
Abstract
Atopic dermatitis (AD) is a common inflammatory skin disorder that manifests as eczematous lesions, often associated with allergic rhinitis and asthma. Historically, moderate-to-severe disease has been managed with systemic immunosuppression, such as oral corticosteroids, which result in relapse and limiting side effects. Due to recent advancements in the identification of interleukin (IL)-4 and IL-13 as key mediators in AD, new biological agents have been developed for treatment. Dupilumab is a recently approved monoclonal antibody that targets the alpha subunit of the IL-4 receptor and, thus, downregulates activity of IL-4 and IL-13. This review discusses the profile of dupilumab and its potential for efficacy and safety in treating moderate-to-severe AD by reviewing data from Phase I–III clinical trials. Results suggest that dupilumab shows great therapeutic promise for AD. Further studies investigating extended use of dupilumab and dupilumab in comparison to other agents are needed to establish long-term efficacy and safety.
Background
Atopic dermatitis (AD) is a chronic inflammatory skin disease characterized by erythema, pruritus, and scaling of skin. AD is clinically diagnosed by these essential features, and the diagnosis is supported by early age of onset, personal or family history of atopy, and xerosis.Citation1 AD has a complex, heterogeneous etiology that includes barrier defects, intrinsic immunological hyperactivity, and extrinsic triggers.Citation2,Citation3 According to a recent study of lifetime worldwide AD prevalence over the period of 1990–2010, there is no overall global trend in the prevalence of AD.Citation4 However, a steady increase in AD prevalence in developing countries has been observed. In general, AD is estimated to affect up to 20% of children in developed countries and 3% of adults worldwide, with up to 50% of pediatric AD cases persisting into adulthood.Citation5,Citation6 In the USA, 10.7% of children and 3.2% of adults are living with AD.Citation7,Citation8
For patients with moderate-to-severe AD, skin lesions encompassing large surface areas are often associated with severe itching. These lesions can cause sleep disturbances and, in turn, symptoms of anxiety, depression, and poor quality of life.Citation9 Topical steroids, topical immunomodulators, and phototherapy are often inadequate in providing sustained improvement in these patients, despite the additive benefit of topicals in decreasing inflammation and restoring epidermal barrier function.Citation2 For patients with poor response to these topicals, the mainstay of treatment is systemic immunosuppression, including oral corticosteroids, cyclosporine, or mycophenolate mofetil. Though these medications may provide moderate relief in AD, the risks often outweigh the benefits of long-term use. In particular, these oral agents are associated with significant side effects such as increased infections, nausea/vomiting, hypertension, and headaches.Citation10,Citation11 In a 10-year chart review of the use of oral immunosuppressive drugs in patients with severe AD, frequent reasons for discontinuation of these therapies included ineffectiveness and adverse events, such as neurological symptoms, gastrointestinal upset, and fatigue/flu-like symptoms.Citation11 Furthermore, for patients with renal impairment and uncontrolled hypertension, oral corticosteroids, mycophenolate mofetil, and cyclosporine are less viable treatment options due to their high risk to exacerbate the underlying comorbidities.
Given the poor therapeutic responses, inconveniences, and therapy-limiting side effects of conventional systemic AD therapeutics, there is a substantial unmet need for more efficacious and promising agents for moderate-to-severe AD with minimal adverse effects. With recent advances in the understanding of the pathological mechanisms of AD, new biological agents have been developed and are being evaluated in clinical trials. In March 2017, dupilumab became the first biologic to be approved by the US Food and Drug Administration for inadequately controlled moderate-to-severe AD.Citation12 The drug received this approval because of its significant demonstration of efficacy and safety in treating AD in three randomized Phase III pivotal trials. The purpose of this article is to review the findings on dupilumab in clinical trials and examine the potential of the drug for inadequately controlled moderate-to-severe AD.
