Abstract
Chronic hepatitis C virus infection is an important public health problem, and the standard treatment (combination of pegylated interferon-α and ribavirin) has an effectiveness rate of only 40%–50%. Novel virus-specific drugs have recently been designed, and multiple compounds are under development. The approval for the clinical use of direct-acting antivirals in 2011 (boceprevir [BOC] and telaprevir, viral NS3 protease inhibitors) has increased recovery rates by up to 70%. Therefore, a highly effective treatment has been envisioned for the first time. This paper focuses on BOC and the implementation of new BOC-based treatment regimes.
Epidemiology, management, and emerging treatments for hepatitis C virus
Chronic hepatitis C virus (HCV) infection is a global public health concern because the infection progresses to end-stage liver disease, hepatocellular carcinoma, and liver failure in a considerable number of infected individuals. Once end-stage liver disease is established, the only reliable therapeutic intervention is liver transplantation, but viral recurrence is inevitable and the graft can be lost in a few years. Until recently, the standard-of-care (SOC) for treatment was based on a combination of pegylated interferon-α (peg-IFNα) and ribavirin (RBV), which is effective in 40% of patients infected with HCV genotype 1.Citation1 New therapies that improve current treatment response rates will be based in specific inhibitors of viral enzymes. Among them, two inhibitors of the viral NS3/4A serine-protease have recently been approved for clinical use. Telaprevir (TPV) (Vertex Pharmaceuticals, Cambridge, MA, USA) and boceprevir (BOC) (Merck and Co, Whitehouse Station, NJ, USA) – the first direct-acting antivirals (DAAs) for HCV to reach the clinical level – will have an impact in new treatment regimes for HCV. In some countries, a new SOC is now available for patients infected with HCV genotype 1, based on a combination of either TPV or BOC with peg-IFN-α and RBV. The introduction of these new regimes increases response rates by to up 75% in treatment-naïve patients infected with HCV genotype 1, and up to 50% in previous partial responders and relapsers who used the peg-IFN-α + RBV treatment. Variations in the latter group depend on the type of the previous response (see below).Citation2 Neither BOC nor TPV are indicated to treat infection caused by other HCV genotypes.
Current management approaches for HCV infection
Peg-IFN-α and RBV are not DAAs, but rather, immunomodulators. Although RBV may act as an immunomodulator and increases HCV mutation rates, the mechanism for HCV inhibition is largely unknown.Citation3,Citation4 Almost all patients who achieve sustained virological response (SVR, absence of detectable HCV RNA in serum 24 weeks after the end of treatment) are considered to be cured from the infection, although negativity at 12 weeks is an increasingly used metric.Citation5 Patients with SVR show histological and clinical improvements with regression of fibrosis, decreased risk for hepatocellular carcinoma, and overall reduction of liver-related morbidity and mortality.Citation6 Treatment success depends on the viral genotype, the stage of liver fibrosis, coexistence of a metabolic syndrome, age, sex, ethnicity, and host genetics. Citation7 The strongest predictor of treatment response is genetic polymorphism upstream from the interferon lambda-3 gene, IL28B. The most favorable genotypes are rs12979860 C/C, rs12980275 A/A, and rs8099917 T/T; the three SNPs in linkage disequilibrium and more common in Asians and Caucasians.Citation8 Regardless of the IL28B genotype, SVR is approximately 40% in patients infected with HCV genotype 1, and ranges from 60%–80% in those infected with genotypes 2 and 3.Citation1 Side effects include flu-like symptoms, anemia, rash, cough, and depression. Serious adverse events (AEs) are uncommon, but may result in death. While dose reductions are frequently required, particularly doses of RBV, treatment discontinuation due to AEs is rarely required (approximately 5%). Unfortunately, dose reductions greater than 20% – especially for RBV – and premature treatment discontinuation reduce the chance of achieving SVR.Citation7
New developments in HCV treatment
The first DAAs for the treatment of HCV chronic infection were approved in 2011 by the Food and Drug Administration and the European Medicines Agency for use in the United States and European Union, respectively. BOC and TPV are each given in combination with Peg-IFN-α and RBV for the treatment of genotype 1 chronic hepatitis C in adult patients with compensated liver disease.Citation9,Citation10 Both drugs are specific inhibitors of the HCV NS3/4A protease. These protease inhibitors (PI) interfere with the virus’ life cycle and inhibit the processing of the viral polyprotein, and likely restore the pathways of the innate immunity.Citation11 Several second-generation HCV NS3/4A protease inhibitors are currently being developed, such as ITMN-191, TMC435350, and MK-7009.Citation12 DAAs that target other HCV proteins are also being evaluated, such as NS4A, NS4B, NS5A, and NS5B polymerase inhibitors; some with highly promising results.Citation12
