Abstract
Imiquimod, an immune-modulating imidazoquinoline compound, has been approved in topical formulation for the treatment of actinic keratoses, superficial basal cell carcinomas, and external genital warts. Its use in the treatment of field cancerization, in particular, has been rapidly evolving. With the recent approval of a new drug application for a new concentration, as well as generic formulations, this drug has emerged at the forefront of treatment for actinic keratoses, with improved dosage scheduling and more patients having access to generic options. In the nearly 15 years since its original approval by the Food and Drug Administration for the treatment of actinic keratoses in 1997, topical imiquimod has been reviewed and studied extensively, not only for its safety and efficacy, but also for its tolerability in patients. This paper provides an indepth review of the literature, and provides clinical evidence for its inclusion in the arsenal of treatment options for patients with actinic keratoses.
Introduction
Actinic keratoses are small, scaly, sandpaper-like papules found on sun-exposed areas of skin including the face, balding scalp, and arms. With an approximate four-year risk of evolving into basal cell carcinoma or squamous cell carcinoma of 1.6% and 2.6%, respectively, these lesions are considered to be premalignant.Citation1,Citation2 There are many treatment options currently available for the treatment of actinic keratoses, including imiquimod, cryotherapy, 5-fluorouracil, 3% diclofenac in 2.5% hyaluronan gel, and topical photodynamic therapy, as well as new emerging potential therapies, such as ingenol-3-angelate. This review focuses on topical imiquimod and its history as a topical immune response modifier in the treatment of actinic keratoses.
Imiquimod, an imidazoquinoline compound, is a low molecular weight immune modifier which upregulates interferon-alpha, tumor necrosis factor-alpha, interleukin (IL)-1, IL-6, IL-8, IL-12, and other cytokines locally. It is capable of inducing both the innate and the adaptive immune responses in order to achieve enhancement of the endogenous immune response, and also upregulates the natural antitumor and antiviral cell response. In 1997, the Food and Drug Administration (FDA) approved topical imiquimod cream at a concentration of 5% to be used for the treatment of typical, nonhyperkeratotic, and nonhypertrophic actinic keratoses on the face or scalp in immunocompetent adults. In 2010, the FDA approved a 3.75% imiquimod formulation for treatment of clinical typical, visible, or palpable actinic keratoses on the face or balding scalp. Formulations, indications, and the dosing regimen are listed in . As new formulations and treatment regimens are approved, more data will emerge on the safety and efficacy of topical imiquimod. Furthermore, we will gain more insight into its tolerability for patients.
Table 1 Imiquimod formulations, indications, and dosing regimens
Overview of imiquimod
Mechanism
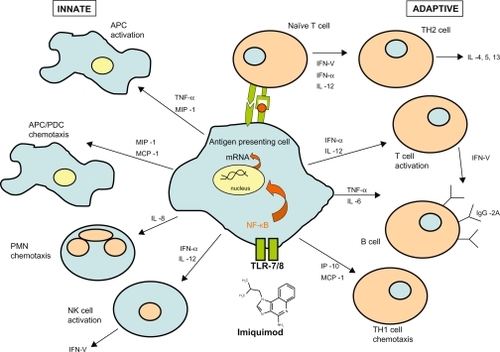
Structurally, the chemical nomenclature of imiquimod is 1-(2-methylpropyl)-1H-imidazo[4,5-c]quinolin-4-amine ().Citation3 Imiquimod acts as an immune modifier by targeting cytokine-producing cells, such as monocytes, macrophages, and dendritic cells bearing toll-like receptor 7/8.Citation4 This first drug of its class acts via innate and acquired immune pathways in order to stimulate release of cytokines, such as tumor necrosis factor-alpha, IL-6, IL-12, and interferon-alpha, as well as activation of natural killer cells, antigen-presenting cells, T cells, and B cells (). This cascade also results in the production of interferon-gamma by Th1 cells.Citation5 Imiquimod induces cellular memory via the activation of effector T cells, Langerhans cells, lymphocytes, and macrophages, which circulate lymphatically and activate the adaptive immune response.
Figure 1 Chemical structure of Imiquimod.
