
Abstract
Notwithstanding the advances in tumor research, diagnosis, and treatment, breast cancer is still a challenge worldwide. This global burden of disease has been associated with population aging and the persistence of cancer-related behaviors. The number of women diagnosed with breast cancer has been estimated as increasing, especially in middle-income countries such as Brazil. Estimates from the Instituto Nacional de Câncer (INCA) point to breast cancer as the major malignant neoplasia in Brazilian women and the main cause of death from cancer in the country. This fact has been associated with increased life expectancy, urbanization, and cancer-related behaviors. Given this scenario, it is clear that there is a need for identifying and discussing which factors have substantially contributed to this growing number of cases in Brazil, including access to treatment, prevention and early diagnosis, weaknesses of the local health policy, and intrinsic genetic peculiarities of the Brazilian population. This review aims to address the role of such factors.
Breast cancer epidemiology in Brazil
Brazil currently has a population of about 200 million people, with a variety of ethnicities distributed in a wide territory that is divided into five geographic regions (). In 2010, the Brazilian population was composed of 48% Caucasians, 44% multiracial, and 7% African descent.Citation1 The health system is organized as two types: the public health system (called Sistema Único de Saúde [SUS]) and the private system, supported individually by the population. It is estimated that about 75% of the population are currently users of the public health system.
Figure 1 Representative geographic distribution of Brazilian macroregions and their respective cancer estimates for the year 2014.

SUS was created in 1988, during the reformulation of the Brazilian Federal Constitution, through a law known as Organic Law of SUS (Lei Orgânica do SUS 8.080), aiming to ensure the complete access of all Brazilians to a public and unpaid health system. Thenceforth, the SUS has become one of the most important social achievements known in the world to aim to ensure free access to health care. The principles that guide this initiative are based on the decentralization and universalization of health services.Citation2
In spite of the efforts to improve diagnosis and treatment, breast cancer is one of the main challenges faced by the Brazilian government. Global statistics demonstrated that 60% of deaths related to breast cancer occur in economically developing countries such as Brazil.Citation3 The Instituto Nacional de Câncer (INCA) is responsible for providing the epidemiological data regarding cancer statistics in the country, and registers data from different regions of Brazil (). The southern region has the highest incidence rates of breast cancer.
It was estimated that about 13,000 women died from breast cancer in 2010.Citation4 Over the last few decades, breast cancer has been pointed to as the leading cause of death from cancer among Brazilian women, as well as the main malignant cancer that affects the female population. Azevedo and MendonçaCitation5 analyzed the breast cancer statistics for 1986, before the implementation of SUS. They showed that 12.8% of Brazilian women died in that year due to cancer causes, and breast cancer was the leading cause of those deaths. Surprisingly, the authors described that the incidence rates of breast cancer were 176.9 cases per 100,000 women in the south region, reaching 277.3 cases per 100,000 women in Sao Paulo in the early 1980s.
Another analysis, published by Moraes in 1998,Citation6 after SUS policy implementation and initial consolidation, revealed that the total number of breast cancer cases was about 32,000 – of which 6.6% were deaths from cancer in that year. Additionally, the author highlighted the huge heterogeneity observed throughout the different geographic regions of the country, in which the rates of disease could vary from 29.15 cases per 100,000 women in the north region to 66.12 cases per 100,000 women in the South Region. Importantly, since that time, the staging profile of women with breast cancer in Brazil was characterized by advanced stages of the disease, evidencing the late diagnosis as a national public health issue. It is important to highlight that Brazil has a diverse ethnic population.
Interestingly, we can observe that the incidence of breast cancer in South American countries is half that of European countries (about 44 cases per 100,000 Latin women versus 84 cases per 100,000 women in Northern Europe). On the other hand, although there is a substantial difference in the number of cases, the mortality rates are similar.Citation7 This reinforces the fact that developing countries such as Brazil are subject to severe problems regarding the access to health services, diagnosis, and modern treatments.