Mode of action, safety, and efficacy of BOC
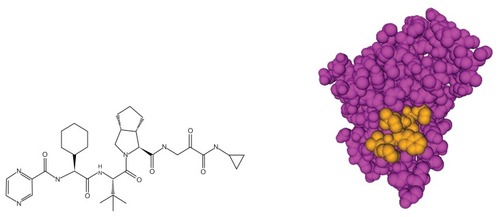
BOC (SCH503034) is a carboxamide-based HCV NS3/4A oral protease inhibitor (), which is an α-ketoamide that forms a stable, covalent and reversible complex with the viral enzyme that inhibits the cleavage of the non-structural part of the HCV polyprotein. BOC reacts with the Ser139 of the active site (serine trap inhibitor), thus compromising the catalytic triad, His57-Asp81-Ser139. In cell culture, BOC suppresses HCV replicon synthesis with IC50 and IC90 values of 200 nM and 400 nM, respectively.Citation13 The antiviral activity was unaffected by the addition of IFN-α.Citation13 BOC has shown a beneficial and safe profile for the treatment of chronic HCV genotype 1 infections in combination with Peg-IFN-α and RBV in adult patients with compensated liver disease, including compensated cirrhosis.Citation14,Citation15 Currently, neither BOC nor TPV should be used in patients infected with HCV genotypes other than genotype 1. Data on the efficacy of first-generation protease inhibitors in non-genotype 1-infected patients is scarce, which indicates some activity in HCV genotypes 2 and 4, but very limited activity in genotype 3-infected patients.Citation16 The clinical efficacy of BOC in adult individuals with chronic HCV genotype 1 infections was established in Phase II and Phase III studies examining the use of BOC both in SOC treatment-naïve and in SOC treatment-experienced subjects (relapsers and non-responders).
Figure 1 BOC, a ketoamide inhibitor of the HCV NS3 protease.
The Phase II study, P03659 (NCT00160251), evaluated the use of BOC (100–800 mg three times daily + SOC) in 357 genotype 1-infected patients from the United States and Europe who were previous non-responders to SOC. The study established that 800 mg was the optimal dose of BOC and that RBV was required to reduce viral breakthrough.Citation17 The Phase II study, SPRINT-1, evaluated the SVR rates of triple therapy (BOC 800 mg three times daily + peg-IFN- α2b + RBV for 24 or 48 weeks) in 520 treatment-naïve patients infected with HCV genotype 1, compared to the standard Peg-IFN-α2b + RBV therapy, as well as reducing the RBV dose (n = 75).Citation18,Citation19 The triple combination arm, with a treatment duration of 48 weeks, showed a significantly higher SVR rate (67%) than the SOC control arm (38%) and the reduced RBV arm (36%). The rates of SVR were even higher (75%) when a 4-week lead-in of SOC was administered before initiating BOC + peg-IFN-α2b + RBV.Citation18,Citation20 The lead-in phase aimed to limit the emergence of the BOC-resistant virus by reducing viral replication before the start of BOC. This study indicates that adding a single DAA to current HCV treatment significantly increased the SVR rates, but that peg- IFN-α + RBV were still necessary for achieving SVR when using only one DAA. In addition, using a lead-in phase of SOC before BOC was initiated appeared to modestly reduce the chance of viral breakthrough, and ultimately, the chance of resistance (9/206 versus 19/210) viral breakthroughs in patients with or without lead-in, respectively.Citation20
Two Phase III trials (SPRINT-2 and RESPOND-2) evaluated 48-week treatment strategies with response-guided therapy in patients with no detectable HCV-RNA at week 8 who later stopped treatment at week 28 (SPRINT-2) or week 36 (RESPOND-2). The SPRINT-2 trial was performed in 1097 treatment-naïve patients who were infected with HCV genotype 1 by dividing them in two cohorts of non-black (n = 938) and black (n = 159) patients. Both cohorts were randomized into three arms: (1) peg-IFNα-2b + RBV for 48 weeks, (2) BOC + peg-IFNα-2b + RBV response-guided, and (3) BOC + peg-IFNα-2b + RBV for 44 weeks. All three arms included a peg-IFNα-2b + RBV lead-in phase during the first 4 weeks. For white patients, the SVR rates were 67% and 68% in the response-guided arm and the 48-week arm, respectively, compared to 40% with SOC for 48 weeks.Citation15,Citation21 For black patients, the SVR rates were 42% and 53% in the response-guided and 48-week arms, respectively, compared to 23% with SOC for 48 weeks.Citation15,Citation21 Overall, the SVR rates between the response-guided and fixed duration BOC arms were not significantly different in the SOC-naïve patients, and the lead-in phase was not associated with increased efficacy. The rates of SVR in both BOC arms were significantly higher, compared to the controls (peg-IFNα-2b + RBV alone) in the previously untreated adult cohort with chronic HCV genotype 1 infection.
