Abstract
Background
Rituximab, a monoclonal antibody that selectively targets CD20-positive B-lymphocytes, is used for the treatment of patients with rheumatoid arthritis (RA) with an inadequate response or tolerance to tumor necrosis factor inhibitors. The objective of this study was to investigate the effects of rituximab treatment on the serum concentrations of vitamin D, interleukin (IL) 2, IL-6, IL-7, and IL-10 in patients with rheumatoid arthritis (RA).
Methods
Forty-five patients, aged 25–78 years, were enrolled into a cohort prospective study. All patients were treated with intravenous rituximab. Disease activity score-28 (DAS-28) and serum concentrations of rheumatoid factor (RF), C-reactive protein (CRP), anticyclic citrullinated peptide (anti-CCP), erythrocyte sedimentation rate (ESR), health assessment questionnaire (HAQ), vitamin D, ILs 2, 6, 7, and 10 were estimated in the patients before and after treatment with rituximab.
Results
DAS-28, HAQ score, and serum concentrations of CRP, RF, anti-CCP, IL-2, IL-6, IL-7, IL-10, and ESR significantly decreased after treatment. All 45 patients had vitamin D deficiency before treatment and this did not significantly change after treatment. However no significant association was found among serum vitamin D concentration and any of the ILs.
Conclusion
We concluded from this study that although rituximab treatment of patients with RA significantly reduced their disease activity and serum concentrations of IL-2, IL-6, IL-7, and IL-10, it did not significantly alter their vitamin D status. Furthermore, no significant association was found among serum vitamin D concentration and any of the ILs.
Introduction
Vitamin D, or cholecalciferol, is a steroidal hormone whose main function is the regulation of calcium homeostasis and bone formation and reabsorption.Citation1 Recently, there has been a plethora of data on the noncalcitropic effects of vitamin D deficiency, separate from its known associations with increased fracture risk.Citation2,Citation3 As an example, vitamin D has been shown to alter the expression of more than 200 genes that affect cellular functions such as proliferation, differentiation, apoptosis, and angiogenesis.Citation4 Thus vitamin D deficiency has been associated with various cancers.Citation5–Citation8
There is also a growing body of evidence that vitamin D is important in the initiation and propagation of a range of autoimmune diseases.Citation9–Citation11 This vitamin inhibits antibody secretion and autoantibody production in B cells.Citation12 It has also been reported that synovium and lymphocytes from patients with rheumatoid arthritis (RA) express vitamin D receptor. The metabolically active form of the vitamin 1, 25 dihydroxyvitamin D3 (1, 25-OHD) inhibits T-cell proliferation and prevents the release of Th-1 cytokines such as interleukin (IL)-2, interferon-γ and tumor necrosis factor (TNF)-α.Citation13
Thus, some but not all studies, have implicated low vitamin D intake as a risk factor in the development of RA. There are reports linking low vitamin D levels with increased disease activity and severity in patients with inflammatory arthritis.Citation14–Citation18 A number of studies have also demonstrated an inverse association between vitamin D and disease activity in patients with inflammatory arthritis but the results of these studies were not similar.Citation19–Citation21
Rituximab is a monoclonal antibody that selectively targets CD20-positive B lymphocytes.Citation22 It is approved for the treatment of patients with RA with an inadequate response or tolerance to TNF inhibitors. The drug has been reported to provide significant and clinically meaningful improvements in disease activity in patients with longstanding RA who had been resistant to one or more anti-TNF therapies.Citation22 Rituximab also inhibits the progression of structural damage in RA patients.Citation23 Since this drug is a B-cell depleter, its use offers an opportunity to study the relationship between vitamin D status and some cytokines. The objectives of this study were therefore (1) to study the effect of rituximab treatment on vitamin D status in patients with RA and (2) to find out if there are any significant associations among serum vitamin D concentrations and proinflammatory cytokines (IL-2, IL-6, and IL-7) and anti-inflammatory cytokines (IL-10) to justify the acclaimed link of vitamin D to cytokine production.
Patients and methods
Study patients
Consecutive patients attending the Rheumatology Outpatient Clinic of Al-Amiri Teaching Hospital, Kuwait, who fulfilled the American College of Rheumatology (formerly the American Rheumatism Association) 1987 revised criteriaCitation24 were recruited for this study.
