Abstract
Background
Biologic disease-modifying antirheumatic drugs (bDMARDs) extend the treatment choices for rheumatoid arthritis patients with suboptimal response or intolerance to conventional DMARDs. The objective of this systematic review and meta-analysis was to compare the relative efficacy of EU-licensed bDMARD combination therapy or monotherapy for patients intolerant of or contraindicated to continued methotrexate.
Methods
Comprehensive, structured literature searches were conducted in Medline, Embase, and the Cochrane Library, as well as hand-searching of conference proceedings and reference lists. Phase II or III randomized controlled trials reporting American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 between 12 and 30 weeks’ follow-up and enrolling adult patients meeting ACR classification criteria for rheumatoid arthritis previously treated with and with an inadequate response to conventional DMARDs were eligible. To estimate the relative efficacy of treatments whilst preserving the randomized comparisons within each trial, a Bayesian network meta-analysis was conducted in WinBUGS using fixed and random-effects, logit-link models fitted to the binomial ACR 20/50/70 trial data.
Results
The systematic review identified 10,625 citations, and after a review of 2450 full-text papers, there were 29 and 14 eligible studies for the combination and monotherapy meta-analyses, respectively. In the combination analysis, all licensed bDMARD combinations had significantly higher odds of ACR 20/50/70 compared to DMARDs alone, except for the rituximab comparison, which did not reach significance for the ACR 70 outcome (based on the 95% credible interval). The etanercept combination was significantly better than the tumor necrosis factor-α inhibitors adalimumab and infliximab in improving ACR 20/50/70 outcomes, with no significant differences between the etanercept combination and certolizumab pegol or tocilizumab. Licensed-dose etanercept, adalimumab, and tocilizumab monotherapy were significantly better than placebo in improving ACR 20/50/70 outcomes. Sensitivity analysis indicated that including studies outside the target population could affect the results.
Conclusion
Licensed bDMARDs are efficacious in patients with an inadequate response to conventional therapy, but tumor necrosis factor-α inhibitor combination therapies are not equally effective.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune inflammatory disease characterized by inflammation of the synovial lining of joints, tendons, and periarticular structures,Citation1 which affects approximately 0.8% of the UK population.Citation2 If untreated, RA leads to joint destruction, functional limitation and severe disability, and has a significant impact on health-related quality of life.Citation3–Citation5 Therefore, RA imposes a significant economic burden on health-care systems and society in general. Citation6 Although the causes of RA are still obscure, research has shown that proinflammatory cytokines, such as tumor necrosis factor-α (TNF-α) and interleukin (IL)-6 or IL-1 play key roles in its pathogenesis.Citation7
Conventional disease-modifying antirheumatic drugs (cDMARDs) are generally offered as first-line treatments (most commonly methotrexate [MTX] alone, or, for active disease, in combination with another DMARD). Biologic DMARDs (bDMARDs) offer a valuable treatment alternative, being recommended for patients with suboptimal response or intolerance to cDMARDs or where continued cDMARD therapy is contraindicated.Citation8,Citation9
A number of bDMARDs have been licensed for such use in the EU. TNF-α inhibitors include etanercept, adalimumab, infliximab, certolizumab pegol, and golimumab. In combination with MTX, the TNF-α inhibitors are each indicated for the treatment of moderate to severe active RA in adults when the response to DMARDs, including MTX, has been inadequate. In addition, adalimumab, etanercept, and certolizumab pegol are licensed as monotherapy in those patients intolerant of MTX or for whom continued MTX is inappropriate.
The costimulatory inhibitor abatacept and the anti-IL-6 therapy tocilizumab, in combination with MTX, are licensed for moderate to severe active RA in adults responding inadequately to previous therapy with one or more cDMARDs including MTX or a TNF-α inhibitor. Tocilizumab is also licensed as monotherapy in patients intolerant of MTX or for whom continued MTX is inappropriate. In addition, the anti-B-cell therapy rituximab, in combination with MTX, is licensed in adult patients with severe active RA with inadequate response or intolerance to other DMARDs including one or more TNF-α inhibitors.
The objective of this systematic review was to compare the clinical efficacy of EU licensed-dose bDMARD combinations for the treatment of adult RA patients after failure on one or more DMARDs, where efficacy was measured using American College of Rheumatology (ACR) response end points from randomized controlled trials (RCTs). A network meta-analysis (NMA) was performed to pool RCT evidence for bDMARDs via common control treatments (eg, MTX control), to provide estimates of relative treatment effects. The rationale for this approach was that there are few trials comparing bDMARDs head-to-head. Therefore, NMA can support inferences to the target RA population, as all the available evidence from relevant RCTs are used in the analysis.
As bDMARD monotherapies are used in a different part of the treatment pathway, ie, in a population intolerant of MTX or for whom continued MTX is inappropriate, a separate analysis of bDMARD monotherapies was performed.
Methods
The methods used for the review and meta-analysis of combination therapy are the same as for monotherapy, except where otherwise stated.
Systematic review
Study eligibility criteria
A protocol was written to define all aspects of the systematic review prior to commencement. The inclusion criteria are shown in . As the data used in a meta-analysis should be from sufficiently similar studies and outcomes to make the results meaningful and to reduce the influence of confounding factors, included studies had to report sufficient data for the ACR 20, 50, or 70 response to treatment end point (defined as a 20%, 50%, or 70% improvement in tender and swollen joints and the same level of improvement in three of the five following variables: patient and physician global assessments of overall disease activity; patient evaluation of pain (pain health assessment questionnaire [HAQ]Citation10); a score of physical disability; and blood acute-phase reactants). End points needed to be measured between 12 and 30 weeks from baseline. Studies in which more than 15% of patients had had previous TNF-α inhibitor treatment were excluded, because this population was more extensively pretreated and considered likely to be less responsive than the TNF-α inhibitor-naïve population. Studies were not restricted by date of publication or publication status.
Table 1 Summary of inclusion criteria for the systematic review and meta-analysis
Data extraction
The data sources to identify published RCTs and ongoing (as yet unpublished) RCTs included:
Electronic databases accessed via OVID and the Cochrane Library: Medline in process and Medline 1950 to present; Embase 1980 to 2010 week 23 and 1980 to 2011 week 14; the Cochrane Library (Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects, Cochrane Central Register of Controlled Trials, and Health Technology Assessment Database). The original search was conducted June 17, 2010. The same search was rerun April 15, 2011 to identify any studies entered into the databases from June 1, 2010.
Hand-searching of reference lists of included RCTs.
Hand-searching of RCTs included in previously conducted systematic reviews/meta-analysesCitation11,Citation12 and the Cochrane reviews on bDMARDs.Citation13–Citation19
Reviewing the Canadian Agency for Drugs and Technologies in Health therapeutic review.Citation20
The following conference proceedings were searched (2005–10): ACR, European League Against Rheumatism, and the British Society for Rheumatology.
The US Institutes of Health online registry and results database of clinical trialsCitation21 was searched to identify ongoing studies.
The structured database search strings were designed to identify RCTs or systematic reviews indexed on Medline, and these strings were then modified for performing searches of Embase and the Cochrane Library to account for differences in syntax and thesaurus headings. Searches included terms for free text and Medical Subject Heading (MeSH) terms to identify RCTs of RA patients taking DMARDs or bDMARDs.
One reviewer screened the title and abstract of studies identified against the eligibility criteria. Full-text papers were then assessed to ensure studies met the criteria or for those studies where eligibility could not be determined from the title/abstract. Any uncertainties as to eligibility were referred to a second reviewer and resolved by consensus. Data were extracted from eligible publications into a predefined data-extraction table by one reviewer and verified by a second.
The data items collected included patient (average age, percentage female, disease duration, baseline severity of RA, MTX- or other DMARD-exposure and TNF-α exposure), intervention (treatment(s) received, dosage and dose schedule), study (study blinding and country(ies), number of patients randomized, follow-up period, frequency of withdrawals), and outcome (ACR 20/50/70) level parameters.
Quality assessment
Risk of bias was assessed using criteria set out in the National Institute for Health and Clinical Excellence (NICE) guidelines manual.Citation22 For studies included in the meta-analysis, a formal assessment of publication bias was conducted via funnel plots with Egger’s linear regression test of asymmetry.Citation23,Citation24
Meta-analysis methodology
For this meta-analysis, the study arms were pooled into treatment groups; we were interested in those study arms where the intervention was used in accordance with the EU license, since these are the treatments used in clinical practice. Therefore, the treatments of interest for therapy in DMARD-experienced patients are licensed bDMARD combinations plus common control arms used to connect the network ().
Table 2 Active licensed treatment arms of interest
In a separate analysis we considered a population of patients who are intolerant of MTX or for whom MTX is contraindicated; the treatments of interest here are licensed bDMARD monotherapies plus common control arms used to connect the network (). As other cDMARDs may be used as monotherapy if MTX is contraindicated, sulfasalazine is also a treatment of interest in the monotherapy analysis. Other control arms were included in the evidence networks to preserve randomization as well as other unlicensed arms. The results for these unlicensed treatments have been omitted from this publication.