The RESPOND-2 trial was performed on 403 treatment-experienced patients who failed SOC therapy (excluding null responders) and evaluated the two treatment strategies mentioned above. The final results indicate that overall SVR rates were 59% and 66% in the response-guided and 48-week arms, respectively, compared to 21% for the retreatment with SOC alone for 48-weeks.Citation14,Citation19 Therefore, the rates of SVR were not significantly different from the response-guided and fixed duration therapy with BOC + peg-IFNα-2b + RBV for 44 weeks for SOC-experienced patients. However, the SVR rates in both BOC arms were significantly higher than the controls group (retreatment with peg-IFNα-2b + RBV alone). The breakdown of the SVR rates between the previous nonresponders and relapsers to previous SOC revealed significantly different outcomes. Previous SOC relapsers showed SVR rates of 69% and 75% in the response-guided and fixed duration BOC arms, respectively, compared to 29% in the control arm (retreatment with peg-IFNα-2b + RBV alone). The SVR rates in previous SOC partial responders were 40% and 52% in the response-guided and fixed-duration therapy BOC arms, respectively, compared to 7% following retreatment with peg-IFNα-2b + RBV alone. Finally, the 4-week Peg-IFNα-2b + RBV lead-in phase was helpful in predicting which patients (less than 1 log10 HCV-RNA first-month decline) would have a lower chance of SVR. In addition, response during the first month of BOC was a predictor of SVR, as the rates in the BOC arms were higher in patients with undetectable HCV-RNA at week 8 of therapy (ie, week 4 of adding BOC).Citation14,Citation19
HCV resistance to BOC
The selection of HCV variants that are resistant to active-site protease inhibitors by amino acid substitutions in the HCV protease domain of NS3 was demonstrated in vitro and in clinical trials of DAA monotherapy.Citation22–Citation28 Several amino acid positions are associated with resistance, yet others may act as compensatory mutations that restore fitness to resistant isolates. summarizes the available data to date on the emergence of HCV resistance to BOC and other NS3/4A protease inhibitors.
Table 1 Mutations in the HCV NS3/4A protease inducing resistance to HCV protease inhibitors
The emergence of compound-specific HCV resistance is rapid in vivo, and can even occur within the first 2 weeks of exposure to a given DAA;Citation17,Citation29–Citation31 however, some resistant strains may show reduced fitness.Citation32 HCV is a highly variable virus with a high mutation rate and a large population size that circulates as a swarm of closely related variants that can be rapidly selected.Citation33 Minority-resistant HCV variants to new DAAs (not detectable by direct population sequencing) can be hidden within the complex genetic pool of the virions that circulate in a single infected patient.Citation34 Using clonal sequence analysis, Susser et al found that minority resistance mutations can be selected at six positions within the HCV NS3 protease during BOC therapy, although 2 weeks after the end of treatment with 400 mg BOC twice or three times daily, the frequency of resistant variants declines and the number of wild-type viruses increases to 95%.Citation35 However, it remains to be determined if such low-frequency resistant variants can compromise subsequent treatment options in the case of treatment failure, because the rapid selection of low-frequency resistant variants was observed during retreatment.Citation29
The available data on HCV resistance have been reviewed recently.Citation12,Citation36 A major feature of resistance to HCV protease inhibitors is cross-resistance. The most relevant resistance mutations are substitutions in residues R155 and A156, which confer high levels of resistance to BOC and TPV and cross-resistance to most NS3 protease inhibitors. Other mutations at V36, T54, and V170 are associated with low levels of resistance to both TPV and BOC. It is important to note that (i) some TPV-resistant variants remain detectable for up to 4 years after cessation of treatment,Citation37 and (ii) that late relapse may occur 24–36 weeks after TPV + peg-IFN-α + RBV therapy.Citation31
