
Abstract
Background
There are overlapping features in histopathologic characteristics of psoriasis and chronic dermatitis, which sometimes make the correct diagnosis difficult.
Objective
The aim of this study was to compare the histopathologic diagnostic features of psoriasis with chronic dermatitis quantitatively.
Patients and methods
In this study, 30 patients with psoriasis and 30 patients with chronic dermatitis were included. Diagnosis of psoriasis or chronic dermatitis was based on clinicopathologic correlation. Photos of histopathologic slides were provided by LABOMED Digital Camera and LABOMED Microscope. Width and length of rete ridges, minimal thickness of suprapapillary plates, thickness of epidermis, thickness of hyperkeratotic layer, and minimal thickness of granular layer were determined using Pixel Pro software on micrometer scale.
Results
Suprapapillary plates and granular layer were significantly thicker in patients with chronic dermatitis compared with patients with psoriasis. The rete ridges were longer and wider, the epidermis was thicker, and the parakeratotic layer was also thicker in patients with psoriasis compared with patients with chronic dermatitis, and the difference between these corresponding parameters in the two groups was statistically significant except for thickness of parakeratotic layer. Moreover, the mean ratio of minimal suprapapillary plate’s thickness to epidermal thickness and the mean ratio of minimal granular layer’s thickness to parakeratotic layer’s thickness were significantly higher in patients with chronic dermatitis compared with those with psoriasis.
Conclusion
Despite overlapping histopathologic features in psoriasis and chronic dermatitis, quantitative histopathologic criteria might be valuable for differentiation of these two conditions. Ratios of minimal suprapapillary plate’s thickness to epidermal thickness and minimal granular layer’s thickness to parakeratotic layer’s thickness can be particularly helpful in this regard.
Introduction
Psoriasis is an autoimmune chronic skin disease that may sometimes significantly impair quality of life.Citation1–Citation3 Overall prevalence of psoriasis in general population is different in different parts of the world, and some recent studies claim that its prevalence is increasing.Citation4 In western world, an estimated 2%–4% of general population are affected by the disease.Citation5 Moreover, psoriasis has been associated with several comorbidities (including cardiovascular, metabolic, and rheumatologic disorders), and these comorbidities are more prevalent in patients with more severe skin disease.Citation6–Citation19 Most researchers believe that psoriasis has multifactorial etiology, and both genetic and environmental factors contribute to its etiopathogenesis.Citation20 The most common clinical form of psoriasis is psoriasis vulgaris, characterized by symmetrically distributed erythematous plaques covered with scale.Citation21 In microscopic evaluation, a significant increase in epidermal thickness (acanthosis), downward extension of rete ridges, diminished granular layer, parakeratosis, thinning of suprapapillary plates, dilatation and tortuosity of capillaries in papillary dermis, Munro’s neutrophilic microabscesses and spongiform pustules of Kogoj constitute the histopathologic characteristics of psoriatic lesion. However, during different stages of evolution of a psoriatic plaque, only some of these features might be present. Munro’s neutrophilic microabscesses and spongiform pustules of Kogoj are considered to be diagnostic for psoriasis, but sometimes they might be absent.Citation22
Chronic dermatitis is clinically characterized by itching, scratching, ulceration, and lichenification of skin.Citation23 Its histopathologic changes include acanthosis, hyperkeratosis, spongiosis, lymphocytic exocytosis, superficial dermal fibrosis, and perivascular lymphocytic infiltration.Citation24
Although some findings such as Munro’s microabscesses and thinning of the granular layer are more common in psoriatic lesion, differentiating psoriasis from chronic dermatitis is generally difficult because many of their histologic features are identical.Citation22 Some studies had previously tried to clarify the histopathologic differences between psoriasis and chronic dermatitis, but their findings are not completely consistent.Citation25,Citation26 Furthermore, they had not used quantitative histopathologic methods to distinguish between these two diseases.
The aim of our study was to compare the histopathologic diagnostic features of psoriasis with chronic dermatitis quantitatively, in order to make the differentiation easier.
