Abstract
Molecular profiling studies have found that estrogen receptor-positive (ER+) human breast cancers are comprised of at least two distinct diseases with differing biologies. With the advent of DNA microarrays, global gene expression patterns were used to define the luminal A and luminal B subtypes of ER+ breast cancer, with luminal B cancers showing a more aggressive phenotype including substantially worse outcomes in patients. The luminal B subtype designation could be considered a surrogate for those ER+ tumors having low progesterone receptors, high proliferation, high grade, and predicted poor response to hormone therapy. While they express estrogen receptors, luminal B cancers do not show a corresponding expression of estrogen-regulated genes, and may therefore rely upon alternative pathways for growth. At the molecular level, luminal B cancers appear dramatically distinct from luminal A cancers, at the levels of gene expression, gene copy, somatic mutation, and DNA methylation; luminal B cancers are also genetically and genomically altered to a greater extent than luminal A cancers. While, in the clinical setting, luminal B is typically regarded as an ER+, hormone-sensitive disease, more research is needed into how to better treat it. Comprehensive profiling initiatives, such as The Cancer Genome Atlas, have recently provided us a catalog of mutated or copy altered genes, from which new therapeutic targets could potentially be mined. Candidate pathways that might be targeted in luminal B include those involving growth factor receptors, including HER2 and EGFR, as well as PI3K/Akt/mTor.
Introduction
Breast cancer encompasses a number of different diseases. In the clinical setting, breast cancers by convention are subdivided according to estrogen receptor (ER) and HER2 status; ER-positive (ER+) tumors typically respond to hormone therapy, while HER2+ tumors respond to anti-HER2 therapy, and no targeted therapy is currently in widespread use for ER−/HER− tumors. Progesterone receptor (PR) is another molecular marker that may be used in the clinic, as loss of PR in ER+ tumors is thought to be predictive for lack of response to hormone therapy.Citation1 Over a decade ago, gene expression profiling (at the mRNA level) uncovered distinct molecular subtypes of breast cancer, each defined by a large number of genes.Citation2–Citation4 These subtypes – which include basal-like, HER2-enriched, normal-like, luminal A, and luminal B – largely reflect the established clinical- and histological-based classifications, with basal-like representing ER−/HER2− cancers, HER2-enriched representing ER−/HER2+, and normal-like and luminal A/B subtypes representing ER+. One notable finding from the gene expression studies was that luminal B cancers showed worse outcomes as compared to luminal A cancers,Citation2 which indicated that ER+ breast cancer itself may be made up of at least two distinct diseases with differing biology.
The luminal B subtype, understood to be the more aggressive form of ER+ breast cancer, is the subject of this review. Here we will broadly describe luminal B breast cancer in terms of its molecular profile, making use of public datasets including those from The Cancer Genome Atlas (TCGA).Citation5–Citation7 The premise put forth here is that luminal B cancers represent a unique subtype of breast cancer, with a distinctive biology from that of luminal A cancers, rather than simply representing a more advanced or aggressive form of luminal A.
Pathophysiology of luminal B breast cancer
Though the designation of luminal B first came about with the early gene expression profiling studies of breast cancer near the start of the millennium, it has long been understood that there exists a more aggressive form of ER+ breast cancer. Earlier studies had noted that ∼30% of ER+ invasive breast cancers showed no benefit from hormone therapy, suggesting that these cancers either augment or entirely bypass the classical estrogen-stimulated mitogenic pathway.Citation8 Markers predicting hormone therapy response within ER+ cancers have been sought, the most notable of these being PR. Loss of PR expression is thought to represent a surrogate for a more aggressive disease phenotype that is less dependent upon estrogen signaling; in correlative studies, PR loss has been associated with lower ER levels, more positive nodes, aneuploidy, larger tumor size, higher proliferation, and expression of growth factor receptors (GFRs) including EGFR and HER2.Citation1
The advent of DNA microarrays made it possible to profile breast cancers for mRNA expression of thousands of genes. Early profiling studies took a fresh approach to classifying breast cancer, allowing the expression data themselves to segregate human breast tumors, rather than relying on prior biological knowledge and possible biases. Expression profiling first defined five intrinsic molecular subtypes of breast cancer: basal-like, HER2-enriched, normal-like, luminal A, and luminal B. A sixth subtype, claudin-low, was discovered later, perhaps due to its greater rarity.Citation9,Citation10 Other additional ER− subtypes could include a “molecular apocrine” subtype (ER−/HER2+ but with activation of androgen receptor signaling), and an “interferon” subtype (with high expression of interferon regulated-genes).Citation11 Recently, there have been some suggestionsCitation12,Citation13 that the normal-like breast cancer might be a mere artifact of sample representation (ie, disproportionately high content of normal tissue contamination), though such concerns would not extend to the other subtypes, including luminal B.