Figure 2 Mechanism of Imiquimod.
Metabolism and pharmacokinetics
When applied topically, the half-life of imiquimod is approximately 30 hours.Citation6 Systemic absorption of imiquimod is minimal when the cream is applied to intact skin, with 97% of the drug recovered from the dosing site in one study. Other studies have demonstrated no quantifiable metabolites in serum, with <0.9% of a single 5 mg dose excreted in urine and feces.Citation7 There is no detectable radioactivity in serum. Kulp et al characterized serum markers in 19 subjects applying two packets (18.75 mg total) of imiquimod cream 3.75% once daily for 21 days to an area of skin on the face or balding scalp totaling approximately 200 cm2.Citation8 After 21 days, the average maximum serum concentration was 0.323 mg/mL, with a half-life of 29 hours. Researchers concluded that systemic exposure of imiquimod was low after 21 days of application.
Differences in the release rates of imiquimod between the generic and brand formulations have been studied in vitro. Due to differences in the compositions of the vehicle creams, there may be differences in the safety and efficacy of generic versus brand medications as well. To answer this question, a nationwide, multicenter, double-blind, 16-week study is underway to compare vehicles used in the generic and brand formulations of imiquimod cream 5% for the treatment of actinic keratoses on the face or scalp.Citation9
Safety
Due to the lack of data in animal models, the use of imiquimod is contraindicated during pregnancy. Imiquimod is listed as a Category C drug. Female patients of child-bearing age should be counseled regarding the importance of contraception before being prescribed imiquimod because its teratogenicity is as yet undetermined.
Clinical data
A double-blind, vehicle-controlled pilot study by Edwards el al evaluated imiquimod cream 5% versus vehicle in 40 subjects with at least three actinic keratoses.Citation10 When treated three times per week for up to 16 weeks, 75% of lesions cleared, compared with 12% in the vehicle group. Some of the first reported cases of imiquimod 5% cream for the treatment of actinic keratoses were by Stockfleth et al in 2001.Citation11 Six patients who had up to 10 actinic keratoses were treated 2–3 times per week for 6–8 weeks, with complete clearance and no recurrences one year later. Persaud et al conducted a study of 22 patients, each acting as their own control, applying topical imiquimod 5% to one side of the body and vehicle to the other.Citation12 At the end of eight weeks, a significant reduction in the number of lesions was observed for the imiquimod-treated side (from 10.1 to 6.2) compared with vehicle (8.1 to 7.6). An open-label trial of imiquimod 5% cream was conducted by Salasche et al, involving 25 patients with 5–20 discrete actinic keratoses, treated three times per week for four weeks, followed by a rest period of four weeks.Citation13 If any lesions remained, patients repeated the eight-week cycle up to a maximum of 24 weeks. Researchers noted that although 45.5% of sites were clear by the end of the first cycle, actinic keratoses continued to clear during the “therapeutic interval” rest period. Complete clearing was achieved in 82% of lesions, including subclinical lesions that were uncovered by treatment with imiquimod. This cycling approach was able to achieve high efficacy while minimizing adverse effects.
Two multicenter, randomized, double-blind, parallel-group, vehicle-controlled Phase III trials were conducted to evaluate the efficacy of imiquimod 5% cream for the treatment of actinic keratoses on the face and balding scalp.Citation14 In total, 436 patients were randomized to apply either imiquimod 5% cream or vehicle once a day two times per week for 16 weeks. Complete clearance rates were 45.1% for the imiquimod group and 3.2% for the vehicle group. Although 17.7% of imiquimod-treated subjects reported severe erythema, only 3% discontinued the study due to adverse events. The second Phase III study involved application of imiquimod 5% or vehicle cream once a day three times per week for 16 weeks in 286 patients.Citation15 Histology-proven complete clearance rates were observed in 57.1% of imiquimod-treated and 2.2% of vehicle-treated subjects, with dropout rates due to adverse events of 4% and 3%, respectively.
