
Abstract
Acute lymphoblastic leukemia (ALL) is a rare hematologic malignancy resulting in the production of abnormal lymphoid precursor cells. Occurring in B-cell and T-cell subtypes, ALL is more common in children, comprising nearly 30% of pediatric malignancies, but also constitutes 1% of adult cancer diagnoses. Outcomes are age-dependent, with five-year overall survival of greater than 90% in children and less than 20% in older adults. L-asparaginase, an enzyme not found in humans, depletes serum levels of L-asparagine. As leukemic cells are unable to synthesize this amino acid, its deprivation results in cell death. The success of asparaginase-containing regimens in the treatment of pediatric ALL, and poor outcomes with conventional cytotoxic regimens in adults, have led to trials of pediatric or pediatric-inspired regimens incorporating asparaginase in the adolescent and young adult (AYA) and adult populations. Initially purified from Escherichia coli, newer formulations of asparaginase have been developed to address short half-life, high immunogenic potential, and manufacturing difficulties. Unfamiliarity with asparaginase use and management of its unique toxicities may result in treatment-decisions that negatively impact outcomes. In this review, we address the current use of asparaginase in the treatment of ALL, with an emphasis on its role in the treatment of adults, key clinical trials, recognition and management of toxicities, and ongoing directions of study.
Introduction
Acute lymphoblastic leukemia (ALL) is a hematologic malignancy of lymphoid precursor cells occurring in B- and T-cell subtypes. While it is the most common childhood malignancy, comprising up to 30% of pediatric cancer and 80% of pediatric leukemia diagnoses, it is relatively rare among adults, comprising 15–20% of adult leukemia cases and less than 1% of adult cancer diagnoses in the United States (US).Citation1 Historically, significantly better outcomes have been seen in pediatric patients, with a five-year overall survival (OS) of nearly 90% in children, and less than 20% for older patients. This is thought to be due in part to the regimens used in the pediatric population, which generally include agents with more frequent and longer durations of administration, though differences in host and disease factors between the two groups are also likely contributory. Non-randomized studies also noted that adolescent and young adults (AYA) treated by pediatricians with expertise in these regimens had better outcomes than those treated by adult oncologists.Citation2–Citation7 These findings have led to further trials of pediatric or pediatric-inspired regimens in AYA and adult patients. L-asparaginase is a central component of most modern pediatric ALL regimens. Therefore, the migration of pediatric strategies into the management of adults with ALL will lead to the wider utilization of this class of agents in this population. Here, we review the role of asparaginase in the treatment of ALL, with an emphasis on its use in the AYA and adult population, the various formulations currently available, its unique side-effect profile, management of treatment-related toxicity, and ongoing clinical trials.
Historical Perspective
The first studies implicating L-asparaginase as an anti-leukemic agent were conducted in the 1950s and 1960s. KiddCitation8 demonstrated that guinea pig serum could induce regression of explanted lymphomas in mice and rats, with a subsequent series of studies identifying L-asparaginase as the serum component responsible for this effect.Citation9–Citation13 The first documented use of L-asparaginase in humans came in 1966. DolowyCitation14 reported a case of a pediatric patient with multiply relapsed ALL who was administered L-asparaginase partially purified from guinea pig serum. While improvement of clinical and laboratory parameters was noted, the patient developed significant toxicity immediately following infusion, including a likely hypersensitivity reaction, and succumbed to pulmonary hemorrhage ten days after administration. In a 1967 case series, Hill reportedCitation15 on three pediatric patients with ALL treated with purified L-asparaginase, all of whom exhibited clinical and laboratory improvement, with one achieving complete remission (CR). These preliminary reports led to larger-scale studies in children, which were able to be conducted following the availability in 1978 of commercially produced L-asparaginase from Escherichia coli (E. coli). Early studiesCitation16 in adults were also performed; however, significant toxicities led to the avoidance of its use in subsequent trials. Consequently, the role of L-asparaginase in the treatment of this population was not readdressed until several years later.
Pharmacology
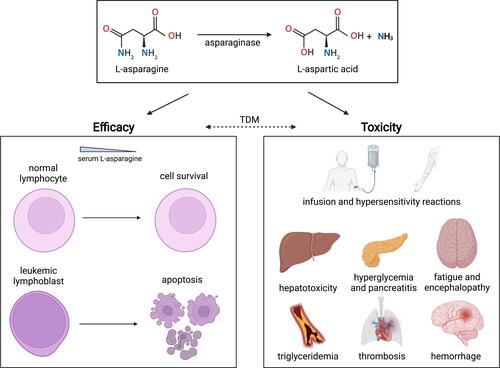
Asparagine is one of twenty amino acids necessary for cell function and survival. It is generated in normal cells by L-asparagine synthetase, which catalyzes the conversion of aspartic acid and glutamine to asparagine and glutamate.Citation17 This enzyme is poorly expressed in leukemic cells, which rely on serum asparagine to fulfill the increased demand of sustained malignant cell growth and proliferation.Citation18 L-asparaginase is an amidase that removes serum asparagine from circulation by hydrolyzing L-asparagine into aspartic acid and ammonia.Citation19 Without an exogenous source of asparagine, protein synthesis is quickly inhibited in the tumor cell, subsequently leading to apoptosis ().
Figure 1 Depiction of the pharmacologic effects of asparaginase. Asparaginase catalyzes (top panel) the degradation of L-asparagine to L-aspartic acid and ammonia (NH3). Unlike normal cells, which express asparagine synthetase, leukemic cells are unable to generate L-asparagine, so its serum depletion results in apoptosis (left panel). Toxicities due to asparaginase (right panel) occur through a variety of mechanisms including decreased protein synthesis, direct effects on metabolites, or more complex mechanisms. Therapeutic drug monitoring (TDM) may allow for individualized asparaginase dosing and maximization of treatment efficacy with reduction of toxicity, but this is not yet widely practiced. Created with BioRender.com.
Asparaginase Formulations
Native Escherichia coli Asparaginase
While absent in humans, L-asparaginase exists in various animals, plants, and microorganisms.Citation19 As noted above, the first commercial L-asparaginase product, FDA-approved in 1978, was isolated from several E. coli strains.Citation19,Citation20 Despite its efficacy in killing leukemic cells, the use of this formulation was hampered by its short half-life, necessitating frequent dosing, as well as high rate of immunogenicity.Citation18,Citation21,Citation22
Pegylated Asparaginase (Pegaspargase, Calaspargase Pegol)
Pegaspargase, comprised of polyethylene glycol (PEG) conjugated to L-asparaginase through a succinimidyl succinate linker, emerged in the 1990s to address the above limitations.Citation21–Citation23 This formulation has an extended plasma half-life, allowing it to be dosed every two weeks rather than thrice weekly. Moreover, the incorporation of the PEG moiety decreases its immunogenicity; however, patients can develop antibodies against the linker.Citation24 Compared to the >30% incidence rate seen with native enzyme, clinical allergic reactions with pegaspargase occurred in 3% of first-line and 10% of relapsed ALL patients without prior reactions.Citation18,Citation25,Citation26
Calaspargase pegol, a novel pegylated preparation, was approved for the treatment of children and young adults with ALL in 2018.Citation27 The use of a succinimidyl carbonate linker to covalently bind E. coli L-asparaginase and PEG, results in increased stability and longer half-life allowing for every-third-week dosing.Citation23
Erwinia chrysanthemi (Native and Recombinant) Asparaginase
Despite the improved convenience and toxicity profile of pegaspargase, the need for an alternative L-asparaginase remained for those who developed hypersensitivity to E. coli-derived L-asparaginases. Erwinia L-asparaginase, which does not share cross-reactivity with Escherichia enzyme, was approved in 2011 for this patient population.Citation19 In the AALL07P2 trial, 93% of patients with clinical allergy to pegaspargase achieved therapeutic activity with Erwinia L-asparaginase.Citation28 However, as the product was manufactured on a batch-by-batch basis, its clinical impact was constrained by drug shortages.Citation29 To combat this, efforts were undertaken to develop a bioengineered version,Citation29 and in 2021, recombinant Erwinia L-asparaginase, manufactured using a Pseudomonas fluorescens expression platform, received FDA approval.Citation29,Citation30
Pharmacokinetics
L-asparaginase mostly resides in the vascular space upon administration, as demonstrated by its small volume of distribution (), with minimal enzyme detected in pleural and peritoneal fluids.Citation18,Citation31 Enzymatic activity can also be measured in cerebrospinal fluid (CSF), where extent and duration of asparagine depletion have been associated with treatment outcomes.Citation31,Citation32
Table 1 Pharmacokinetic Properties of L-Asparaginase Products
L-asparaginase is thought to be metabolized via proteolytic enzymes in tissues.Citation22,Citation30 It is not excreted renally.Citation31 The PEG moiety increases steric hindrance, limiting access of circulating peptidases and proteases,Citation33 and thereby significantly extending half-life. Erwinia formulations have shorter half-lives than their E. coli counterparts and therefore require more frequent administration to achieve similar therapeutic effects.Citation26,Citation34,Citation35
Pharmacodynamics and Therapeutic Drug Monitoring
The primary goal of L-asparaginase therapy is total asparagine depletion in the blood and CSF.Citation22,Citation26 However, it is difficult to measure serum asparagine concentration consistently and accurately due to technical and logistical constraints.Citation26 Since there is a direct correlation between the level of L-asparaginase activity and reduction in asparagine concentration, serum asparaginase activity (SAA) has become a clinical surrogate to predict pharmacodynamic success.Citation26,Citation34,Citation36 SAA ≥0.1IU/mL was proposed as the minimum threshold for meaningful efficacy, following a 1981 study demonstrating that plasma and CSF asparagine were undetectable at this level. This has been subsequently validated in multiple studies.Citation26,Citation37
Asparaginase in Pediatric ALL
In the years following initial reports suggesting a role for L-asparaginase in ALL therapy, as detailed below and in , several clinical trials were performed to assess safety, efficacy, and optimal dosing of different forms of asparaginase when combined with chemotherapy in pediatric cohorts. These studies ultimately demonstrated improved outcomes, and the inclusion of asparaginase has now become standard of care in pediatric patients. The current paradigm of pediatric ALL management is divided into discrete phases of multiagent chemotherapy: remission induction, intensive consolidation including CNS-directed therapy, delayed-intensification, and low-intensity maintenance chemotherapy.Citation38 Asparaginase is typically incorporated into induction, consolidation, and intensification stages. While this review focuses on asparaginase in adult ALL, we discuss several key pediatric studies here (summarized in ) to provide important context. For more details, we refer the interested reader to other reviews on this topic.Citation39,Citation40
Table 2 Selected Pediatric Studies Incorporating Asparaginase in ALL Treatment Regimens
Several studies assessed the addition of asparaginase to standard chemotherapy in either induction or intensification phases. In the US Children’s Cancer Study Group (CCG) 101/143 trial,Citation41 patients received native E. coli L-asparaginase in addition to vincristine and prednisone during induction, with a statistically significant improvement in CR rate and decrease in treatment failure rate, compared to patients receiving only vincristine and prednisone in the prior CCG 903 trial. The prospective Dana Farber Cancer Institute (DCFI) 77–01 studyCitation42 half of the patients were randomized to receive weekly high-dose L-asparaginase during intensification with improvement in disease-free survival (DFS) in patients receiving L-asparaginase. The subsequent DCFI 88–01 studyCitation43 also noted improved event-free survival (EFS) in patients receiving high-dose L-asparaginase during intensification/continuation cycles.