Methods
Relevant articles on disease activity in AD and clinical trials of dupilumab were searched and selected from the databases of PubMed and ClinicalTrials.gov using the following terms: dupilumab, AD, disease activity, interleukin (IL)-4, IL-13, thymus and activation-regulated chemokine (TARC), eotaxin 3 (CCL26), comorbidity, quality of life, efficacy, biologic, and adverse effects. Additional publications were collected from references identified in articles and related citations in PubMed. As of June 2017, Phase I, II, and III clinical trials of dupilumab have been published. In total, 31 relevant papers were reviewed and referenced.
Results
Pathogenesis and disease activity in AD
Ongoing debates regarding the pathogenesis of AD have led to the following description of two forms of the disease: 1) the intrinsic form resulting from abnormal epidermal structure and function, and 2) the extrinsic form due to cutaneous inflammation caused by immune responses to extrinsic antigens.Citation13,Citation14 Moreover, there has been identification of increased activity of T lymphocytes secreting effector cytokines and dysregulation of both cell-mediated immune responses and inflammatory cascades in AD skin.Citation13 Yet, over the past several years, attention has been turned specifically toward type 2 inflammatory mediators as targets for AD therapy.
In particular, IL-4 and IL-13, cytokines from T helper type 2 (Th2) cells, are key mediators of the inflammation in AD. These cytokines upregulate the expression of chemokines such as TARC and CCL26.Citation10,Citation15–Citation18 This increased expression of TARC and CCL26 relates to increased disease activity, including the selective migration of Th2 lymphocytes and eosinophils into AD lesions, which cause inflammation.Citation15–Citation18 Additionally, in synergy with Toll-like receptor 2 ligands, IL-4 potentiates the chronicity of AD through IL-4-mediated suppression of IL-10.Citation19 IL-4 and IL-13 also decrease the keratinocyte expression of barrier proteins, such as filaggrin, involucrin, and loricrin, triggering epidermal hyperplasia.Citation20,Citation21 Additional effects of these cytokines on keratinocytes include the suppression of keratinocyte differentiation and the synthesis of antimicrobial peptides and lipids.Citation13,Citation22,Citation23 This activity further disrupts the skin barrier through aberrant expression of human β-defensins (hBD-2 and hBD-3) and cathelicidin (LL-37) leading to an increase in the susceptibility of lesional skin to infection by microorganisms, such as Staphylococcus aureus.Citation13,Citation24,Citation25 Moreover, IL-4 and IL-13 induce B-cell differentiation leading to immunoglobulin E (IgE) class switching.Citation26 This phenomenon explains the elevation of IgE levels in AD, which is often associated with the extrinsic form of the disease.Citation10,Citation27,Citation28 Given that both IL-4 and IL-13 act through a common receptor (IL-4 receptor alpha; IL-4Rα), IL-4Rα has become a target of interest in treating AD. Inhibition of IL-4Rα has resulted in normalization of skin gene expression from lesional toward nonlesional skin, reduction of TARC expression, and efficacy in the suppression of itch.Citation10,Citation28–Citation30
Dupilumab: mechanism of action
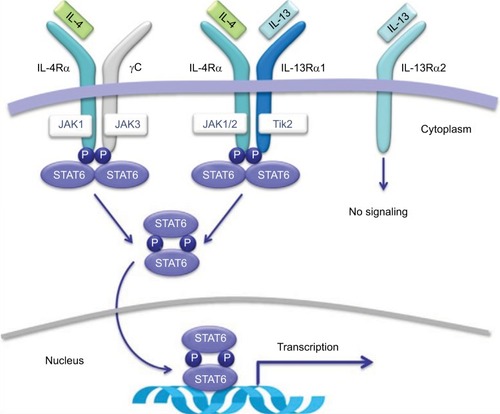
Dupilumab is a fully human monoclonal antibody that binds to the IL-4Rα, resulting in inhibition of both IL-4 and IL-13 signaling.Citation10,Citation12 This blockade by dupilumab reduces the type 2 helper T-cell-mediated inflammation cascade in AD. Specifically, competitive inhibition at the IL-4Rα inhibits activation of the signal transducer and activator of transcription 6 (STAT6)/Janus kinase 1 (JAK1) signaling cascade ().Citation31,Citation32 Overexpression of STAT6 has been demonstrated to decrease epidermal differentiation complex genes, such as the genes for loricrin and involucrin, and enhance penetration of pathogens across the skin barrier leading to AD-like skin disease in mice models.Citation20,Citation33
Figure 1 Receptor signaling for IL-4 and IL-13.