Another pair of similar Phase III trials evaluated 492 patients randomized to apply either imiquimod 5% cream or vehicle three times a week for 16 weeks.Citation16 At eight weeks post-treatment, imiquimod-treated patients experienced an 86.6% reduction in the number of baseline lesions as compared with 14.3% for vehicle-treated patients. Long-term follow-up studies (1–2 years post-treatment) have shown continued clinical benefit of imiquimod treatment for actinic keratoses, with the majority of treated patients remaining clear, and low rates of recurrence.Citation17
A meta-analysis comparing the efficacy of imiquimod 5% cream versus 5-fluorouracil for the treatment of actinic keratoses on the face and scalp concluded that imiquimod was more efficacious than 5-fluorouracil (70% ± 12% versus 52% ± 18%, respectively).Citation18 Tanghetti and Werschler conducted a trial assessing 39 patients randomized to receive either 5-fluorouracil twice daily or imiquimod 5% twice weekly for treatment of actinic keratoses for 16 weeks.Citation19 At the end of the study at week 24, reduction in the total actinic keratosis count was 94% for 5-fluorouracil compared with 66% for imiquimod. However, more recent studies have reported sustained field clearance rates in all patients one year after treatment. In 75 patients treated with imiquimod 5% three times weekly for four weeks, 5-fluorouracil twice daily for four weeks or cryotherapy (including also those not cleared at the end of therapy), sustained clearance was achieved in 73%, 33%, and 4% of patients, respectively.Citation20
Stockfleth et al evaluated the response to a shortened course of treatment.Citation21 In an open-label Phase IIIb trial, 829 subjects applied imiquimod 5% cream or vehicle to the treatment area three times weekly for four weeks, followed by a four-week period of no treatment. If actinic keratoses remained, then a second four-week course of treatment was initiated. Complete and partial (≥75% lesion reduction) clearance rates were 68.9% and 80.2%, respectively, similar to those observed after 16-week treatment courses. To investigate whether a lower concentration of imiquimod might be efficacious in the treatment of actinic keratoses with reduced adverse reactions, two placebo-controlled studies were performed comparing imiquimod 2.5% and 3.75% to the face or balding scalp for two-week or three-week cycles.Citation22,Citation23 Results were similar for the two trials. In the two-week cycle study (daily treatment for two weeks, two weeks of no treatment, followed by another two weeks of daily treatment), mean reductions from baseline lesion count were 25% for placebo, 72% for imiquimod 2.5%, and 82% for imiquimod 3.75%.Citation22 Furthermore, the sustained clearance of lesions in these patients remained significant at one-year follow-up, with 33% of imiquimod 2.5% subjects and 41% of imiquimod 3.75% subjects remaining 100% clear of lesions.
When used in combination with cryotherapy, imiquimod has the ability to increase clearance of lesions. In a study of 63 subjects, when imiquimod 5% cream was used post-cryotherapy, a significantly greater total number of actinic keratoses were cleared compared with vehicle (23% versus 9%).Citation24 Imiquimod cream 3.75% was also evaluated post-cryotherapy in a multicenter, double-blind, vehicle-controlled study.Citation25 Patients with at least five actinic keratoses on the face were treated with cryotherapy, leaving at least five lesions untreated. One to two weeks post-cryotherapy, imiquimod 3.75% or vehicle cream was applied to the treatment area in two-week cycles as described previously. Complete clearance rates were 30% for imiquimod versus 3% for vehicle, with mean total lesion reductions of 87% versus 50%, respectively.
To assess field-directed therapies used in combination, the sequential use of photodynamic therapy with aminolevulinic acid followed by imiquimod was performed in 25 subjects with facial actinic keratoses.Citation26 One month after photodynamic therapy, imiquimod or vehicle was applied to the area twice weekly for 16 weeks. At one year of follow-up, median lesion reduction was 90% for imiquimod versus 75% for vehicle, with no subject discontinuing due to an adverse event.