Patients and methods
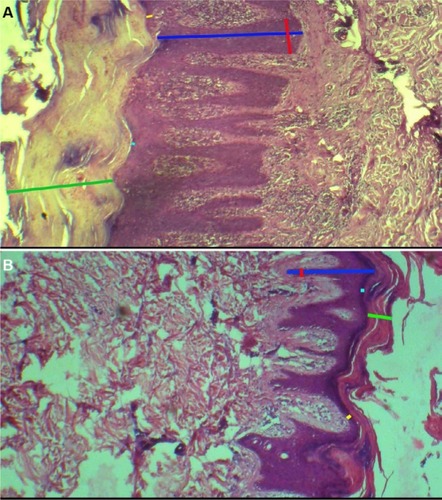
This cross-sectional study was conducted in Hamadan, west of Iran. The ethics committee of Hamadan University of Medical Sciences approved the study protocol (ethics committee code: IR.UMSHA.REC.1395.271), and written informed consent was obtained from all participants. Thirty patients with clinical diagnosis of psoriasis and 30 patients with clinical diagnosis of chronic dermatitis, whose biopsies also confirmed the clinical diagnosis, were included in the study. The definite diagnosis was based on clinicopathologic correlation (only individuals with typical clinical features along with typical histopathologic findings of psoriasis were included in the psoriasis group and vice versa). Demographic characteristics such as age and gender, as well as clinical information were recorded. Photos of histologic slides were obtained using LABOMED microscope and digital camera (LaboAmerica, Fremont, CA, USA) at two magnifications (×100 and ×400). A computer was connected to the camera, and Pixel Pro software (Labomed, Los Angeles, CA, USA) was installed on the computer for imaging and microscopic measurements. Width and length of rete ridges (at the longest rete ridge), minimal thickness of suprapapillary plates (defined as the shortest distance between the top of dermal papilla and cornified layer), thickness of epidermis (at the thickest part), thickness of hyperkeratotic layer (the thickest part of parakeratotic or orthokeratotic hyperkeratosis), and minimal thickness of granular layer (the thinnest portion of granular layer in the parakeratotic area) were determined using Pixel Pro software on the micrometer scale by a pathologist ().
Figure 1 (A) Histopathology of psoriasis (H&E ×100). (B) Histopathology of chronic dermatitis (H&E ×100).
In descriptive statistics section, mean and SD were used to report quantitative variables with normal distribution, while median was used for the remaining quantitative variables. Qualitative variables were also described using ratio and percentage. To compare the quantitative variables in two groups, independent samples t-test was used if the distribution was normal. For those variables without normal distribution, nonparametric tests (including Mann–Whitney U-test) were used. To compare the qualitative-nominal variables in the two groups (such as gender and anatomic location), chi-square test or Fisher’s exact test was used. All the statistical analyses were carried out using SPSS 16.0 for Windows (SPSS Inc., Chicago, IL, USA) and p-values <0.05 were considered significant.
Results
Thirty patients with psoriasis and 30 patients with chronic dermatitis were included in this study. Twenty-one patients with dermatitis were female (70%), while in the psoriasis group, 20 patients (66.7%) were male. The mean age of patients in the dermatitis group was not significantly different from the mean age of patients in the psoriasis group (41.86±17.44 versus 38.2±14.03 years, respectively). The most common anatomical location was upper limb in the dermatitis group (33.3%), while in the psoriasis group, it was lower extremity (36.7%).
The mean length of rete ridge in patients with psoriasis was higher than those with chronic dermatitis (4479.6 versus 2369.4 μm, respectively [p=0.001]). The mean width of rete ridge in patients with dermatitis was lower than those with psoriasis (580.4 versus 1053.9 μm, respectively [p=0.001]).
The mean thickness of suprapapillary plate in patients with psoriasis was lower than that in patients with chronic dermatitis (498.2 versus 621.6 μm, respectively [p=0.022]). Moreover, the average thickness of epidermis was higher in patients with psoriasis than that in patients with chronic dermatitis (5047.2 versus 2487.6 μm, respectively [p=0.001]).
The average thickness of granular layer in patients with chronic dermatitis was 133.9 μm, while in patients with psoriasis it was 41.7 μm (p=0.001). The mean thickness of parakeratotic layer in patients with chronic dermatitis was 1130.8 μm and in patients with psoriasis, it was 1228.6 μm, but this difference was not statistically significant (p=0.094; ).
Table 1 Comparison of quantitative histopathologic parameters between chronic dermatitis and psoriasis
The mean width to length ratio of rete ridge in patients with chronic dermatitis was lower than that in patients with psoriasis, but this difference was not significant (p=0.964). The mean ratio of suprapapillary plate’s thickness to epidermal thickness and the mean ratio of granular layer’s thickness to parakeratotic layer’s thickness were higher in patients with chronic dermatitis than in those with psoriasis (p=0.001 for both; ).