The analyses of the ACR 20/50/70 outcomes were conducted on an intent-to-treat (ITT) basis, or modified ITT (number actually receiving treatment at baseline) if the number randomized to treatment is not reported. An ITT analysis requires imputing outcomes for the missing participants, although there is no overall consensus on how to do this;Citation25 for the ACR 20/50/70 outcomes, it is assumed that missing participants did not achieve the required improvement (ie, a worst-case scenario).
Direct and indirect meta-analysis
A fixed and random-effects meta-analysis was conducted in Stata IC version 11.2 using the Metan package SJ9_2: sbe24_3 (StataCorp, College Station, TX).Citation26,Citation27 The random-effects analysis used the method of DerSimonian and Laird, with the estimate of heterogeneity taken from the Mantel– Haenszel model. The fixed-effect analysis used the Mantel– Haenszel method. For binomial data analysis, if a study contains a zero observation (eg, no patients achieved ACR 70), Stata adds 0.5 to each cell of the trial by default.
Indirect comparisons between treatment (A) and other treatments of interest (B) via a common comparator (C) were made using the Bucher methodCitation28,Citation29 and the pooled odds ratio (OR) produced from the direct meta-analysis.
Network meta-analysis
In an NMA, treatment effects are calculated for all treatments using all available evidence in one simultaneous analysis.Citation30–Citation32 NMA methods build on the principles of indirect comparisonsCitation28,Citation29 and preserve the randomized comparisons within each trial.
The models were fitted to the data using Bayesian Markov chain Monte Carlo methods (specifically Gibbs sampling), using WinBUGS software version 1.4.3.Citation33–Citation35 WinBUGS code for NMA of dichotomous and standard Bayesian random-effects meta-analysis was adapted from code developed by the MRC Biostatistics UnitCitation36 and the NICE Decision Support Unit.Citation37
The WinBUGS models were run for a minimum of 100,000 iterations to ensure model convergence. Subsequently, two chains of 20,000 were sampled from the posterior distributions. These samples were used to calculate the median/mean and where relevant the 95% credible interval (CrI), which is the interval from percentiles 2.5 to the 97.5. For treatment effects, medians are presented as the best estimate for the central value, since means may be overly influenced by outliers.
Analysis of baseline risk
To calculate the absolute probability of responding to each treatment, we first conducted a standard direct random-effects meta-analysis that pooled data on the log-odds (or mean difference from baseline) of responding to the reference control treatment. The reference treatment is chosen to be the control that has the most data available, ie, the DMARD control in this analysis. The (mean and standard deviation) pooled log-odds (or mean differences) of responding to the reference treatment were then used as priors in the main NMA to inform the calculation of the absolute efficacy of each treatment.Citation38
Analysis of treatment effects
For dichotomous end points, such as ACR 20/50/70, the NMA calculates the ORs for all treatments compared with other treatments. The base case models were random-effects models; fixed-effect models were used as sensitivity analyses. Random-effects NMA differs from fixed-effect NMA in that it allows the true treatment effect (eg, OR between two treatments) to vary between studies due to heterogeneity. In these random-effects models, a uniform (uninformative) prior is used for the between-studies standard deviation (as per HasselbladCitation39 and GelmanCitation40).
For the ACR 70 outcome, some studies reported zero events in the DMARD control arm, requiring a continuity correction to be applied. A fixed value of 0.5 was added to the numerator (and 1 to the denominator) for all arms of the affected trial.Citation37,Citation41 The fixed-value correction overcomes computational errors, but it biases study estimates towards no difference and overestimates variances. Biases will be more apparent in trials where the treatment arms are of unequal effect.
Covariate analysis
Covariate analyses were conducted to explore potentially confounding factors. We conducted a study-level covariate analysis to take into account the following differences in study protocols (DMARD-experienced analysis): (1) Length of follow-up: the model included a study level continuous variable to adjust for the time point at which the response was measured (in weeks). Xweeks is a covariate centered at mean follow-up across the included studies, such that the coefficient βweeks estimates the incremental difference in (log) treatment effect for each week above/below the average follow-up across studies. (2) Studies where MTX was administered at a low dose: the Japanese maximum dose of 8 mg/week was used as a cutoff (Xmtx = 1 if study population received MTX within the normal dose range [maximum dose more than 8 mg/week]; 0 otherwise). The coefficient βmtx estimates the incremental (log) treatment effect between low-dose concomitant MTX and normal-dose concomitant MTX.
We conducted an additional covariate analysis to take into account the following study-arm level differences in patient characteristics: (1) average age at baseline, and (2) average disease duration at baseline. This covariate model included these continuous variables to adjust for differences in patient age and disease duration (in years) across study arms. Xage and Xduration are covariates centered at mean age and disease duration, respectively, such that the coefficient βage and βduration estimate the incremental difference in the (log) treatment effect for each year above/below the average age or disease duration across study arms.
Subgroup analyses
The following additional analyses were conducted for combination therapy:
As base case, but remove studies that included MTX-naïve patients, ie, subgroup is the MTX-experienced population. The studies removed for this analysis were Combe et alCitation42 and Genovese et al.Citation43
As base case, but remove the certolizumab trials RAPID 1 and RAPID 2,Citation44,Citation45 on the basis of study design/pattern of withdrawals where many trial participants, particularly those randomized to the MTX control arm, were withdrawn early because of lack of efficacy and given rescue medication prior to the primary end point at week 24 being reached. Week 16 withdrawals in RAPID 1: 62.8% placebo, 21.1% certolizumab 200 mg, 17.4% certolizumab 400 mg. Week 16 withdrawals in RAPID 2: 81.1% placebo, 21.1% certolizumab 200 mg, 21.1% certolizumab 400 mg.
As base case, but remove open-label etanercept trials of Kameda et alCitation46 and van Riel et alCitation47 and the etanercept trial with the early escape design of Genovese et al.Citation48
As base case, but remove studies that contain (up to 15% of) patients who are TNF-α inhibitor-experienced, in addition to being MTX-experienced. These studies were: Genovese et al,Citation43 Keystone et al,Citation44 Kremer et al,Citation49,Citation50 Maini et al,Citation51 Smolen et al,Citation45,Citation52 and Zhang et al.Citation53 The rationale is that these patients have had more previous treatments.
As base case, but include data from the Klareskog et al trialCitation1,Citation54 at 24 weeks. This trial is not representative of the inadequate responder population required by the systematic review selection criteria, as some of the population enrolled were MTX-naïve. Some previous meta-analyses have included this study, however, so its influence is examined here by including it in a sensitivity analysis. Data for this analysis were 24-week data from the unpublished clinical study report.Citation55
Sensitivity analysis for monotherapy was conducted as follows: as base case, but include data from the TEMPO trial (24-week data from the unpublished clinical study reportCitation55). Subset analysis was not conducted: removing studies in MTX-naïve or TNF-α-experienced populations from the base case would leave too few remaining studies.
Model fit
The mean residual deviances provided an estimate of how well the values predicted by the model fit the observed dataset.Citation56 For an adequate model fit, the sum of the residual deviances should be approximately equal to the total number of study arms in the observed dataset. In addition the deviance information criterion (DIC) output by WinBUGsCitation57 was recorded. The model with the lowest DIC is estimated to be the model that would best predict a replicate dataset of the same structure as that currently observed.
Consistency of NMA estimates
An informal assessment of consistency was performed by comparing the treatment effects estimated via the NMA against the pair-wise direct meta-analysis results and results of the indirect Bucher analysis to identify potential discrepancies between the results from the different methods.
Furthermore, the network diagrams were examined to determine the number of independent loops in the network of evidence for which inconsistency in the evidence could occur.Citation38 Disregarding loops that occur solely from a multi-arm trial (since within-trial treatment effects are not independent), the size of any inconsistency was determined for each independent loop using the Bucher methodCitation28,Citation29 and the Z-test (or chi-squared test if one edge of the loop is shared with other loops) to determine if the inconsistency was statistically significant.
Results
Literature search results
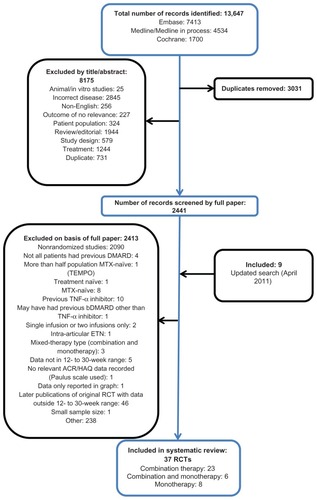
A total of 10,616 potentially relevant records were identified, excluding duplicates from the original search, of which 8175 were excluded on screening the title and abstract. On application of the inclusion criteria to the 2441 full-text papers, a further 2415 were excluded. Nine additional studies were identified from the updated search. Thirty-seven publications were included; 23 assessing combination therapy onlyCitation43–Citation45,Citation48–Citation50,Citation52,Citation53,Citation58–Citation72 eight monotherapy only,Citation73–Citation80 and six monotherapy in addition to combination-therapy armsCitation42,Citation46,Citation47,Citation51,Citation81,Citation82 ().