HCV-resistant mutations can also emerge rapidly when BOC is used in monotherapy or is combined with peg- IFN-α.Citation35 After BOC monotherapy, high frequencies of resistant variants were detected by clonal sequencing of HCV quasi-species in some patients at their 1-year follow-up. Moreover, resistant mutations are rapidly selected during retreatment with BOC + peg-IFN-α in some patients.Citation29,Citation38 In the SPRINT-1 trial emergence of resistant viruses, assessed by population sequencing, was detected early on viral breakthrough, mainly in mutations V36M, T54S, and R155K (>25% of samples), as well as T54A, V55A, R155T, A156S, V158I, and V170A (5%–25% of samples), and V36A, V36L, and I170T (<5% of samples).Citation20 In addition, more than 25% of patients with viral breakthroughs carried cross-resistant mutations of both BOC and TPV.Citation20 Data from the follow-up study, P05063 (NCT00689390), indicate that at least one resistant mutation persists for more than 1 year in patients who did not achieve SVR in previous BOC trials (n = 174).Citation39 The most common resistance mutations were R155K (64%), T54S (54%), V36M (54%), and T54A (22%) during follow-up. Furthermore, the overall reversion to the wild-type virus was seen in 59% of the patients over a 2-year period, but T54S- and R155K-carrying viruses reverted more slowly. The authors reported no late relapse in patients who achieved SVR (n = 290) in this follow-up cohort.Citation39
Because HCV isolates are widely variable, and infections with HCV genotypes other than genotype 1 account for a large number of chronic carriers worldwide,Citation40 defining the variability of HCV NS3/4A protease in natural isolates will be an important step in determining the potential selection of naturally resistant strains, as in the case of human immunodeficiency virus (HIV).Citation41 A relevant polymorphism of NS3/4 proteases between HCV subtypes was found in sites associated either with resistance or with compensatory mutations after an analysis of more than 350 worldwide viral isolates (genotypes 1–6).Citation42 For instance, V170A (which confers low levels of resistance to BOC) was present in 184/275 HCV genotype 1 isolates, and D168V/A was an amino acid signature in HCV genotype 3, which explains the reduced sensitivity of genotype 3 viruses to ciluprevir, and potentially to other protease inhibitors.Citation42 The different genetic barriers to resistance between HCV subtypes 1a and 1b illustrate the relevance of the variation between the genotypes and subtypes. The genetic barrier refers to the number of nucleotide substitutions required for the virus to acquire resistance to the drug. For BOC and TPV, the differences in genetic barriers include higher viral breakthrough rates and the selection of resistant variants observed in patients infected with subtype 1a, compared to those with subtype 1b. The resistance mutation, R155K, emerges through a single nucleotide substitution in subtype 1a viruses, but requires two different substitutions in subtype 1b viruses.Citation43
Later studies involving a large number of patients also detected variants associated with resistance to PI in 5.5% and 1.4% of patients from the United States, Switzerland, and Germany who were infected with subtypes 1a or 1b, respectively, including the V36L/M and R115K variants associated with low or high-level resistance.Citation44 In HCV genotype 1-infected patients, 0.9% and 0.7% of viruses carried the V36M or the R155K variants, respectively, and patients with the R155K virus appeared to have slower viral load declines during TVR + peg-IFN-α + RBV treatment than those with wt viruses. Finally, in patients from Australia, Switzerland, and the UK, the prevalence of single resistance mutations to NS3 protease inhibitors can account for up to 4.4% of viral isolates, and the frequencies for single or combined resistance mutations to NS3 protease and/or NS5b polymerase inhibitors can be found in up to 21.5%, 44.4%, or 41.8% for subtypes 1a, 1b, or 3a, respectively.Citation45 Although the overall frequency of single resistance mutations is low in all of these studies, naturally occurring polymorphisms that confer resistance to DAAs could eventually compromise the treatment response of DAA-based regimes.Citation46
In summary, the absence of response to triple BOC + peg- IFN-α + RBV therapy is associated with the selection of viral resistant mutations. Because several second-generation NS3 protease inhibitors are in advanced clinical development, the selection of viral resistance may compromise future therapeutic options involving DAAs of the same class, and therefore, should be avoided whenever possible.