As noted above, the mRNA-based classifications, as originally defined by Perou and colleagues, largely reflected the histological-based classifications. The luminal and normal-like subtypes reflect the ER+ form of breast cancer. The designation of luminal was derived due to the finding that these cancers show mRNA and protein expression of keratins 8/18,Citation3 typically associated with luminal epithelial cells (as opposed to basal cells which express keratins 5/6). The luminal subtype of breast cancer was further subdivided into A and B groups, as luminal B showed widespread expression differences as well as substantially worse outcomes.Citation2 In the future, as larger cohorts of breast tumors are profiled at multiple data levels, the molecular designations of breast cancer may be further refined.
While the intrinsic molecular subtypes of breast cancer have been defined and examined on the basis of hundreds of genes,Citation2,Citation3,Citation9,Citation14 in the interests of a more focused gene list for the purposes of a clinical assay, the PAM50 assay was developed, which consists of 50 genes by which breast cancers can be classified by mRNA-based subtype.Citation13,Citation15,Citation16 illustrates the patterns of the PAM50 genes, both in an expression profile dataset (N = 240) from the research group which first developed the assay,Citation14 and in a compendium of nine separate datasetsCitation17–Citation25 profiled on the same assay platform (N = 1340, previously collected by Kessler et al).Citation26 It is notable how the PAM50 gene patterns are remarkably consistent between the two datasets. It is also evident that luminal B shares some gene patterns with luminal A (eg, ER genes ESR1, FOXA1, and BCL2) and some patterns with basal-like including expression of proliferation markers (eg, Ki-67 gene MKI67, survivin gene BIRC5, and cyclin B1 gene). It has been put forth that luminal B might represent the ER+/HER2+ form of breast cancer;Citation4 however, in our compendium dataset, HER2 gene ERBB2 does not show high levels in luminal B ().
Figure 1 Luminal B breast cancer is associated with substantially worse patient outcomes. (A) Expression patterns of the PAM50 gene setCitation13 (41 genes represented on the U133A array platform) in the mRNA profile datasets from Hoadley et al,Citation14 (N = 247) and Kessler et al.Citation26 U133A compendium (N = 1340, representing nine separate studies). Using the PAM50 genes and the Hoadley subtype assignments, inter-profile correlations between the Hoadley and Kessler datasets were used to assign mRNA-based subtypes (basal-like, HER2-enriched, normal-like, luminal A, luminal B) to the Kessler profiles. (B) Kaplan–Meier plot of distant metastasis-free survivals for the mRNA-based subtypes. Survival capped at 20 years.
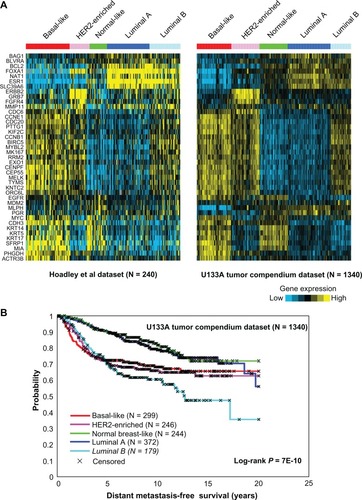
Within the compendium dataset,Citation26 as reported elsewhere, luminal B cancers have much worse outcomes compared to luminal A, the outcomes of luminal B being comparable to, if not worse than that of the basal-like and HER2-enriched subtypes (). Between different patient cohorts, the relative outcomes of the intrinsic mRNA-based subtypes may vary; for example, the HER2-enriched subtype may have a better outcome in patients treated with anti-HER2 therapy,Citation27,Citation28 and in at least one early study using a small cohort, normal-like breast cancers actually showed a worse outcome comparable to that of luminal B.Citation2 However, luminal B has been found to consistently show poor outcomes in studies using sizable datasets, including patients receiving antiestrogen therapy (such as the Loi et al dataset,Citation21 which is represented in our compendium).
