
Abstract
Purpose
The long-term complications of colon cancer surgery are now being investigated to a greater extent given the improvement in survival rates for all stages of colon and rectal cancer. Patient quality of life is now playing a significant role in the cancer survivorship and sexual complications are part of that survivorship spectrum.
Patients and Methods
A sexual health questionnaire (EORTC SHQ-22©) was employed to perform an audit of the sexual complications following surgery. Ethics approval was obtained from the university of Saskatchewan and a telephonic interview was conducted. This was pre-empted by a telephonic consent script by our medical office assistant.
Results
Twenty-two percent of the patients were deceased, and 52% of the patients could not be reached telephonically. The rates of sexual complications were well within the published rates from tertiary centers employing colorectal specialists.
Discussion
Sexual complications are a newer form of complications given the proximity of the pelvic parasympathetic plexus to the sacral promontory. The complication rates for our community surgeons are equivalent to that of colorectal specialists from tertiary centres. Further explanation of the sexual complication risks should form part of the discussion for all surgeons undertaking colon or rectal surgery.
Limitation
The lack of documented pre-operative sexual dysfunction and a small patient cohort hampered the findings of this study.
Conclusion
The sexual complication rates at our institute are well within published rates of sexual dysfunction, post colonic and rectal surgery.
Introduction
The long-term survivorship of colorectal cancer patients has increased in the past decade due to a multitude of factors. These include better patient selection, minimally invasive surgical techniques, and a combination of adjuvant therapies. The five-year survivorship has increased for all stages of colorectal cancer to the extent that the concept of cancer as a chronic disease is now a reality.Citation1–3 This has led to an increasing awareness of the long-term complications of colorectal cancer surgery. At the forefront of this is the patient`s quality of life through oncological remission. Concepts such as daily activities of living and sexual function are now being discussed in an open forum.Citation4 Sexuality has an important role in quality of life as most studies show that colorectal cancer patients remain sexually active post-treatment. Sexual function in cancer survivors can affect a patient’s self-perception as well as their partner’s.Citation2,Citation4 The etiology of sexual dysfunction has been attributed to pelvic autonomic nerve damage. This includes the inferior mesenteric plexus, superior hypogastric plexus, hypogastric nerves, and pelvic plexus.Citation1,Citation5,Citation6 The pathophysiology involves poor surgical technique, radiotherapy, or post-operative inflammation and fibrosis that incorporates the autonomic nerves. The majority of studies involving sexual function are often from tertiary centers involving colorectal specialists. Ours is one of the first studies to look at the sexual outcomes in a community hospital involving community general surgeons who perform colorectal cancer surgery. This was a retrospective audit to investigate if the long-term complications are on par with published rates from tertiary centers. We believe this is the first audit of its kind in rural Canada.
Materials and Methods
This was a retrospective audit that involved obtaining ethics approval from the University of Saskatchewan and a sexual health questionnaire. Approval from the ethics committee and the Division of General Surgery was obtained. All data from patients who underwent surgery for left-sided colorectal cancer in Prince Albert, Saskatchewan between 2011 and 2021 was analyzed. A medical office assistant then made initial contact with the patient in the form of a telephone consent script . We then interviewed the patients who agreed to participate in the study.
Figure 1 Telephone consent script.
This was initially approved by the University of Saskatchewan ethics committee prior to initiation.
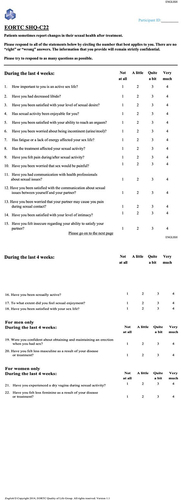
Approval was obtained from the European Organisation for Research and Treatment of Cancer (EORTC) to use their EORTC SHQ-22© sexual quality of life questionnaire . This questionnaire was developed to assess the sexual health in male and female cancer survivors. This is a cross-culturally validated measure that can be used to assess the sexual health of cancer patients in clinical trials as well as in clinical practice. The breakdown of patients is distributed in . This study complies with the framework of ethical guidelines set out in the Declaration of Helsinki. Ethics approval was obtained from the ethics committee at the University of Saskatchewan, protocol number BIO-1018.
Table 1 Breakdown of Patients and Respondents
Figure 2 EORTC SHQ-22 sexual quality of life questionnaire.