Figure 1 Flow diagram of included/excluded studies.
Systematic review results for combination studies
Of the 29 studies with at least one combination-therapy arm () three assessed abatacept,Citation49,Citation66,Citation69 five adalimumab,Citation59,Citation62,Citation64,Citation65,Citation71 two certolizumab pegol,Citation44,Citation45 six etanercept,Citation42,Citation46–Citation48,Citation67,Citation70 three golimumab,Citation50,Citation63,Citation82 six infliximab (one of which had an abatacept arm also, providing the only head-to-head comparison),Citation53,Citation58,Citation60,Citation68,Citation69,Citation72 two rituximab,Citation61,Citation81 and three tocilizumab.Citation43,Citation51,Citation52 All studies utilized licensed doses, with the exception of one golimumab study.Citation50
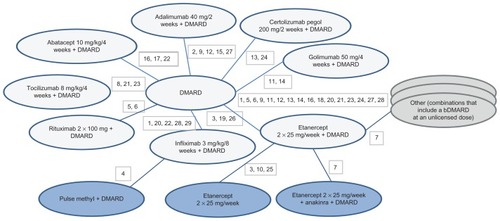
Figure 2 Network diagram for ACR20/50/70 outcomes for bDMARD combination therapies.
Notes: 1, Abe 2006; 2, Chen 2009; 3, Combe 2006; 4, Durez 2004; 5, Edwards 2004; 6, Emery 2010 (SERENE); 7, Genovese 2004; 8, Genovese 2008 (TOWARD); 9, Huang 2009; 10, Kameda 2010 (JESMR); 11, Kay 2008; 12, Keystone 2004 (DE019); 13, Keystone 2008 (RAPID 1); 14, Keystone 2009 (GO-FORWARD); 15, Kim 2007; 16, Kremer 2003; 17, Kremer 2006 (AIM); 18, Kremer 2010; 19, Lan 2004; 20, Maini 1999 (ATTRACT); 21, Maini 2006 (CHARISMA); 22, Schiff 2008 (ATTEST); 23, Smolen 2008 (OPTION); 24, Smolen 2009a (RAPID 2); 25, van Riel 2006 (ADORE); 26, Weinblatt 1999; 27, Weinblatt 2003 (ARMADA); 28, Westhovens 2006b (START); 29, Zhang 2006. DMARD 25 arms, 3039 patients; abatacept 10 mg/kg/4 weeks + DMARD 3 arms, 704 patients; adalimumab 40 mg/2 weeks + DMARD 5 arms, 495 patients; certolizumab pegol 200 mg/2 weeks + DMARD 2 arms, 639 patients; etanercept 2 × 25 mg/week + DMARD 6 arms, 500 patients; golimumab 50 mg/4 weeks + DMARD 2 arms, 124 patients; infliximab 3 mg/kg/8 weeks + DMARD 6 arms, 760 patients; rituximab 2 × 1000 mg + DMARD 2 arms, 212 patients; tocilizumab 8 mg/kg/4 weeks + DMARD 3 arms, 1058 patients.
Study and patient characteristics are summarized in . The majority of RCTs were double-blind, three being open-label.Citation46,Citation47,Citation60 In total the included studies randomized 11,490 patients. Included patients had active RA in spite of prior treatment with a DMARD. Not all studies reported baseline disease activity score (DAS). Of those that did, 13 involved populations with more severe RA: eleven trials had a mean or median baseline DAS28 of 5.9 or above,Citation44,Citation45,Citation47,Citation51,Citation52,Citation59,Citation61,Citation66,Citation69,Citation81,Citation82 and in two trials of either abatacept or infliximab, the authors noted the particularly severe or active nature of disease in the study population.Citation49,Citation68 In two trials involving either etanercept or infliximab, the mean baseline DAS28 was between 5.0 and 5.2,Citation42,Citation72 indicating that the population would have included some patients with severe RA and others with more moderate-severity disease. The definition of “active RA” was inconsistent across studies, with some requiring ≥ six tender joints and ≥six swollen joints, whilst others required ≥ twelve tender joints and ≥ten swollen joints. One study of infliximab in particular may have enrolled patients with less active RA, as its definition of active RA included having ≥ eight tender joints and only ≥ three swollen joints.Citation53 In most trials, the patient population was anti-TNFα inhibitor-naïve. Patients had a mean age of between 48 and 58 years and had on average suffered from RA for 5–10 years (around 9 months in Maini et alCitation51 and 13 years in Weinblatt et alCitation71). These trials were, therefore, broadly representative of the population of interest, namely, adult patients with moderate–severe active RA, previously treated with (and with insufficient response to) MTX or another DMARD, irrespective of disease duration.
Table 3 Characteristics of included combination therapy studies
The risk of bias, as assessed by NICE criteria, was considered low for the majority of included studies. For five studies, the risk of bias was unclear,Citation50,Citation53,Citation59,Citation61,Citation67 due to incomplete reporting. Only the study by van Riel et alCitation47 was considered to have a high risk of bias, as there was no concealment of treatment allocation (and several other parameters were unclear).
Data for the ACR 20/50/70 end points are presented in . The follow-up period was 24 weeks in 18 of the 29 trials,Citation42–Citation46,Citation48–Citation50,Citation52,Citation61,Citation62,Citation64–Citation66,Citation70,Citation71,Citation81,Citation82 ranging from 12 weeksCitation59,Citation67 to 30.Citation68– show funnel plots for ACR 20/50/70, respectively, for all studies with DMARD control arm used in the combination-therapy meta-analysis. An asymmetrical funnel plot suggests publication bias or systematic difference between smaller and larger studies, and might therefore suggest that simple meta-analysis of the dataset was not appropriate. Funnel plots also highlight outlier studies, where the control-arm response is either particularly high (leading to an underestimate of the active treatment effect by comparison) or particularly low (leading to an overestimate of the active treatment’s relative effect).Citation23,Citation24 For ACR 20, there is a good, symmetrical spread of control responses either side of the mean response (). RAPID 1,Citation44 RAPID 2,Citation45 TOWARD,Citation43 and ARMARDACitation71 may underestimate the log-odds of ACR 20 response in the control arm, and hence overestimate the treatment effects (). Conversely, AIM,Citation66 ATTEST,Citation69 Huang et al,Citation62 and Zhang et alCitation53 may overestimate the log-odds of ACR 20 response in the control arm, and hence underestimate the treatment effects (). For ACR 50, there is a reasonable spread of control responses either side of the mean response (). RAPID 1,Citation44 RAPID 2,Citation45 TOWARD,Citation43 and ATTRACTCitation68 may overestimate treatment effects, and CHARISMA,Citation51 ATTEST,Citation69 Huang et al,Citation62 and Zhang et alCitation53 underestimate them (). For ACR 70, the spread of control responses is asymmetrical in the direction of lower-than-expected responses (). OPTIONCitation52 and TOWARDCitation43 may overestimate treatment effects, whereas CHARISMA,Citation51 Huang et al,Citation62 and Zhang et alCitation53 may underestimate them ().
Figure 3 Funnel plot comparing the log odds of response across combination study control arms: log odds of DMARD control achieving ACR20.
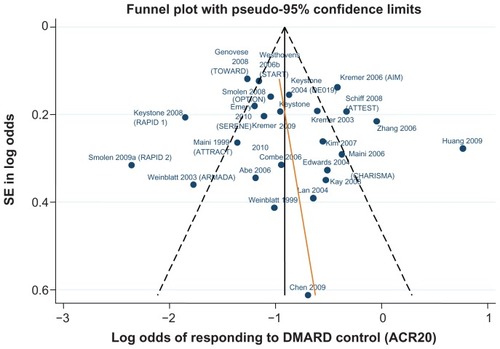
Figure 4 Funnel plot comparing the log odds of response across combination study control arms: log odds of DMARD control achieving ACR50.
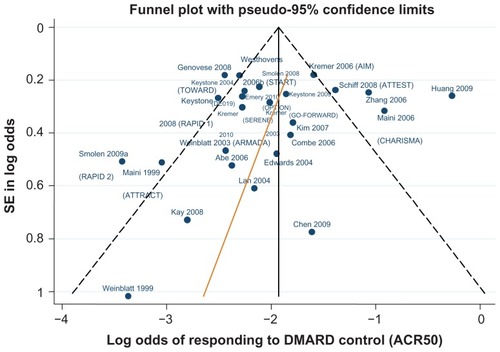
Figure 5 Funnel plot comparing the log odds of response across combination study control arms: log odds of DMARD control achieving ACR70.