Diagnosis of luminal B breast cancer
Assays for diagnosing luminal B breast cancer in the clinic are currently available, though it will likely take some time for these assays to become routine, as new clinical practices are often gradually adopted. PR is one marker that is frequently measured in the clinic along with ER, in order to further subdivide ER+ breast cancers by prognosis or anticipated therapeutic response,Citation1,Citation28–Citation31 though the association of PR with hormone response has not been observed everywhere,Citation32,Citation33 which may be an indicator of a single biomarker having insufficient information as compared to a biomarker panel. Clinical variables such as grade or Ki-67 can help distinguish the subset of ER+ breast tumors with expected worse outcomes.Citation34 The PAM50 assay,Citation13,Citation15,Citation16 which classifies breast cancer by mRNA-based subtype, is compatible with formalin-fixed, paraffin-embedded-derived RNA, which facilitates its use in the clinic; the assay is currently being developed for clinical use on the NanoString nCounter™ Analysis System (Nanostring Technologies, Seattle, WA) and is also offered as a laboratory-developed test, using a qualitative reverse-transcription polymerase chain reaction format from ARUP Laboratories (Salt Lake City, UT).Citation15
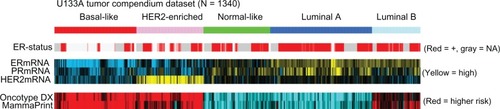
While numerous prognostic gene signatures of breast cancer have been developed using expression profiling, it is understood that the different signatures by and large work by differentiating luminal A breast cancers from all other subtypes including luminal B.Citation15,Citation35 In addition to PAM50, other gene assays for predicting the outcome of ER+ breast cancer include Oncotype DX (Genomic Health, Redwood City, CA) and MammaPrint (Agendia, Amsterdam, The Netherlands). Oncotype DX, based on 16 cancer-related genes,Citation36 is perhaps the most widely used clinical gene-expression assay in the USA,Citation15 while MammaPrint is based on 70 genes.Citation37 Similar to what has been observed elsewhere using other datasets,Citation35,Citation38,Citation39 in the Kessler U133A compendium breast tumor dataset, luminal B tumors have lower PR mRNA levels and predicted worse outcomes according to either Oncotype DX or MammaPrint signatures (). Therefore, there are a number of ways the luminal B or poor prognostic subset of ER+ breast cancer may be defined in the clinical setting. While the various assays may rely on different prognostic gene sets, the genes all appear to point to an overall biological phenomenon, likely involving hundreds if not thousands of genes, of which a handful may be represented in a given assay.
Figure 2 The luminal B subtype represents both ER+ breast cancer with low PR levels and ER+ breast cancer with predicted worse outcome.
Abbreviations: ER+ estrogen receptor-positive; PR, progesterone receptor; ER, estrogen receptor.