All patients first received one course of intravenous (IV) rituximab 1000 mg and a second IV infusion of 1000 mg 2 weeks later after IV methylpredinosolone 100 mg premedication. There was a washout period of at least 3 months before giving rituximab to those who had been on TNF-α blockers. All the patients were assessed before rituximab treatment and 6 months after the second dose of rituximab. The assessment consisted of counting the number of tender and swollen joints, estimation of the erythrocyte sedimentation rate (ESR) by the Westergren method, measurement of serum concentrations of C-reactive protein (CRP) by the nephelometric method, and evaluation of disease activity by the Disease Activity for 28 Joint Indices Score (DAS-28).Citation25 Functional disability was measured by using the Arabic version of the Health Assessment Questionnaire (HAQ).Citation26 All patients gave written informed consents and the study protocol was approved by the local ethics committee.
Measurement of serum 25-OH-D concentrations
Banked serum samples collected from the patients before and after treatment with rituximab were analyzed for 25-OH-D3 using the commercially available Immunodiagnostic Systems RIA kit (Immunodiagnostic Systems Ltd, Boldon Tyne and Wear, UK). This kit is a liquid phase radioimmunoassay kit for the quantitation of 25-hydroxy vitamin D and other hydroxylated metabolites in human serum or plasma. The sensitivity of the assay in our laboratory is <3 nmol/L while the intra assay and inter assay coefficient of variations were 5.0 and 8.1%, respectively. Insufficiency of 25-OH-D was defined as <70 nmol/L (<30 ng/mL) and deficiency as <50 nmol/L (<20 ng/mL). The normal range in our laboratory is 70–100 nmol/L.
Measurement of serum IL-2, IL-6, IL-7, and IL-10 concentrations
The serum concentrations of these ILs in patients with RA before and after treatment with rituximab were estimated by using commercially available ELISA kits from IMMUNOTECH SAS (Marsielle, France). The instructions of the manufacturer of the kits were followed.
Statistical analysis
Data were analyzed using the Statistical Package for Social Sciences Software ([SPSS] v17.0; SPSS Inc, Chicago, IL). The variables were examined for normality with the Kolmogorov-Smirnov test, and descriptive statistics presented as appropriate. The differences between pretreatment and post-treatment values were compared using nonparametric Mann–Whitney or Kruskal–Wallis tests. Vitamin D concentrations were tested for any relationship with IL concentrations using Spearman correlation coefficient. The two-tailed probability P < 0.05 was considered statistically significant.
Results
Demographic characteristics
A total of 45 patients with active RA were enrolled into the study. Of these, 34 (75.6%) were females and 11 (24.4%) were males (). The mean age of the patients was 48.9 ± 1.78 years with a range of 25–78 years. The mean age at disease onset was 36.6 ± 11.4 years ranging from 14–70 years. The median RA duration was 10 years ranging from 6 months to 28 years. None of the patients had any significant dietary change that might affect vitamin D intake during the study. None of the patients had abnormal liver or renal functions that might affect the serum vitamin D concentrations.
Table 1 Demographic and clinical characteristics of patients with active RA before treatment with rituximab
Clinical and laboratory parameters
shows a significant decrease in DAS-28, HAQ, serum concentrations of RF, CRP, anti-CCP, and ESR following treatment of RA patients with rituximab, suggesting that the drug was effective in reducing the inflammation of RA.
Table 2 Clinical and laboratory parameters in patients with RA before and after treatment with rituximab
Serum concentrations of vitamin D, IL-2, IL-6, IL-7, and IL-10
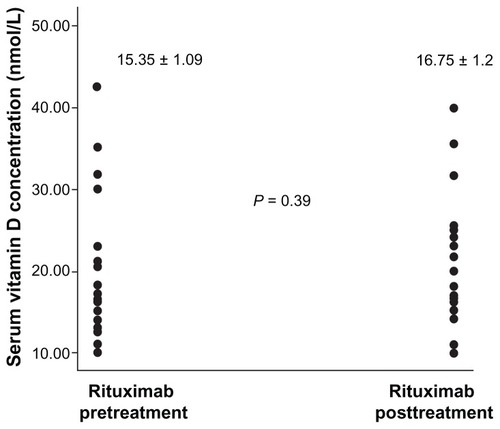
is a scatter plot showing the distribution of serum vitamin D concentrations in patients with RA before and after treatment with rituximab. All patients, before and after treatment, had serum vitamin D concentrations of less than 50 nmol/L, the deficiency value in our laboratory. We did not include controls in this study because our aim was not to compare the prevalences of vitamin D deficiencies between patients with RA and the healthy population but to demonstrate the effect of rituximab treatment on vitamin D status. also shows that rituximab treatment did not significantly alter the status of vitamin D in patients with RA.