Table 2 Comparison of quantitative histopathologic parameter ratios between chronic dermatitis and psoriasis
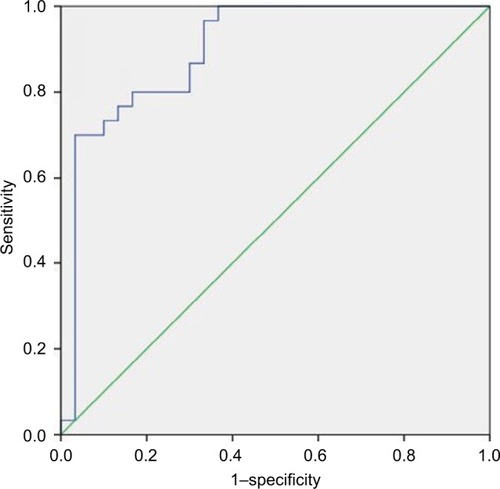
In receiver operating characteristic curve analysis, a ratio of 0.06 for granular layer’s thickness to parakeratotic layer’s thickness was the best cutoff point (sensitivity of 90% and specificity of 80%), thus the ratios ≤0.06 were in favor of the diagnosis of psoriasis (). Moreover, a ratio of 0.13 for suprapapillary plate’s thickness to epidermal thickness was the best cutoff point (sensitivity of 80% and specificity of 90%), thus the ratios ≤0.13 were in favor of the diagnosis of psoriasis ().
Figure 2 ROC curve for granular layer’s thickness to parakeratotic layer’s thickness ratio.
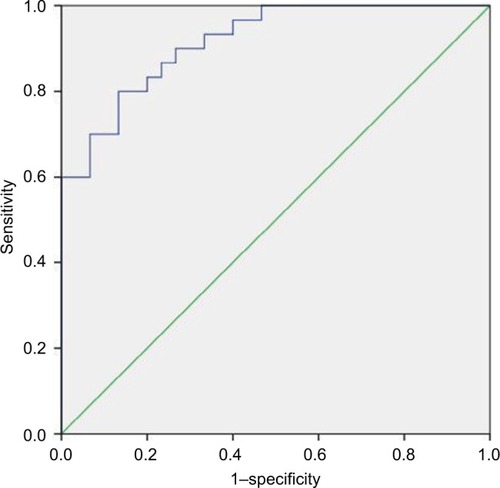
Figure 3 ROC curve for suprapapillary plate’s thickness to epidermal thickness ratio.
Discussion
Psoriasis is a chronic inflammatory skin disease with characteristic clinicopathologic findings, but its differentiation from chronic dermatitis may sometimes become difficult.
We showed that the thickness of suprapapillary plate and granular layer was greater in patients with chronic dermatitis compared with patients with psoriasis (p=0.022, p=0.001, respectively). We also demonstrated that the length and the width of rete ridge, the epidermal thickness, and the thickness of parakeratosis were greater in patients with psoriasis compared with those with chronic dermatitis, and the differences were significant except for the thickness of parakeratosis (p=0.001, p=0.001, p=0.001, p=0.094, respectively). Kamyab-Hesari et al have shown that in addition to Munro’s microabscesses and tortuosity of capillaries in the papillary dermis, hypogranulosis, suprapapillary thinning, and confluent parakeratosis were significantly in favor of the diagnosis of psoriasis.Citation25 Although their findings have not been quantitatively reported, they are consistent with ours. In another study conducted by Aydin et al 41.2% of patients with psoriasis had no granular layer compared to 36% of patients with chronic dermatitis.Citation26 Our quantitative findings are also consistent with their results. These findings point toward the importance of the loss of granular layer in differentiating psoriasis from dermatitis.
In our study, the thickness of parakeratotic layer was slightly greater in patients with psoriasis compared with those with chronic dermatitis, but the difference was not statistically significant. It should be noted that this parameter may be affected by excoriation in both conditions, and therefore it is not a reliable distinguishing factor.
Based on our findings, the suprapapillary plates were thinner in patients with psoriasis compared with those with chronic dermatitis (p=0.022). In the study conducted by Aydin et al, the suprapapillary thinning was also found to be more common in patients with psoriasis compared with those with dermatitis, but the difference was not significant. The absence of a significant difference in their study may be due to lack of quantitative measurements.