The Pediatric Oncology Group (POG) 8704 study addressed patients with T-cell ALL.Citation44 Patients were treated with rotating combinations of chemotherapy including L-asparaginase followed by randomization to receive or not receive weekly. Those who were randomized to receive asparaginase noted significant improvement in four-year continuous CR rate, though at the expense of increased toxicities.
The Italian, Dutch, Hungarian (IDH) ALL-91 studyCitation45 assessed whether the addition of weekly high-dose L-asparaginase (25,000 IU/m2) to a modified Berlin-Frankfurt-Muenster (BFM) backbone and demonstrated improved ten-year DFS in those receiving L-asparaginase. Uniquely, >90% of patients received Erwinia asparaginase due to unavailability of E. coli asparaginase.
Several studies assessed whether increased L-asparaginase intensity would improve outcomes as well as the efficacy of pegaspargase versus native E. coli enzyme. In the POG 9310 study,Citation46 patients with relapsed B-ALL were randomized to receive pegaspargase (2500 IU/m2) either weekly (four doses) or biweekly (two doses), during reinduction. The overall CR rate was 90% with increased CR in the cohort receiving weekly (97%) versus biweekly (82%) dosing, p=0.003. Higher CR rate was associated with increased asparaginase activity (p=0.012).
The DFCI 91–01 studyCitation47 assessed intensification of post-remission therapy in patients with newly diagnosed ALL, with the addition of prolonged (30 week) asparaginase administration and dexamethasone in place of prednisone. Furthermore, in addition to randomizations of doxorubicin infusion and cranial radiation dosing, patients were randomized to receive either pegaspargase 2500 IU/m2 IM every other week (15 doses) or native E. coli asparaginase 25,000 IU/m2 IM weekly (30 doses). Patients who received ≥26 weeks of L-asparaginase had a 5-year EFS (90%) compared to those who tolerated 25 weeks or less (73%), p<0.01. Patients ≥9 years were more likely to tolerate <25 weeks (p<0.01). Toxicities were more common in older patients (48% for age 9–18 versus 24% for age <9, p<0.01). No statistically significant difference was noted between asparaginase formulations. This protocol was shown to be superior to prior DFCI protocols with improved EFS (p=0.03).
Two recent Children’s Oncology Group (COG) studies, AALL0232Citation48 and AALL0434Citation49 yielded differing results when it came to the role of pegaspargase in the interim maintenance phase of their backbone for patients with either B-ALL or T-ALL, respectively. Both compared high-dose methotrexate (HD-MTX; 2–5 g/m2 administered over 24 hours with leucovorin rescue) versus the Capizzi regimen (C-MTX) of dose-escalated MTX (100–300 mg/m2) plus pegaspargase during interim maintenance. Five-year EFS was higher for patients receiving HD-MTX versus C-MTX in AALL0232, with the opposite findings in AALL0434. In contrast to the AALL0232 study, fewer relapses were noted in the AALL0434 C-MTX group (32) versus the HD-MTX group (59), including fewer CNS relapses (6 versus 23, respectively). As described above, since pegaspargase itself does not exhibit CNS penetration, this finding was attributed to increased asparagine depletion in patients receiving C-MTX given the two additional cycles of pegaspargase received by this cohort during interim maintenance, though these results may be confounded by differences in timing of cranial radiation in the two studies.
Evidence for Treatment of Adult ALL with Pediatric or Pediatric-Inspired Regimens
Despite this evolution in pediatric ALL care over the course of several decades, progress for adults with ALL has lagged. Several retrospective analyses were performed to assess why despite achieving similar CR rates, outcomes for AYA and adult ALL were inferior to those of pediatric patients. One relatively consistent conclusion was that AYA treated on pediatric studies (many of which utilize more intense administration of asparaginase) fared better, suggesting that this subset of patients is generally better served with these treatment approaches.
A retrospective analysisCitation2 of adolescents undergoing treatment in the pediatric FRALLE-93 and adult LALA-94 trials demonstrated improved outcomes with patients treated on the pediatric protocol with CR of 94% versus 83% (p=0.04) and estimated 5-year EFS 57% versus 41% (p<0.0001). de Bont and others retrospectively assessed adolescent patients treated in the Netherlands on either the pediatric Dutch Childhood Oncology Group (DCOG) or adult Dutch-Belgian Hemato-Oncology Cooperative Study Group (HOVON) treatment protocols.Citation3 They noted a 35% higher 5-year probability of survival for those treated on the pediatric protocol and improved 5-year EFS (69% versus 34%, p=0.0001). These findings were attributed to both lower relapse rates and treatment-related mortality rates in the pediatric protocol cohorts. They speculate that key differences between the protocols may have contributed, including the inclusion of reinduction/intensification and maintenance phases in the pediatric protocols, shortened interval between pediatric courses, and absence of methotrexate and increased frequency of allogeneic transplant in the adult protocols.
A retrospective analysis of AYA with newly diagnosed ALL treated with pediatric protocols on consecutive trials in the CCG or the Cancer and Leukemia Group B (CALGB)Citation7 also noted similar findings. Despite similar CR rates of 90% between the two groups, 7-year EFS was 63% in the CCG group versus 34% in the CALGB group (p<0.001 with relative HR 2.2). OS at 7 years was 67% versus 46% (p<0.001 with relative HR 1.9). A meta-analysisCitation50 conducted in 2012 included the above trials as well as eight additional comparative studies with a total of 2489 AYA patients treated with either pediatric-inspired or conventional adult regimens. This study demonstrated a lower 3-year all-cause mortality rate in the pediatric-inspired regimen cohort (relative risk (RR) 0.58) as well as a higher CR rate (RR 1.05), longer EFS (RR 1.66), and lower relapse rate (RR 0.51).
Prospective Studies with Asparaginase in AYA and Adult ALL
Again, early setbacks due to asparaginase-related toxicity in adults limited its use to the pediatric and adolescent population. However, beginning in the 1990s, several studies reassessed its use in the AYA and adult population. Key characteristics and findings from selected trials are summarized in .
Table 3 Selected AYA and Adult Studies Utilizing Asparaginase-Containing Pediatric or Pediatric-Inspired Regimens
The PETHEMA ALL-96Citation6 study was one of the first prospective studies to demonstrate similar response and tolerability to a pediatric regimen in AYA patients. Adolescents (ages 15–18) and young adults (ages 19–30) with standard-risk ALL were enrolled. E. coli asparaginase was administered in induction, consolidation, and maintenance cycles with a cumulative dose of 320,000 U/m2. Overall CR rate was 98% and OS was 61%, without significant difference in the latter between adolescents (77%) and young adults (63%, p=0.44). Of note, 8% developed hypersensitivity reactions to asparaginase requiring treatment interruption, with dose modifications more commonly required in young adults (33% of cycles) versus adolescents (19%, p=0.03). The trial also assessed a cohort of older patients (ages 56–77) on the same regimen. CR was achieved in 57.6%, with a high rate of early death (36.4%). This prompted removal of asparaginase and cyclophosphamide from induction, which subsequently improved survival from 20% to 52%.
The HOVON 70 studyCitation51 utilized the FRALLE pediatric approach in previously untreated high-risk adult ALL (ages 17–40). E. coli asparaginase (6000 IU/m2) was included in remission induction and intensification cycles. Allogeneic hematopoietic cell transplantation (HCT) was offered to standard- and high-risk patients. Overall CR rate was 91%, 24-month EFS 66%, and OS 72%. These results were improved compared to outcomes from prior HOVON studies, suggesting the feasibility and efficacy of such a regimen in the AYA population.
Several studies included adult patients in addition to AYA. The Group of Research on ALL (GRAALL) 2003 studyCitation52 assessed a pediatric-inspired ALL regimen in AYA and adult patients (15–60 years) with Philadelphia chromosome (Ph) negative ALL. Patients received multiphase, multiagent chemotherapy with E. coli L-asparaginase administered during remission induction, late-intensification, and consolidation. Allogeneic HCT was offered to high-risk patients in first CR. CR rate was 93.5% with EFS 55% and OS 60%. Results from this trial were retrospectively compared to historical data from the LALA-94 trial,Citation53 demonstrating significant improvement in CR, EFS, and OS. Notably, when comparing older (>45 years) versus younger patients, there was a higher cumulative incidence of treatment-related death (23% versus 5%, p<0.001) and higher rate of death in CR (22% versus 5%, p<0.001), suggesting the need for dose adjustment or alternative approaches in older patients.
The GRAALL-2005 studyCitation54 was a larger-scale study built on GRAALL-2003, enrolling patients up to 59 years old. Patients received E. coli asparaginase for a cumulative planned dose of 48,000 IU/m2 during first induction and late intensification phases. Overall CR was 91.9%, with 5-year OS of 52.5% and EFS of 52.2%. Notably, patients ≥55 years old fared poorly, with lower 5-year EFS (25.8% versus 55.7%) owing to decreased tolerance of and poorer compliance to planned chemotherapy. Median cumulative dose of L-asparaginase received was greater in patients aged 18–54 compared to those 55 or older (48,000 versus 36,000 IU/m2, p<0.001). This study did identify a higher best prognostic age cutoff (55) compared to GRAALL-2003 (45), owing in part to differences in sample sizes and presumably increased physician experience with the administration of such regimens in older patients. A single institution studyCitation55 in adults (18–60) assessed a modified version of the DFCI 91–01 protocol including L-asparaginase during induction and 30 weeks of high-dose L-asparaginase (12,500 IU/m2) during intensification with induction CR of 89%, 5Y OS 63%, and RFS 71%.