Figure 1 Scatter plot of vitamin D in patients with rheumatoid arthritis before and after treatment with rituximab.
shows that the mean serum concentrations of IL-2, IL-6, IL-7, and IL-10 significantly fell in patients with RA following treatment with rituximab. For example, serum IL-2 concentration fell from 52.56 ± 6.29 pg/mL before treatment to 8.77 ± 1.81 pg/mL after treatment while IL-7 fell from 146.63 ± 9.23 pg/mL before treatment to 68.71 ± 11.63 pg/mL after treatment.
Table 3 Serum concentrations of vitamin D, IL-2, IL-6, IL-7, and IL-10 in patients with RA before and after treatment with rituximab
Association among serum vitamin D concentration and serum ILs before and after treatment with rituximab
shows that there were no significant associations among serum vitamin D concentration and serum IL-2, IL-6, IL-7, and IL-10 in patients with RA before and after treatment with rituximab.
Table 4 Association among serum vitamin D concentration and serum ILs in patients with RA before treatment with rituximab
Discussion
Although our objectives in this study did not include the investigation of the prevalence of vitamin D deficiency in patients with RA (and this was why we did not include any healthy controls), it is important to note that all 45 patients with RA had vitamin D deficiency before treatment. This finding is in accord with the almost pandemic vitamin D hypovitaminosis reported all over the world in generalCitation26,Citation27 and in patients with RA in particular.Citation28–Citation30
The second important result from this study was that treatment of RA patients with rituximab did not alter their vitamin D status. To the best of our knowledge, this is the first report of the effect of rituximab treatment on serum vitamin D concentrations in patients with RA. It was surprising that rituximab did not affect vitamin D status since vitamin D has been reported to inhibit antibody secretion and T cell proliferation.Citation12,Citation13 Rituximab is known to deplete B cells that produce antibodies. Therefore one would have expected that rituximab treatment would cause a significant reduction in serum vitamin D concentration. Why this was not so is not clear but further investigations on the relationship between vitamin D, antibody production by B cells, and cytokine serum concentrations need to be carried out on a large population.
The third important result of this study was that rituximab treatment of patients with RA significantly reduced their disease activity and their serum concentrations of RF, CRP, anti-CCP, and ESR. In this study, we found significant reductions in the serum concentrations of proinflammatory interleukins such as IL-2, IL-6, and IL-7. The reduction in disease activity in RA after treatment with rituximab might be due to the reductions in these proinflammatory ILs. It was surprising to find that treatment with rituximab in patients with RA also reduced their serum concentrations of IL-10, an anti-inflammatory IL. This might be due to the fact that rituximab depletes all B lymphocytes. The long term effect of this reduction in patients treated with rituximab is not known.
Perhaps the most important finding in this study was that the serum concentration of vitamin D was not significantly associated with serum concentration of either IL-2, IL-6, IL-7, or IL-10. These findings contradict the reports that vitamin D downregulates the production of several cytokines such as IL-2, IL-6, IL-12, interferon-γ, TNF-α, and TNF-β in in vitro studies.Citation31,Citation32 Our results, however, were in agreement with those of Vilarrasa et alCitation33 who recently reported that no significant associations were found amongst 25-OHD and plasma concentrations of IL-18 and other cytokines. Further studies on larger sample sizes of healthy populations are needed to investigate the associations among serum vitamin D and IL concentrations.
Conclusion
We discovered from our study that treatment of RA patients with rituximab did not significantly alter their already depleted vitamin D status, although it significantly reduced their indices of inflammation and their serum concentrations of IL-2, IL-6, IL-7, and IL-10.
Disclosure
The authors report no conflicts of interest in this work.