Mortality rates of breast cancer in Brazil
Overview
shows the profile of deaths by breast cancer in Brazil according to the DATASUS online database.Citation8 During the period ranging from 1992–2012, a progressive increase in the mortality rates due to breast cancer disease in Brazil was observed. Furthermore, shows the number of deaths associated with breast cancer and specific age groups in the period 1992–2012.Citation8 The highest number of deaths is observed in the age group ranging from 50–69 years (45.5% of the cases). In this context, several factors must be considered, especially regarding the increased number of death notifications related to this disease. Concerning this issue, INCA and DATASUS implemented the SISMAMA, an online tool that registers information about breast and gynecological cancer screening.Citation9 In the period from 2009–2013, the SISMAMA registered more than 12 million mammograms nationwide. About 1.4% of these cases indicated a high cancer risk, corresponding to approximately 168,000 cases. An important set of mammograms report pathological alterations in women aged over 40 years, which may be related to aging.Citation10,Citation11
Figure 2 Breast cancer mortality rates in Brazil in the period 1992–2012.
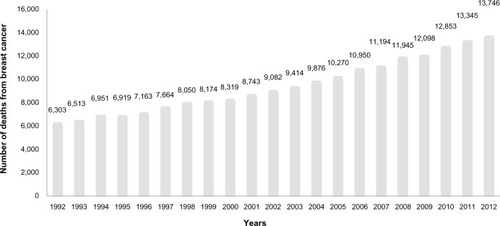
Table 1 Number of deaths associated with breast cancer and specific age groups in the period 1992–2012
The contributions of specific risk factors for explaining breast cancer rates in Brazilian women are considered and discussed as follows.
Biological features
In part, the deaths associated with breast cancer may be associated with the aggressive biological profile of tumors. The determination of the molecular cancer subtype is globally achieved by immunohistochemical analysis. In Brazil, testing for the molecular markers of breast cancer is not standardized, and it is not present in all cancer centers.Citation4 Data concerning the immunohistochemical profiling of breast cancer in patients attended by SUS have demonstrated that the Brazilian women with breast cancer presents a similar molecular pattern of disease when compared to other regions of the globe, with predominance of the luminal subtype among the affected population,Citation12–Citation16 which represents a good prognosis for treatment response and disease survival. Endocrine and genetic factors are among the main prognostic determinants for breast cancer.Citation17
Molecular studies have shown the presence of pivotal known gene modifications in breast tumors, such as BRCA mutations, especially in Brazil. BRCA is the main known gene that confers breast cancer susceptibility, and one of the first studies reporting such mutations in Brazilian women with familial history was reported by Dufloth et al in 2005.Citation18 The authors reported that the prevalence of BRCA1/BRCA2 mutations in Brazilian women in the southern region diagnosed with breast cancer was 13%. Other studies have been conducted to investigate the prevalence of BRCA-related mutations in Brazil. An investigation aiming to investigate the risk factors associated with hereditary breast and ovarian cancer syndrome was conducted by Ewald et al.Citation19 The authors identified a high frequency of BRCA founder mutation (c.5266dup) in Brazilian women diagnosed with bilateral breast cancer (5% of 137 investigated women). It is important to highlight that this prevalence is similar to that found in other populations.Citation20 Finally, as is happening worldwide, the aging of the Brazilian population is increasing year by year.Citation21
Population screening and early diagnosis
The current methods available for breast cancer screening and diagnosis are able to detect the disease at early stages. Among the variety of factors that contribute to the high mortality of breast cancer worldwide, the lack of availability of early detection services is a global problem for developing countries.Citation3 Although mammograms are encouraged by the SUS and offered without any cost to the target female population, the screenings often fail to provide accurate results. Undoubtedly, the delay that occurs between the initial suspected lesion and the confirmation of diagnosis affects the outcome profiling of breast cancerCitation21 and is still a problem in Brazil.