Source: Copyright 2014. Dove Medical Press. Reproduced from Vatrella A, Fabozzi I, Calabrese C, Maselli R, Pelaia G. Dupilumab: a novel treatment for asthma. J Asthma Allergy. 2014;7:123–130.Citation32
Abbreviations: IL, interleukin; IL-4Rα, IL-4 receptor alpha subunit; IL-13α1, IL-13 receptor alpha 1 subunit; IL-13α2, IL-13 receptor alpha 2 subunit; JAK, Janus kinase; STAT, signal transducer and activator of transcription.
Dupilumab: Phase I trials
In two 4-week randomized, double-blind, placebo-controlled, dose-increasing Phase I trials, dupilumab was evaluated as a monotherapy for moderate-to-severe AD in adults.Citation28,Citation34 In the M4A trial, 30 subjects received 75, 150, or 300 mg of subcutaneous dupilumab or placebo weekly for 4 weeks. The subjects were randomly assigned to receive placebo or dupilumab in a 1:4 ratio. In the M4B trial, 37 subjects were studied with 150 or 300 mg of subcutaneous dupilumab or placebo weekly for 4 weeks. These subjects were also randomized to receive placebo or dupilumab, but in a 1:3 ratio. Both the M4A and M4B trials were designed to assess safety as the primary end point. From composite analysis of both studies, by day 29, 59% of patients receiving dupilumab showed 50% reduction in the Eczema Area and Severity Index (EASI) score (EASI-50) compared to 19% of the placebo group (). In addition, significant improvements in Investigator Global Assessment (IGA) scores and pruritus scores for all dupilumab doses combined were observed in both studies. Concerning safety data, nasopharyngitis and headache were the most common side effects with no evidence of serious adverse events in either trial.Citation28,Citation34
Table 1 Clinical efficacy and safety in Phase I–II trials
In addition to clinical improvement and safety, gene expression profiles of lesional sites after 150 and 300 mg dupilumab shifted to a more nonlesional molecular phenotype within 4 weeks.Citation34,Citation35 Lesional skin showed overall improvement in transcriptome by 24% in the 150 mg dose group and 49% in 300 mg dose group compared to 21% in the placebo group.Citation28,Citation34 Notably, markers of epidermal proliferation (K16 and K6B, which reduced epidermal hyperplasia) were downregulated by dupilumab.Citation34,Citation35 T-cell markers and other inflammatory mediators, such as chemokines, were also downregulated by dupilumab. Dupilumab also upregulated genes related with skin barrier functions such as structure-related gene, MATN4, lipid-metabolism-related genes, PLIN4, ADIPOQ, and PLIN1, and barrier-related function genes, CLDN8, ELN, and CLDN11.Citation35
Dupilumab: Phase IIa trials
In a 12-week-long monotherapy study, M12, dupilumab demonstrated significant improvement in reduction of involvement and severity of AD in adults with moderate-to-severe disease. In the M12 study, subjects were randomized to receive subcutaneous 300 mg dupilumab (n=55) or placebo (n=54) weekly for 12 weeks. Dupilumab resulted in substan-tial improvement in multiple clinical measures in EASI-50, EASI-75, and IGA scores (), and pruritus numerical rating scale (NRS) score by day 85. Of note, 85% of patients on dupilumab achieved EASI 50 compared to 35% in the placebo group. Overall, pruritus NRS scores decreased by 56% in the dupilumab group compared to 15% in the placebo group. Serum TARC and serum IgE levels also decreased significantly more in dupilumab patients.Citation28,Citation34