References
- ArnsonYAmitalHShoenfeldYVitamin D and autoimmunity: new aetiological and therapeutic considerationsAnn Rheum Dis2007661137114217557889
- LookerACPfeifferCMLacherDASchleicherRLPiccianoMFYetleyEASerum 25-hydroxyvitamin D status of the US population: 1988–1994 compared with 2000–2004Am J Clin Nutr2008881519152719064511
- CherniackEPLevisSTroenBRHypovitaminosis D: a widespread epidemicGeriatrics200863243018376898
- CutoloMVitamin D and autoimmune rheumatic diseasesRheumatology20094821021218930963
- KrishnanAVTrumpDLJohnsonCSFeldmanDThe role of vitamin D in cancer prevention and treatmentEndocrinol Metab Clin North Am20103940141820511060
- AndersonLNCotterchioMViethRKnightJAVitamin D and calcium intakes and breast cancer risk in pre- and postmenopausal womenAm J Clin Nutr2010911699170720392891
- KarlssonSOlaussonJLundhDVitamin D and prostate cancer: the role of membrane initiated signaling pathways in prostate cancer progressionJ Steroid Biochem Mol Biol201012141341620398754
- TseAKZhuGYWanCKShenXLYuZLFongWF1alpha, 25-Dihydroxyvitamin D3 inhibits transcriptional potential of nuclear factor kappa B in breast cancer cellsMol Immunol2010471728173820371119
- HolickMFHigh prevalence of vitamin D inadequacy and implications for healthMayo Clin Proc20068135337316529140
- CutoloMOtsaKPalinoSYprusMVeldiTSerioloBVitamin D involvement in rheumatoid arthritis and systemic lupus erthymatosusAnn Rheum Dis20096744644719213751
- Pérez-LópezFRVitamin D and its implications for musculoskeletal health in women: an updateMaturitas20075811713717604580
- RitterhouseLLCroweSRNiewoldTBVitamin D deficiency is associated with an increased autoimmune response in healthy individuals and in patients with systemic lupus erthematosusAnn Rheum Dis2011701569157421586442
- RanganathanPGenetics of bone loss in rheumatoid arthritis – role of vitamin D receptor polymorphismsRheumatology200948434234619151030
- LiaoKPAlfredssonLKarlsonEWEnvironmental influences on risk for rheumatoid arthritisCurr Opin Rheumatol200921327928319318947
- NielenMMvan SchaardenburgDLemsWFVitamin D deficiency does not increase the risk of rheumatoid arthritisArthritis Rheum2006543719372017075887
- CostenbaderKHFeskanichDHolmesMKarlsonEWBenito-GarciaEVitamin D intake and risks of systemic lupus erythematosus and arthritis in womenAnn Rheum Dis20086753053517666449
- MerlinoLACurtisJMikulsTRCerhanJRCriswellLASaagKGVitamin D intake is inversely associated with rheumatoid arthritis: results from the Iowa Women’s Health StudyArthritis Rheum200450727714730601
- PatelSFarragherTBerryJBunnDSilmanASymmonsDAssociation between serum vitamin D metabolite levels and disease activity in patients with early inflammatory polyarthritisArthritis Rheum2007562143214917599737
- TurhanoğluADGülerHYöndenZAslanFMansurogluAOzerCThe relationship between vitamin D and disease activity and functional health status in rheumatoid arthritisRheumatol Int20103191191420300755
- CraigSMYuFCurtisJRVitamin D status and its associations with disease activity and severity in African Americans with recent-onset rheumatoid arthritisJ Rheumatol20103727528120032100
- Braun-MoscoviciYToledanoKMarkovitsDRozinANahirAMBalbir-GurmanAVitamin D level: is it related to disease activity in inflammatory joint disease?Rheumatol Int20113149349920033415
- CohenSBEmeryPGreenwaldMWRituximab for rheumatoid arthritis refractory to anti-tumor necrosis factor therapy: Results of a multicenter, randomized, double-blind, placebo-controlled, phase III trial evaluating primary efficacy and safety at twenty-four weeksArthritis Rheum2006542793280616947627
- KeystoneEEmeryPPeterfyCGRituximab inhibits structural joint damage in patients with rheumatoid arthritis with an inadequate response to tumour necrosis factor inhibitor therapiesAnn Rheum Dis20096821622118388156
- ArnettFCEdworthySMBlochDAThe American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritisArthritis Rheum1988313153243358796
- PrevooMLvan ‘t HofMAKuperHHvan LeeuwenMAvan de PutteLBvan RielPLModified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritisArthritis Rheum19953844487818570
- ShehabDAl-JarallahKMoussaMAValidation of the Arabic version of the Health Assessment Questionnaire (HAQ) in patients with rheumatoid arthritisRev Rhum Engl Ed1998653873929670330
- Gannagé-YaredMHTohméAHalabyGHypovitaminosis D: a major worldwide public health problemPresse Med20013065365811346909
- AdamsJSHewisonMUpdate in vitamin DJ Clin Endocrinol Metab20109547147820133466
- ZoldESzodorayPGaalJVitamin D deficiency in undifferentiated connective tissue diseaseArthritis Res Ther200810R12318928561
- DamanhouriLHVitamin D deficiency in Saudi patients with systemic lupus erythematosusSaudi Med J2009301291129519838436
- MauricioDMandrup-PoulsenTNerupJVitamin D analogues in insulin-dependent diabetes mellitus and other autoimmune diseases: a therapeutic perspectiveDiabetes Metab Rev19961257688861501
- LemireJMJ Immunomodulatory actions of 1, 25-dihydroxyvitamin D3Steroid Biochem Mol Biol199553599602
- VilarrasaNVendrellJMaravallJIs plasma 25(OH) D related to adipokines, inflammatory cytokines and insulin résistance in both a healthy and morbidly obese population?Endocrinology201038235242