Results
Discussion
It is important to acknowledge that this survey is merely a snapshot into the lives of our colorectal cancer survivors and not an attempt to define their post-surgical quality of life in terms of sexual complications. The questions answered related to the preceding four weeks post-surgery and the duration between survey completion and their actual completion of surgical and oncological therapy varied greatly. It is therefore difficult to estimate the actual effects of the treatment paradigm given the discrepancy in this time period for the various patients interviewed.
Forty-seven percent of the patients still feel that a sex life was an important part of their lives (). Sixty-six percent did not report a drop in their sexual libido post cancer surgery and adjuvant therapy (). Fifty-five percent of the respondents reported being satisfied with their level of sexual desire (). Fifty-four percent reported being satisfied with their level of sexual activity (). This study did not have the depth to focus and assess specific sexual dysfunctions, pathologies or subgroups of men or women. It is more of an overview about the topic of sexual function and health of patients undergoing colorectal surgery for malignancy. Deceased patients made up 22% of our patient cohort ().
Figure 3 Question 1.
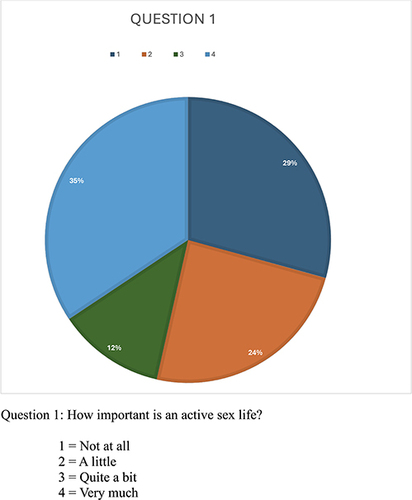
Figure 4 Question 2.
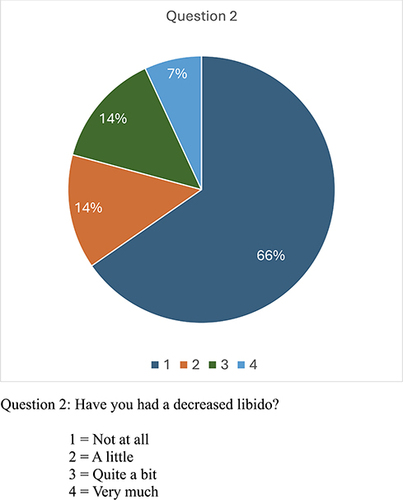
Figure 5 Question 3.
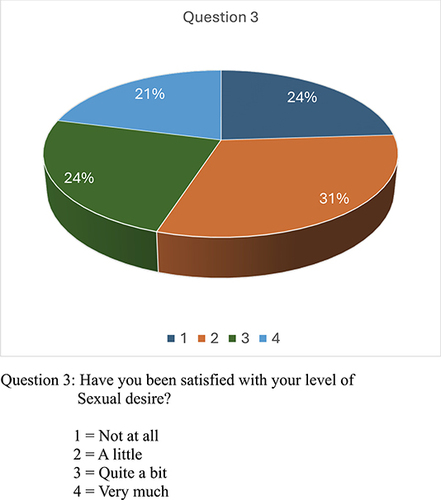
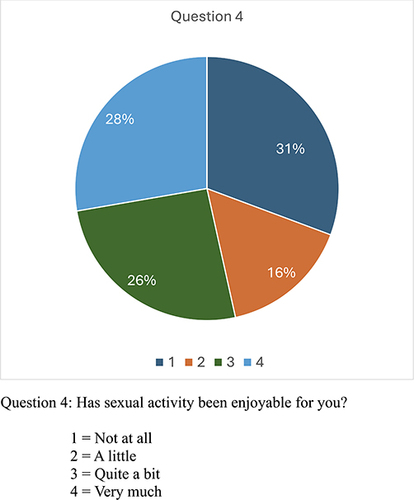
Figure 6 Question 4.