Nonmelanoma skin cancer affects a disproportionately large number of immunosuppressed patients. Ulrich et al reported five of six organ transplant recipients being successfully treated for actinic keratoses with topical imiquimod 5% cream.Citation27 In this nonrandomized pilot study, imiquimod 5% was applied 2–3 times per week for 12–16 weeks, with complete clearance of all lesions in five of six patients. Another study assessed graft function in 24 transplant patients receiving treatment with imiquimod, finding that it was not altered, and that therapy was well tolerated.Citation28 A larger, multicenter, randomized, placebo-controlled study was undertaken by Ulrich et al involving 43 transplant patients with actinic keratoses.Citation29 Patients applied imiquimod 5% cream or vehicle three times per week for 16 weeks to a defined treatment area of 100 cm.Citation2 Efficacy was similar to that in immunocompetent patients, with no patients experiencing transplant rejection or discontinuing due to drug-related adverse events.
Patient acceptability
Due to the ease, convenience, privacy, and autonomy associated with self-administration, treatment of dermatologic conditions with imiquimod cream is preferred by patients over physician-administered modalities.Citation30 Patient preference should guide treatment, because clearance rates are significantly enhanced with good patient compliance with any treatment regimen.
Patient preferences comparing imiquimod 5% and 3.75% have not been formally surveyed to date. However, the reduced total treatment time for the 3.75% cream from 16 weeks to six weeks offers a distinct advantage over the 5% cream in terms of patient compliance. Patients must still be made aware of the importance of prevention, sun avoidance, frequent skin examinations by a dermatologist, as well as the use of sun-protective outerwear and sun block.
Adverse effects
The most common adverse effect from topically applied imiquimod cream is a localized skin reaction at the application site. Generally, imiquimod is well accepted, with few patients choosing to discontinue therapy or withdrawal from clinical trials due to intolerable side effects. Commonly, patients experience mild to moderate discomfort, with erythema, itching, burning, pain, edema, ulceration, and induration being reported most often. The erythema is characteristic of the local immune response, as imiquimod unmasks subclinical lesions and treats them in the process. A positive correlation exists between histologic clearance rates for actinic keratoses and the severity of erythema, crusting, scabbing, and erosion.Citation31 provides an example of a characteristic patient response during a course of imiquimod therapy.
Figure 3 Characteristic patient response during a course of imiquimod therapy for actinic keratoses.

Rarely, imiquimod can trigger or exacerbate existing inflammatory conditions. Cases of arthritis,Citation32 pemphigus foliaceous,Citation33 psoriasis,Citation34 actinic cheilitis,Citation35 pityriasis rubra pilaris,Citation36 alopecia,Citation37 erosive pustular dermatosis of the scalp,Citation38 and subacute cutaneous lupus erythematosusCitation39 attributed to treatment with imiquimod have been alleged in the literature.
Cost analysis
A pharmacoeconomic analysis of the treatment of actinic keratosis found that although imiquimod is the initially more expensive of the medications approved by the FDA, when treating multiple lesions, it offers an advantage over cryotherapy or photodynamic therapy with 5-aminolevulinic acid in that patients do not need to return over multiple days for in-office treatment, thus reducing the cost to the patient.Citation40
Studies have demonstrated a low incidence of new actinic keratotic lesions after treatment with imiquimod, due to its ability to induce immunologic memory.Citation41 This long-term clearance offers an advantage in terms of the cost of retreating areas of recurrence. By treating the field of cancerization, subclinical lesions are eradicated, thus eliminating the need to wait until these lesions are clinically visible and further progressed.
Conclusion
Topical imiquimod has proven to be safe and efficacious in the treatment of actinic keratoses, with tolerable transient local adverse effects. The ability of imiquimod to elicit an immune response and to treat subclinical lesions makes it among the most strategic therapies for these patients. With the availability of two concentrations, as well as generic formulations, imiquimod cream will no doubt continue to be used as effective monotherapy for patients with field cancerization in larger exposed skin areas. The research reviewed here highlights over a decade of clinical data on topical imiquimod. Field-directed therapies for the treatment of actinic keratoses will continue to emerge in this rapidly evolving field. Although no topical therapy has 100% efficacy without recurrence, imiquimod is among the forefront of these therapies, with much evidence-based justification for its place in the dermatologist’s arsenal.
Disclosure
BB is a consultant for Graceway Pharmaceuticals, Pharma-Derm, and CHS Pharma. CC has no conflicts of interest to report.