Next, several studies assessed pegaspargase in AYA or adult patients in lieu of or in comparison to native L-asparaginase. The German Multicenter Study Group for Adult ALL (GMALL) protocols are pediatric-inspired regimens based on prior BFM protocols optimized for adults. Gökbuget reportedCitation56 on the results of AYA patients (ages 15–35) in two consecutive studies, GMALL 05/93 and 07/03, with the latter implementing refinements to the protocol, including pegaspargase instead of native L-asparaginase. Improved outcomes were noted in the latter trial, attributed to intensification of treatment, with CR rate increased from 88% to 91% (p=0.001) and OS from 46% to 65% (p<0.0001).
In the CALGB 9511 study,Citation57 Wetzler et al assessed outcomes in patients receiving pegaspargase in lieu of native L-asparaginase in adults. Patients received pegaspargase at 2000 U/m2 subcutaneously (3750 U maximum) during induction and early intensification courses. Asparagine depletion was defined by SAA >0.03 U/mL for 14 consecutive days following administration. Inferior OS and DFS were noted for patients not achieving depletion, with adjusted HR 1.8 and 1.8, respectively.
DeAngelo reportedCitation58 on the treatment adult patients (ages 18–50) with newly diagnosed ALL (including Ph-positive disease) in a multicenter study treated with the DFCI 01–175 protocol. Patients received E. coli L-asparaginase initially at a single 25,000 IU/m2 dose during induction, with additional doses during consolidation pharmacokinetically dose-adjusted based on SAA. Patients with persistently low SAA were switched to pegaspargase or Erwinia asparaginase. CR following 1 month of induction therapy was 85%, with 4-year DFS 69% and OS 67%. A 72% of patients were able to receive at least 26 doses, and asparaginase-related toxicities were similar in incidence to those reported in older children.
The Nordic Society of Pediatric Hematology and Oncology (NOPHO) ALL2008 studyCitation59 assessed a pediatric regimen in patients (ages 1–45) with Ph-negative ALL, with treatment protocol unmodified based on age. Patients first received induction chemotherapy including steroids and multiagent chemotherapy. They were then risk-stratified to receive further treatment with either standard ALL post-induction therapy with delayed intensifications and maintenance or multiple intensive ALL blocks in addition to delayed intensification and maintenance. Regardless of risk, all patients received pegaspargase, high-dose methotrexate, and mercaptopurine, though pediatric patients received pegaspargase at 1000 IU/m2 randomized at 2 or 6-week intervals. EFS rates were 89%, 80%, and 74% for ages 1–9, 10–17, and 18–45, respectively. While most treatment-related toxicities in this study were not affected by age, increased frequency of thrombosis, pancreatitis, and osteonecrosis was associated with age >10, with similar incidence between adolescents and adults.
The Cancer and Leukemia Group B (CALGB) 10403 studyCitation60 was a prospective trial studying the efficacy of a pediatric regimen in AYA (ages 17–39) with newly diagnosed Ph-negative ALL. The treatment regimen replicated one arm of the COG AALL0232 study with pegaspargase (2500 IU/m2 intramuscular [IM] or intravenous [IV]) administered during all courses of treatment except for the final maintenance course. HCT was at the discretion of the treating physician (except those with t(4;11), who received HCT in first CR). Median OS was not reached after a median follow-up of 64 months, with estimated 3-year OS 73%, 3-year EFS 59%, and median EFS 78.1 months. The regimen was well tolerated, with treatment-related deaths in 3%. Asparaginase-associated toxicities were similar to prior studies. Overall, this study demonstrated the efficacy of an intensive pediatric regimen in patients up to 40 years, with improved outcomes (compared to 3-year OS 55% in earlier CALGB studies of this age group) and a relatively low treatment-related mortality. Of note, there were increased rates of hepatic and thrombotic events compared to patients enrolled in the AALL0232 study, with obesity as a risk factor for worse outcomes.Citation61
The United Kingdom ALL UKALL14 studyCitation62 utilized a pediatric-inspired regimen in adults (ages 20–60) with untreated ALL or LBL. CR/CRi rate of 97% was achieved with 3-year EFS and OS of 67.8% and 76.4%. Notably, the study included 6 doses of pegaspargase 2000 IU/m2 administered in a synchronized manner to avoid concurrent toxicity with other regimen constituents. High-grade asparaginase-related toxicities occurred with increased frequency those age 40–60.
One notable exception among these different treatment regimens is hyperCVAD (hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone alternating with methotrexate and cytarabine), which is unique in that it does not include asparaginase. While there has not yet been a head-to-head comparison with hyperCVAD, Rytting reported results from a prospective study of an augmented BFM regimen in AYA with Ph-ALL and compared them to a historical cohort of similar patients given hyperCVAD.Citation63 Overall, they found very similar outcomes in terms of 3-year OS (74% vs 71%) and complete remission duration (70% vs 66%) between the augmented BFM and hyperCVAD groups, respectively. Many skeptics of pediatric-inspired therapy for young adults will cite these data, and though not a prospective randomized trial, they are compelling. That said, one interesting caveat to this analysis pertains to the use of rituximab: Over half of the patients treated with hyperCVAD had CD20+ disease and thus were given rituximab, based on this group’s prior experience,Citation64 whereas none of the patients treated with augmented BFM received the monoclonal antibody due to paucity of evidence for rituximab use in that patient population at the time. Given that rituximab use has since been validated by a randomized study to yield superior outcomes when added to a pediatric-inspired regimen for adults with CD20+ B-ALL,Citation65 one must consider how the outcomes may have differed had the use of rituximab been consistent between both arms.
Asparaginase Toxicities and Management
Asparaginase has a unique side-effect profile (). Given its rare use outside of the treatment of ALL and (until relatively recently) the pediatric population, many adult oncologists encounter difficulties in the management of treatment-related toxicities. This can lead to poor outcomes due to treatment- or disease-related morbidity and mortality, the latter stemming from inappropriate dosing changes or early discontinuation. An expert panel developed recommendationsCitation66 in 2011 for the management of asparaginase-related toxicities, which have since been incorporated into the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines,Citation67 and have been revisited in more recent years given its increasing use in the AYA and adult population.Citation68–Citation70 We review these here (with management recommendations summarized in ).
Table 4 Selected Asparaginase Associated Toxicities and Their Management
Hepatic Toxicity
Hepatic toxicity includes the most common significant asparaginase-associated adverse events, with high-grade events occurring in up to 50% of adult cases.Citation60,Citation71 These can manifest in a broad range of signs and symptoms, from laboratory elevations of transaminases, alkaline phosphatase, and/or bilirubin to synthetic dysfunction leading to hypoalbuminemia, hypofibrinogenemia, or coagulation factor deficiencies. Hepatic toxicity is almost always reversible, and more severe complications are relatively rare. Overt liver failure occurred in 1% of patients in the CALGB 10403 studyCitation60 and veno-occlusive disease was noted in <1% in ALL2008Citation59 trial. Though rare, the incidence of acute liver failure has been linked to other factors or comorbidities, including age and obesity.Citation71 Hepatic toxicity appears to be dose-dependent and has a typical onset of 2–3 weeks following administration. Although it is almost always reversible, prolonged resolution (>30 days) has been observed.Citation72 The underlying mechanism is unclear, though someCitation73 have implicated increased mitochondrial stress and alterations in lipoprotein metabolism due to asparagine/glutamine depletion.
Given the reversibility, management typically involves pausing asparaginase pending resolution, depending on the toxicity grade. Discontinuation is not usually recommended, nor is there evidence to change formulation.Citation68–Citation70 Dose reduction can be considered given the propensity of prolonged bilirubinemia, to minimize treatment delays. Prevention strategies are aimed at mitigating risk factors. Dose reduction in patients with risk factors such as obesity can be considered. There is evidenceCitation74–Citation80 from case reports and series for the use of L-carnitine (with or without B-complex vitamins) and ursodiol for prophylaxis or treatment. A prospective trial (NCT03564678) is currently ongoing to assess the benefits of L-carnitine and vitamin B complex in the treatment of pegaspargase hepatotoxicity.
Hyperammonemia
Ammonia is generated as a byproduct of asparaginase activity and hyperammonemia should be considered in patients who develop extreme fatigue (“asparaginase blues”) or encephalopathy during treatment; and this has been reported in both pediatricCitation81,Citation82 and adultCitation81,Citation83 populations, though the correlation between hyperammonemia and central neurotoxicity is not entirely clear.Citation82 Additional symptoms include headache, nausea, and rash and can be difficult to differentiate from infusion reactions.Citation84 Measurement of serum ammonia levels following a suspected infusion reaction may be beneficial to clarify the underlying etiology. Management includes administration of lactulose and supportive care.
Hyperglycemia
Hyperglycemia is commonly seen in both pediatric and adult patients treated with asparaginase, with an all-grade incidence of >90% and up to one-third of patients experiencing grade ≥3. Risk factors include obesity and prior history of diabetes mellitus, both of which are common in the adult population, as well as concomitant use of steroids, which is typical of most asparaginase-containing regimens. Insulin production may also be diminished in the setting of asparagine depletion or pancreatitis, resulting in elevated glucose. Uncontrolled hyperglycemia can lead to complications including diabetic ketoacidosis. Management includes insulin therapy to achieve glycemic control and holding glucocorticoids and asparaginase temporarily for high-grade toxicity.
Hypersensitivity Reactions
Asparaginase is foreign to humans, and hypersensitivity reactions have been noted since its initial use.Citation15 Current formulations differ in their immunogenicity. Prior to the development of pegylated asparaginase, up to one-third of patients developed hypersensitivity reactions to native E. coli asparaginase. Allergic reactions to pegaspargase occur in up to 22% of adults,Citation68 with up to 10% of patients experiencing grade ≥3 reactions. Route of administration (IM versus IV) appeared to affect rates of high-grade hypersensitivity reactions,Citation85 though other studies have not demonstrated such a significant difference.Citation86 In studies of calaspargase pegol, hypersensitivity reactions were noted in up to 27%.Citation36,Citation87 The safety of Erwinia-derived asparaginase following hypersensitivity to other forms of L-asparaginase has been demonstrated,Citation88,Citation89 with little cross reactivity between products of different bacterial species.