Current and emerging novel targets and therapies
As luminal B breast cancer expresses ER, the estrogen pathway is regarded as a therapeutic target for this disease, though the case could readily be made that additional targets are needed. According to 2011 St Gallen consensus recommendations, where luminal B could be defined in the clinical setting as ER+/HER2−/Ki67+, standard treatment would include endocrine therapy with or without cytotoxic therapy.Citation15,Citation40 However, a large percentage of ER+ breast cancers, which may be regarded as representing luminal B, do not respond to endocrine therapy.Citation8,Citation41 Where PR (under-expressed in luminal B) has long been studied as a marker of functional ER, therapeutic targets for ER+/PR− disease have been considered.Citation1 Studies suggest that estrogen-independent disease represents a switch from using the estrogen pathway to using an alternative GFR signaling pathway; such candidates including HER2, EGFR, IGF, and Akt/PI3K/mTOR.Citation42–Citation46
Molecular profiling is one means of identifying novel therapeutic candidates for diseases such as luminal B breast cancer, and to this end, the TCGA initiative is currently engaged in profiling human cancers at multiple levels of molecular complexity, including mRNA, protein (by RPPA assay), microRNA, gene promoter methylation, DNA copy, and somatic mutation.Citation5–Citation7 TCGA recently completed a study of breast cancer,Citation7 which provided a great deal of insight into the molecular profile of luminal B as well as the other intrinsic subtypes. In this review, we will discuss findings of the TCGA study particularly relevant to luminal B (as all TCGA tumors were subtyped according to their mRNA profile), providing some views of the associated data as well, which are all public.Citation7,Citation47
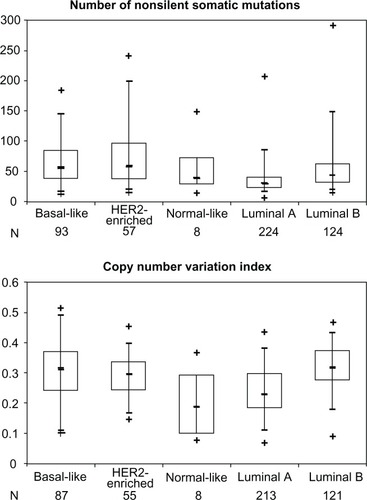
The TCGA study results further demonstrated that luminal B appears quite distinct from luminal A at the molecular level, reinforcing the notion that the two subtypes represent different diseases. For one thing, as the mRNA-based subtypes were originally defined in an unsupervised fashion, allowing the mRNA profile data to group tumors, the same exercise was also carried out to define subtypes at each level of microRNA, methylation, and protein; the mRNA-based subtypes were found to be reflected in the other molecular data types,Citation7 and those results are represented here in a different format () to highlight the finding that the mRNA-based luminal B subtype overlaps highly with specific subtypes at the methylation and protein levels (though interestingly not at the microRNA level), showing patterns distinct from those of luminal A. Furthermore, luminal B cancers were somatically mutated and copy altered to a significantly greater extent than luminal A cancers, at levels comparable to what was observable in basal-like and HER2-enriched cancers (), consistent with previous findings.Citation17,Citation39
Figure 3 The (mRNA-based) luminal B breast cancer subtype is reflected in alternative classifications of breast cancer, based on molecular profiling at levels of microRNA, methylation, and protein.
Abbreviations: TCGA, The Cancer Genome Atlas; RPPA, reverse-phase protein array.
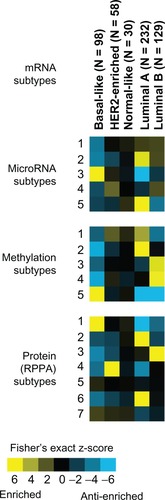
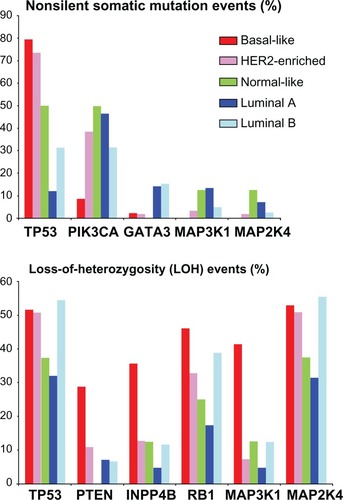
Figure 4 Luminal B cancers are genetically and genomically altered to a greater extent than luminal A cancers (and comparable to the ER− subtypes).
Abbreviations: ER−, estrogen receptor-negative; TCGA, The Cancer Genome Atlas; LOH, loss of heterozygosity.