TNM (tumor, node, metastasis) staging of women diagnosed with breast cancer in Brazil is presented predominantly as advanced disease. A prospective study from the Grupo Brasileiro de Estudos do Câncer de Mama (GBECAM) assessed epidemiological data from women diagnosed with breast cancer in all Brazilian regions and showed that about 40% of diagnosed women were staged at TNM III–IV. The results revealed that the median age at diagnosis of such patients is about 58 years, and indicated that these women with breast cancer assisted by SUS presented advanced disease at diagnosis and poor prognosis, probably due to reduced access to modern therapies.Citation22
Brazil uses the Breast Image Reporting and Data System (BI-RADS) to categorize the results obtained from mammogram screenings.Citation9 An overview of the BI-RADS classification of mammograms in Brazilian women for breast cancer screening is presented in . In accordance with Ministry of Health policies, mammograms are encouraged by SUS, targeting the female population over 50 years of age and being performed every 2 years, or annually in the case of altered clinical exams. Women presenting with familial history are encouraged to undergo annual screening of the breasts.Citation23 It is estimated that 50% of Brazilian women older than 50 years have had at least one mammography in their life,Citation24 but there are no reliable data regarding posterior follow-up by a new mammogram. The International Agency for Research on CancerCitation25 recommends that at least 70% of the target female population should be screened with mammograms.Citation26 Following the recommendations from the International Agency for Research on Cancer could further substantially contribute to understanding the mortality rates observed in the last 20 years, which are represented in . Educational programs are strongly encouraged by the government, since, unfortunately, there is a lack of awareness among Brazilian women about the relevance of early detection via annual mammograms after the age of 50 years.
Table 2 Distribution according to the BI-RADS of mammograms performed in the period 2009–2013
Screening policies have to be urgently expanded, since it is estimated that only 60% of the target population had mammograms in 2008.Citation27 A survey conducted by the Brazilian Society of Mastology (Sociedade Brasileira de Mastologia [SBM]) indicated that there were 4,228 mammogram devices in Brazil in 2013, with more than one-half available under SUS, totaling 2,226 devices.Citation28 The Ministry of Health recommends one piece of equipment per 240,000 habitants; therefore, this number is more than sufficient.Citation29 Therefore, the problem is not due to a lack of equipment, but to the geographic concentration of these devices in the more developed areas.Citation1
Lifestyle
Globally, we have observed continuous increasing changes in lifestyle are observable among developing countries. In the past, Brazil was an essentially agricultural country, whose growing industrial and economic development began after the end of the military political regime (early 1990s), when the economic opening of the country toward purchase of imported products occurred. The increased purchasing power subsequently changed the eating habits of the population toward the attainment of manufactured products. Since then, a gradual increase in the weight of the population has been observed; currently, about 30% of individuals are pre-obese/obese.Citation25 This lifestyle modification, in association with increased physical inactivity, extensive working hours, and intensive exposure to carcinogens, helps to explain the cumulative growing incidence of cancer in the Brazilian population year after year.Citation30,Citation31 In addition, the increasing incidences of hormonal contraceptive use, postmenopausal hormone replacement therapy, nulliparity, late age at first birth, and enhanced alcohol consumption by women have increased the risk for breast cancer development in all countries.Citation3
Challenges in therapeutic approaches
At the end of the 1980s, Brazil experienced a political movement toward economic opening of its borders and the entry of new technologies, as well as access to imported drugs. At that time, there was little research regarding the development of new drugs in Brazil, and this fact strongly limited access to the chemotherapeutic drugs available in developed countries. Thus, the chemotherapeutic regimens in Brazil could not follow the international guidelines of the early 1990s, because the necessary drugs for breast cancer treatment were not available. Therefore, oncologists adapted such protocols according to the availability of such drugs in the country (the main drugs are shown in ). Furthermore, scientific publications regarding this theme at that time are scarce.
Figure 3 Timeline representing the main treatment options employed under Brazil’s public health system (SUS) for treating breast cancer patients.
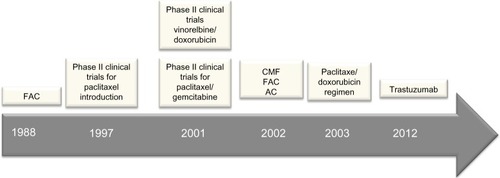
Historically, the first report after SUS implementation in Brazil was published by Baracat et al,Citation32 a reference group until nowadays in the field of breast cancer chemotherapy. The group reported the use of the CAF protocol (cyclophosphamide, doxorubicin, fluorouracil) for treating Brazilian women diagnosed with inflammatory breast cancer. A subsequent study was published in 1997, and described the Phase II clinical evaluation of doxorubicin/paclitaxel plus G-CSF for metastatic breast cancer in patients attending the Hospital das Clínicas de Porto Alegre.Citation33 In the same year, Murad et alCitation34 published the Phase II clinical trial for paclitaxel and ifosfamide testing in Brazil, intended for treating women with metastatic disease.