In a 4-week-long randomized, double-blind, parallel-group, placebo-controlled clinical trial (C4), dupilumab was also evaluated in combination with topical corticosteroids (TCSs). Subjects were randomized in a 2:1 ratio to receive subcutaneous 300 mg dupilumab (n=21) or placebo (n=10) weekly for 4 weeks in combination with a regimen of TCSs. The primary end points were the occurrence and severity of adverse events. All subjects in the dupilumab plus TCS group achieved EASI-50 by 4 weeks, while only 50% in the placebo plus TCS group achieved the same ().Citation28 Again, the dupilumab group showed significant improvement in pruritus NRS and IGA scores compared to the placebo group. Moreover, the dupilumab group used 50% less TCSs in comparison to the placebo group. There was also a greater decline of TARC and IgE levels in the dupilumab group.Citation28,Citation34 In the combined safety data for studies of M4A, M4B, M12, and C4, adverse events occurred at similar rates in the dupilumab and placebo groups.Citation34
Dupilumab: Phase IIb trial
In an international, multicenter, randomized, double-blind, dose-ranging, placebo-controlled clinical trial, the efficacy and safety of five different dosings of dupilumab were evaluated over a period of 16 weeks. Subjects were randomly assigned to receive subcutaneous placebo (n=61) or dupilumab 100 mg (n=65) monthly, 300 mg (n=65) monthly, 200 mg (n=61) every 2 weeks, 300 mg (n=64) biweekly, and 300 mg (n=63) weekly. By week 16, dupilumab showed improved EASI scores and resulted in significant improvement in SCORAD (Scoring Atopic Dermatitis) scores in a dose-dependent manner (). All of the 300 mg dupilumab dose regimens resulted in more than 3 points decrease in pruritus NRS scores in 37%–54% of subjects versus 8% of subjects in the placebo group. Furthermore, dupilumab resulted in early and sustained improvement in depression, anxiety, and quality-of-life scores. Mean percentage changes in TARC at week 16 correlated with clinical outcomes such as EASI, SCORAD, and IGA scores.Citation29
Dupilumab: Phase III trials
In 2016, two identically designed Phase III trials of dupilumab were carried out for subjects with moderate-to-severe AD. Subjects were randomly assigned in a 1:1:1 ratio to receive, subcutaneous 300 mg dupilumab or placebo weekly or the same dose of dupilumab every other week alternating with placebo for 16 weeks. The primary outcome was the proportion of subjects who had both a score of 0 or 1 (clear or almost clear) on IGA and a reduction of 2 points or more in that score from baseline at week 16. Over 600 patients participated in each trial, with 671 subjects for SOLO 1 and 708 subjects for SOLO 2 randomized to receive dupilumab or placebo. In SOLO 1, the primary outcome point was achieved by 38% of patients receiving dupilumab every other week, 37% of those receiving dupilumab weekly, and 10% of subjects who received placebo (). SOLO 2 demonstrated comparable results, with 36% of patients in both dupilumab groups and 8% of the placebo group reaching the primary outcome point. Additionally, those in the placebo group received more rescue treatment than those in the dupilumab groups.Citation30
Table 2 Clinical efficacy and safety in Phase III trials
In both trials, dupilumab significantly decreased patient-reported symptoms of AD, with improvement in sleep, anxiety, depression, and, therefore, quality of life of subjects. In Dermatology Life Quality Index (DLQI) and Patient-Oriented Eczema Measure (POEM) scores, dupilumab groups demonstrated twice as much improvement compared to placebo groups. At week 16, among the subjects who had Hospital Anxiety and Depression Scale (HADS)-Anxiety or HADS-Depression scores ≥8 at baseline, significantly more dupilumab-treated subjects had HADS scores of <8 compared to the placebo group.Citation30