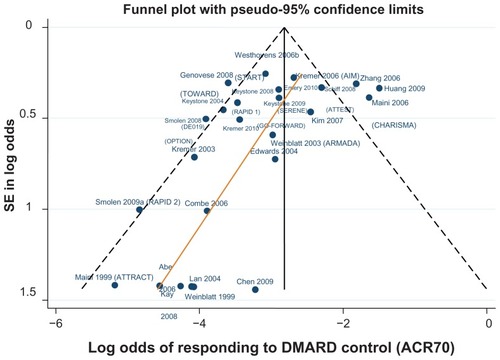
Table 4 ACR20/50/70 data used in the combination therapy NMA
Meta-analysis results for combination-therapy analysis
The results from the NMA are shown in (comparison versus DMARD control), with comparisons of etanercept versus other licensed bDMARDs in .
Table 5 American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 network meta-analysis base case results for combination treatments in DMARD-experienced patients: licensed biologic DMARD combinations versus DMARD alone
Table 6 American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 network meta-analysis base case results for combination treatments in DMARD-experienced patients: licensed ETN combination versus other licensed biologic DMARD combination
The random-effects model did not show a significant difference in ACR 70 for rituximab 2 × 1000 mg + DMARD compared to DMARD alone. Otherwise, all licensed bDMARD combinations have significantly higher odds of ACR 20/50/70 compared to DMARDs alone (based on the 95% CrI, ).
The etanercept combination was significantly better than the other TNF-α inhibitors, adalimumab, and infliximab in improving ACR 20/50/70 outcomes (based on the 95% CrI, ). The etanercept combination was also significantly better than abatacept in improving ACR 20/50/70 outcomes, significantly better than golimumab in improving ACR 20 and rituximab in improving ACR 70 (based on the 95% CrI, ). There were no significant differences between the etanercept combination and certolizumab pegol or tocilizumab.
Regarding model selection, there were sufficient studies for random-effects models to be used. The base case NMA models displayed good convergence, and for all outcomes the random-effects model had the best fit based on lowest DIC and mean residual deviance (the sum of the residual deviances divided by the total number of study arms in the observed data set) (). For ACR 70 data, a continuity correction was applied in order to account for several instances of zero events in the control arms for this outcome. Between study heterogeneity, as shown by the standard deviation in treatment effects between studies () was quite high among studies in the network (ACR 20 standard deviation [SD] on a logarithmic scale = 0.31, ACR 50 SD = 0.40, and ACR 70 SD = 0.50). This suggests that the predicted difference on a natural scale between a study’s OR estimate and our NMA estimate may vary (between upper and lower limits) by 3.44 for ACR 20, 4.84 for ACR 50, and 7.23 for ACR 70. There is, therefore, greater uncertainty around the ACR 70 results than around ACR 50 or ACR 20.
Table 7 Comparison of model fit for base case combination therapy network meta-analysis models
The NMA results compare well with the direct head-to-head analysis (Table S1, ) and with the Bucher indirect comparisons (Table S2, ), though no formal test of consistency could be conducted, due to there being no independent loops of evidence. The NMA has a wider CrI compared to direct estimates from head-to-head trials: the lower bounds are similar, but the NMA estimates a much higher upper bound. Similarly, there is more uncertainty (in favor of etanercept) in the NMA estimates of etanercept versus the other licensed combinations compared to the estimates obtained from the Bucher indirect comparison.
shows the results of the study-level covariate analysis, which estimates the treatment effects taking into account the impact of low-dose MTX (maximum dose less than 8 mg/week) and length of follow-up for reporting the ACR outcomes. A low dose of background MTX did not have a statistically significant impact on ACR 20/50/70, and length of follow-up did not have a statistically significant impact on ACR 20 or ACR 50. The βmtx coefficient was statistically significant in the analysis of ACR 70 outcomes (based on the 95% CrI, ), such that a longer length of follow-up was associated with higher odds of ACR 70 response. However, this single significant result should be viewed with caution, since the criteria for significance (type I error, the probability of rejecting the null hypothesis when it is true − < 5%) does not take into account multiple significance testing, ie, no correction for multiple testing was applied, and no reduction in the criteria for significance (to 1%, for example) was made to keep the type I error to a minimum, and as such this result could have occurred by chance.
Table 8 Results from combination therapy network meta-analysis study-level covariate analysis for American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 end point
In an additional covariate analysis of patient characteristics (at study-arm level), longer disease duration was associated with higher odds of ACR 50 and higher patient age with higher odds of ACR 70. Otherwise, age and disease duration were not statistically significant (Table S3). As the base case and covariate odds ratios for each treatment are not largely different, our conclusion regarding the differential effectiveness of etanercept vs adalimumab or infliximab remains unaltered.
The results of the pr-defined sensitivity analyses are shown in Table S4. Removing the RAPID 1/2 or TNF-α-exposed trials had very little impact on the treatment-effect estimates. Removing the etanercept studies had very little impact on the treatment-effect estimates for etanercept for ACR 50 and 70 outcomes, but lowered the treatment-effect estimates for etanercept and certolizumab for ACR 20. The inclusion of the TEMPO study lowered the treatment-effect estimates for etanercept for ACR 20/50/70.
Systematic review results for monotherapy studies
Fourteen studies qualified for inclusion in the analysis of bDMARD monotherapy (): two studies with a licensed-dose adalimumab arm,Citation74,Citation78 plus one additional study with nonlicensed adalimumab arms,Citation79 five trials including licensed-dose etanercept,Citation42,Citation46,Citation47,Citation73,Citation75 plus one additional study including nonlicensed etanercept,Citation80 and three studies including licensed tocilizumab.Citation51,Citation76,Citation77 There were two additional studies that included only nonlicensed rituximab and golimumab arms.Citation81,Citation82 There were no studies included in the review that assessed a certolizumab monotherapy arm: the FAST4 WARD trialCitation83 was excluded on the basis that patients may have had a prior bDMARD (other than TNF-α).
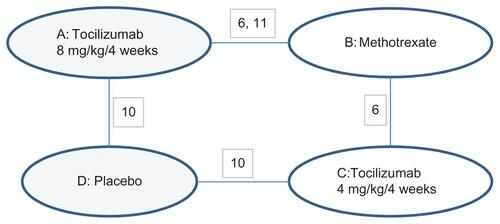
Figure 6 Network diagram for ACR20/50/70 outcomes for bDMARD monotherapy.
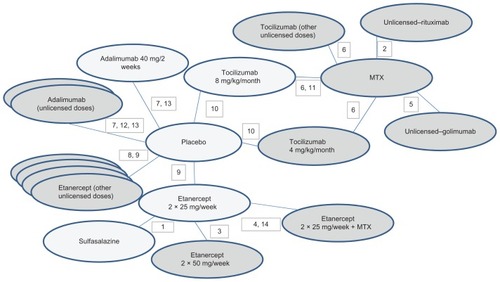
Study characteristics and patient characteristics are summarized in . All studies were double-blind, with the exception of two that were open-label.Citation46,Citation47 The range of baseline disease severity, as measured by DAS28 score, was from moderate–severe (DAS28 5.0–5.2Citation42) to very severe (DAS28 7.0–7.1Citation78,Citation79). Seven studies enrolled anti-TNF-α-naïve patients.Citation42,Citation46,Citation47,Citation73–Citation75,Citation81 In one study, 14% of patients had prior exposure to etanercept or infliximab, but not in the 12 weeks prior to enrolment.Citation51 In another,Citation78 there had been no biologic treatment permitted in the 6 months prior to enrolment. In two,Citation77,Citation84 the status was not reported (so for these, an assumption of patients being anti-TNF-α-naïve was made). The mean age ranged from 51Citation75 to 57Citation74 years. The percentage of female participants in any treatment arm varied from 61%Citation80 to 90%.Citation84 Mean disease duration ranged from 8.4 yearsCitation74 to 13 years.Citation75 The risk of bias was highest in the open-label studies.Citation46,Citation47 Data for ACR 20/50/70 for the monotherapy analysis are presented in .
Table 9 Characteristics of included monotherapy studies
Table 10 American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 data used in the monotherapy network meta-analysis
The patients enrolled in the adalimumab studies were broadly similar in terms of disease duration, but one of the adalimumab trialsCitation78 may have involved patients who had had some prior biologic exposure (though not in the 6 months prior to enrolment), and may therefore have enrolled a group less likely to respond.