Dosing, patient adherence, and AEs
There are some concerns regarding patients’ ability to follow the dosing scheme for these new regimes. BOC dosing consists of four 200 mg capsules three times daily (8-hour intervals, with meals). Furthermore, the capsules cannot be dissolved nor broken. Regular treatment duration is 48 weeks. After the first 4-week lead-in phase with peg-IFN-α + RBV, patients are given the combination BOC + peg-IFN-α + RBV during an additional 32-week period, followed by 12 weeks of peg-IFN-α + RBV alone to complete the 48-week total treatment duration schedule. Treatment-naïve patients may be eligible for response-guided therapy (RGT) to reduce the total treatment duration to 28 weeks without detrimental effect on overall SVR rates.Citation21 However, better SVR rates were observed with the 48-week treatment in prior partial-and non-responders.Citation14
Adherence will be a key factor in assuring the success of new therapies, especially in currently approved regimes that use only one DAA, because of the evidenced risk of viral resistance to first-generation protease inhibitors when drug levels drop during treatment.Citation47 This issue is particularly relevant because viral mutants can emerge with cross-resistance profiles to newer second-generation linear and macrocyclic NS3 protease inhibitors.
Administering BOC three times daily, added to twice-daily RBV and once-weekly peg-IFN-α, is a complicated dosing profile that may compromise triple therapy regimes. Second-generation protease inhibitors need to minimize these problems. In addition, triple BOC + peg-IFN-α + RBV therapy can be associated with AEs that may be serious enough to compromise adherence and/or result in treatment discontinuation.
The most common AEs in subjects taking BOC (800 mg) plus peg-IFN-α + RBV are fatigue, headache, anemia, nausea, and dysgeusia (26%).Citation17,Citation18,Citation20 The frequency of anemia is more common in patients receiving BOC + SOC compared to those receiving SOC alone,Citation18,Citation20 and a similar picture is seen with TPV.Citation31,Citation48 In Phase III trials, anemia and dysgeusia were more common in the BOC arms than in the SOC control arms,Citation19,Citation21 and 40% of patients used epoietin alfa in the SPRINT-1 trial.Citation18 Therefore, there is a risk of additive toxic effects. Both BOC and TPV cause anemia, but because no head-to-head comparison is currently available, it is not possible to know which regime causes more anemia. Recent communications have shown that for both BOC and TPV, a RBV reduction up to 600 mg per day does not impair treatment response, and therefore, should be the first step in the management of anemia (European Association for the Study of the Liver Meeting 2012). If it is necessary to discontinue RBV, then BOC should also be stopped. Finally, BOC is metabolized by liver enzymes such as cytochrome P450 (CYP450), and several drug–drug interactions are currently under examination by ongoing studies that also require careful monitoring.Citation49,Citation50
Conclusions
The addition of BOC to peg-IFN-α + RBV significantly increases the possibility of recovery in HCV genotype 1-infected patients: from an overall 40% with peg- IFN-α + RBV alone to up 75% with the concomitant use of BOC.Citation14,Citation15,Citation51 BOC in combination with peg-IFN-α + RBV is a more effective treatment for chronic HCV genotype 1 infection than peg-IFN-α + RBV alone, for both treatment-naive patients and previous relapsers or partial responders to peg- IFN-α + RBV SOC. However, triple therapy needs closer, more detailed, and more frequent monitoring because it is more often associated with AEs, and therapy failure is associated with the selection of resistant viruses.
Patients are more likely to develop complications over a 5–10 year term (ie, liver fibrosis F3–F4) and will benefit most from the new triple therapies. Furthermore, patients with a good prognosis (ie, liver fibrosis F0–F2) might also receive only peg-IFN-α + RBV in certain situations (ie, if they carry a favorable IL28B genotype and/or respond to interferon during the first 4 weeks of therapy). Such patients may also wait for newer, more effective DAAs to be approved (ie, if there are concerns regarding the tolerability of triple therapy). In the subset of patients with a high likelihood of achieving SVR with SOC alone (ie, favorable clinical characteristics, IL28 genotype, and early viral response during SOC), the addition of a protease inhibitor may have little additional benefit in terms of SVR, but will deliver the advantage of shortened treatment duration.Citation21,Citation52 Nevertheless, patients with a significant >1 log10 reduction in HCV-RNA levels at week 4 of Peg-IFN-α + RBV lead-in (sensitivity to peg-IFN-α + RBV), have a significantly higher chance for SVR with BOC triple therapy.Citation53,Citation54