In adults, premedication is now routinely administered based on data from CALGB 10403, which noted a decrease in the incidence of hypersensitivity reactions from 10% to 4% following a protocol amendment to premedicate asparaginase administration with acetaminophen, diphenhydramine, and hydrocortisone. Similar results have been noted in the pediatric populationCitation90 and were deemed to be cost-effective.Citation91
Because asparaginase hypersensitivity is often associated with activity-neutralizing antibodies, recognition and mitigation is critical to ensure that therapeutic efficacy is not impacted. Multiple studies have clearly established inferior outcomes with early discontinuation or dose reduction. This can be challenging, as transient infusion reactions may mimic low-grade hypersensitivity reactions, and the use of premedication may mask a reaction that would signify the development of neutralizing antibodies. “Silent inactivation” of asparaginase can occur in the absence of detectable antibodies or clinical hypersensitivity. While there is evidence that therapeutic drug monitoring (TDM) can be beneficial in these settings, no standard algorithm for TDM exists at this time, and its use has generally been limited to the context of clinical trials.
Management involves the use of premedication for low-grade reactions (with consideration of TDMCitation92) and discontinuation of the offending asparaginase product for high-grade allergic or anaphylactic events with transition to Erwinia asparaginase.
Hypertriglyceridemia
There is significant variability in the incidence of hypertriglyceridemia in patients treated with asparaginase, with up to 18% incidence in pediatric and AYA patientsCitation69 and greater than 50% in adult patients.Citation71,Citation93 Formulation-dependent effects have been noted, with patients receiving pegaspargase in the Total XVI trialCitation94 having higher incidence of grade 4 hypertriglyceridemia compared to those in the Total XV trial receiving native E. coli L-asparaginase (10.5% versus 5.5%, p=0.007). Notably, a subset of patients receiving Erwinia asparaginase in the Total XVI trial did not develop grade 4 hypertriglyceridemia.Citation82 There was no association between hypertriglyceridemia and pancreatitis found in these studies. Because triglyceride levels often resolve to baseline without medical intervention, asparaginase can be continued without dose modification, with consideration of fibrates for high-grade toxicity.
Coagulopathies and Thromboses
Asparaginase-associated coagulopathies are thought to occur through pleiotropic effects on the coagulation and fibrinolytic pathways. Asparagine depletion leads to decreased serum levels of protein C, protein S, plasminogen, antithrombin (AT), and fibrinogen. This can be exacerbated by synthetic dysfunction due to hepatotoxicity. Concomitant use of corticosteroids also contributes through inhibition of fibrinolysis and increased levels of von Willebrand factor, factor VIII, and plasminogen activator inhibitor-1.Citation68 The incidence is age-dependent, with other risk factors including obesity, lower white blood cell counts, or mediastinal mass at diagnosis.Citation68 The incidence of thrombotic events in the pediatric population is ≤5% based on DCFI clinical trials.
Lower-limb and catheter-associated venous thromboembolism (VTE) are the most common, though other life-threatening events such as pulmonary embolism (PE), arterial thromboembolism, and cavernous sinus thromboses (CST) can occur. The latter is often associated with intracranial hemorrhage. Thrombotic events tend to occur earlier during therapy, so factors contributing to their development are likely not limited to asparaginase effects: disease-related prothrombotic state, venous catheter placement, and/or steroid administration.Citation95
Recommendations for management are similar to that for other VTEs with some special considerations (). Successful use of direct oral anticoagulants (DOAC) has been reported, though it is currently not recommended for use by some in this setting.Citation95 Asparaginase should be held pending stability and discontinued for CST or other grade 4 events. For hemorrhagic events, asparaginase should be held or discontinued depending on location and degree, with consideration of factor replacement.
The role of prophylaxis is less clear. In a retrospective studyCitation96 of patients treated on DFCI Consortium protocols, VTE occurred in 8% of patients, with higher incidence in adults (34%). The role of VTE prophylaxis in adult patients was assessedCitation97 following a protocol amendment to patients treated at DCFI. Two-year cumulative incidence of VTE (41% to 28%) and PE (16% to 8%) both improved, but not with statistical significance. However, bleeding complications were also not significantly increased with the addition of anticoagulation (0% versus 6%, p=0.26). Prophylactic administration of cryoprecipitate is not recommended in the absence of active bleeding due to the increased risk of VTE observed in patients receiving cryoprecipitate in this setting,Citation71,Citation95 nor is prophylactic AT replacement.
Pancreatitis
Asparaginase-associated pancreatitis (AAP) has been noted in the earliest studies,Citation98–Citation100 however the mechanism remains unclear. Incidence in pediatric patients is up to 18%Citation59,Citation63,Citation101 and up to 14% in adults.Citation59,Citation60,Citation63,Citation71,Citation102 Several studies have attempted to identify risk factors for development of AAP. One systematic reviewCitation103 identified older age, higher disease-risk stratification, pegaspargase, and dosing as potential risk factors. Multiple studies have identified potential genetic associations,Citation104–Citation106 including those already known to be associated with alcohol-induced or idiopathic pancreatitis in adults. Asparaginase should be held pending resolution of asymptomatic (chemical) pancreatitis and should be permanently discontinued for grade ≥3 toxicity. Prophylactic use of octreotide in both pediatric and adult patients at risk for AAP may be beneficial,Citation107 however this is currently not in widespread use.
Future Directions and Ongoing Trials
Novel Asparaginase Formulations
JZP-458
JZP-458 (RylazeTM - Jazz Pharmaceuticals) is a recombinant Erwinia asparaginase produced in Pseudomonas fluorescens without immunologic cross-reactivity with native asparaginase.Citation30 A randomized, single-center, open-label Phase 1 study in healthy adultsCitation108 demonstrated safety, tolerability, and therapeutic SAA levels when dosed at 25 mg/m2 IM and 37.5 m/m2 IV on a Monday/Wednesday/Friday schedule. A Phase 2/3 studyCitation109 (NCT04145531) is ongoing in patients with ALL/LBL who experienced hypersensitivity reactions or silent inactivation with E. coli asparaginase and at least one treatment course remaining. Each course of asparaginase was substituted with 6 doses of JZP-458 on a Monday/Wednesday/Friday schedule with escalating doses in each cohort. Preliminary dataCitation110 demonstrated a positive risk-benefit profile when dosed at 25 mg/m2 IM on Monday and Wednesday and 50 mg/m2 on Friday with therapeutic SAA levels detected in >90% at 48 and 72 hours post-administration. Grade ≥3 all-cause toxicities occurred in 72% of patients with abnormal liver function tests (62%) as the most common all-grade toxicity. Hypersensitivity reactions occurred in 25% (any-grade) and 2% (grade ≥3) of patients.
Eryaspase
Eryaspase (GRASPA® - Erytech) is a formulation of erythrocyte-encapsulated E. coli asparaginase designed to increase its half-life and bioavailability and decrease immunogenicity. Several trials investigated this formulation in pediatric and adult ALL.Citation111,Citation112 Among the more definitive studies, the GRASPALL 2009–06 trialCitation111 assessed eryaspase combined with multiagent chemotherapy in adult and pediatric patients with relapsed Ph-negative ALL. Patients who had no prior allergy to L-asparaginase were randomized to receive either native asparaginase (10,000 IU/m2) or eryaspase (150 IU/kg); those with prior allergy received eryaspase. Hypersensitivity reactions were less frequent (0% vs 43%, p<0.001) and asparaginase activity maintained for longer (25.5 vs 9.8 days, p<0.001) in the eryaspase cohort. The NOR-GRASPALL 2016 study (NCT03267030) is evaluating eryaspase in combination with multiagent chemotherapy in patients with non-high-risk ALL who develop pegaspargase hypersensitivity. Patients received eryaspase at 150 U/kg to complete asparaginase therapy (1–7 doses). Preliminary dataCitation112 demonstrated detectable SAA at expected nadirs 14 days following administration in 94.7% of patients with 90.7% of samples >100 U/L and 69.3% >400 U/L. Adverse events related to eryaspase were noted in 22%, including six patients with a possible allergic reaction and three with low activity.
Calaspargase Pegol
Calaspargase pegol (AsparlasTM - Servier Pharmaceuticals) was FDA approved in 2018, with data from the DCFI 11–001 Phase III trialCitation23 noting similar outcomes, SAA, and toxicity profile to pegaspargase in patients (ages 1–21) with newly diagnosed ALL or LBL randomized to receive either IV pegaspargase or calaspargase pegol. Given these findings in this population, a multicenter, open-label, single-arm phase 2/3 trial (NCT04817761) is underway, incorporating calaspargase pegol into a COG backbone for adults (ages 22–65) with newly diagnosed Ph-negative ALL.
Asparaginase ± Immunotherapy
Immunotherapeutic approaches targeting leukemic antigens have demonstrated tremendous promise in the treatment of ALL, both in the upfront and relapsed/refractory (R/R) setting, which raises the potential for addition of these agents to multiagent chemotherapy backbones containing asparaginase.
Inotuzumab ozogamicin (InO) is an antibody–drug conjugate consisting of a humanized anti-CD22 IgG4 monoclonal antibody linked to the cytotoxic agent calicheamicin. InO is FDA-approved as monotherapy for R/R B-ALL based on data demonstrating high rates of CR in patients treated with InO compared to salvage chemotherapy alone.Citation113,Citation114 The A041501 clinical trialCitation115 (NCT03150693) is a phase III trial combining InO with multiagent chemotherapy similar to the C10403 regimen in AYA patients with newly diagnosed B-ALL. InO is administered on days 1, 8, and 15 during the remission induction phase with a primary outcome measure of EFS.
Blinatumomab is a bispecific T-cell engager targeting CD19 and CD3 approved for R/R B-ALL based on results of the TOWER trialCitation116 and for treatment of MRD based on the BLAST trial.Citation117 Several studies are currently evaluating its efficacy as frontline therapy in both pediatric and adult B-ALL. The AALL1731 trial (NCT03914625) is a Phase 3 study investigating the addition of blinatumomab in between cycles of a standard asparaginase-containing multiagent chemotherapy regimen with primary endpoints of DFS in children and young adults (ages 1–31) with newly diagnosed standard-risk B-ALL, B-ALL associated with Down syndrome, or localized B-LBL.
Both InO and blinatumomab are associated with hepatic toxicity,Citation118 including sinusoidal obstruction syndrome in the case of InO, particularly in those undergoing subsequent HCT. Given the relatively high incidence of hepatotoxicity in patients receiving asparaginase, it will be important to determine whether the combination blinatumomab or InO in regimens containing asparaginase whether administered simultaneous or in sequentially will exacerbate these toxicities.