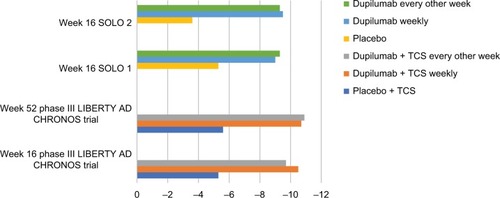
In a 1-year-long randomized, double-blinded, placebo-controlled clinical trial (LIBERTY AD CHRONOS), dupilumab was evaluated as concomitant therapy with TCSs in adults with moderate-to-severe AD and inadequate response to TCSs alone.Citation12 Subjects were randomized in a 3:1:3 ratio to receive subcutaneous 300 mg dupilumab weekly (n=319), 300 mg dupilumab every 2 weeks (n=106), or placebo (n=315), with all three groups receiving concomitant TCSs with or without topical calcineurin inhibitors (TCI) tapered, discontinued, or restarted on the basis of disease activity. By week 16, 39% of patients in each dupilumab group achieved the coprimary endpoint of IGA 0/1 compared to 12% in the placebo group (). The other coprimary endpoint of 75% reduction in EASI score (EASI-75) was achieved by 64% of the weekly dupilumab group, 69% of the dupilumab every other week group, and 23% of the placebo group. Overall, patients receiving dupilumab had more days free of TCSs/TCI and/or systemic rescue medication use than those in the placebo group at 16 weeks and 52 weeks. Additionally, corresponding SCORAD, POEM, HADS, and DLQI scores were significantly reduced in the dupilumab groups compared to the placebo group.Citation12 Improvement of NRS and DLQI scores in all three Phase III trials for dupilumab patients is demonstrated in and .Citation12,Citation30
Figure 2 Percentage of patients who achieved peak pruritus numerical rating scale score improvement ≥4 points from baseline in Phase III trials.
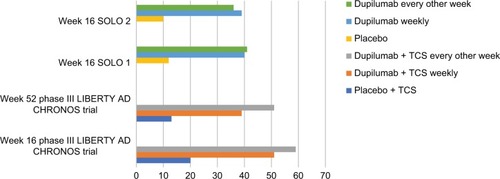
Figure 3 Least squares mean change in Dermatology Life Quality Index score from baseline in Phase III trials.
Discussion
Literature concerning the impact of dupilumab in the pathogenesis of AD includes Phase I, II, and III clinical trials. Results from these trials show that dupilumab improves clinical symptoms of moderate-to-severe AD and decreases T-cell markers, markers of epidermal proliferation, and inflammatory mediators and chemokines.Citation28 In particular, compared to placebo and lower doses, the 300 mg dose of dupilumab demonstrated the greatest improvement in EASI and NRS scores, and transcriptome of lesional skin in Phase I and II studies.Citation28,Citation34 Moreover, the 300 mg dose every other week resulted in similar efficacy to the 300 mg weekly dose in achieving primary and secondary outcome measures in Phase III trials.Citation12,Citation30 Notably, the greatest percentage of patients achieved improvement in EASI or IGA when dupilumab was administered at 300 mg every other week with concomitant TCS use.Citation12
Additionally, the frequency of adverse events was demonstrated to be similar between placebo and dupilumab groups, with the most commonly reported adverse events including headaches and nasopharyngitis in Phase I and II trials.Citation28 In comparison, the most common adverse events reported in Phase III trials were exacerbations of AD (10%–18%), injection-site reactions (15%–19%), and nasopharyngitis (10%–23%), with conjunctivitis also occurring in 14% or more of patients on dupilumab in the 1-year-long Phase III trial.Citation12,Citation30 Of note, in Phase I and II trials dupilumab also demonstrated decreased total number of skin infections compared to placebo (4%–5% versus 10%–24%).Citation28 Moreover, across the four Phase I and II trials, the rate of skin infections in the placebo groups was 0.2 per patient compared to 0.05 infections per patient in the dupilumab groups.Citation28 This particular finding supports the concept that dupilumab improves epidermal barrier function.