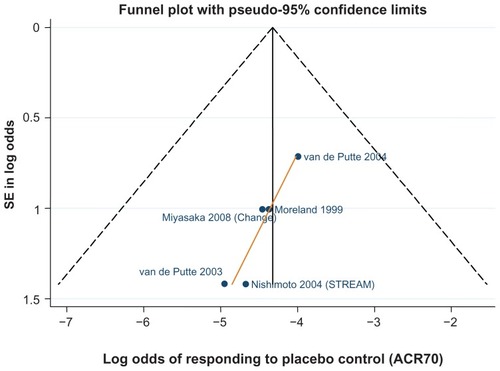
Tocilizumab studies had on average a shorter disease duration (8.3Citation77 and 8.5 yearsCitation84) compared to the etanercept and adalimumab monotherapy studies. – show funnel plots for ACR 20/50/70, respectively, for all studies with placebo control arm used in the monotherapy meta-analysis.
Figure 7 Funnel plot comparing the log odds of response across monotherapy study control arms: log odds of placebo control achieving ACR20.
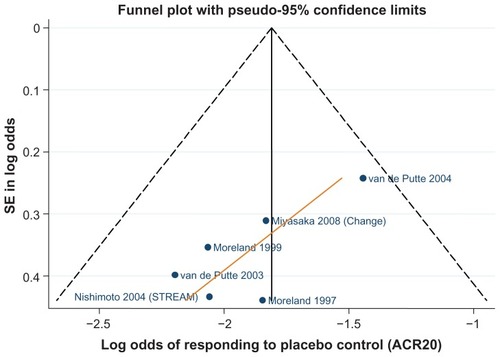
Figure 8 Funnel plot comparing the log odds of response across monotherapy study control arms: log odds of placebo control achieving ACR50.
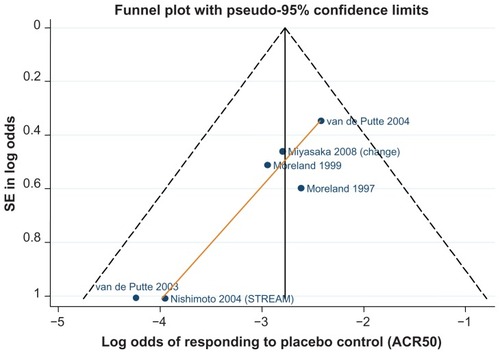
Figure 9 Funnel plot comparing the log odds of response across monotherapy study control arms: log odds of placebo control achieving ACR70.
Meta-analysis results for monotherapy analysis
The results from the NMA are shown in (comparison versus placebo control), with comparisons of etanercept versus other licensed bDMARDs shown in . Licensed-dose etanercept, adalimumab, and tocilizumab monotherapy were significantly better than placebo in improving ACR 20/50/70 outcomes (based on the 95% CrI, ). Etanercept monotherapy was significantly better than sulfasalazine in improving ACR 20/50/70 outcomes (based on the 95% CrI, ).
Table 11 American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 network meta-analysis base case results for monotherapy treatments in DMARD-experienced patients: licensed DMARD monotherapy versus placebo
Table 12 American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 network meta-analysis base case results for monotherapy treatments in DMARD-experienced patients: licensed ETN monotherapy versus other licensed DMARD monotherapy
As expected, the NMA had wider confidence intervals compared to direct estimates from head-to-head trials. In general, the NMA models displayed fair convergence, though some of the ACR 70 models did not converge. The random-effects model had the best fit (). A continuity correction was applied to the ACR 70 data where zero events occurred in the control arms, and between-study heterogeneity estimates were high (ACR 20 SD on a logarithmic scale = 0.81, ACR 50 SD = 0.55, and ACR 70 SD = 0.76). This suggests that the predicted difference on a natural scale between a study’s OR estimate and our NMA estimate may vary (between upper and lower limits) by 24.64 for ACR 20, 8.8 for ACR 50, and 19.8 for ACR 70 (). As a result of between-study heterogeneity, therefore, there is more uncertainty associated with the ACR 20 and ACR 70 treatment-effect estimates for monotherapy, compared to the ACR 50 outcome.
Table 13 Comparison of model fit for monotherapy network meta-analysis models
The NMA results compare well with direct head-to-head analysis (Table S5, ) and with Bucher indirect comparisons (Table S6, ). Examination of the monotherapy evidence network shows that there was one independent loop for which inconsistency of the direct and indirect evidence can be assessed (Figure S1). The analysis indicates that the inconsistency on this loop is not significant (P > 0.05 for ACR 20/50/70; Tables S7–S9).
A covariate analysis was not conducted, as there were too few monotherapy studies to make such an analysis robust. The results of the predefined sensitivity analyses are shown in Table S10. The inclusion of the TEMPO study lowers the treatment-effect estimates for etanercept monotherapy.
Discussion
bDMARDs, in combination with a conventional DMARD, have been shown to be efficacious in patients who have had an inadequate response to prior DMARD therapy, thus representing an important addition to the RA treatment algorithm for patients and their health-care provider. Based on the clinical data identified in a systematic review, we conducted NMAs obtaining pooled estimates of relative treatment effects, allowing pair-wise comparisons and ranking of licensed bDMARD therapies. We also conducted a separate analysis of bDMARD monotherapy treatments, which are licensed for use in patients who cannot tolerate MTX or for whom MTX is contraindicated. Our results show that all licensed bDMARD combinations have significantly higher odds (based on the 95% CrI) for ACR 20/50/70 compared to MTX or DMARD monotherapy, ACR 70 results for RTX being the only exception.
For DMARD experienced patients, our results also show that the etanercept combination is significantly better than the adalimumab and infliximab combinations and comparable to the certolizumab combination in improving ACR 20/50/70 outcomes (based on the 95% CrI). Therefore, previous meta-analyses that pooled TNF-α inhibitors into a single group may have underestimated the efficacy of etanercept.Citation85,Citation86
The internal validity of any NMA is dependent upon three key considerations: RCT identification, individual RCT quality, and the degree of confounding bias because of similarity or consistency assumptions not being met.
Regarding the first of these, an extensive systematic review was conducted to ensure identification of all relevant RCTs. The extent of publication bias was assessed, the slope of the colored lines in the funnel plots (–, combination NMA; –, monotherapy NMA) indicating a small degree of publication bias. The network of RCTs was fairly balanced for most treatments. In the combination analysis, there was some network asymmetry, however; a greater weight of evidence was available for tocilizumab (three trials and 1058 patients) and a smaller such weight for golimumab (two arms and 124 patients).
Regarding the second consideration, quality assessment of individual RCTs did identify some open-label or early escape design studies that may have been more prone to bias, but the effect of including these in the base case was assessed – by sensitivity analyses – which showed that including these studies did not bias the treatment-effect estimates in favor of etanercept.
Regarding the third consideration, meta-analysis has the underlying assumption that trials and outcomes are sufficiently similar to allow data to be pooled, and the consistency assumption relies on there being no imbalance in modifiers of relative treatment effects across studies. In our NMA, the similarity assumption was supported by the eligibility criteria applied for study selection, and the adjustment of the results by way of covariate analyses for the potential effect modifiers, low dosing of MTX, length of follow-up, age, and disease duration. This covariate adjustment aimed to reduce the impact of any bias due to similarity and/or consistency violations. Low dosing of MTX did not have a statistically significant impact on ACR 20/50/70, nor did length of follow-up for ACR 20/50. Longer disease duration was associated with higher odds of ACR 50 and higher age with higher odds of ACR 70. Adjusting for age and disease duration did not alter our conclusion. We further examined the influence of exposure to prior anti-TNF-α therapies and of incorporating the TEMPO trial, a trial that included some MTX-naïve patients or patients that were not MTX-inadequate responders, by sensitivity analyses: overall, removing subsets of trials had very little impact on treatment-effect estimates, but meta-analysis that included the TEMPO trialCitation85,Citation87 underestimated the efficacy of etanercept in the DMARD-experienced/inadequate-response population because of the high MTX control arm response rate in patients previously untreated with MTX, ie, these patients were still able to benefit from MTX.
There remained heterogeneity among the studies in our NMA. The patient characteristic that differed across studies but that was not assessed as a covariate was the number of prior DMARD treatments. This is one area, therefore, where the similarity assumption may be challenged, and should be considered for covariate adjustment in future research.
One tocilizumab study, in particular – CHARISMACitation51 – enrolled patients with a mean duration of disease of only 9.2 months.Citation51 This does not appear to have influenced the treatment estimates here, however. The CHARISMA study is small compared to the other tocilizumab studies – OPTIONCitation52 and TOWARDCitation43 – so will have less weight in the meta-analysis. The random-effects direct meta-analysis of tocilizumab versus DMARD did not indicate any significant heterogeneity in effect on ACR 20 between OPTION, CHARISMA, and TOWARD (ACR 20 l2 = 0%, P = 0.86; ACR 50 I2 = 30.6%, P = 0.24; ACR 70 I2 = 59.7%, P = 0.08). In the direct meta-analysis of tocilizumab versus DMARD for ACR 50 and ACR 70, CHARISMA had a lower ACR 50 and ACR 70 treatment effect (relative to DMARD) compared to OPTION and TOWARD. This was somewhat counterintuitive, as one would expect that patients with shorter disease duration (fewer previous lines of treatment) would have better response to treatment than would patients with longer disease duration (who have had more previous treatments). The different ACR 50 and ACR 70 relative effects observed in CHARISMA, therefore, may be due to factors other than disease duration, and we conclude that the short duration of disease in the CHARISMA study population did not impact on the treatment-effect estimates.