Asparaginase ± Targeted Agents
Tyrosine kinase inhibitors (TKI) are an essential component of the management of Ph-positive ALL and have been added to intensive regimens containing asparaginase in the pediatric population. Dasatinib in combination with multiagent chemotherapy including asparaginase in the adult population has also been reported. In the EWALL-PH-01 study,Citation119 dasatinib administered in combination with a low-intensity asparaginase-containing regimen in older patients (age≥55) resulted in CR of 96%, 1-year RFS 58%, and 5-year OS 36%. In contrast, significant toxicity was noted in the UKALL14 study using imatinib.Citation120 Other targeted agents are also being actively studied in ALL. A phase 1 trial (NCT03571321) is ongoing to assess the benefit of ruxolitinib in combination with multiagent chemotherapy including pegaspargase for AYA with Ph-like ALL who achieved CR following induction chemotherapy.
Therapeutic Drug Monitoring
TDM for serum asparaginase activity is feasible with FDA and CLIA-certified assays currently available, which can be used in the context of concern for silent inactivation or an ambiguous allergic reaction. SAA of ≥0.1 IU/mL has been accepted as a suitable target trough level to ensure clinically efficacious serum asparagine depletion. Given the differing pharmacokinetics of pegaspargase and Erwinia asparaginase, experts recommend this trough to be achieved 14 days post-administration for pegaspargase and prior to each dose for Erwinia asparaginase.Citation26 The optimal level prior to 14 days is unclear; however, several experts recommend that all patients receiving asparaginase be tested regardless to minimize the possibility of underdosing due to missed silent inactivation with SAA measurement 3–7 days following non-Erwinia asparaginase administration and immediate transition to Erwinia asparaginase for level <0.1 IU/mL. TDM also offers the possibility of individualized dosing strategies, though this is not done outside of the context of clinical trials. Intriguing recent data from the DCOG ALL-11 studyCitation121,Citation122 noted that TDM could result in significant dose reductions of pegaspargase with retained therapeutic activity, though notably the effect on toxicity was minimal. Another recent studyCitation24 did not note a significant association between overall asparaginase-associated toxicity and SAA, but it did note increased risk of pancreatitis and osteonecrosis with increasing SAA.
Institutional Approach to Use of Asparaginase in Adults with ALL
As we have described, there are many different strategies in which asparaginase can be considered in the management of adult ALL. However, how to implement such approaches optimally remains a subject of some debate. Lacking a uniformly accepted strategy, these are some general principles used at our center when deciding between these many different approaches. They are based on the totality of the literature summarized above, though specific references are cited when appropriate.
In the context of front-line therapy, we primarily reserve the use of pegaspargase for young adults with Ph-negative ALL as part of the C10403 regimen.Citation60 For patients with relapsed disease, particularly T-cell ALL and/or with CNS involvement, we may use pediatric salvage regimens like ALL R3Citation123 or POG 9412.Citation124 We will generally use these approaches for patients up to age 40, though older age within this range and elevated BMI (particularly over 30 kg/m2) raises concerns for toxicity. One way to potentially mitigate this is to cap doses of pegaspargase (3750 U). We do not use any form of thrombotic prophylaxis. In fact, we typically do not monitor clotting times and fibrinogen levels: they will often be abnormal, enticing practitioners to intervene out of concern for hemorrhagic complication, despite the greater risk of thrombosis.Citation125
Our practice surrounding the risk of asparaginase-mediated reactions has varied, in part due to the shifting availability of Erwinia asparaginase. As of this writing, we typically provide premedication in the form of acetaminophen, diphenhydramine, and (when not being given as part of the treatment regimen) corticosteroids to prevent infusion-related reactions. The downside of such an approach is that it may increase the risk of silent inactivation. However, this is an uncommon phenomenon, and any adverse reaction regardless of etiology can negatively impact the patient (up to and including refusal to receive subsequent doses). Historically, we have not routinely monitored SAA levels. One reason for this was due to system-based challenges in identifying a reliable laboratory that could perform this assay in a timely fashion. The other (and more important) reason was lack of access to an alternative asparaginase product to use in patients identified as having silent inactivation of pegaspargase. With these issues recently addressed, we are revisiting our approach to this problem. Separately, while strategies to dose-adjust pegaspargase based on SAA results are intellectually appealing, the data supporting such methods are relatively lacking. In the event of an infusion-related reaction, we generally use the timing and nature of symptoms and signs to discriminate between anaphylactoid vs antibody-mediated hypersensitivity reactions.Citation84 In cases that are harder to discriminate, we will check a SAA and ammonia levels as soon as feasible. If antibody-mediated neutralization is ultimately suspected, we will then switch to Erwinia asparaginase for all subsequent doses. This includes an attempt to make up for the dose impacted by the observed reaction, since the reaction would render that dose inert.
There tends to be less nuance and controversy surrounding management of other adverse events from asparaginase, so our practice typically follows the recommendations and guidelines cited above (). Despite the limited data,Citation74 we have used L-carnitine and vitamin B complex in cases of severe hepatic toxicity (eg, bilirubin >10 mg/dL); our anecdotal experience has been mixed. Since the evidence supporting this strategy is relatively modest (ie, unclear magnitude of benefit and theoretical deleterious impact on therapeutic intent of asparaginase), we have reserved this intervention for the most significant cases of liver injury. In cases of significant hypertriglyceridemia, we typically institute gemfibrozil for the remainder of the asparaginase-containing portion of the treatment, discontinuing this agent once the asparaginase-containing portion of the treatment is complete and fasting lipid levels have improved. VTE is typically managed either with LMWH or DOAC. While the latter have not been studied thoroughly in this specific situation, their safety profile, ease of administration, and mechanism of action make them appealing, particularly since they work independent of antithrombin levels. Similar to gemfibrozil, we typically continue therapeutic anticoagulation for at least as long as the asparaginase-containing treatment, assuming that asparaginase was the inciting event. Clinically significant pancreatitis almost always leads to permanent discontinuation of asparaginase.
Conclusion
Asparaginase has been an essential component of ALL therapy for decades. However, until relatively recently, its use has been limited to the pediatric population. Its success in these patients and several seminal studies demonstrating its potential to improve outcomes in the AYA and adult population has led to its broader use. In these populations, however, particularly in older adult patients, it is associated with increased morbidity. An understanding of its unique side-effect profile and management is critical to mitigate treatment-related morbidity and to avoid inferior outcomes due to inappropriate dose reduction or cessation. Ongoing areas of investigation include the incorporation of asparaginase into current adult treatment paradigms, combination with immunotherapy or targeted agents, novel formulations, and therapeutic drug monitoring.
Disclosure
RDC has received research funding from Amgen, Kite/Gilead, Merck, Pfizer, Servier, and Vanda Pharmaceuticals; honoraria/consulting fees from Amgen, Kite/Gilead, and Pfizer; travel support from Pfizer; participation on a data safety monitoring board for Pepromene Bio. KRJ is supported by the University of Washington, Division of Hematology Training Grant, NIH T32HL007093. The authors report no other conflicts of interest in this work.
References
- Howlader NA, Krapcho M, Miller D, et al. SEER cancer statistics review, 1975–2018; 2021. Available from: https://seer.cancer.gov/csr/1975_2018/. Accessed February 13, 2022.
- Boissel N, Auclerc MF, Lhéritier V, et al. Should adolescents with acute lymphoblastic leukemia be treated as old children or young adults? Comparison of the French FRALLE-93 and LALA-94 trials. J Clin Oncol. 2003;21(5):774–780. doi:10.1200/JCO.2003.02.053
- de Bont JM, Holt B, Dekker AW, van der Does-van den Berg A, Sonneveld P, Pieters R. Significant difference in outcome for adolescents with acute lymphoblastic leukemia treated on pediatric vs adult protocols in the Netherlands. Leukemia. 2004;18(12):2032–2035. doi:10.1038/sj.leu.2403538
- Hallböök H, Gustafsson G, Smedmyr B, Söderhäll S, Heyman M. Treatment outcome in young adults and children >10 years of age with acute lymphoblastic leukemia in Sweden: a comparison between a pediatric protocol and an adult protocol. Cancer. 2006;107(7):1551–1561. doi:10.1002/cncr.22189
- Ramanujachar R, Richards S, Hann I, et al. Adolescents with acute lymphoblastic leukaemia: outcome on UK national paediatric (ALL97) and adult (UKALLXII/E2993) trials. Pediatr Blood Cancer. 2007;48(3):254–261. doi:10.1002/pbc.20749
- Ribera JM, Oriol A, Sanz MA, et al. Comparison of the results of the treatment of adolescents and young adults with standard-risk acute lymphoblastic leukemia with the Programa Español de Tratamiento en Hematología pediatric-based protocol ALL-96. J Clin Oncol. 2008;26(11):1843–1849. doi:10.1200/JCO.2007.13.7265
- Stock W, La M, Sanford B, et al. What determines the outcomes for adolescents and young adults with acute lymphoblastic leukemia treated on cooperative group protocols? A comparison of Children’s Cancer Group and Cancer and Leukemia Group B studies. Blood. 2008;112(5):1646–1654. doi:10.1182/blood-2008-01-130237
- Kidd JG. Regression of transplanted lymphomas induced in vivo by means of normal Guinea pig serum. I. Course of transplanted cancers of various kinds in mice and rats given Guinea pig serum, horse serum, or rabbit serum. J Exp Med. 1953;98(6):565–582. doi:10.1084/jem.98.6.565
- Broome JD. Evidence that the L-asparaginase activity of guinea pig serum is responsible for its antilymphoma effects. Nature. 1961;191(4793):1114–1115. doi:10.1038/1911114a0
- Broome JD. Evidence that the L-asparaginase of Guinea pig serum is responsible for its antilymphoma effects. I. Properties of the L-asparaginase of Guinea pig serum in relation to those of the antilymphoma substance. J Exp Med. 1963;118(1):99–120. doi:10.1084/jem.118.1.99
- Broome JD. Evidence that the L-asparaginase of Guinea pig serum is responsible for its antilymphoma effects. II. Lymphoma 6C3HED cells cultured in a medium devoid of L-asparagine lose their susceptibility to the effects of Guinea pig serum in vivo. J Exp Med. 1963;118(1):121–148. doi:10.1084/jem.118.1.121
- Ho DH, Whitecar JP Jr, Luce JK, Frei E 3rd. L-asparagine requirement and the effect of L-asparaginase on the normal and leukemic human bone marrow. Cancer Res. 1970;30(2):466–472.