The TCGA study has yielded a catalog of genes that are genetically or genomically altered in luminal B cancers, and many of these aberrations could have essential roles in the disease phenotype; the nontrivial challenge, however, would be in our being able to distinguish the driving alterations from those that are simply passengers. In terms of the mutation landscape, PIK3CA and TP53 are the most frequent somatic targets in breast cancer, as well as in the luminal B subset (). Numerous other genes appear recurrently mutated at a much lower frequency, and many of these could be found to have important roles in at least a subset of luminal B cancers. In terms of the copy landscape, there is a very large number of genes amplified or deleted in luminal B, the complete list being too large to enumerate here (but available in the TCGA report).Citation7 Copy loss events that show differential patterns among the subtypes include those involving TP53, PTEN, INPP4B, RB1, MAP3K1, and MAP2K4 ().
Figure 5 Luminal B cancers have distinct patterns of alterations in genes impacting key pathways including p53, PI3K, Rb, and MAP kinase.
Abbreviations: LOH, loss of heterozygosity; TCGA, The Cancer Genome Atlas.
The origin of luminal B breast cancer
Observations and unanswered questions as to the origin of luminal B breast cancers may follow a similar line of reasoning regarding the origin of ER− breast cancer.Citation8 Luminal B cancers, though ER+, are resistant to hormone therapy and have a distinct molecular phenotype from hormone-sensitive luminal A cancers, with luminal B sharing many molecular features with ER− cancer subtypes ( and ). One important question is whether luminal B cancer/cancer precursors evolve from luminal A cancer/cancer precursors, or have a path of initiation and progression that is completely distinct from luminal A; these two alternate hypotheses are represented graphically in , though these are only conceptual, and the truth may well lie somewhere in between the two.
Figure 6 Two different models to explain the possible origin of the breast cancer subtypes (including luminal B). (A) “Linear evolution” model, whereby cancer cells or cancer precursor cells gradually evolve (by accumulation of genomic alterations) from a luminal A or normal-like subtype (with ER/PR expression), to a luminal B subtype (with loss of PR and possible gain of growth factor receptor, or GFR signaling), to either a HER2-enriched or Basal-like subtype (with complete loss of ER signaling and increase of GFR signaling). (B) “Distinct pathways of progression” model, whereby each breast cancer subtype follows a path of initiation and progression that is independent of that of the other subtypes.
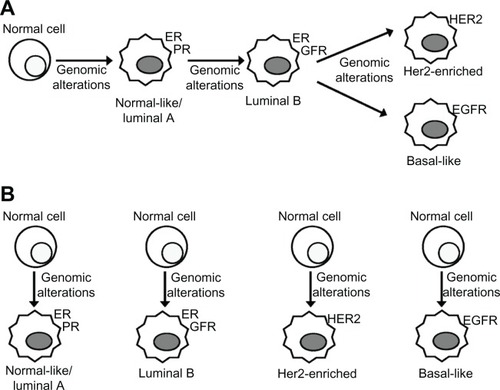
Some observations may suggest that luminal B and other hormone resistant breast cancer subtypes evolve from luminal A cancer or a precursor to luminal A. For example, ER− breast cancers (and by implication luminal B) are believed to evolve from ER+ precursors or cells.Citation8 Estrogen dynamically regulates several factors and is regulated by others, and loss of ER function and increase of GFR may well occur during the progression of breast cancer to a hormone-resistant state.Citation1 Cell line models of ER+, hormone-sensitive (ie, luminal A-like) cancers can be manipulated experimentally into switching to use of alternative GFR signaling pathways, often resulting in downregulation of ER or PR or both,Citation38,Citation48,Citation49 and conversely some ER− cancers can be made to express ER and become hormone-sensitive;Citation50 this would suggest that many breast cancers at least are not genetically hard-wired for dependence upon a single pathway, but may evolve from one pathway to another. Additionally, we see that, compared to luminal A, luminal B cancers have significantly greater numbers of mutations and copy number alterations (), consistent with the idea of a cancer cell acquiring alterations in the path from a luminal A to a luminal B state.