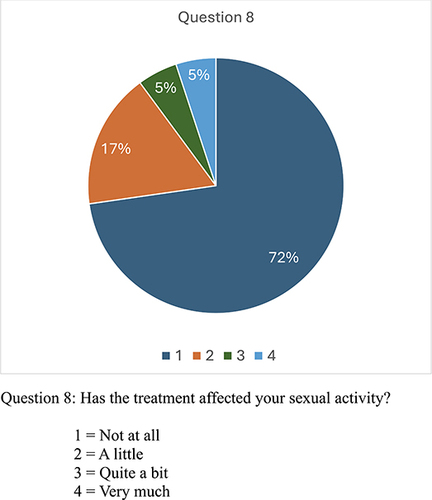
Sixteen percent and 19% of the respondents had issues with sexual orgasm and urinary and stool incontinence ( and ). This is far lower than recently published rates from tertiary centres.Citation7,Citation8 Sixty percent felt their lack of energy did not affect their sex life (), while 72% felt the surgical and oncological treatment they underwent did not affect their sexual activity (). The type of surgeries included were not limited to the pelvis and while we looked at left sided colonic and rectal surgeries, right hemicolectomies are also linked to sexual dysfunction (). Apart from the sympathetic and parasympathetic nerve involvement, the psychological factors of sexual dysfunction includes stress, the presence of cancer, body dysmorphism due to a potential stoma, pre-surgical relationship issues, the various types of adjuvant therapy and their associated side effects.Citation9–11 To be able to determine a specific etiology is beyond the scope of our article.
Table 2 Types of Surgeries and Anastomosis
Figure 7 Question 5.
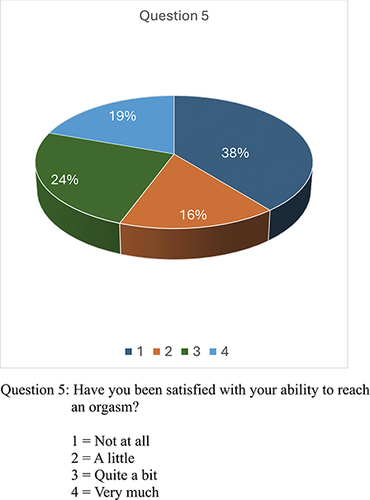
Figure 8 Question 6.
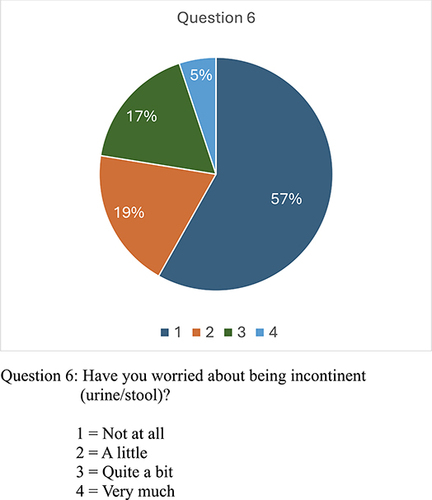
Figure 9 Question 7.
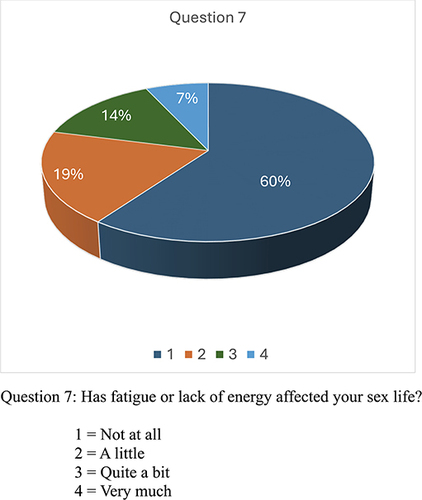
Figure 10 Question 8.