The 2000s were years of ongoing chemotherapy clinical trials in Brazil, and several international publications reported the advances. In 2001, Murad et al tested paclitaxel/gemcitabine in a Phase II clinical trial for metastatic breast cancer treatment.Citation35 Hegg et al,Citation36 in the same year, published the Phase II clinical trial for fractionated vinorelbine/doxorubicin as first-line therapy for advanced breast cancer. Another study, conducted by Costa et al in 2002,Citation37 described advances occurring in the field of chemotherapy, most of them based on anthracycline-based regimens. The authors reported the use of several protocols for breast cancer treatment, such as the CMF protocol (cyclophosphamide, methotrexate, 5-fluorouracil), the FAC protocol (5-fluorouracil, adriamycin, cyclophosphamide), and the FEC (5-fluorouracil, epirubicin, and cyclophosphamide) and AC protocols (adriamycin, cyclophosphamide).
The current SUS protocol, based on paclitaxel (175 mg/m2) and doxorubicin (60 mg/m2), began last decade in Brazil, in about the year 2003.Citation38 Also in 2003, publications reported the use of the sentinel lymph node biopsy in a pilot study in Brazil.Citation39 In 2012, trastuzumab-based chemotherapy was introduced in SUS. A study regarding the use of trastuzumab in the Brazilian population was published in the same year.Citation40
When establishing a comparative timeline, there is a clear delay between the introduction of chemotherapeutic drugs in developed countries and its usage in the Brazilian population. Nevertheless, considering that SUS is a public health system that offers prevention, diagnosis, and treatment for breast cancer at no cost, it is important to emphasize that, despite its limitations, the system has achieved important gains for the population. Breast cancer chemotherapy is a high-cost treatment, which most of the Brazilian population would not be able to afford. In this context, SUS policies have worked to ensure free and fast access to oncologic treatments, as well as to support all the phases of diagnosis and follow-up. To regulate these actions, the National Policy of Oncologic Attention (Política Nacional de Atenção Oncológica) was recently created, which aims to develop actions to ensure that all oncologic patients have full access to the public health system.Citation41,Citation42
Perspectives and conclusion
Brazil is a model example of a country that has developed a successful public health system. The SUS faces a wide range of challenges concerning full access, early diagnosis, and modern therapeutics, as well expansion of their coverage area across the country. Pivotal advances have been achieved, which resulted in the National Policy of Oncologic Attention. Investment in local research must be strongly expanded, and should serve as the basis for the development of targeted strategies directed to the particularities of the Brazilian population. This concentration of effort could also facilitate the implementation of more expensive treatments against breast cancer under the SUS and means that high-cost/better quality treatments would be more accessible to the Brazilian population.
Disclosure
The authors report no conflicts of interest in this work.