Alternatively, other observations can suggest that luminal B and the other breast cancer subtypes develop and evolve independently of each other. The decision for a cell to be hormone-independent versus hormone-dependent likely happens early on, before the transition to an invasive breast cancer cell; breast cancers are understood to evolve in a non-obligatory fashion through an increasingly abnormal series of hyperplasias, atypical hyperplasias, and noninvasive or in situ carcinomas, with the earlier precursor cells being nearly all ER+ and the later (pre-invasive) precursor cells having a much greater proportion of ER− cells.Citation8 Furthermore, when examining gene expression profiles of primary tumors and distant metastases from the same patients, one study found that the subtype associations were preserved throughout the metastatic process of breast cancer.Citation51
At the molecular level, the various subtypes appear quite distinct from each other, making it difficult to trace a clear path of genomic alterations leading from one subtype to another. For example, while luminal B may appear genomically altered to a similar extent to that of basal-like (), the copy profile of basal-like dramatically differs from that of any of the other subtypes, with basal-like sharing extensive copy and transcriptional similarities with serous ovarian cancers.Citation7 DNA methylation profilingCitation7 associates specific patterns of epigenetic hardwiring with luminal B cancers, which appear quite distinct to that associated with luminal A or basal-like cancers (). When individual genes are considered, we find for example, that somatic mutations in PIK3CA are most frequent in luminal A cancers (46%), less frequent in luminal B (31%), and least frequent in basal-like cancers (9%, ); this would seem counter to the notion of luminal B or basal-like cancers having originally started from a luminal A genetic profile. Similarly, other studies, such as ones comparing molecular features of high-grade (eg, luminal B or basal-like) versus low-grade breast cancers, have concluded that a clear path of progression between the two would be difficult to define.Citation52
Clinical potential and future research
At present, luminal B breast cancer is routinely treated as an ER+, hormone-sensitive disease.Citation15,Citation40 While often considered as simply a more aggressive form of the ER+ subtype, luminal B might be considered more in the future as a type of breast cancer that is entirely distinct in many ways from luminal A. While triple-negative (ER−/PR−/HER2−) breast cancer is of particular interest to the research community, owing to there being as yet no systematic targeted therapy for this disease, the same level of effort might be directed as well towards identifying new therapies for luminal B cancers. As luminal B cancers appear to rely less on the estrogen pathway, recent clinical trial studies have considered targeting alternate pathways in advanced stage ER+ cancer, include EGFR (eg, using the drug gefitinib)Citation42 and PI3K/Akt/mTOR (eg, using everolimus).Citation43 The recent BOLERO-2 clinical trial results showed progression-free survival in patients with hormone refractory ER+ disease being substantially prolonged by mTOR inhibitor everolimus.Citation43 While results such as these are encouraging, more study is needed to assess the efficacy of such drugs in the adjuvant setting.
Conclusion and future perspective
Over the years, comprehensive molecular profiling of breast cancer has deepened our understanding of luminal B breast cancer as a unique disease, distinct from either luminal A or ER− cancers. The recent TCGA study and others have provided an extensive catalog of the genetic and genomic aberrations associated with luminal B, and the nontrivial task remains of distinguishing those aberrations that are simply correlative from those that have a driving role in the disease phenotype. Better therapeutic approaches and targets are needed for a large subset of ER+ tumors that might initially have been deemed treatable, and the molecular profile of luminal B may well provide additional clues needed to tackle this important challenge.
Acknowledgements
The author is supported in part by NIH/NCI grants P30 CA125123, P50 CA58183-16, and U24CA143843.
Disclosure
The author reports no conflicts of interest in this work.
