cancer antigen 15-13 assays in detecting symptomatic metastasis in breast cancer patientsEast Mediterr Health J2012181055105923301361
- ElfagiehMAbdallaFGliwanABoderJNicholsWBuhmeidaASerum tumour markers as a diagnostic and prognostic tool in Libyan breast cancerTumour Biol2012332371237722948780
- MorcosNYZakharyNISaidMMTadrosMMPostoperative simple biochemical markers for prediction of bone metastases in Egyptian breast cancer patientsEcancermedicalscience2013730523653670
- KhatcheressianJLHurleyPBantugEBreast cancer follow-up and management after primary treatment: American Society of Clinical Oncology clinical practice guideline updateJ Clin Oncol20133196196523129741
- BottiniABerrutiATampelliniMInfluence of neoadjuvant chemotherapy on serum tumor markers CA 15-13, MCA, CEA, TPS and TPA in breast cancer patients with operable diseaseTumor Biol199718301310