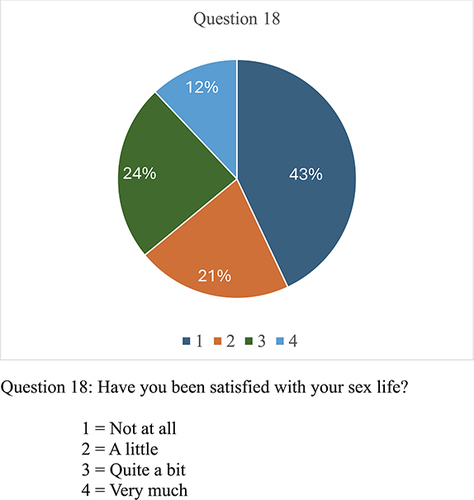
Four percent of the patients experienced pain during or after intercourse () and 95% of the respondents did not have a fear of dyspareunia (). Ninety-eight percent of the patients did not contact a health professional about their sexual issues post-surgery and 50% were not happy about communicating their concerns with their intimate partner ( and ). Given our demographics in rural Canada with an overall conservative ethos, these findings are not surprising. Ninety-seven percent did not report a fear of intimate partner dyspareunia (), and 34% were not happy with their level of intimacy with their sexual partner ().16% of respondents felt insecure about their ability to satisfy their partner sexually (). Sixty-four percent of the patients were sexually active in the past month prior to answering the questionnaire (). Fifty-five percent of the respondents did not experience sexual enjoyment in the last month, while four percent enjoyed it very much ().36% of respondents felt satisfied with their overall sex life ().
Figure 11 Question 9.
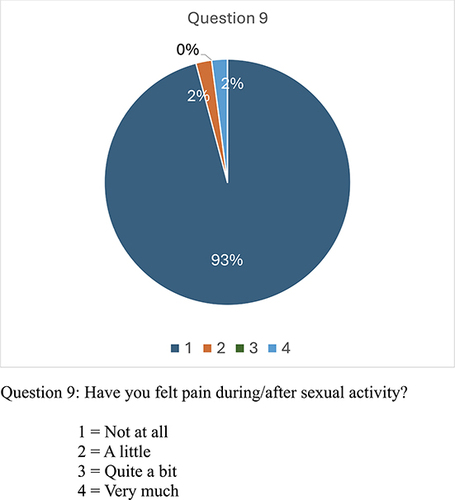
Figure 12 Question 10.
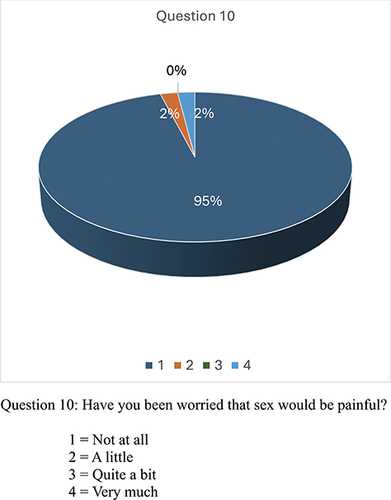
Figure 13 Question 11.
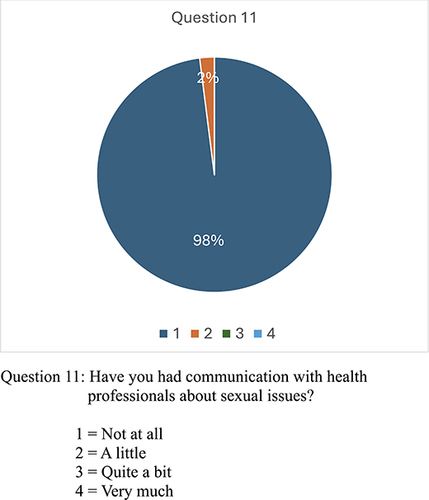
Figure 14 Question 12.
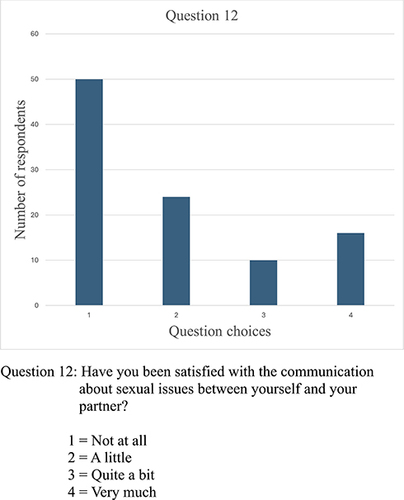
Figure 15 Question 13.
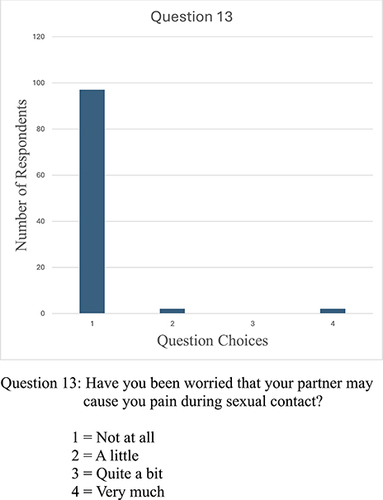
Figure 16 Question 14.