In another subset of patients, lack of sensitivity to peg-IFN-α + RBV may compromise the effectiveness of BOC.Citation14,Citation15,Citation51 After 4 weeks of peg-IFN-α + RBV lead-in, patients with <1 log10 decline in HCV RNA showed significantly reduced SVR rates, increased levels of virological failure, and resistance mutations.Citation15 The addition of BOC should be evaluated carefully in these patients, due to the risk for viral resistance in the case of treatment failure, although SVR rates with BOC triple therapy are higher in this subgroup than those obtained with peg-IFN-α + RBV alone.Citation15 Alternatively, these patients have the option of waiting for new, more effective, second-generation dual DAA-regimes. Citation52,Citation55 Exposure to BOC in previous null responders to peg-IFN-α + RBV with <1 log10 decline in HCV RNA after the lead-in phase should be avoided since without the peg-IFN-α + RBV selective pressure BOC-resistant variants are rapidly selected. Reported results with TPV in previous null-responders are limited to SVR rates of 15% in patients with <1 log10 decline during the 4-week lead-in period.Citation54
Provisional guidelines and proposals for consensus are currently underway for the use of BOC and TPV.Citation52,Citation56,Citation57 Ideally, a risk-benefit analysis should be performed for each patient to determine whether new triple therapies will be administered and to minimize the number of treated patients with low probability for achieving SVR (and selection for resistant viruses). Potential factors compromising the effectiveness of triple therapy include previous null-response to peg- IFN-α + RBV SOC, adherence, AEs, side effects, advanced fibrosis, and availability of frequent HCV-RNA monitoring during treatment. New DAA-based regimes must follow strict treatment discontinuation rules (futility rules) based on viral load measurements to avoid functional monotherapy and the emergence of viral resistance in the absence of response.Citation9,Citation10 For BOC, all drugs (BOC, peg-IFN-α, and RBV) must be stopped if HCV-RNA values are higher than or equal to 100 IU/mL at week 8 of triple therapy, or if HCV-RNA is found positive by a sensitive PCR assay at week 20 of triple therapy. In addition, if peg-IFN-α + RBV administration is discontinued, BOC administration should be stopped immediately to avoid monotherapy.Citation9,Citation10
Finally, evaluation of the efficacy of BOC and other DAAs in special settings such as in decompensated cirrhosis, liver transplantation, and patients co-infected with HIV is urgently needed, because such patients are most in need of highly effective treatment regimes.
Acknowledgments
This work was supported by the Fondo de Investigación Sanitaria, Instituto de Salud Carlos III, Spanish Ministry of Science (PS09/01707, PI10/00512 and CIBER-esp/CIBERehd), and by Generalitat Valenciana (AP-053/10). FXL holds a PI position supported by the Fondo de Investigación Sanitaria, Instituto de Salud Carlos III, Spanish Ministry of Science.
Disclosure
The authors report no conflicts of interest in this work.
References
- HeathcoteEJAntiviral therapy: chronic hepatitis CJ Viral Hepat200714Suppl 1S82S88
- KronenbergerBZeuzemSNew developments in HCV therapyJ Viral Hepat201219Suppl 1S48S51
- CuevasJMGonzález-CandelasFMoyaASanjuanREffect of ribavirin on the mutation rate and spectrum of hepatitis C virus in vivoJ Virol200983115760576419321623
- TamRCPaiBBardJRibavirin polarizes human T cell responses towards a Type 1 cytokine profileJ Hepatol199930337638210190717
- MaylinSMartinot-PeignouxMMoucariREradication of hepatitis C virus in patients successfully treated for chronic hepatitis CGastroenterology2008135382182918593587
- CardosoACMoucariRFigueiredo-MendesCImpact of peginterferon and ribavirin therapy on hepatocellular carcinoma: incidence and survival in hepatitis C patients with advanced fibrosisJ Hepatol201052565265720346533
- AsselahTEstrabaudEBiecheIHepatitis C: viral and host factors associated with non-response to pegylated interferon plus ribavirinLiver Int20103091259126920633102