- Yellin TO, Wriston JC Jr. Antagonism of purified asparaginase from Guinea pig serum toward lymphoma. Science. 1966;151(3713):998–999. doi:10.1126/science.151.3713.998
- Dolowy WC, Henson D, Cornet J, Sellin H. Toxic and antineoplastic effects of L-asparaginase. Study of mice with lymphoma and normal monkeys and report on a child with leukemia. Cancer. 1966;19(12):1813–1819. doi:10.1002/1097-0142(196612)19:12<1813::AID-CNCR2820191208>3.0.CO;2-E
- Hill JM, Roberts J, Loeb E, Khan A, MacLellan A, Hill RW. L-asparaginase therapy for leukemia and other malignant neoplasms. Remission in human leukemia. JAMA. 1967;202(9):882–888. doi:10.1001/jama.1967.03130220070012
- Oettgen HF, Stephenson PA, Schwartz MK, et al. Toxicity of E. coli L-asparaginase in man. Cancer. 1970;25(2):253–278. doi:10.1002/1097-0142(197002)25:2<253::AID-CNCR2820250204>3.0.CO;2-U
- Lomelino CL, Andring JT, McKenna R, Kilberg MS. Asparagine synthetase: function, structure, and role in disease. J Biol Chem. 2017;292(49):19952–19958. doi:10.1074/jbc.R117.819060
- Narta UK, Kanwar SS, Azmi W. Pharmacological and clinical evaluation of L-asparaginase in the treatment of leukemia. Crit Rev Oncol Hematol. 2007;61(3):208–221. doi:10.1016/j.critrevonc.2006.07.009
- Batool T, Makky EA, Jalal M, Yusoff MM. A comprehensive review on L-Asparaginase and its applications. Appl Biochem Biotechnol. 2016;178(5):900–923. doi:10.1007/s12010-015-1917-3
- Lubkowski J, Wlodawer A. Structural and biochemical properties of L-asparaginase. Febs J. 2021;288(14):4183–4209. doi:10.1111/febs.16042
- Ettinger LJ, Kurtzberg J, Voûte PA, Jürgens H, Halpern SL. An open-label, multicenter study of polyethylene glycol-L-asparaginase for the treatment of acute lymphoblastic leukemia. Cancer. 1995;75(5):1176–1181. doi:10.1002/1097-0142(19950301)75:5<1176::AID-CNCR2820750519>3.0.CO;2-Y
- Heo YA, Syed YY, Keam SJ. Pegaspargase: a review in acute lymphoblastic leukaemia. Drugs. 2019;79(7):767–777. doi:10.1007/s40265-019-01120-1
- Vrooman LM, Blonquist TM, Stevenson KE, et al. Efficacy and toxicity of pegaspargase and calaspargase pegol in childhood acute lymphoblastic leukemia: results of DFCI 11-001. J Clin Oncol. 2021;39(31):3496–3505. doi:10.1200/JCO.20.03692
- Kloos R, van der Sluis IM, Mastrobattista E, Hennink W, Pieters R, Verhoef JJ. Acute lymphoblastic leukaemia patients treated with PEGasparaginase develop antibodies to PEG and the succinate linker. Br J Haematol. 2020;189(3):442–451. doi:10.1111/bjh.16254
- Servier Pharmaceuticals. Oncaspar (pegaspargase): US prescribing information; 2021. Available from: http://www.fda.gov. Accessed February 4, 2022.
- van der Sluis IM, Vrooman LM, Pieters R, et al. Consensus expert recommendations for identification and management of asparaginase hypersensitivity and silent inactivation. Haematologica. 2016;101(3):279–285. doi:10.3324/haematol.2015.137380
- Servier Pharmaceuticals. Asparlas (calaspargase pegol): US prescribing information; 2021. Available from: http://www.fda.gov. Accessed February 4, 2022.
- Salzer WL, Asselin B, Supko JG, et al. Erwinia asparaginase achieves therapeutic activity after pegaspargase allergy: a report from the Children’s Oncology Group. Blood. 2013;122(4):507–514. doi:10.1182/blood-2013-01-480822
- Maese L, Rizzari C, Coleman R, Power A, van der Sluis I, Rau RE. Can recombinant technology address asparaginase Erwinia chrysanthemi shortages? Pediatr Blood Cancer. 2021;68(10):e29169. doi:10.1002/pbc.29169
- Jazz Pharmaceuticals. Rylaze (asparaginase erwinia chrysanthemi (recombinant)-rywn): US prescribing information. Available from: http://www.fda.gov. Accessed February 4, 2022.
- Schwartz MK, Lash ED, Oettgen HF, Tomato FA. L-asparaginase activity in plasma and other biological fluids. Cancer. 1970;25(2):244–252. doi:10.1002/1097-0142(197002)25:2<244::AID-CNCR2820250203>3.0.CO;2-V
- Henriksen LT, Nersting J, Raja RA, et al. Cerebrospinal fluid asparagine depletion during pegylated asparaginase therapy in children with acute lymphoblastic leukaemia. Br J Haematol. 2014;166(2):213–220. doi:10.1111/bjh.12865
- Swierczewska M, Lee KC, Lee S. What is the future of PEGylated therapies? Expert Opin Emerg Drugs. 2015;20(4):531–536. doi:10.1517/14728214.2015.1113254
- Asselin B, Rizzari C. Asparaginase pharmacokinetics and implications of therapeutic drug monitoring. Leuk Lymphoma. 2015;56(8):2273–2280. doi:10.3109/10428194.2014.1003056
- Asselin BL, Whitin JC, Coppola DJ, Rupp IP, Sallan SE, Cohen HJ. Comparative pharmacokinetic studies of three asparaginase preparations. J Clin Oncol. 1993;11(9):1780–1786. doi:10.1200/JCO.1993.11.9.1780
- Angiolillo AL, Schore RJ, Devidas M, et al. Pharmacokinetic and pharmacodynamic properties of calaspargase pegol Escherichia coli L-asparaginase in the treatment of patients with acute lymphoblastic leukemia: results from Children’s Oncology Group Study AALL07P4. J Clin Oncol. 2014;32(34):3874–3882. doi:10.1200/JCO.2014.55.5763
- Riccardi R, Holcenberg JS, Glaubiger DL, Wood JH, Poplack DG. L-asparaginase pharmacokinetics and asparagine levels in cerebrospinal fluid of rhesus monkeys and humans. Cancer Res. 1981;41(11 Pt 1):4554–4558.
- Hunger SP, Mullighan CG, Longo DL. Acute lymphoblastic leukemia in children. N Engl J Med. 2015;373(16):1541–1552. doi:10.1056/NEJMra1400972
- Bender C, Maese L, Carter-Febres M, Verma A. Clinical utility of pegaspargase in children, adolescents and young adult patients with acute lymphoblastic leukemia: a review. Blood Lymphat Cancer. 2021;11:25–40. doi:10.2147/BLCTT.S245210
- Egler RA, Ahuja SP, Matloub Y. L-asparaginase in the treatment of patients with acute lymphoblastic leukemia. J Pharmacol Pharmacother. 2016;7(2):62–71. doi:10.4103/0976-500X.184769
- Ortega JA, Nesbit ME Jr, Donaldson MH, et al. L-Asparaginase, vincristine, and prednisone for induction of first remission in acute lymphocytic leukemia. Cancer Res. 1977;37(2):535–540.
- Sallan SE, Hitchcock-Bryan S, Gelber R, Cassady JR, Frei E 3rd, Nathan DG. Influence of intensive asparaginase in the treatment of childhood non-T-cell acute lymphoblastic leukemia. Cancer Res. 1983;43(11):5601–5607.
- Clavell LA, Gelber RD, Cohen HJ, et al. Four-agent induction and intensive asparaginase therapy for treatment of childhood acute lymphoblastic leukemia. N Engl J Med. 1986;315(11):657–663. doi:10.1056/NEJM198609113151101
- Amylon MD, Shuster J, Pullen J, et al. Intensive high-dose asparaginase consolidation improves survival for pediatric patients with T cell acute lymphoblastic leukemia and advanced stage lymphoblastic lymphoma: a Pediatric Oncology Group study. Leukemia. 1999;13(3):335–342. doi:10.1038/sj.leu.2401310
- Pession A, Valsecchi MG, Masera G, et al. Long-term results of a randomized trial on extended use of high dose L-asparaginase for standard risk childhood acute lymphoblastic leukemia. J Clin Oncol. 2005;23(28):7161–7167. doi:10.1200/JCO.2005.11.411
- Abshire TC, Pollock BH, Billett AL, Bradley P, Buchanan GR. Weekly polyethylene glycol conjugated L-asparaginase compared with biweekly dosing produces superior induction remission rates in childhood relapsed acute lymphoblastic leukemia: a Pediatric Oncology Group Study. Blood. 2000;96(5):1709–1715. doi:10.1182/blood.V96.5.1709
- Silverman LB, Gelber RD, Dalton VK, et al. Improved outcome for children with acute lymphoblastic leukemia: results of Dana-Farber Consortium Protocol 91-01. Blood. 2001;97(5):1211–1218. doi:10.1182/blood.V97.5.1211
- Larsen EC, Devidas M, Chen S, et al. Dexamethasone and high-dose methotrexate improve outcome for children and young adults with high-risk B-acute lymphoblastic leukemia: a report from Children’s Oncology Group Study AALL0232. J Clin Oncol. 2016;34(20):2380–2388. doi:10.1200/JCO.2015.62.4544
- Winter SS, Dunsmore KP, Devidas M, et al. Improved survival for children and young adults with T-lineage acute lymphoblastic leukemia: results From the Children’s Oncology Group AALL0434 methotrexate randomization. J Clin Oncol. 2018;36(29):2926–2934. doi:10.1200/JCO.2018.77.7250
- Ram R, Wolach O, Vidal L, Gafter-Gvili A, Shpilberg O, Raanani P. Adolescents and young adults with acute lymphoblastic leukemia have a better outcome when treated with pediatric-inspired regimens: systematic review and meta-analysis. Am J Hematol. 2012;87(5):472–478. doi:10.1002/ajh.23149
- Rijneveld AW, van der Holt B, Daenen SM, et al. Intensified chemotherapy inspired by a pediatric regimen combined with allogeneic transplantation in adult patients with acute lymphoblastic leukemia up to the age of 40. Leukemia. 2011;25(11):1697–1703. doi:10.1038/leu.2011.141
- Huguet F, Leguay T, Raffoux E, et al. Pediatric-inspired therapy in adults with Philadelphia chromosome-negative acute lymphoblastic leukemia: the GRAALL-2003 study. J Clin Oncol. 2009;27(6):911–918. doi:10.1200/JCO.2008.18.6916
- Thomas X, Boiron JM, Huguet F, et al. Outcome of treatment in adults with acute lymphoblastic leukemia: analysis of the LALA-94 trial. J Clin Oncol. 2004;22(20):4075–4086. doi:10.1200/JCO.2004.10.050
- Huguet F, Chevret S, Leguay T, et al. Intensified therapy of acute lymphoblastic leukemia in adults: report of the randomized GRAALL-2005 clinical trial. J Clin Oncol. 2018;36(24):2514–2523. doi:10.1200/JCO.2017.76.8192
- Storring JM, Minden MD, Kao S, et al. Treatment of adults with BCR-ABL negative acute lymphoblastic leukaemia with a modified paediatric regimen. Br J Haematol. 2009;146(1):76–85. doi:10.1111/j.1365-2141.2009.07712.x
- Gökbuget N, Beck J, Brandt K, et al. Significant improvement of outcome in Adolescents and Young adults (AYAs) aged 15–35 years with Acute Lymphoblastic Leukemia (ALL) with a pediatric derived adult ALL protocol; results of 1529 AYAs in 2 consecutive trials of the German Multicenter Study Group for adult ALL (GMALL). Blood. 2013;122(21):839.