References
- GrossmanDLeffellDJThe molecular basis of nonmelanoma skin cancerArch Dermatol199713310126312709382565
- CriscioneVDWeinstockMANaylorMFActinic keratoses: Natural history and risk of malignant transformation in the Veterans Affairs Topical Tretinoin Chemoprevention TrialCancer2009115112523253019382202
- BuckHWImiquimod (Aldara cream)Infect Dis Obstet Gynecol19986249519702584
- HemmiHKaishoTTakeuchiOSmall anti-viral compounds activate immune cells via the TLR7 MyD88-dependent signaling pathwayNat Immunol20023219620011812998
- MillerRLGersterJFOwensMLImiquimod applied topically: A novel immune response modifier and new class of drugInt J Immunopharmacol1999211111410411278
- OwensMLBridsonWESmithSLMyersJAFoxTLWellsTMPercutaneous penetration of Aldara™ cream, 5% during the topical treatment of genital and perianal wartsPoster presented at the 46th annual clinical meeting of the American College of Obstetricians and GynecologistsNew Orleans, LAMay 9–13, 1998
- TygumKISmithSLMyersJAPercutaneous penetration of [14C]-imiquimod from a single application of creamPharm Res.1995129 Suppl Abstr 7339.
- KulpJLevySFeinMCAdamsMFurstJMengTCPharmacokinetics of imiquimod 3.75% cream applied daily for 3 weeks to actinic keratoses on the face and/or balding scalpArch Dermatol Res2010302753954420204654
- US Food and Drug AdministrationBioequivalence of generic imiquimod cream, 5% when compared to Aldara™ (imiquimod) cream, 5% in the treatment of actinic keratosis Clinicaltrials.gov Identifier: NCT00948428. Available at: http://clinicaltrials.gov/ct2/show/NCT00948428. Accessed March 22, 2011.
- EdwardsLOwensMLAndresKLA pilot study evaluating imiquimod 5% cream versus vehicle in the treatment of actinic keratosesPoster presented at the 58th annual meeting of the American Academy of DermatologySan Francisco, CAMarch 10–15, 2000
- StockflethEMeyerTBenninghoffBChristophersESuccessful treatment of actinic keratosis with imiquimod cream 5%: A report of six casesBr J Dermatol200114451050105311359396
- PersaudANShamuelovaEShererDClinical effect of imiquimod 5% cream in the treatment of actinic keratosisJ Am Acad Dermatol200247455355612271300
- SalascheSJLevineNMorrisonLCycle therapy of actinic keratoses of the face and scalp with 5% topical imiquimod cream: An open-label trialJ Am Acad Dermatol200247457157712271303
- LebwohlMDinehartSWhitingDImiquimod 5% cream for the treatment of actinic keratosis: Results from two phase III, randomized, double-blind, parallel group, vehicle-controlled trialsJ Am Acad Dermatol200450571472115097955
- SzeimiesRMGerritsenMJGuptaGImiquimod 5% cream for the treatment of actinic keratosis: Results from a phase III, randomized, double-blind, vehicle-controlled, clinical trial with histologyJ Am Acad Dermatol200451454755515389189
- KormanNMoyRLingMDosing with 5% imiquimod cream 3 times per week for the treatment of actinic keratosis: Results of two phase 3, randomized, double-blind, parallel-group, vehicle-controlled trialsArch Dermatol2005141446747315837864
- LeePKHarwellWBLovenKHLong-term clinical outcomes following treatment of actinic keratosis with imiquimod 5% creamDermatol Surg200531665966415996416
- GuptaAKDaveyVMcPhailHEvaluation of the effectiveness of imiquimod and 5-fluorouracil for the treatment of actinic keratosis: Critical review and meta-analysis of efficacy studiesJ Cutan Med Surg20059520921416502198
- TanghettiEWerschlerPComparison of 5% 5-fluorouracil cream and 5% imiquimod cream in the management of actinic keratoses on the face and scalpJ Drugs Dermatol20076214414717373172
- KrawtchenkoNRoewert-HuberJUlrichMMannISterryWStockflethEA randomised study of topical 5% imiquimod vs topical 5-fluorouracil vs cryosurgery in immunocompetent patients with actinic keratoses: A comparison of clinical and histological outcomes including 1-year follow-upBr J Dermatol2007157Suppl 2344018067630