In addition to its clinical efficacy, dupilumab also demonstrated improved quality of life as well, with significant reduction of DLQI and POEM scores.Citation30 Overall, these results suggest that IL-4 and IL-13 are important mediators in the pathogenesis and morbidity of AD. However, additional trials over an extended period of time are necessary to establish a long-term safety and efficacy profile of dupilumab.
The recent recognition of AD as a predominantly Th2-mediated disease has led the way for the investigation of a variety of therapeutics that target specific inflammatory mediators involved in innate immunity. Multiple biologics are currently being investigated in clinical trials, including antibodies that specifically target IL-13, IL-17, IL-22, IL-31, and IL-12/IL-23p40.Citation36 Topical and oral phosphodiesterase-4 inhibitors are also being investigated in Phase II and Phase III clinical trials, along with a JAK inhibitor and therapeutics targeting thymic stromal lymphopoietin and chemoattractant receptor-homologous molecule expressed on Th2 cells.Citation36 These novel therapies have shown promising results. Notably, IL-31 inhibition has shown significant reduction of pruritus in patients with AD.Citation37 Yet, despite these ongoing investigations into the use of multiple biologics for treatment of AD, dupilumab remains the first and only biologic to be approved for moderate-to-severe AD.
Prior to the development of dupilumab, treatments available for AD included topical and oral glucocorticoids, calcineurin inhibitors, cyclosporine, methotrexate, azathioprine, and mycophenolic acid precursors. Currently, there are no studies comparing dupilumab to other systemic treatments approved for AD. However, prior to the approval of dupilumab, a systematic review of 34 randomized control trials involving 1,653 patients compared the efficacy and safety of 12 systemic treatments using the Grading of Recommendations Assessment, Development, and Evaluation approach.Citation38 Azathioprine and methotrexate were recommended as second- and third-line treatments, respectively, according to moderate-quality evidence.Citation38 Cyclosporine A (CsA) received the strongest recommendation as a first-line treatment for short-term use in AD. Additionally, evidence based on four trials demonstrated that long-term treatment with CsA can be recommended for up to 1 year.Citation38–Citation42 However, comparison of associated risks of long-term use of CsA, such as nephrotoxicity and hypertension, to that of year-long use of dupilumab, such as nasopharyngitis and conjunctivitis, suggests that dupilumab is likely a safer long-term option.Citation12,Citation39–Citation43 Yet, due to variations in trial designs, it is problematic to compare safety and efficacy data between studies of systemic treatments and dupilumab.Citation29,Citation38
Future evaluations should focus on comparing the efficacy and safety of dupilumab against available systemic treatments in head-to-head trials. In addition, further studies observing the long-term efficacy and safety of dupilumab are also needed. In particular, extended observation to assess immunogenicity is warranted. Specifically, an assessment of the development of neutralizing antibodies over long-term use may provide further insight into how immunogenicity may affect long-term efficacy of dupilumab. Overall, the administration of dupilumab every other week and its relative safety and efficacy offer a convenient and lower-risk alternative to currently available systemic treatments for moderate-to-severe AD.
Disclosure
Dr Alison Ehrlich is an investigator for Sun Pharmaceuticals, Abbvie, Pfizer, UCB Biopharma, Merck, Leo Pharma, Eli Lilly, and is a speaker for Eli Lilly, Celgene, and Abbvie. Dr Alison Ehrlich was also a former principal investigator for the SOLO 2 trial. Dr Olabola Awosika’s fellowship is funded by Janssen Biotech, Inc. The authors report no other conflicts of interest in this work.