References
- CuiXSchiffRArpinoGOsborneCKLeeAVBiology of progesterone receptor loss in breast cancer and its implications for endocrine therapyJ Clin Oncol200523307721773516234531
- SørlieTPerouCMTibshiraniRGene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implicationsProc Natl Acad Sci U S A20019819108691087411553815
- PerouCMSørlieTEisenMBMolecular portraits of human breast tumoursNature2000406679774775210963602
- PratAPerouCDeconstructing the molecular portraits of breast cancerMol Oncol20115152321147047
- Cancer Genome Atlas Research NetworkComprehensive genomic characterization defines human glioblastoma genes and core pathwaysNature200845572161061106818772890
- Cancer Genome Atlas Research NetworkIntegrated genomic analyses of ovarian carcinomaNature2011474735360961521720365
- Cancer Genome Atlas Research Network. Comprehensive molecular portraits of human breast tumorsNature2012
- AllredDCBrownPMedinaDThe origins of estrogen receptor alpha-positive and estrogen receptor alpha-negative human breast cancerBreast Cancer Res20046624024515535853
- HerschkowitzJISiminKWeigmanVJIdentification of conserved gene expression features between murine mammary carcinoma models and human breast tumorsGenome Biol200785R7617493263
- CreightonCJLiXLandisMResidual breast cancers after conventional therapy display mesenchymal as well as tumor-initiating featuresProc Natl Acad Sci U S A200910633138201382519666588
- FarmerPBonnefoiHBecetteVIdentification of molecular apocrine breast tumours by microarray analysisOncogene200524294660467115897907
- PeppercornJPerouCMCareyLAMolecular subtypes in breast cancer evaluation and management: divide and conquerCancer Invest200826111018181038
- ParkerJSMullinsMCheangMCSupervised risk predictor of breast cancer based on intrinsic subtypesJ Clin Oncol20092781160116719204204
- HoadleyKAWeigmanVJFanCEGFR associated expression profiles vary with breast tumor subtypeBMC Genomics2007825817663798
- PratAEllisMJPerouCMPractical implications of gene-expression-based assays for breast oncologistsNat Rev Clin Oncol201191485722143140
- NielsenTOParkerJSLeungSA comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor-positive breast cancerClin Cancer Res201016215222523220837693
- ChinKDeVriesSFridlyandJGenomic and transcriptional aberrations linked to breast cancer pathophysiologiesCancer Cell200610652954117157792
- MillerLDSmedsJGeorgeJAn expression signature for p53 status in human breast cancer predicts mutation status, transcriptional effects, and patient survivalProc Natl Acad Sci U S A200510238135501355516141321
- DesmedtCPietteFLoiSStrong time dependence of the 76-gene prognostic signature for node-negative breast cancer patients in the TRANSBIG multicenter independent validation seriesClin Cancer Res200713113207321417545524
- WangYKlijnJGZhangYGene-expression profiles to predict distant metastasis of lymph-node-negative primary breast cancerLancet2005365946067167915721472
- LoiSHaibe-KainsBDesmedtCDefinition of clinically distinct molecular subtypes in estrogen receptor-positive breast carcinomas through genomic gradeJ Clin Oncol200725101239124617401012
- SchmidtMBBöhmDvon TörneCThe humoral immune system has a key prognostic impact in node-negative breast cancerCancer Res200868135405541318593943
- ZhangYSieuwertsAMMcGreevyMThe 76-gene signature defines high-risk patients that benefit from adjuvant tamoxifen therapyBreast Cancer Res Treat2009116230330918821012
- MinnAJGuptaGPSiegelPMGenes that mediate breast cancer metastasis to lungNature2005436705051852416049480
- MinnAJGuptaGPPaduaDLung metastasis genes couple breast tumor size and metastatic spreadProc Natl Acad Sci U S A2007104166740674517420468
- KesslerJDKahleKTSunTA SUMOylation-dependent transcriptional subprogram is required for Myc-driven tumorigenesisScience2012335606634835322157079
- BaselgaJTreatment of HER2-overexpressing breast cancerAnn Oncol201021Suppl 7vii36vii4020943641
- OldenhuisCNOostingSFGietemaJAde VriesEGPrognostic versus predictive value of biomarkers in oncologyEur J Cancer200844794695318396036
- BardouVJArpinoGElledgeRMOsborneCKClarkGMProgesterone receptor status significantly improves outcome prediction over estrogen receptor status alone for adjuvant endocrine therapy in two large breast cancer databasesJ Clin Oncol200321101973197912743151