- GeDFellayJThompsonAJGenetic variation in IL28B predicts hepatitis C treatment-induced viral clearanceNature2009461726239940119684573
- Boceprevir, EMA Label http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002332/WC500109789.pdfAccessed May 15, 2012
- Boceprevir, FDA Label http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/202258lbl.pdfAccessed May 15, 2012
- LiXDSunLSethRBPinedaGChenZJHepatitis C virus protease NS3/4A cleaves mitochondrial antiviral signaling protein off the mitochondria to evade innate immunityProc Natl Acad Sci U S A200510249177171772216301520
- GelmanMAGlennJSMixing the right hepatitis C inhibitor cocktailTrends Mol Med20111713446
- MalcolmBALiuRLahserFSCH 503034, a mechanism-based inhibitor of hepatitis C virus NS3 protease, suppresses polyprotein maturation and enhances the antiviral activity of alpha interferon in replicon cellsAntimicrob Agents Chemother20065031013102016495264
- BaconBRGordonSCLawitzEBoceprevir for previously treated chronic HCV genotype 1 infectionN Engl J Med2011364131207121721449784
- PoordadFMcConeJBaconBRBoceprevir for untreated chronic HCV genotype 1 infectionN England J Med2011364131195120621449783
- MangiaAMottolaLTreatment of non-genotype 1 hepatitis C virus patientsCurr Gastroenterol Rep2012141879322113745
- SchiffEPoordadEJacobsonIBoceprevir (B) combination therapy in null responders (NR): response dependent on interferon responsivenessJ Hepatol200848Suppl 2S46
- KwoPLawitzEMcConeJHCV SPRINT-1 final results: SVR from a phase 2 study of boceprevir plus pegintron (Peg-IFN alpha-2b)/RBV in treatment-naive subjects with genotype 1 chronic hepatitis CJ Hepatol200950Suppl 1S4
- BaconBRGordonSCLawitzERESPOND-2 final results: high sustained virologic response among genotype 1 previous nonresponders and relapsers to peginterferon/ribavirin when re-treated with boceprevir plus PEGINTRON (Peginterferon alfa-2b)/ribavirinHepatology201052Suppl 1S430A
- KwoPYLawitzEJMcConeJEfficacy of boceprevir, an NS3 protease inhibitor, in combination with peginterferon alfa-2b and ribavirin in treatment-naive patients with genotype 1 hepatitis C infection (SPRINT-1): an open-label, randomised, multicentre phase 2 trialLancet2010376974270571620692693
- BronowickiJMcConeJBaconBRResponse-guided therapy (RGT) with boceprevir (BOC) + peginterferon alfa-2b/ribavirin (P/R) for treatment-naïve patients with hepatitis C virus (HCV) genotype (G) 1 was Similar to a 48-Wk fixed-duration regimen with BOC + P/R in SPRINT-2Hepatology201052Suppl 1S881A
- LuLPilot-MatiasTJStewartKDMutations conferring resistance to a potent hepatitis C virus serine protease inhibitor in vitroAntimicrob Agents Chemother20044862260226615155230
- TrozziCBartholomewLCeccacciAIn vitro selection and characterization of hepatitis C virus serine protease variants resistant to an active-site peptide inhibitorJ Virol20037763669367912610142
- LinCLinKLuongYPIn vitro resistance studies of hepatitis C virus serine protease inhibitors, VX-950 and BILN 2061: structural analysis indicates different resistance mechanismsJ Biol Chem200427917175081751414766754
- MoHLuLPilot-MatiasTMutations conferring resistance to a hepatitis C virus (HCV) RNA-dependent RNA polymerase inhibitor alone or in combination with an HCV serine protease inhibitor in vitroAntimicrob Agents Chemother200549104305431416189112
- YiMTongXSkeltonAMutations conferring resistance to SCH6, a novel hepatitis C virus NS3/4A protease inhibitor: Reduced RNA replication fitness and partial rescue by second-site mutationsJ Biol Chem2005281128205821516352601
- SeiwertSHongJLimSTanHKossenKBlattL [abstract]Rev Antiviral Ther2007156
- ZhouYMuhUHanzelkaBLPhenotypic and structural analyses of hepatitis C virus NS3 protease arg155 variants: sensitivity to telaprevir (VX-950) and interferon alphaJ Biol Chem200728231226192262817556358
- SusserSForestierNWelkerMWDetection of resistant variants in the hepatitis C virus ns3 protease gene by clonal sequencing at long-term follow-up in patients treated with boceprevirJ Hepatol200950Suppl 1S12
- McHutchisonJGEversonGTGordonSCTelaprevir with peginterferon and ribavirin for chronic HCV genotype 1 infectionN Engl J Med2009360181827183819403902
- HezodeCForestierNDusheikoGTelaprevir and peginterferon with or without ribavirin for chronic HCV infectionN Engl J Med2009360181839185019403903
- SarrazinCKiefferTLBartelsDDynamic hepatitis C virus genotypic and phenotypic changes in patients treated with the protease inhibitor telaprevirGastroenterology200713251767177717484874