Differences in placebo/MTX responses across trials were assessed by way of funnel plots, identifying some studies within the network that under- or overestimated the response to placebo/MTX, meaning that they would over- or underestimate, respectively, the treatment effect. From review of the funnel plots, it can be deduced that the overall treatment effects on ACR 20 and ACR 50 may be overestimated for certolizumab pegol.Citation44,Citation45 The low response to MTX observed in the certolizumab pegol RAPID 1Citation44 and RAPID 2Citation45 trials (see and ) may be explained by the early escape trial design, whereby patients who had failed to respond at weeks 12–14 were withdrawn from treatment at week 16 and classified as nonresponders. More than half of the patients were withdrawn from the MTX control arms, whereas a lower percentage of certolizumab combination-arm patients were withdrawn. This imbalance in withdrawals may have had an impact on the treatment effects measured by these studies: week 16 withdrawals in RAPID 1 – 62.8% placebo, 21.1% certolizumab 200 mg, 17.4% certolizumab 400 mg; week 16 withdrawals in RAPID2 – 81.1% placebo, 21.1% certolizumab 200 mg, 21.1% certolizumab 400 mg. The ITT primary outcome at 24 weeks suggested a greater treatment effect for CZP compared to placebo than was the case before early escape.
Treatment effects may be overestimated for tocilizumab on ACR 20 and ACR 50Citation43 and on ACR 70.Citation43,Citation52 Infliximab treatment effects may be underestimated for ACR 20 and ACR 70.Citation53,Citation69 For ACR 50, two studiesCitation53,Citation69 underestimated the treatment effect, and one studyCitation68 provided an overestimate. For adalimumab, the effect may be an underestimate for ACR 50 and 70.Citation62 For ACR 20, one study may have underestimated the adalimumab effectCitation62 and another overestimated it.Citation71 The treatment effect of abatacept on ACR 20 may be an underestimate.Citation66 There were no etanercept studies that were outliers on the funnel plots, suggesting that the treatment effects for etanercept were within the bounds of what might be expected.
The assumption of consistency between the direct and indirect evidence could not be assessed formally in the combination analyses, as there were no independent loops of evidence in the network: for ACR outcomes, there was only one studyCitation69 that compared one licensed-treatment combination (infliximab) directly to another (abatacept) head-to-head. The combination network was comprised solely of indirect comparisons via MTX/DMARD. However, the results of direct meta-analyses and of the indirect Bucher were compared to base case results from the NMA to gauge consistency. For example, etanercept vs DMARD direct (data from etanercept vs DMARD trials only) was compared to etanercept vs DMARD as estimated by the NMA, and etanercept vs other bDMARDs indirect (as no head-to-head data) was compared to etanercept vs other bDMARDs as estimated by the NMA. The NMA had a wider confidence interval compared to the direct estimates from head-to-head trials: when comparing confidence intervals, the lower bounds were similar but the NMA estimated a much higher upper bound. Similarly, there is more uncertainty (in favor of etanercept) in the NMA estimates of etanercept versus the other licensed combinations compared to the estimates obtained from the Bucher indirect comparison. In the monotherapy analyses, one loop of evidence was present in the network, enabling a formal test of the consistency assumption. This test indicated that the direct and indirect treatment-effect estimates were not statistically significantly different, indicating that the consistency assumption held.
The relative treatment-effect estimates observed in our NMA were not influenced by any prior distribution estimates, as noninformative priors were used, meaning that prior to the data being applied, any result was taken to be equally likely, and that the posterior results were driven by the data. Model selection in our NMA was based on the best model fit, as indicated by the lowest DIC and average residual deviance values.
Regarding the heterogeneity observed among studies in the network, it may be argued that this might present a challenge to the similarity assumption. It does, however, better support the external validity of these NMA results: this variation in patient populations is more likely to reflect real-world practice.
Our outcome measure was ACR response, a good shortterm measure of disease response that is widely reported in clinical trials of RA. Other measures, such as the HAQ, might be more relevant for longer-term progression measurement. However, HAQ is not so broadly reported and is not as sensitive in measuring short-term changes in RA symptoms.
Our data relate to the population of adult patients with active, moderate–severe RA who have failed on or had an inadequate response to MTX or other conventional DMARDs. In these patients, the treatments evaluated were effective. In relation to other NMAs, our data illustrate that evidence from the different TNF-α inhibitors should not be combined together in meta-analyses, because efficacy differs between drugs in this class. Etanercept is a fusion protein including a soluble fragment of human p75-soluble TNF receptor and human immunoglobulin G1, whereas adalimumab and infliximab are MAbs directed against TNF. Differences in the kinetics and mode of action between etanercept and the MAbs have been reported,Citation88 and these differences may provide a plausible biological rationale for the differences in treatment-effect estimates observed in our NMA. Differences in the findings of published NMAs of biological DMARDs in RA have been reviewed and attributed to methodological shortcomings and inconsistencies.Citation89 Our NMA was performed incorporating many of the recommended criteria,Citation89 for a high-quality NMA including clear statement of the population (DMARD-MTX-inadequate responders, as distinct from TNF-α-inadequate responders, or DMARD- or MTX-naïve populations), analyzing monotherapy and combination therapy in separate networks (thereby avoiding lumping of mono- and combination therapy without controlling for concomitant DMARD use), exploring heterogeneity and effect modification by covariate analyses, and examining the influence of particular trials or sets of trials by sensitivity analyses.
Our data do not address treatment effects in the population of patients who have failed TNF-α treatment, as this is a later stage in the treatment pathway. Likewise, further review work would be required to gain treatment-effect estimates for bDMARDs in a moderate-RA population, which implies introducing bDMARDs at an earlier stage. Future NMAs, whilst mindful of the risk of multiplicity, should consider covariate adjustment for the number of prior DMARD treatments, C-reactive protein, or baseline HAQ, if sufficient data are available.
Supplementary materials
Table S1. Direct meta-analysis of American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 outcomes: combination therapy
Table S2. Bucher indirect meta-analysis of American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 outcomes: combination therapy
Table S3. Results from combination therapy NMA study arm level (patient characteristics) covariate analysis for American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 end point
Table S4. Combination therapy network meta-analysis sensitivity analysis results for American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 end point
Table S5. Direct meta-analysis of American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 outcomes: licensed DMARD monotherapy versus placebo in DMARD-experienced patients
Table S6. Bucher indirect meta-analysis of American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 outcomes: licensed DMARD monotherapy in DMARD-experienced patients
Table S7. Direct and indirect meta-analysis of ACR50 on Tocilizumab 4 mg/kg/4 weeks—Tocilizumab 8 mg/kg/4 weeks loop
Table S8. Direct and indirect meta-analysis of ACR20 on Tocilizumab 4 mg/kg/4 weeks—Tocilizumab 8 mg/kg/4 weeks loop
Table S9. Direct and indirect meta-analysis of ACR70 on Tocilizumab 4 mg/kg/4 weeks—Tocilizumab 8 mg/kg/4 weeks loop
Table S10. Monotherapy network meta-analysis sensitivity analysis results for American College of Rheumatology (ACR) criteria scores of 20, 50, and 70 end point
Figure S1. Part of the monotherapy evidence network containing the tocilizumab 4 mg/kg/4 weeks–tocilizumab 8 mg/kg/4 weeks loop.
Notes: 6, Maini 2006 (CHARISMA); 10, Nishimoto 2004 (STREAM); 11, Nishimoto 2009 (SATORI).
Disclosure
This study was sponsored by Pfizer Ltd, UK. Michelle Orme, Katherine MacGilchrist, and Stephen Mitchell were paid consultants to Pfizer Ltd, UK in connection with this study. Dean Spurden and Alex Bird are paid employees of Pfizer Ltd, UK.