References
- Instituto Brasileiro de Geografia e Estatística (IBGE)Escassez e Fartura: Distribuição da Oferta de Equipamentos de Diagnóstico por Imagem no Brasil [Scarcity and abundance: distribution of supply diagnostic imaging equipment in Brazil]Rio de JaneiroIBGE2009 [cited February 14, 2013]. Available from: http://www.ibge.gov.br/home/estatistica/populacao/indic_sociosaude/2009/com_esca.pdfAccessed August 2, 2014 Portuguese
- Ministério da Saúde. Secretaria ExecutivaSUS: Princípios e Conquistas [SUS: Principles and Achievements]BrasíliaMinistério da Saúde2000 Available from: http://bvsms.saude.gov.br/bvs/publicacoes/sus_principios.pdfAccessed August 4, 2014 Portuguese
- JemalABrayFCenterMMFerlayJWardEFormanDGlobal cancer statisticsCA Cancer J Clin2011612699021296855
- LeeBLLiedkePEBarriosCHSimonSDFinkelsteinDMGossPEBreast cancer in Brazil: present status and future goalsLancet Oncol2012133e95e10222381937
- AzevedoGMendonçaSCancer in the female population in BrazilRev Saude Publica19932716875 Portuguese8310272
- MoraesMFA mortalidade por câncer de mama no Brasil [Mortality from breast cancer in Brazil]Revista Brasileira de Cancerologia1998442 Portuguese
- FerlayJShinHRBrayFFormanDMathersCParkinDMEstimates of worldwide burden of cancer in 2008: GLOBOCAN 2008Int J Cancer2010127122893291721351269
- DATASUS [database on the Internet]Ministério da Saúde2008 Available from: http://www2.datasus.gov.br/DATASUS/index.php?area=01Accessed July 28, 2014 Portuguese
- SISMAMASistema de Informação do Controle do Câncer de Mama – manual gerencial [Information Systems for Control of Breast Cancer – Manual Management]. Equipe de Elaboração: Maria Beatriz Kneipp DiasRio de JaneiroBrazillian Ministry of Health Available from: http://www2.inca.gov.br/wps/wcm/connect/cancermama/site/home/sismamaAccessed July 28, 2014 Portuguese
- PrataPRA transição epidemiológica no Brasil [The epidemiologic transition in Brazil]Cad Saude Publica19928168175 Portuguese
- DollRAre we winning the fight against cancer? An epidemiological assessment. EACR – Mühlbock memorial lectureEur J Cancer1990265005082141517
- HerreraACPanisCVictorinoVJMolecular subtype is determinant on inflammatory status and immunological profile from invasive breast cancer patientsCancer Immunol Immunother2012612193220122618884
- PanisCVictorinoVJHerreraACDifferential oxidative status and immune characterization of the early and advanced stages of human breast cancerBreast Cancer Res Treat201213388188822048816
- PanisCLemosLGVictorinoVJImmunological effects of taxol and adryamicin in breast cancer patientsCancer Immunol Immunother20126148148821959683
- PanisCHerreraACVictorinoVJOxidative stress and hematological profiles of advanced breast cancer patients subjected to paclitaxel or doxorubicin chemotherapyBreast Cancer Res Treat2012133899721811816
- PanisCHerreraACVictorinoVJAranomeACecchiniRScreening of circulating TGF-β levels and its clinicopathological significance in human breast cancerAnticancer Res20133373774223393376
- AdamiHOHunterDTrichopoulosDTextbook of Cancer Epidemiology2nd edOxfordOxford University Press2008
- DuflothRMCarvalhoSHeinrichJKAnalysis of BRCA1 and BRCA2 mutations in Brazilian breast cancer patients with positive family historySao Paulo Med J2005123419219716389418
- EwaldIPIzettiPVargasFRPrevalence of the BRCA1 founder mutation c.5266dupin Brazilian individuals at-risk for the hereditary breast and ovarian cancer syndromeHered Cancer Clin Pract201191222185575
- KoifmanSKoifmanRJEnvironment and cancer in Brazil: an overview from a public health perspectiveMutat Res20035442–330531114644332
- RichardsMASmithPRamirezAJFentimanISRubensRDThe influence on survival of delay in the presentation and treatment of symptomatic breast cancerBr J Cancer19997985886410070881
- SimonSDBinesJBarriosCHClinical characteristics and outcome of treatment of Brazilian women with breast cancer treated at public and private institutions – the AMAZONE project of the Brazilian breast cancer study group (GBECAM)Abstracts of the 2009 CTRC-AACR San Antonio Breast Cancer SymposiumDecember 9–13, 2009San Antonio, TX Suppl to volume 69, Issue 24 of Cancer Research