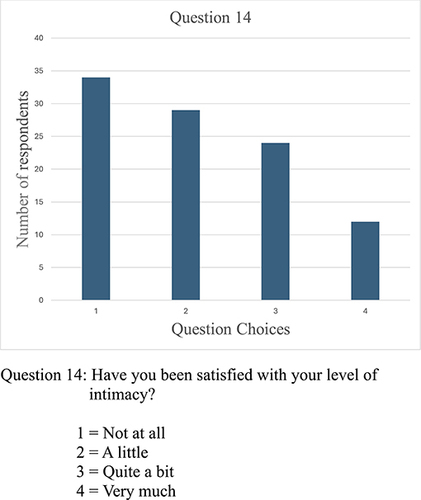
Figure 17 Question 15.
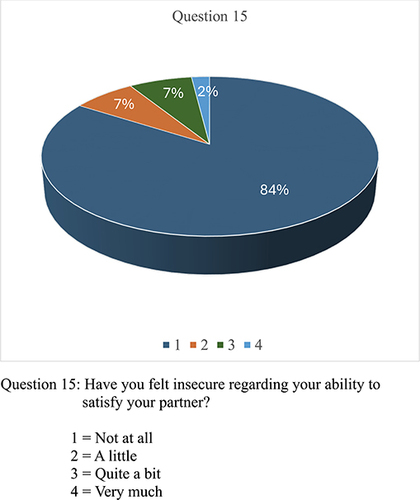
Figure 18 Question 16.
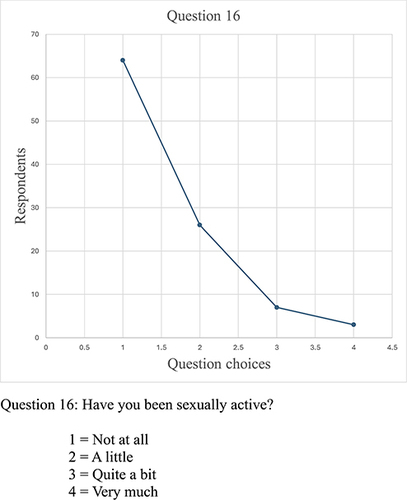
Figure 19 Question 17.
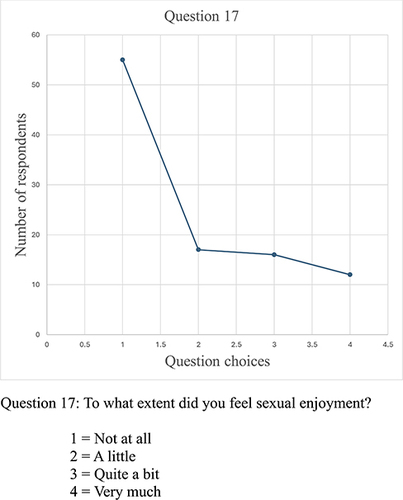
Figure 20 Question 18.
A shortcoming of our study was the inability to document the underlying sexual dysfunction prior to the cancer diagnosis and treatment. Documented pre-operative sexual dysfunction would further reduce the incidence of the reported sexual dysfunction via the EORTC SHQ-22 questionnaire.Citation12,Citation13 A second issue is the inability to validate the patient responses as the interviews were conducted telephonically.
A personal interview would have allowed us to gauge the emotional response to the questions as well to exclude any underlying anxiety or reticence in the respondents. This study is severely underpowered through the small patient cohort and what is needed in the future is a multicentered prospective audit with documented preoperative rates of sexual function.Citation12,Citation13 This will also help to eliminate selection bias as the patients questioned were all cancer survivors at the time of the audit. The sexual dysfunction of deceased patients was not known and therefore difficult to determine if this would have skewed our findings in a positive or negative manner.