References
- LeeDMWeinblattMERheumatoid arthritisLancet2001358928590391111567728
- SymmonsDTurnerGWebbRThe prevalence of rheumatoid arthritis in the United Kingdom: new estimates for a new centuryRheumatology (Oxford)200241779380012096230
- AlishiriGHBayatNSalimzadehAHealth-related quality of life and disease activity in rheumatoid arthritisJ Res Med Sci201116789790322279457
- SmithHSSmithARSeidnerPPainful rheumatoid arthritisPain Physician2011145E427E45821927056
- StrandVSharpVKoenigASComparison of health-related quality of life in rheumatoid arthritis, psoriatic arthritis and psoriasis and effects of etanercept treatmentAnn Rheum Dis20127171143115022258482
- BoonenAMauWThe economic burden of disease: comparison between rheumatoid arthritis and ankylosing spondylitisClin Exp Rheumatol2009274 Suppl 55S112S11719822056
- FosterWCarruthersDLipGYBlannADInflammatory cytokines, endothelial markers and adhesion molecules in rheumatoid arthritis: effect of intensive anti-inflammatory treatmentJ Thromb Thrombolysis201029443744219578810
- ThwaitesCFinneyARheumatoid arthritis. 2: Exploring treatment options to achieve early control and remissionNurs Times201010610182020426296
- National Institute for Health and Clinical ExcellenceRheumatoid arthritis (CG79): full guidelineLondon, UKNICE2009 Available from: http://guidance.nice.org.uk/CG79/GuidanceAccessed October 30, 2012
- FriesJFSpitzPKrainesRGHolmanHRMeasurement of patient outcome in arthritisArthritis Rheum19802321371457362664
- SmolenJSLandeweRBreedveldFCEULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugsAnn Rheum Dis201069696497520444750
- ChenYFJobanputraPBartonPA systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectivenessHealth Technol Assess20061042iiiivxixiii1229
- MaxwellLJSinghJAAbatacept for rheumatoid arthritis: a Cochrane systematic reviewJ Rheumatol201037223424520080922
- Navarro-SarabiaFAriza-ArizaRHernandez-CruzBVillanuevaIAdalimumab for treating rheumatoid arthritisJ Rheumatol20063361075108116652437
- BlumenauerBJuddMCranneyAEtanercept for the treatment of rheumatoid arthritisCochrane Database Syst Rev20034CD00452514584021
- SinghJANoorbaloochiSSinghGGolimumab for rheumatoid arthritis: a systematic reviewJ Rheumatol20103761096110420436075
- BlumenauerBJuddMWellsGInfliximab for the treatment of rheumatoid arthritisCochrane Database Syst Rev20023CD00378512137712
- SinghJAChristensenRWellsGABiologics for rheumatoid arthritis: an overview of Cochrane reviewsSao Paulo Med J2010128530931021181074
- SinghJABegSLopez-OlivoMATocilizumab for rheumatoid arthritis: a Cochrane systematic reviewJ Rheumatol2011381102020952462
- Canadian Agency for Drugs and Technologies in HealthClinical and Economic Overview: Biological Response Modifier Agents for Adults with Rheumatoid ArthritisOttawa, ONCADTH2010 Available from: http://www.cadth.ca/media/pdf/TR_RA_Clinical_and_Economic_Overview_e.pdfAccessed May 2, 2012
- ClinicalTrialsgov [homepage on the Internet]US National Institutes of Health Available from: http://clinicaltrials.govAccessed April 11, 2012
- National Institute for Health and Clinical ExcellenceAppendix D: Methodology checklist – randomised controlled trialsLondon, UKNICE2009 Available from: http://www.nice.org.uk/media/633/21/The_guidelines_manual_2009_-_Appendix_D_Methodology_checklist_-_randomised_controlled_trials.pdfAccessed October 30, 2012
- SuttonAJDuvalSJTweedieRLAbramsKRJonesDREmpirical assessment of effect of publication bias on meta-analysesBMJ200032072491574157710845965
- EggerMDavey SmithGSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBMJ199731571096296349310563
- HigginsJPTDeeksJJAltmanDGIntention-to-treat issues for dichotomous dataCochrane Handbook for Systematic Reviews of InterventionsChichester, UKJohn Wiley & Sons2009
- HarrisRBradburnMDeeksJJHarbordRAltmanDGSterneJMetan: fixed- and random-effects meta-analysisStata J200881328
- [No authors listed]Software updates (Metan)Stata J200884594
- BucherHCGuyattGHGriffithLEWalterSDThe results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trialsJ Clin Epidemiol19975066836919250266
- GlennyAMAltmanDGSongFIndirect comparisons of competing interventionsHealth Technol Assess20059261134iiiiv16014203
- CaldwellDMAdesAEHigginsJPSimultaneous comparison of multiple treatments: combining direct and indirect evidenceBMJ2005331752189790016223826
- SuttonAAdesAECooperNAbramsKUse of indirect and mixed treatment comparisons for technology assessmentPharmacoeconomics200826975376718767896
- LuGAdesAECombination of direct and indirect evidence in mixed treatment comparisonsStat Med200423203105312415449338
- The BUGS project, MRC Biostatistics UnitBayesian Inference Using Gibbs Sampling (BUGS) project. WinBUGS 1.4.3 Available from: http://www.mrc-bsu.cam.ac.uk/bugs/winbugs/contents.shtmlAccessed October 30, 2012
- SpiegelhalterDJAbramsKRMylesJPBayesian Approaches to Clinical Trials and Health Care EvaluationChichester, UKJohn Wiley & Sons2004
- SuttonAJAbramsKRBayesian methods in meta-analysis and evidence synthesisStat Methods Med Res200110427730311491414
- The BUGS ProjectWinbugs 1.4 beta versionNew examples for WinBUGS Available from: http://www.mrc-bsu.cam.ac.uk/bugs/winbugs/examples.shtmlAccessed October 30, 2012
- DiasSWeltonNSuttonAAdesAENICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analyisis of randomised controlled trialsLondon, UKNICE2011 Available from: http://www.nicedsu.org.uk/Evidence-Synthesis-TSD-series(2391675).htm
- DiasSWeltonNJSuttonAJAdesAENICE DSU technical support document 5: evidence synthesis in the baseline natural history modelLondon, UKNICE2011 Available from: http://www.nicedsu.org.uk/Evidence-Synthesis-TSD-series(2391675).htm
- HasselbladVMeta-analysis of multitreatment studiesMed Decis Making199818137439456207
- GelmanAPrior distributions for variance parameters in heirarchical modelsBayesian Anal200613515533
- HigginsJPTDeeksJJAltmanDGSpecial topics in statistics: rare events. Studies with zero-cell countsCochrane Handbook for Systematic Reviews of InterventionsChichester, UKJohn Wiley & Sons2009
- CombeBCodreanuCFioccoUEtanercept and sulfasalazine, alone and combined, in patients with active rheumatoid arthritis despite receiving sulfasalazine: a double-blind comparisonAnn Rheum Dis200665101357136216606651
- GenoveseMCMcKayJDNasonovELInterleukin-6 receptor inhibition with tocilizumab reduces disease activity in rheumatoid arthritis with inadequate response to disease-modifying antirheumatic drugs: the tocilizumab in combination with traditional disease-modifying antirheumatic drug therapy studyArthritis Rheum200858102968298018821691
- KeystoneEHeijdeDMasonDJrCertolizumab pegol plus methotrexate is significantly more effective than placebo plus methotrexate in active rheumatoid arthritis: findings of a fifty-two-week, phase III, multicenter, randomized, double-blind, placebo-controlled, parallel-group studyArthritis Rheum200858113319332918975346
- SmolenJLandeweRBMeasePEfficacy and safety of certolizumab pegol plus methotrexate in active rheumatoid arthritis: the RAPID 2 study. A randomised controlled trialAnn Rheum Dis200968679780419015207
- KamedaHUekiYSaitoKEtanercept (ETN) with methotrexate (MTX) is better than ETN monotherapy in patients with active rheumatoid arthritis despite MTX therapy: a randomized trialMod Rheumatol201020653153820574649
- van RielPLTaggartAJSanyJEfficacy and safety of combination etanercept and methotrexate versus etanercept alone in patients with rheumatoid arthritis with an inadequate response to methotrexate: the ADORE studyAnn Rheum Dis200665111478148316464988
- GenoveseMCCohenSMorelandLCombination therapy with etanercept and anakinra in the treatment of patients with rheumatoid arthritis who have been treated unsuccessfully with methotrexateArthritis Rheum20045051412141915146410
- KremerJMWesthovensRLeonMTreatment of rheumatoid arthritis by selective inhibition of T-cell activation with fusion protein CTLA4IgN Engl J Med2003349201907191514614165
- KremerJRitchlinCMendelsohnAGolimumab, a new human anti-tumor necrosis factor alpha antibody, administered intravenously in patients with active rheumatoid arthritis: forty-eight-week efficacy and safety results of a phase III randomized, double-blind, placebo-controlled studyArthritis Rheum201062491792820131276
- MainiRNTaylorPCSzechinskiJDouble-blind randomized controlled clinical trial of the interleukin-6 receptor antagonist, tocilizumab, in European patients with rheumatoid arthritis who had an incomplete response to methotrexateArthritis Rheum20065492817282916947782