- Instituto Nacional de CâncerControle do Câncer de Mama: fatores de risco [Breast cancer control: risk factors] [webpage on the Internet]Rio de JaneiroMinistério da Saúde Available from: http://www2.inca.gov.br/wps/wcm/connect/acoes_programas/site/home/nobrasil/programa_controle_cancer_mama/fatores_riscoAccessed July 28, 2014 Portuguese
- Lima-CostaMFMatosDLPrevalence and factors associated with mammograms in the 50–69-year age group: a study based on the Brazilian National Household Sample Survey (PNAD-2003)Cad Saude Publica20072316651673 Portuguese17572816
- BoylePLevinBWorld Cancer Report 2008LyonInternational Agency for Research on Cancer2008 Available from: http://www.iarc.fr/en/publications/pdfs-online/wcr/2008/Accessed August 15th, 2014
- AndersonBOCazapEEl SaghirNSOptimisation of breast cancer management in low-resource and middle-resource countries: executive summary of the Breast Health Global Initiative consensus, 2010Lancet Oncol20111238739821463833
- FIOCRUZ – Cobertura de mamografia – PROADESSII – Fiocruz2011 Available from: http://www.proadess.icict.fiocruz.br/index.php?pag=fic&cod=A07&tab=1Accessed August 2, 2014 Portuguese
- FreitasRFRahalRMSRodriguesDCNDados sobre produção de mamografias no Brasil, em 2012 e 2013 e número de mamógrafos em uso em 2013 [Data regarding mammograms in Brazil, between 2012 and 2013, and the number of mammographs]. Fevereiro de 2014 Available from: http://www.sbmastologia.com.br/index/index.php/component/content/article/50-destaque-medico/321-dados-sobre-producaoAccessed July 28, 2014 Portuguese
- Portaria n.° 1101/GM [Ordinance No 1101 / GM]BrasíliaMinistério da Saúde2002 Available from: http://dtr2001.saude.gov.br/sas/PORTARIAS/Port2002/Gm/GM-1101.htmAccessed November 19, 2014 Portuguese
- LaurentiRTransição demográfica e transição epidemiológica [Demographic and epidemiologic transition]Anais do 1° Congresso Brasileiro de Epidemiologia1990 set 2–6Campinas, BrasilRio de JaneiroAbrasco1990143165 Portuguese
- AlbalaCVioFYanezMTransición epidemiológica en América Latina: comparación de cuatro países [Epidemiological transition in Latin America: comparison of 4 countries]Rev Med Chil19971256719727 Portuguese9580335
- BaracatFFde LimaGRde OliveiraABBaracatFBaracatFInflammatory carcinoma of the breast. Experience of 43 cases at the Instituto do Câncer Arnaldo Vieira de CarvalhoRev Paul Med198810611420 Portuguese3238260
- SchwartsmannGMansDRMenkeCHA phase II study of doxorubicin/paclitaxel plus G-CSF for metastatic breast cancerOncology (Williston Park)1997114 Suppl 324299144687
- MuradAMGuimaraesRCAmorimWCMoriciACFerreira-FilhoAFSchwartsmannGPhase II trial of the use of paclitaxel and gemcitabine as a salvage treatment in metastatic breast cancerBreast Cancer Res Treat199745147539285116
- MuradAMGuimarãesRCAragãoBCScalabrini’NetoAORodriguesVHGarciaRGemcitabine and paclitaxel as salvage therapy in metastatic breast cancerOncology (Williston Park)2001152 Suppl 3252711252885
- HeggRCostaMAPerdicarisMA phase II trial of fractionated vinorelbine/doxorubicin as first line therapy for advanced breast cancerCurr Med Res Opin200116422523411268706
- CostaLJVarellaPCdel GiglioAWeight changes during chemotherapy for breast cancerSao Paulo Med J2002120411311712436158
- AnelliABrentaniRRGadelhaAPAmorim De AlbuquerqueASoaresFCorrelation of p53 status with outcome of neoadjuvant chemotherapy using paclitaxel and doxorubicin in stage IIIB breast cancerAnn Oncol200314342843212598349
- PiatoJRBarrosACPinceratoKMSampaioAPPinottiJASentinel lymph node biopsy in breast cancer after neoadjuvant chemotherapy. A pilot studyEur J Surg Oncol200329211812012633552
- GianniLPienkowskiTImYHEfficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trialLancet Oncol2012131253222153890
- Ministério da Saúde (Br). Secretaria de Atenção à SaúdeControle dos Cânceres do Colo do Útero e da Mama [Control of breast and uterine cancers]BrasíliaMinistério da Saúde2014 Portuguese
- Ministério da Saúde (Br). Secretaria de Atenção à SaúdeControle dos Cânceres do Colo do Útero e da Mama [Control of breast and uterine cancers]BrasíliaMinistério da Saúde2006 Portuguese