References
- EichenfeldLFTomWLChamlinSLGuidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitisJ Am Acad Dermatol201470233835124290431
- WeidingerSNovakNAtopic dermatitisLancet2016387100231109112226377142
- SkabytskaYKaeslerSVolzTBiedermannTThe role of innate immune signaling in the pathogenesis of atopic dermatitis and consequences for treatmentsSemin Immunopathol2016381294326573298
- DeckersIAMcLeanSLinssenSMommersMvan SchayckCPSheikhAInvestigating international time trends in the incidence and prevalence of atopic eczema 1990–2010: a systematic review of epidemiological studiesPLoS One201277e3980322808063
- Mei-Yen YongATayYKAtopic dermatitis: racial and ethnic differencesDermatol Clin201735339540228577807
- MargolisJSAbuabaraKBilkerWHoffstadOMargolisDJPersistence of mild to moderate atopic dermatitisJAMA Dermatol2014150659360024696036
- SilverbergJIHanifinJMAdult eczema prevalence and associations with asthma and other health and demographic factors: A US population–based studyJ Allergy Clin Immunol201313251132113824094544
- ShawTECurrieGPKoudelkaCWSimpsonELEczema prevalence in the United States: data from the 2003 National Survey of Children’s HealthJ Invest Dermatol20111311677320739951
- SimpsonELBeiberTEckertLPatient burden of moderate to severe atopic dermatitis (AD): Insights from a phase 2b clinical trial of dupilumab in adultsJ Am Acad Dermatol201674349149826777100
- GandhiNAPirozziGGrahamNMCommonality of the IL-4/IL-13 pathway in atopic diseaseExp Rev Clin Immunol2017135425437
- GarritsenFMRoekevischEvan der SchaftJDeinumJSpulsPIde Bruin-WellerMSTen years’ experience with oral immunosuppressive treatment in adult patients with atopic dermatitis in two academic centresJ Eur Acad Dermatol Venereol201529101905191225752497
- BlauveltAde Bruin-WellerMGooderhamMLong-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): a 1-year, randomized, double-blinded, placebo-controlled, phase 3 trialLancet2017389100862287230328478972
- WangAXXu LandénNNew insights into T cells and their signature cytokines in atopic dermatitisIUBMB Life201567860161026178387
- DharmageSCLoweAJMathesonMCBurgessJAAllenKJAbramsonMJAtopic dermatitis and the atopic march revisitedAllergy2014691172724117677
- KakinumaTNakamuraKWakugawaMThymus and activation-regulated chemokine in atopic dermatitis: Serum thymus and activation-regulated chemokine level is closely related with disease activityJ Allergy Clin Immunol2001107353554111240957
- HijnenDDe Bruin-WellerMOostingBSerum thymus and activation-regulated chemokine (TARC) and cutaneous T cell–attracting chemokine (CTACK) levels in allergic diseases: TARC and CTACK are disease-specific markers for atopic dermatitisJ Allergy Clin Immunol2004113233434014767451
- KagamiSKakinumaTSaekiHSignificant elevation of serum levels of eotaxin-3/CCL26, but not of eotaxin-2/CCL24, in patients with atopic dermatitis: serum eotaxin-3/CCL26 levels reflect the disease activity of atopic dermatitisClin Exp Immunol2003134230931314616792
- KagamiSSaekiHKomineMInterleukin-4 and interleukin-13 enhance CCL26 production in a human keratinocyte cell line, HaCaT cellsClin Exp Immunol2005141345946616045735
- KaeslerSVolzTSkabytskaYToll-like receptor 2 ligands promote chronic atopic dermatitis through IL-4-mediated suppression of IL-10J Allergy Clin Immunol20141341929924698321
- KimBELeungDYBoguniewiczMHowellMDLoricrin and involucrin expression is down-regulated by Th2 cytokines through STAT-6Clin Immunol2008126333233718166499
- HowellMDKimBEGaoPCytokine modulation of atopic dermatitis filaggrin skin expressionJ Allergy Clin Immunol20091243 Suppl 2R7R1219720210