- SmolenJSBeaulieuARubbert-RothAEffect of interleukin-6 receptor inhibition with tocilizumab in patients with rheumatoid arthritis (OPTION study): a double-blind, placebo-controlled, randomised trialLancet2008371961798799718358926
- ZhangFCHouYHuangFInfliximab versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a preliminary study from ChinaInt J Rheum Dis200692127130
- KlareskogLvan der HeijdeDde JagerJPTherapeutic effect of the combination of etanercept and methotrexate compared with each treatment alone in patients with rheumatoid arthritis: double-blind randomised controlled trialLancet2004363941067568115001324
- PfizerTEMPO CSR 36848. 24-week data, Table 9.4.2.2AData on file
- CooperNJSuttonAJLuGKhuntiKMixed comparison of stroke prevention treatments in individuals with nonrheumatic atrial fibrillationArch Intern Med2006166121269127516801509
- The BUGS ProjectDIC: deviance information criterion Available from: http://www.mrc-bsu.cam.ac.uk/bugs/winbugs/dicpage.shtmlAccessed October 30, 2012
- AbeTTakeuchiTMiyasakaNA multicenter, double-blind, randomized, placebo controlled trial of infliximab combined with low dose methotrexate in Japanese patients with rheumatoid arthritisJ Rheumatol2006331374416395748
- ChenDYChouSJHsiehTYRandomized, double-blind, placebo-controlled, comparative study of human anti-TNF antibody adalimumab in combination with methotrexate and methotrexate alone in Taiwanese patients with active rheumatoid arthritisJ Formos Med Assoc2009108431031919369178
- DurezPNzeusseu ToukapALauwerysBRA randomised comparative study of the short term clinical and biological effects of intravenous pulse methylprednisolone and infliximab in patients with active rheumatoid arthritis despite methotrexate treatmentAnn Rheum Dis20046391069107415308515
- EmeryPDeodharARigbyWFEfficacy and safety of different doses and retreatment of rituximab: a randomised, placebo-controlled trial in patients who are biological naive with active rheumatoid arthritis and an inadequate response to methotrexate (Study Evaluating Rituximab’s Efficacy in MTX iNadequate rEsponders (SERENE))Ann Rheum Dis20106991629163520488885
- HuangFZhangFCBaoCDAdalimumab plus methotrexate for the treatment of rheumatoid arthritis: a multi-center randomized, double-blind, placebo-controlled clinical studyZhonghua Nei Ke Za Zhi20094811916921 Chinese20079321
- KayJMattesonELDasguptaBGolimumab in patients with active rheumatoid arthritis despite treatment with methotrexate: a randomized, double-blind, placebo-controlled, dose-ranging studyArthritis Rheum200858496497518383539
- KeystoneECSchiffMHKremerJMOnce-weekly administration of 50 mg etanercept in patients with active rheumatoid arthritis: results of a multicenter, randomized, double-blind, placebo-controlled trialArthritis Rheum200450235336314872476
- KimHYLeeSKSongYWA randomized, double-blind, placebo-controlled, phase III study of the human anti-tumor necrosis factor antibody adalimumab administered as subcutaneous injections in Korean rheumatoid arthritis patients treated with methotrexateInt J Rheum Dis2007101916
- KremerJMGenantHKMorelandLWEffects of abatacept in patients with methotrexate-resistant active rheumatoid arthritis: a randomized trialAnn Intern Med20061441286587616785475
- LanJLChouSJChenDYChenYHHsiehTYYoungMJrA comparative study of etanercept plus methotrexate and methotrexate alone in Taiwanese patients with active rheumatoid arthritis: a 12-week, double-blind, randomized, placebo-controlled studyJ Formos Med Assoc2004103861862315340661
- MainiRSt ClairEWBreedveldFInfliximab (chimeric anti-tumour necrosis factor alpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomised phase III trial. ATTRACT Study GroupLancet199935491941932193910622295
- SchiffMKeisermanMCoddingCEfficacy and safety of abatacept or infliximab vs placebo in ATTEST: a phase III, multi-centre, randomised, double-blind, placebo-controlled study in patients with rheumatoid arthritis and an inadequate response to methotrexateAnn Rheum Dis20086781096110318055472
- WeinblattMEKremerJMBankhurstADA trial of etanercept, a recombinant tumor necrosis factor receptor:Fc fusion protein, in patients with rheumatoid arthritis receiving methotrexateN Engl J Med199934042532599920948
- WeinblattMEKeystoneECFurstDEAdalimumab, a fully human anti-tumor necrosis factor alpha monoclonal antibody, for the treatment of rheumatoid arthritis in patients taking concomitant methotrexate: the ARMADA trialArthritis Rheum2003481354512528101
- WesthovensRYocumDHanJThe safety of infliximab, combined with background treatments, among patients with rheumatoid arthritis and various comorbidities: a large, randomized, placebo-controlled trialArthritis Rheum20065441075108616572442
- JohnsenAKSchiffMHMeasePJComparison of 2 doses of etanercept (50 vs 100 mg) in active rheumatoid arthritis: a randomized double blind studyJ Rheumatol200633465966416482646
- MiyasakaNClinical investigation in highly disease-affected rheumatoid arthritis patients in Japan with adalimumab applying standard and general evaluation: the CHANGE studyMod Rheumatol200818325226218330677
- MorelandLWSchiffMHBaumgartnerSWEtanercept therapy in rheumatoid arthritis. A randomized, controlled trialAnn Intern Med1999130647848610075615
- NishimotoNMiyasakaNYamamotoKStudy of active controlled tocilizumab monotherapy for rheumatoid arthritis patients with an inadequate response to methotrexate (SATORI): significant reduction in disease activity and serum vascular endothelial growth factor by IL-6 receptor inhibition therapyMod Rheumatol2009191121918979150
- NishimotoNYoshizakiKMiyasakaNTreatment of rheumatoid arthritis with humanized anti-interleukin-6 receptor antibody: a multicenter, double-blind, placebo-controlled trialArthritis Rheum20045061761176915188351
- van de PutteLBAtkinsCMalaiseMEfficacy and safety of adalimumab as monotherapy in patients with rheumatoid arthritis for whom previous disease modifying antirheumatic drug treatment has failedAnn Rheum Dis200463550851615082480
- van de PutteLBARauRBreedveldFCEfficacy and safety of the fully human anti-tumour necrosis factor a monoclonal antibody adalimumab (D2E7) in DMARD refractory patients with rheumatoid arthritis: a 12 week, phase II studyAnn Rheum Dis200362121168117714644854
- MorelandLWBaumgartnerSWSchiffMHTreatment of rheumatoid arthritis with a recombinant human tumor necrosis factor receptor (p75)-Fc fusion proteinN Engl J Med199733731411479219699
- EdwardsJCSzczepanskiLSzechinskiJEfficacy of B-cell-targeted therapy with rituximab in patients with rheumatoid arthritisN Engl J Med2004350252572258115201414
- KeystoneECGenoveseMCKlareskogLGolimumab, a human antibody to tumour necrosis factor {alpha} given by monthly subcutaneous injections, in active rheumatoid arthritis despite methotrexate therapy: the GO-FORWARD StudyAnn Rheum Dis200968678979619066176
- FleischmannRVencovskyJvan VollenhovenRFEfficacy and safety of certolizumab pegol monotherapy every 4 weeks in patients with rheumatoid arthritis failing previous disease-modifying antirheumatic therapy: the FAST4WARD studyAnn Rheum Dis200968680581119015206
- NishimotoNMiyasakaNYamamotoKKawaiSTakeuchiTAzumaJLong-term safety and efficacy of tocilizumab, an anti-IL-6 receptor monoclonal antibody, in monotherapy, in patients with rheumatoid arthritis (the STREAM study): evidence of safety and efficacy in a 5-year extension studyAnn Rheum Dis200968101580158419019888
- BergmanGJDHochbergMCBoersMWintfeldNKielhornAJansenJPIndirect comparison of tocilizumab and other biologic agents in patients with rheumatoid arthritis and inadequate response to disease-modifying antirheumatic drugsSemin Arthritis Rheum201039642544120223500
- National Institute for Health and Clinical ExcellenceRheumatoid arthritis – adalimumab, etanercept and infliximab (TA130)London, UKNICE2007 Available from: http://guidance.nice.org.uk/TA130Accessed October 30, 2012
- National Institute for Health and Clinical ExcellenceRheumatoid arthritis (after the failure of previous anti-rheumatic drugs) – golimumab (TA225)London, UKNICE2011 Available from: http://guidance.nice.org.uk/TA225Accessed October 30, 2012
- TraceyDKlareskogLSassoEHSalfeldJGTakPPTumor necrosis factor antagonist mechanisms of action: a comprehensive reviewPharmacol Ther2008117224427918155297
- ThorlundKDruytsEAvina-ZubietaJAWuPMillsEWhy the findings of published multiple treatment comparison meta-analyses of biologic treatments for rheumatoid arthritis are different: an overview of recurrent methodological shortcomingsAnn Rheum Dis Epub October 20, 2012