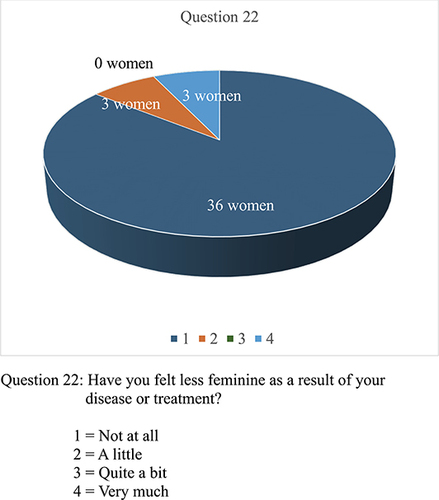
Fifty-one percent of the males did not feel confident about maintaining an erection during intercourse but 88% of the males said that their masculinity was not affected by the treatment they underwent ( and ). This is in keeping with previous studies.Citation14 Sixty-five percent of the female respondents did not report vaginal dryness during intercourse, similar to published outcomes.Citation12 Eighty-six percent did not feel less feminine because of the treatment they underwent ( and ). Similar percentages of males and females (88% vs 86%) reported that their sexuality was unaffected by their treatment.Citation14 This may be due to the elderly patient cohort and the relevance of current sexual activity in their lives. Certainly, this opinion could change in patients with hereditary colorectal cancer seen in younger patients in their twenties and thirties.Citation15,Citation16
Figure 21 Question 19.
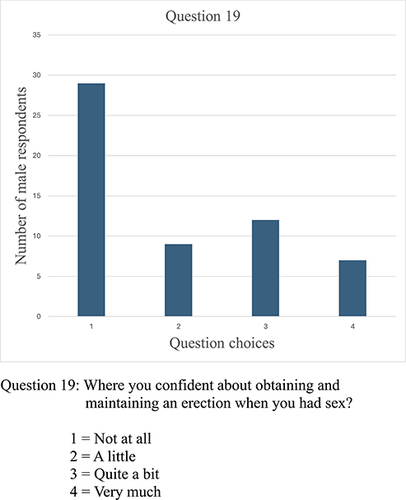
Figure 22 Question 20.
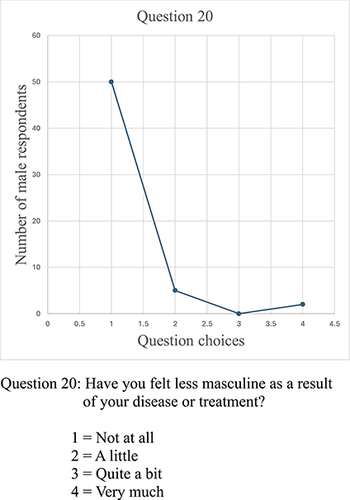
Figure 23 Question 21.
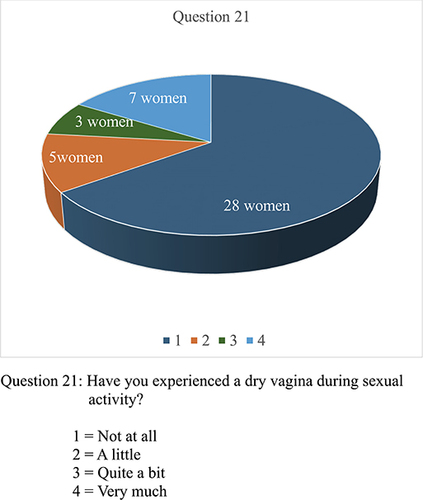
Figure 24 Question 22.
Fifty-seven percent of the patients had undergone previous abdominal operations , increasing the complexity of surgery and therefore the risk of nerve damage due to intra-abdominal adhesions. A handsewn anastomosis performed in 25% of the surgeries was not shown to be a risk factor. The inability to derive an active reference point also hampers the findings of our study. Age-related parameters of sexual dysfunction in a cancer-free population would need to be ascertained as a control group, representative of our local community, to derive a realistic baseline group for comparison with patients in our study.Citation13,Citation17 If the incidence of sexual dysfunction in our cancer group is similar to the control group, one could argue there is no significant effect of undergoing cancer treatment as regards sexual dysfunction in our surgical cohort.
A significant short coming of the study is the actual number of respondents that participated. Thirty-nine percent of the eligible patients answered the survey . Twenty-two percent were deceased ().
We were unable to contact 52% of the eligible respondents for the study. This is seen in other studies as well where obtaining the current phone number is the rate limiting step.Citation18,Citation19 This could have influenced the findings in the study. The transient population in northern Saskatchewan, with large numbers of migrant workers, may also have played a role in this.