- ArpinoGWeissHLeeAVEstrogen receptor-positive, progesterone receptor-negative breast cancer: association with growth factor receptor expression and tamoxifen resistanceJ Natl Cancer Inst200597171254126116145046
- OsborneCKYochmowitzMGKnightWA3rdMcGuireWLThe value of estrogen and progesterone receptors in the treatment of breast cancerCancer198046Suppl 12288428887448733
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG)DaviesCGodwinJRelevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trialsLancet2011378979377178421802721
- Early Breast Cancer Trialists’ Collaborative GroupSystemic treatment of early breast cancer by hormonal, cytotoxic, or immune therapy. 133 randomised trials involving 31,000 recurrences and 24,000 deaths among 75,000 womenLancet1992339878571851345869
- CheangMCChiaSKVoducDKi67 index, HER2 status, and prognosis of patients with luminal B breast cancerJ Natl Cancer Inst20091011073675019436038
- FanCOhDSWesselsLConcordance among gene-expression-based predictors for breast cancerN Engl J Med2006355656056916899776
- PaikSShakSTangGA multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancerN Engl J Med2004351272817282615591335
- van ‘t VeerLJDaiHvan de VijverMJGene expression profiling predicts clinical outcome of breast cancerNature2002415687153053611823860
- CreightonCJFuXHennessyBTProteomic and transcriptomic profiling reveals a link between the PI3K pathway and lower estrogen-receptor (ER) levels and activity in ER+ breast cancerBreast Cancer Res2010123R4020569503
- CreightonCJOsborneCKvan de VijverMJMolecular profiles of progesterone receptor loss in human breast tumorsBreast Cancer Res Treat2009114228729918425577
- GoldhirschAWoodWCCoatesASStrategies for subtypes – dealing with the diversity of breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011Ann Oncol20112281736174721709140
- OsborneCKSteroid hormone receptors in breast cancer managementBreast Cancer Res Treat199851322723810068081
- OsborneCKNevenPDirixLYGefitinib or placebo in combination with tamoxifen in patients with hormone receptor-positive metastatic breast cancer: a randomized phase II studyClin Cancer Res20111751147115921220480
- BaselgaJCamponeMPiccartMEverolimus in postmenopausal hormone-receptor-positive advanced breast cancerN Engl J Med2012366652052922149876
- CasaAJDearthRKLitzenburgerBCLeeAVCuiXThe type I insulin-like growth factor receptor pathway: a key player in cancer therapeutic resistanceFront Biosci2008133273328718508432
- KimHJCuiXHilsenbeckSGLeeAVProgesterone receptor loss correlates with human epidermal growth factor receptor 2 overexpression in estrogen receptor-positive breast cancerClin Cancer Res2006123 Pt 21013s1018s16467118
- ShouJMassarwehSOsborneCKMechanisms of tamoxifen resistance: Increased estrogen receptor-HER2/neu cross-talk in ER/HER2-positive breast cancerJ Natl Cancer Inst2004961292693515199112
- TCGA Data Portal [database on the Internet]Bethesda (MD)National Cancer Institutec2007 – [accessed Nov 2010]. Available from: http://tcga-data.nci.nih.gov/tcga/.
- CreightonCJMassarwehSHuangSDevelopment of resistance to targeted therapies transforms the clinically associated molecular profile subtype of breast tumor xenograftsCancer Res200868187493750118794137
- MillerTWHennessyBTGonzález-AnguloAMHyperactivation of phosphatidylinositol-3 kinase promotes escape from hormone dependence in estrogen receptor-positive human breast cancerJ Clin Invest201012072406241320530877
- BaylissJHilgerAVishnuPDiehlKEl-AshryDReversal of the estrogen receptor negative phenotype in breast cancer and restoration of antiestrogen responseClin Cancer Res200713237029703618056179
- WeigeltBHuZHeXMolecular portraits and 70-gene prognosis signature are preserved throughout the metastatic process of breast cancerCancer Res200565209155915816230372
- Abdel-FatahTMPoweDGHodiZReis-FilhoJSLeeAHEllisIOMorphologic and molecular evolutionary pathways of low nuclear grade invasive breast cancers and their putative precursor lesions: further evidence to support the concept of low nuclear grade breast neoplasia familyAm J Surg Pathol200832451352318223478