- KamsteegMBergersMDe BoerRType 2 helper T-cell cytokines induce morphologic and molecular characteristics of atopic dermatitis in human skin equivalentAm J Pathol201117852091209921514424
- SawadaEYoshidaNSugiuraAImokawaGTh1 cytokines accentuate but Th2 cytokines attenuate ceramide production in the stratum corneum of human epidermal equivalents: an implication for the disrupted barrier mechanism in atopic dermatitisJ Dermatol Sci2012681253522884781
- ParkKYKimDHJeongMSLiKSeoSJChanges of antimicrobial peptides and transepidermal water loss after topical application of tacrolimus and ceramide-dominant emollient in patients with atopic dermatitisJ Korean Med Sci201025576677120436715
- YamasakiKGalloRLAntimicrobial peptides in human skin diseaseEur J Dermatol2008181112118086583
- LebmanDACoffmanRLInterleukin 4 causes isotype switching to IgE in T cell-stimulated clonal B cell culturesJ Exp Med198816838538623049907
- BieberTAtopic dermatitisN Engl J Med2008358141483149418385500
- BeckLAThaçiDHamiltonJDDupilumab treatment in adults with moderate-to-severe atopic dermatitisN Engl J Med2014371213013925006719
- ThaçiDSimpsonELBeckLAEfficacy and safety of dupilumab in adults with moderate-to-severe atopic dermatitis inadequately controlled by topical treatments: a randomised, placebo-controlled, dose-ranging phase 2b trialLancet201638710013405226454361
- SimpsonELBieberT1Guttman-YasskyESOLO 1 and SOLO 2 InvestigatorsTwo Phase 3 trials of dupilumab versus placebo in atopic dermatitisN Engl J Med2016375242335234827690741
- BaoLZhangHChanLSThe involvement of the JAK-STAT signaling pathway in chronic inflammatory skin disease atopic dermatitisJAKSTAT201323e2413724069552
- VatrellaAFabozziICalabreseCMaselliRPelaiaGDupilumab: a novel treatment for asthmaJ Asthma Allergy2014712313025214796
- SehraSYaoYHowellMDIL-4 regulates skin homeostasis and the predisposition toward allergic skin inflammationJ Immunol201018463186319020147633
- HamiltonJDUngarBGuttman-YasskyEDrug evaluation review: dupilumab in atopic dermatitisImmunotherapy20157101043105826598956
- HamiltonJDSuárez-FariñasMDhingraNDupilumab improves the molecular signature in skin of patients with moderate-to-severe atopic dermatitisJ Allergy Clin Immunol201413461293130025482871
- HeratizadehAWerfelTAnti-inflammatory therapies in atopic dermatitisAllergy201671121666167527735066
- RuzickaTHanifinJMFurueMAnti–Interleukin-31 receptor a antibody for atopic dermatitisN Engl J Med2017376982683528249150
- RoekevischESpulsPIKuesterDLimpensJSchmittJEfficacy and safety of systemic treatments for moderate-to-severe atopic dermatitis: a systematic reviewJ Allergy Clin Immunol2014133242943824269258
- HarperJIAhmedIBarclayGCyclosporine for severe childhood atopic dermatitis: short course versus continuous therapyBr J Dermatol20001421525810651694
- ZonneveldIMDe RieMABeljaardsRCThe long-term safety and efficacy of cyclosporin in severe refractory atopic dermatitis: a comparison of two dosage regimensBr J Dermatol1996135Suppl 4815208881899
- GranlundHErkkoPRemitzAComparison of cyclosporin and UVAB phototherapy for intermittent one-year treatment of atopic dermatitisActa Derm Venereol2001811222711411908
- HaeckIMKnolMJTen BergeOvan VelsenSGde Bruin-WellerMSBruijnzeel-KoomenCAEnteric-coated mycophenolate sodium versus cyclosporin A as long-term treatment in adult patients with severe atopic dermatitis: a randomized controlled trialJ Am Acad Dermatol20116461074108421458107
- SchmittJSchakelKFolster-HolstRPrednisolone vs. cyclosporine for severe adult eczema. An investigator-initiated double-blind placebo-controlled multicenter trialBr J Dermatol2010162366166819863501