- Wetzler M, Sanford BL, Kurtzberg J, et al. Effective asparagine depletion with pegylated asparaginase results in improved outcomes in adult acute lymphoblastic leukemia: cancer and Leukemia Group B Study 9511. Blood. 2007;109(10):4164–4167. doi:10.1182/blood-2006-09-045351
- DeAngelo DJ, Stevenson KE, Dahlberg SE, et al. Long-term outcome of a pediatric-inspired regimen used for adults aged 18–50 years with newly diagnosed acute lymphoblastic leukemia. Leukemia. 2015;29(3):526–534. doi:10.1038/leu.2014.229
- Toft N, Birgens H, Abrahamsson J, et al. Results of NOPHO ALL2008 treatment for patients aged 1–45 years with acute lymphoblastic leukemia. Leukemia. 2018;32(3):606–615. doi:10.1038/leu.2017.265
- Stock W, Luger SM, Advani AS, et al. A pediatric regimen for older adolescents and young adults with acute lymphoblastic leukemia: results of CALGB 10403. Blood. 2019;133(14):1548–1559. doi:10.1182/blood-2018-10-881961
- Advani AS, Larsen E, Laumann K, et al. Comparison of CALGB 10403 (Alliance) and COG AALL0232 toxicity results in young adults with acute lymphoblastic leukemia. Blood Adv. 2021;5(2):504–512. doi:10.1182/bloodadvances.2020002439
- Geyer MB, Ritchie EK, Rao AV, et al. Pediatric-inspired chemotherapy incorporating pegaspargase is safe and results in high rates of minimal residual disease negativity in adults up to age 60 with Philadelphia chromosome-negative acute lymphoblastic leukemia. Haematologica. 2021;106(8):2086–2094. doi:10.3324/haematol.2020.251686
- Rytting ME, Thomas DA, O’Brien SM, et al. Augmented Berlin-Frankfurt-Münster therapy in adolescents and young adults (AYAs) with acute lymphoblastic leukemia (ALL). Cancer. 2014;120(23):3660–3668. doi:10.1002/cncr.28930
- Thomas DA, O’Brien S, Faderl S, et al. Chemoimmunotherapy with a modified hyper-CVAD and rituximab regimen improves outcome in de novo Philadelphia chromosome-negative precursor B-lineage acute lymphoblastic leukemia. J Clin Oncol. 2010;28(24):3880–3889. doi:10.1200/JCO.2009.26.9456
- Maury S, Chevret S, Thomas X, et al. Rituximab in B-lineage adult acute lymphoblastic leukemia. N Engl J Med. 2016;375(11):1044–1053. doi:10.1056/NEJMoa1605085
- Stock W, Douer D, DeAngelo DJ, et al. Prevention and management of asparaginase/pegasparaginase-associated toxicities in adults and older adolescents: recommendations of an expert panel. Leuk Lymphoma. 2011;52(12):2237–2253. doi:10.3109/10428194.2011.596963
- National Comprehensive Cancer Network. Acute lymphoblastic leukemia (version 4.2021). Available from: https://www.nccn.org. Accessed February 13, 2022.
- Aldoss I, Douer D. How I treat the toxicities of pegasparaginase in adults with acute lymphoblastic leukemia. Blood. 2020;135(13):987–995. doi:10.1182/blood.2019002132
- Burke PW, Hoelzer D, Park JH, Schmiegelow K, Douer D. Managing toxicities with asparaginase-based therapies in adult ALL: summary of an ESMO Open-Cancer Horizons roundtable discussion. ESMO Open. 2020;5(5):e000858. doi:10.1136/esmoopen-2020-000858
- Schmiegelow K, Rank CU, Stock W, Dworkin E, van der Sluis I. SOHO state of the art updates and next questions: management of asparaginase toxicity in adolescents and young adults with acute lymphoblastic leukemia. Clin Lymphoma Myeloma Leuk. 2021;21(11):725–733. doi:10.1016/j.clml.2021.07.009
- Aldoss I, Douer D, Behrendt CE, et al. Toxicity profile of repeated doses of PEG-asparaginase incorporated into a pediatric-type regimen for adult acute lymphoblastic leukemia. Eur J Haematol. 2016;96(4):375–380. doi:10.1111/ejh.12600
- Burke PW, Aldoss I, Lunning MA, et al. Pegaspargase-related high-grade hepatotoxicity in a pediatric-inspired adult acute lymphoblastic leukemia regimen does not predict recurrent hepatotoxicity with subsequent doses. Leuk Res. 2018;66:49–56. doi:10.1016/j.leukres.2017.12.013
- Bodmer M, Sulz M, Stadlmann S, Droll A, Terracciano L, Krähenbühl S. Fatal liver failure in an adult patient with acute lymphoblastic leukemia following treatment with L-asparaginase. Digestion. 2006;74(1):28–32. doi:10.1159/000095827
- Al-Nawakil C, Willems L, Mauprivez C, et al. Successful treatment of l-asparaginase-induced severe acute hepatotoxicity using mitochondrial cofactors. Leuk Lymphoma. 2014;55(7):1670–1674. doi:10.3109/10428194.2013.845886
- Alshiekh-Nasany R, Douer D. L-carnitine for treatment of pegasparaginase-induced hepatotoxicity. Acta Haematol. 2016;135(4):208–210. doi:10.1159/000442342
- Arora S, Klair J, Bellizzi AM, Tanaka T. L-carnitine and vitamin B complex for PEG-L-asparaginase-induced hepatotoxicity. ACG Case Rep J. 2019;6(8):e00194. doi:10.14309/crj.0000000000000194
- Blackman A, Boutin A, Shimanovsky A, Baker WJ, Forcello N. Levocarnitine and vitamin B complex for the treatment of pegaspargase-induced hepatotoxicity: a case report and review of the literature. J Oncol Pharm Pract. 2018;24(5):393–397. doi:10.1177/1078155217710714
- Lu G, Karur V, Herrington JD, Walker MG. Successful treatment of pegaspargase-induced acute hepatotoxicity with vitamin B complex and L-carnitine. Proc. 2016;29(1):46–47. doi:10.1080/08998280.2016.11929355
- Schulte R, Hinson A, Huynh V, et al. Levocarnitine for pegaspargase-induced hepatotoxicity in older children and young adults with acute lymphoblastic leukemia. Cancer Med. 2021;10(21):7551–7560. doi:10.1002/cam4.4281
- Trang E, Ngo D, Chen J, Aldoss I, Salhotra A, Pullarkat V. Levocarnitine for pegasparaginase-induced hepatotoxicity in acute lymphoblastic leukemia. Leuk Lymphoma. 2020;61(13):3161–3164. doi:10.1080/10428194.2020.1805108
- Sudour H, Schmitt C, Contet A, Chastagner P, Feillet F. Acute metabolic encephalopathy in two patients treated with asparaginase and ondasetron. Am J Hematol. 2011;86(3):323–325. doi:10.1002/ajh.21964
- Tong WH, Pieters R, de Groot-Kruseman HA, et al. The toxicity of very prolonged courses of PEGasparaginase or Erwinia asparaginase in relation to asparaginase activity, with a special focus on dyslipidemia. Haematologica. 2014;99(11):1716–1721. doi:10.3324/haematol.2014.109413
- Beziat G, Tavitian S, Picard M, Faguer S, Recher C, Huguet F. Multiple severe toxicities of L-asparaginase and their innovative management during induction therapy of acute lymphoblastic leukemia in an adult patient. Case Rep Hematol. 2019;2019:9086570. doi:10.1155/2019/9086570
- Burke MJ, Rheingold SR. Differentiating hypersensitivity versus infusion-related reactions in pediatric patients receiving intravenous asparaginase therapy for acute lymphoblastic leukemia. Leuk Lymphoma. 2017;58(3):540–551. doi:10.1080/10428194.2016.1213826
- Burke MJ, Devidas M, Maloney K, et al. Severe pegaspargase hypersensitivity reaction rates (grade ≥3) with intravenous infusion vs. intramuscular injection: analysis of 54,280 doses administered to 16,534 patients on children’s oncology group (COG) clinical trials. Leuk Lymphoma. 2018;59(7):1624–1633. doi:10.1080/10428194.2017.1397658
- Beaupin LK, Bostrom B, Barth MJ, et al. Pegaspargase hypersensitivity reactions: intravenous infusion versus intramuscular injection - a review. Leuk Lymphoma. 2017;58(4):766–772. doi:10.1080/10428194.2016.1218004
- Li RJ, Jin R, Liu C, et al. FDA approval summary: calaspargase Pegol-mknl for treatment of acute lymphoblastic leukemia in children and young adults. Clin Cancer Res. 2020;26(2):328–331. doi:10.1158/1078-0432.CCR-19-1255
- Plourde PV, Jeha S, Hijiya N, et al. Safety profile of asparaginase Erwinia chrysanthemi in a large compassionate-use trial. Pediatr Blood Cancer. 2014;61(7):1232–1238. doi:10.1002/pbc.24938
- Vrooman LM, Supko JG, Neuberg DS, et al. Erwinia asparaginase after allergy to E. coli asparaginase in children with acute lymphoblastic leukemia. Pediatr Blood Cancer. 2010;54(2):199–205. doi:10.1002/pbc.22225
- Cooper SL, Young DJ, Bowen CJ, Arwood NM, Poggi SG, Brown PA. Universal premedication and therapeutic drug monitoring for asparaginase-based therapy prevents infusion-associated acute adverse events and drug substitutions. Pediatr Blood Cancer. 2019;66(8):e27797. doi:10.1002/pbc.27797
- McCormick M, Lapinski J, Friehling E, Smith K. Premedication prior to peg-asparaginase is cost-effective for pediatric leukemia patients. Blood. 2020;136(Supplement 1):7. doi:10.1182/blood-2020-134749
- Salzer W, Bostrom B, Messinger Y, Perissinotti AJ, Marini B. Asparaginase activity levels and monitoring in patients with acute lymphoblastic leukemia. Leuk Lymphoma. 2018;59(8):1797–1806. doi:10.1080/10428194.2017.1386305
- Daley RJ, Rajeeve S, Kabel CC, et al. Tolerability and toxicity of pegaspargase in adults 40 years and older with acute lymphoblastic leukemia. Leuk Lymphoma. 2021;62(1):176–184. doi:10.1080/10428194.2020.1824068
- Finch ER, Smith CA, Yang W, et al. Asparaginase formulation impacts hypertriglyceridemia during therapy for acute lymphoblastic leukemia. Pediatr Blood Cancer. 2020;67(1):e28040. doi:10.1002/pbc.28040
- Zwicker JI, Wang T-F, DeAngelo DJ, et al. The prevention and management of asparaginase-related venous thromboembolism in adults: guidance from the SSC on Hemostasis and Malignancy of the ISTH. J Thromb Haemost. 2020;18(2):278–284. doi:10.1111/jth.14671
- Grace RF, Dahlberg SE, Neuberg D, et al. The frequency and management of asparaginase-related thrombosis in paediatric and adult patients with acute lymphoblastic leukaemia treated on Dana-Farber Cancer Institute consortium protocols. Br J Haematol. 2011;152(4):452–459. doi:10.1111/j.1365-2141.2010.08524.x
- Grace RF, DeAngelo DJ, Stevenson KE, et al. The use of prophylactic anticoagulation during induction and consolidation chemotherapy in adults with acute lymphoblastic leukemia. J Thromb Thrombolysis. 2018;45(2):306–314. doi:10.1007/s11239-017-1597-7
- Haskell CM, Canellos GP, Leventhal BG, et al. L-asparaginase: therapeutic and toxic effects in patients with neoplastic disease. N Engl J Med. 1969;281(19):1028–1034. doi:10.1056/NEJM196911062811902
- Hill JM, Loeb E, MacLellan A, et al. Response to highly purified L-asparaginase during therapy of acute leukemia. Cancer Res. 1969;29(8):1574–1580.