A significant finding of our audit was the fact that none of the patients contacted, were even aware of the possibility of sexual dysfunction following colon and rectal surgery and their adjuvant therapy. Neither the surgeons nor the oncologists had broached this Discussion in either the pre- or post-treatment phases.Citation20,Citation21 This not only highlights but also perpetuates the reticence to identify but also treat this chronic complication in the management of colorectal cancer patients.
Whether this will continue to be part of the surgical complication discussion and oncological remission effects remains to be seen. In previous studies, health care workers expressed the inability to have a significant discussion about sexual dysfunction in cancer patients.Citation2,Citation13 The use of tools such as sexual health questionnaires may serve to alleviate this issue.Citation22,Citation23
An encouraging aspect of this audit is that the documented rate of sexual dysfunction falls within published rates from tertiary centers. The colorectal cancer surgeries were undertaken by community general surgeons and to have similar outcomes to colorectal surgeons in tertiary centers is a testament to the quality of surgical work undertaken in rural Saskatchewan.
Limitations
This study remains underpowered due to the small patient cohort and the lack of documented, preoperative sexual dysfunction in our patients. The small number of telephonic respondents also serves to highlight the difficulty in surgical research in rural Saskatchewan.
The large transient population only serves to accentuate this problem.
Twenty-two percent of respondents were deceased at the time of the interview and fifty-two percent of eligible respondents could not be contacted. Their sexual complication rate could have skewed our results in a positive or negative way.
Conclusion
We present an audit of sexual complications following left sided colonic and rectal surgery in rural Saskatchewan. The documented complication rates, falls within recognized and published rates of colorectal surgeons in tertiary centers. This is a testament to the community surgeons in our hospital and the quality of surgical care delivered.
Ethics Statement
Ethics approval was obtained from the University of Saskatchewan ethics committee.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We would like to thank the members of the division of general surgery in the Victoria hospital, Prince Albert, Saskatchewan for their permission to access the data and support during the preparation of this manuscript. We also thank our medical office assistant, Ms. Kendall Leigh Kalinowski for her invaluable assistance during the telephonic interview process.
References
- Costa P, Cardoso JM, Louro H, et al. Impact on sexual function of surgical treatment in rectal cancer. Int Braz J Urol. 2018;44(1):141–149. PMID: 29219281; PMCID: PMC5815544. doi:10.1590/S1677-5538.IBJU.2017.0318
- Averyt JC, Nishimoto PW. Addressing sexual dysfunction in colorectal cancer survivorship care. J Gastrointest Oncol. 2014;5(5):388–394. PMID: 25276411; PMCID: PMC4173048. doi:10.3978/j.issn.2078-6891.2014.059
- Włodarczyk M, Sobolewska J, Nowak A, et al. Sexual dysfunctions following low anterior resection of the rectum in rectal cancer patients. Pol Przegl Chir. 2019;91(3):21–26. PMID: 31243171. doi:10.5604/01.3001.0013.1482
- Mercadante S, Vitrano V, Catania V. Sexual issues in early and late stage cancer: a review. Support Care Cancer. 2010;18(6):659–665. PMID: 20237806. doi:10.1007/s00520-010-0814-0
- Walsh PC, Mostwin JL. Radical prostatectomy and cystoprostatectomy with preservation of potency. Results using a new nerve-sparing technique. Br J Urol. 1984;56(6):694–697. PMID: 6534493. doi:10.1111/j.1464-410x.1984.tb06149.x
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;1(8496):1479–1482. PMID: 2425199. doi:10.1016/s0140-6736(86)91510-2