- StockflethESterryWCarey-YardMBichelJMulticentre, open-label study using imiquimod 5% cream in one or two 4-week courses of treatment for multiple actinic keratoses on the headBr J Dermatol2007157Suppl 2414618067631
- SwansonNAbramovitsWBermanBKulpJRigelDSLevySImiquimod 2.5% and 3.75% for the treatment of actinic keratoses: Results of two placebo-controlled studies of daily application to the face and balding scalp for two 2-week cyclesJ Am Acad Dermatol201062458259020133013
- HankeCWBeerKRStockflethEWuJRosenTLevySImiquimod 2.5% and 3.75% for the treatment of actinic keratoses: Results of two placebo-controlled studies of daily application to the face and balding scalp for two 3-week cyclesJ Am Acad Dermatol201062457358120133012
- TanJKThomasDRPoulinYMaddinFTangJEfficacy of imiquimod as an adjunct to cryotherapy for actinic keratosesJ Cutan Med Surg200711619520118042331
- JorizzoJLMarkowitzOLebwohlMGA randomized, double-blinded, placebo-controlled, multicenter, efficacy and safety study of 3.75% imiquimod cream following cryosurgery for the treatment of actinic keratosesJ Drugs Dermatol2010991101110820865842
- ShaffelburgMTreatment of actinic keratoses with sequential use of photodynamic therapy and imiquimod 5% creamJ Drugs Dermatol200981353919180894
- UlrichCBuschJOMeyerTSuccessful treatment of multiple actinic keratoses in organ transplant patients with topical 5% imiquimod: A report of six casesBr J Dermatol2006155245145416882188
- Ben M’barekLMebazaaAEuvrardS5% topical imiquimod tolerance in transplant recipientsDermatology2007215213013317684375
- UlrichCBichelJEuvrardSTopical immunomodulation under systemic immunosuppression: Results of a multicentre, randomized, placebo-controlled safety and efficacy study of imiquimod 5% cream for the treatment of actinic keratoses in kidney, heart, and liver transplant patientsBr J Dermatol2007157Suppl 2253118067628
- O’MahoneyCLawCGollnickHPMMariniMNew patient-applied therapy for anogenital warts is rated favourably by patientsInt J STD AIDS20011256557011516364
- SkinnerRRole of topical therapies in the management of cutaneous diseaseJ Cutan Med Surg20048Suppl 3223115647859
- BensonEImiquimod: Potential risk of an immunostimulantAustralas J Dermatol200445212312415068461
- LinRLaddDJPowellDJWayBVLocalized pemphigus foliaceous induced by topical imiquimodArch Dermatol200414088989015262711
- FantiPADikaEVaccariSMiscialCVarottiCGeneralized psoriasis induced by topical treatment of actinic keratosis with imiquimodInt J Dermatol200645121464146517184267
- GreenbergHLCohenJLRosenTOrengoISevere reaction to 5% imiquimod cream with excellent clinical and cosmetic outcomesJ Drugs Dermatol20076445245817668546
- YangFCJessupCDahiyaMReynoldsRPityriasis rubra pilaris exacerbation with topical use of imiquimodInt J Dermatol200847101076107818986361
- CondeJDavisKNtuenEBalmerNJonesDMcMichaelAA case of imiquimod-induced alopeciaJ Dermatolog Treat201021212212419488918
- VaccaroMBarbuzzaOGuarneriBErosive pustular dermatosis of the scalp following treatment with topical imiquimod for actinic keratosisArch Dermatol2009145111340134119917978
- BurnettTJEnglishJC3rdFerrisLKDevelopment of subacute cutaneous lupus erythematosus associated with the use of imiquimod to treat actinic keratosesJ Drugs Dermatol2010981022102420684157
- GoldMHPharmacoeconomic analysis of the treatment of multiple actinic keratosesJ Drugs Dermatol200871232518246694
- StockflethEChristophersEBenninghoffBSterryWLow incidence of new actinic keratoses after topical 5% imiquimod cream treatment: A long-term follow-up studyArch Dermatol2004140154215611446