- DomingoEGenetic variation and quasi-speciesCurr Opin Genet Dev19922161631633428
- NájeraIHolguínAQuinones-MateuMEPol gene quasispecies of human immunodeficiency virus: mutations associated with drug resistance in virus from patients undergoing no drug therapyJ Virol199569123317983713
- SusserSWelschCWangYCharacterization of resistance to the protease inhibitor boceprevir in hepatitis C virus-infected patientsHepatology20095061709171819787809
- HalfonPLocarniniSHepatitis C virus resistance to protease inhibitorsJ Hepatol201155119220621284949
- SusserSForestierNVermehrenJDecline of detectable resistance mutations within the NS3 protease quasispecies during long-term follow-up after treatment with telaprevirJ Hepatol201052Suppl 1S300
- VermehrenJSusserSLangeCMMutations selected in the hepatitis C virus NS3 protease domain during sequential treatment with boceprevir with and without pegylated interferon alfa-2bJ Viral Hepat201219212012722239501
- VierlingJMRalstonRLawitzEJLong-term outcomes following combination treatment with boceprevir plus pegintron/ribavirin (P/R) in patients with chronic hepatitis C, genotype 1 (CHC-G1)J Hepatol201052Suppl 1S470S471
- SimmondsPGenetic diversity and evolution of hepatitis C virus – 15 years onJ Gen Virol200485113173318815483230
- CondraJHSchleifWABlahyOMIn vivo emergence of HIV-1 variants resistant to multiple protease inhibitorsNature199537465225695717700387
- López-LabradorFXMoyaAGonzález-CandelasFMapping natural polymorphisms of hepatitis C virus NS3/4A protease and antiviral resistance to inhibitors in worldwide isolatesAntivir Ther200813448149418672527
- SarrazinCZeuzemSResistance to direct antiviral agents in patients with hepatitis C virus infectionGastroenterology2010138244746220006612
- KuntzenTTimmJBericalANaturally occurring dominant resistance mutations to hepatitis C virus protease and polymerase inhibitors in treatment-naive patientsHepatology20084861769177819026009
- GaudieriSRauchAPfafferottKHepatitis C virus drug resistance and immune-driven adaptations: Relevance to new antiviral therapyHepatology20094941069108219263475
- KiefferTLSarrazinCMillerJSTelaprevir and pegylated interferon-alpha-2a inhibit wild-type and resistant genotype 1 hepatitis C virus replication in patientsHepatology200746363163917680654
- RongLDahariHRibeiroRMPerelsonASRapid emergence of protease inhibitor resistance in hepatitis C virusSci Transl Med20102303032
- McHutchisonJGMannsMPMuirAJTelaprevir for previously treated chronic HCV infectionN Engl J Med2010362141292130320375406
- KlibanovOMVickerySBOlinJLSmithLSWilliamsSHBoceprevir: a novel NS3/4 protease inhibitor for the treatment of hepatitis CPharmacotherapy201232217319022392426
- HezodeCBoceprevir and telaprevir for the treatment of chronic hepatitis C: safety management in clinical practiceLiver Int201232Suppl 1S32S38
- BaconBRKhalidOTriple therapy with boceprevir for HCV genotype 1 infection: Phase III results in relapsers and nonrespondersLiver Int201232Suppl 1S51S53
- RamachandranPFraserAAgarwalKUK consensus guidelines for the use of the protease inhibitors boceprevir and telaprevir in genotype 1 chronic hepatitis C infected patientsAliment Pharmacol and Ther201235664766222296568
- ReddyKRBrunoSRossaroLPredictors of sustained virologic response among treatment-naive patients with hepatitis C virus genotype 1 when treated with boceprevir (BOC) plus peginterferon alfa-2b/ribavirin (Pr)J Hepatol201154Suppl 1S190S190
- FosterGRZeuzemSAndreonePSubanalyses of the telaprevir lead-in arm in the realize study: response at week 4 is not a substitute for prior null response categorizationJ Hepatol201154Suppl 1S3S4
- LokASGardinerDFLawitzEPreliminary study of two antiviral agents for hepatitis C genotype 1N Engl J Med2012366321622422256805
- JacobsonIMPawlotskyJ-MAfdhalNHA practical guide for the use of boceprevir and telaprevir for the treatment of hepatitis CJ Viral Hepat201219Suppl 2S1S26
- ThomasDLBartlettJGPetersMGShermanKESulkowskiMSPhamPAProvisional guidance on the use of hepatitis C virus protease inhibitors for treatment of hepatitis C in HIV-infected personsClin Infect Dis201254797998322173234
- NairLGSannigrahiMBogenSP4 capped amides and lactams as HCV NS3 protease inhibitors with improved potency and DMPK profileBioorg Med Chem Lett20102056757020004570
- BerenguerMLópez-LabradorFXBoceprevir in the treatment of chronic hepatitis C virus infectionVirus Adaptation and Treatment20113717