- Jones OM, John SK, Horseman N, Lawrance RJ, Fozard JB. Low anastomotic leak rate after colorectal surgery: a single-centre study. Colorectal Dis. 2007;9(8):740–744. PMID: 17477854. doi:10.1111/j.1463-1318.2007.01210.x
- Law WL, Choi HK, Lee YM, Ho JW. The impact of postoperative complications on long-term outcomes following curative resection for colorectal cancer. Ann Surg Oncol. 2007;14(9):2559–2566. PMID: 17522945. doi:10.1245/s10434-007-9434-4
- Li K, He X, Tong S, Zheng Y. Risk factors for sexual dysfunction after rectal cancer surgery in 948 consecutive patients: a prospective cohort study. Eur J Surg Oncol. 2021;47(8):2087–2092. PMID: 33832775. doi:10.1016/j.ejso.2021.03.251
- Eveno C, Lamblin A, Mariette C, Pocard M. Sexual and urinary dysfunction after proctectomy for rectal cancer. J Visc Surg. 2010;147(1):e21–30. PMID: 20587375. doi:10.1016/j.jviscsurg.2010.02.001
- Laohawiriyakamol S, Chewatanakornkul S, Wanichsuwan W, Ruangsin S, Sunpaweravong S, Bejrananda T. Urogenital dysfunction after laparoscopic surgery for rectal or sigmoid colon cancer. Asian J Surg. 2023;46(1):492–500. PMID: 35717291. doi:10.1016/j.asjsur.2022.06.004
- Den Oudsten BL, Traa MJ, Thong MS, et al. Higher prevalence of sexual dysfunction in colon and rectal cancer survivors compared with the normative population: a population-based study. Eur J Cancer. 2012;48(17):3161–3170. PMID: 22608772. doi:10.1016/j.ejca.2012.04.004
- Traa MJ, De Vries J, Roukema JA, Den Oudsten BL. Sexual (dys)function and the quality of sexual life in patients with colorectal cancer: a systematic review. Ann Oncol. 2012;23(1):19–27. PMID: 21508174. doi:10.1093/annonc/mdr133
- Ho VP, Lee Y, Stein SL, Temple LK. Sexual function after treatment for rectal cancer: a review. Dis Colon Rectum. 2011;54(1):113–125. PMID: 21160322. doi:10.1007/DCR.0b013e3181fb7b82
- Schmidt CE, Bestmann B, Kuchler T, Longo WE, Kremer B. Impact of age on quality of life in patients with rectal cancer. World J Surg. 2005;29(2):190–197. PMID: 15654662. doi:10.1007/s00268-004-7556-4
- Schmidt C, Daun A, Malchow B, Küchler T. Sexual impairment and its effects on quality of life in patients with rectal cancer. Dtsch Arztebl Int. 2010;107(8):123–130. PMID: 20300220; PMCID: PMC2840249. doi:10.3238/arztebl.2010.0123
- Milbury K, Cohen L, Jenkins R, Skibber JM, Schover LR. The association between psychosocial and medical factors with long-term sexual dysfunction after treatment for colorectal cancer. Support Care Cancer. 2013;21(3):793–802. PMID: 22948439; PMCID: PMC4437688. doi:10.1007/s00520-012-1582-9
- Ledebo A, Bock D, Prytz M, Haglind E, Angenete E. Urogenital function 3 years after abdominoperineal excision for rectal cancer. Colorectal Dis. 2018;20(6):O123–O134. PMID: 29679517. doi:10.1111/codi.14229
- Angenete E, Asplund D, Andersson J, Haglind E. Self-reported experience of sexual function and quality after abdominoperineal excision in a prospective cohort. Int J Surg. 2014;12(11):1221–1227. PMID: 25311774. doi:10.1016/j.ijsu.2014.10.003
- Dames NB, Squire SE, Devlin AB, Fish R, Bisset CN, Tozer P. Respondents to the sex after colorectal surgery survey. ‘Let’s talk about sex’: a patient-led survey on sexual function after colorectal and pelvic floor surgery. Colorectal Dis. 2021;23(6):1524–1551. PMID: 33615666; PMCID: PMC9291989. doi:10.1111/codi.15598
- Canty J, Stabile C, Milli L, Seidel B, Goldfrank D, Carter J. Sexual function in women with colorectal/anal cancer. Sex Med Rev. 2019;7(2):202–222. PMID: 30655196; PMCID: PMC6445765. doi:10.1016/j.sxmr.2018.12.001
- Althof SE, Parish SJ. Clinical interviewing techniques and sexuality questionnaires for male and female cancer patients. J Sex Med. 2013;10 Suppl 1:35–42. PMID: 23387910. doi:10.1111/jsm.12035
- Liot E, Christou N, de Sousa S, et al. Patients’ related sexual outcomes in colorectal surgery. Front Oncol. 2022;12:968978. PMID: 36591495; PMCID: PMC9800886. doi:10.3389/fonc.2022.968978