- Shaw MT, Barnes CC, Madden FJ, Bagshawe KD. L-asparaginase and pancreatitis. Lancet. 1970;2(7675):721. doi:10.1016/S0140-6736(70)91990-2
- Wolthers BO, Frandsen TL, Baruchel A, et al. Asparaginase-associated pancreatitis in childhood acute lymphoblastic leukaemia: an observational Ponte di Legno Toxicity Working Group study. Lancet Oncol. 2017;18(9):1238–1248. doi:10.1016/S1470-2045(17)30424-2
- Douer D, Aldoss I, Lunning MA, et al. Pharmacokinetics-based integration of multiple doses of intravenous pegaspargase in a pediatric regimen for adults with newly diagnosed acute lymphoblastic leukemia. J Clin Oncol. 2014;32(9):905–911. doi:10.1200/JCO.2013.50.2708
- Oparaji JA, Rose F, Okafor D, et al. Risk factors for asparaginase-associated pancreatitis: a systematic review. J Clin Gastroenterol. 2017;51(10):907–913. doi:10.1097/MCG.0000000000000827
- Grimes AC, Chen Y, Bansal H, et al. Genetic markers for treatment-related pancreatitis in a cohort of Hispanic children with acute lymphoblastic leukemia. Support Care Cancer. 2021;29(2):725–731. doi:10.1007/s00520-020-05530-w
- Wang J, Cheng S, Hu L, Huang T, Huang Z, Hu S. Association of asparaginase-associated pancreatitis and ULK2 gene polymorphism. Int J Clin Exp Pathol. 2020;13(3):347–356.
- Wolthers BO, Frandsen TL, Patel CJ, et al. Trypsin-encoding PRSS1-PRSS2 variations influence the risk of asparaginase-associated pancreatitis in children with acute lymphoblastic leukemia: a Ponte di Legno toxicity working group report. Haematologica. 2019;104(3):556–563. doi:10.3324/haematol.2018.199356
- Sakaguchi S, Higa T, Suzuki M, Fujimura J, Shimizu T. Prophylactic use of octreotide for asparaginase-induced acute pancreatitis. Int J Hematol. 2017;106(2):266–268. doi:10.1007/s12185-017-2219-z
- Lin T, Hernandez-Illas M, Rey A, et al. A randomized Phase I study to evaluate the safety, tolerability, and pharmacokinetics of recombinant erwinia asparaginase (JZP-458) in healthy adult volunteers. Clin Transl Sci. 2021;14(3):870–879. doi:10.1111/cts.12947
- Maese L, Rau RE, Raetz EA, et al. A phase II/III study of JZP-458 in patients with acute lymphoblastic leukemia (ALL)/lymphoblastic lymphoma (LBL) who are hypersensitive to E. coli-derived asparaginases. J Clin Oncol. 2020;38(15_suppl):TPS7568–TPS7568. doi:10.1200/JCO.2020.38.15_suppl.TPS7568
- Maese L, Loh ML, Lin T, et al. Initial results from a Phase 2/3 study of recombinant erwinia asparaginase (JZP458) in patients with Acute Lymphoblastic Leukemia (ALL)/Lymphoblastic Lymphoma (LBL) who are allergic/hypersensitive to E. coli-derived asparaginases. Blood. 2021;138(Supplement 1):2307. doi:10.1182/blood-2021-147023
- Bertrand Y, Baruchel A, Thomas XG, et al. Clinical activity of ERY001 (erythrocyte encapsulated l-asparaginase) and native l-asparaginase (L-ASP) in combination with COOPRALL regimen in phase III randomized trial in patients with relapsed acute lymphoblastic leukemia (ALL). J Clin Oncol. 2015;33(15_suppl):7004. doi:10.1200/jco.2015.33.15_suppl.7004
- Lynggaard LS, Gottschalk Højfeldt S, Moeller L, et al. NOR-GRASPALL2016 (NCT03267030): asparaginase encapsulated in erythrocytes (eryaspase) - a promising alternative to peg-asparaginase in case of hypersensitivity. Blood. 2020;136(Supplement 1):13–14. doi:10.1182/blood-2020-139373
- Kantarjian HM, DeAngelo DJ, Stelljes M, et al. Inotuzumab ozogamicin versus standard of care in relapsed or refractory acute lymphoblastic leukemia: final report and long-term survival follow-up from the randomized, phase 3 INO-VATE study. Cancer. 2019;125(14):2474–2487. doi:10.1002/cncr.32116
- Kantarjian HM, DeAngelo DJ, Stelljes M, et al. Inotuzumab ozogamicin versus standard therapy for acute lymphoblastic leukemia. N Engl J Med. 2016;375(8):740–753. doi:10.1056/NEJMoa1509277
- Alliance for Clinical Trials in Oncology. Inotuzumab ozogamicin and frontline chemotherapy in treating young adults with newly diagnosed B acute lymphoblastic leukemia. Available from: https://clinicaltrials.gov/ct2/show/NCT03150693. Accessed February 13, 2022.
- Kantarjian H, Stein A, Gökbuget N, et al. Blinatumomab versus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med. 2017;376(9):836–847. doi:10.1056/NEJMoa1609783
- Gökbuget N, Dombret H, Bonifacio M, et al. Blinatumomab for minimal residual disease in adults with B-cell precursor acute lymphoblastic leukemia. Blood. 2018;131(14):1522–1531. doi:10.1182/blood-2017-08-798322
- Kantarjian HM, DeAngelo DJ, Advani AS, et al. Hepatic adverse event profile of inotuzumab ozogamicin in adult patients with relapsed or refractory acute lymphoblastic leukaemia: results from the open-label, randomised, phase 3 INO-VATE study. Lancet Haematol. 2017;4(8):e387–e398. doi:10.1016/S2352-3026(17)30103-5
- Rousselot P, Coudé MM, Gokbuget N, et al. Dasatinib and low-intensity chemotherapy in elderly patients with Philadelphia chromosome-positive ALL. Blood. 2016;128(6):774–782. doi:10.1182/blood-2016-02-700153
- Patel B, Kirkwood AA, Dey A, et al. Pegylated-asparaginase during induction therapy for adult acute lymphoblastic leukaemia: toxicity data from the UKALL14 trial. Leukemia. 2017;31(1):58–64. doi:10.1038/leu.2016.219
- Kloos RQH, Pieters R, Jumelet FMV, de Groot-Kruseman HA, van den Bos C, van der Sluis IM. Individualized asparaginase dosing in childhood acute lymphoblastic leukemia. J Clin Oncol. 2020;38(7):715–724. doi:10.1200/JCO.19.02292
- Kloos RQH, Mathôt R, Pieters R, van der Sluis IM. Individualized dosing guidelines for PEGasparaginase and factors influencing the clearance: a population pharmacokinetic model. Haematologica. 2021;106(5):1254–1261. doi:10.3324/haematol.2019.242289
- Parker C, Waters R, Leighton C, et al. Effect of mitoxantrone on outcome of children with first relapse of acute lymphoblastic leukaemia (ALL R3): an open-label randomised trial. Lancet. 2010;376(9757):2009–2017. doi:10.1016/S0140-6736(10)62002-8
- Barredo JC, Devidas M, Lauer SJ, et al. Isolated CNS relapse of acute lymphoblastic leukemia treated with intensive systemic chemotherapy and delayed CNS radiation: a pediatric oncology group study. J Clin Oncol. 2006;24(19):3142–3149. doi:10.1200/JCO.2005.03.3373
- Truelove E, Fielding AK, Hunt BJ. The coagulopathy and thrombotic risk associated with L-asparaginase treatment in adults with acute lymphoblastic leukaemia. Leukemia. 2013;27(3):553–559. doi:10.1038/leu.2012.290