The findings of our study are also consistent with the study conducted by Mehta et al, in which suprapapillary thinning and the absence of granular layer were shown to be significantly more common in patients with psoriasis.Citation27
Given the histopathologic nature of psoriasis and chronic dermatitis, these findings are not unexpected. However, it should be kept in mind that the presence or absence of all these typical histologic features depends on the age of the lesion, the site of sampling, and the presence or absence of excoriation. The site of sampling is particularly important, because it can affect considerably the interpretation of epidermal thickness, length of rete ridges, granular layer’s thickness, and cornified layer’s thickness. In order to remove the confounding effects of this variable, we decided to use three ratios: width to length of rete ridge, thickness of suprapapillary plate to epidermal thickness, and granular layer’s thickness to parakeratotic layer’s thickness.
Although the mean ratio of width to length of rete ridge was lower in patients with chronic dermatitis compared with those with psoriasis, this difference was not statistically significant (p=0.964). We hypothesized that this is due to simultaneous increase in length and width of rete ridges in psoriasis.
The mean ratio of suprapapillary plate’s thickness to epidermal thickness and the mean ratio of granular layer’s thickness to parakeratotic layer’s thickness were higher in patients with chronic dermatitis compared with those with psoriasis (p=0.001 for both). This may be due to a significant difference in the thickness of suprapapillary plate and granular layer between the two groups.
Limitation
A major limitation of this study is that we examined typical cases of psoriasis and chronic dermatitis, while histopathology is mostly needed in borderline cases. However, our study is merely a starting point, and we had to begin with typical cases, but future studies should definitely concentrate on borderline ones.
Conclusion
The major differential diagnosis of psoriasis, both clinically and histopathologically, is chronic dermatitis. Despite the overlapping histopathologic features, some findings (such as diminished granular layer, parakeratosis, suprapapillary thinning, and Munro’s microabscesses) are in favor of the diagnosis of psoriasis. Unfortunately, all these parameters may be affected by the severity and duration of disease, secondary changes due to excoriation, and anatomical location of biopsy. We showed that by using quantitative parameters, diagnostic accuracy may be increased. Specifically, using the cutoff point of 0.06 for the ratio of granular layer’s thickness to parakeratotic layer’s thickness and 0.13 for the ratio of suprapapillary plate’s thickness to epidermal thickness may help to differentiate psoriasis from chronic dermatitis. In other words, ratios ≤0.06 for granular layer’s thickness to parakeratotic layer’s thickness and ≤0.13 for suprapapillary plate’s thickness to epidermal thickness are in favor of the diagnosis of psoriasis.
Acknowledgments
This study was conducted based on the approved MD thesis of Zahra Hamian (thesis no.: 9506023239), and we would like to thank the vice-chancellor for research and technology at Hamadan University of Medical Sciences for thesis approval.
Disclosure
The authors report no conflicts of interest in this work.
References
- LopesNPietriGHoweTSS38 – Psoriasis (PSO) patients’ profile and impact of the disease on patients’ quality of life and work productivity in a real-life setting in BrazilValue Health2017209A807
- GuptaMAGuptaAKQuality of life of psoriasis patientsJ Eur Acad Dermatol Venereol20001424124211204506
- KaufmanBPAlexisAFPsoriasis in skin of color: insights into the epidemiology, clinical presentation, genetics, quality-of-life impact, and Treatment of Psoriasis in Non-White Racial/Ethnic GroupsAm J Clin Dermatol Epub2017125
- DanielsenKOlsenAOWilsgaardTFurbergASIs the prevalence of psoriasis increasing? A 30-year follow-up of a population-based cohortBr J Dermatol201316861303131023374051
- ParisiRSymmonsDPGriffithsCEAshcroftDMIdentification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) project teamGlobal epidemiology of psoriasis: a systematic review of incidence and prevalenceJ Invest Dermatol2013133237738523014338
- YeungHTakeshitaJMehtaNNPsoriasis severity and the prevalence of major medical comorbidity: a population-based studyJAMA Dermatol2013149101173117923925466
- DattiloGBorgiaFGuarneriCCardiovascular risk in psoriasis: current state of the artCurr Vasc Pharmacol Epub20171116
- DattiloGImbalzanoECasaleMPsoriasis and cardiovascular risk: correlation between psoriasis and cardiovascular functional indicesAngiology2018691313729212353
- EgebergASkovLJoshiAAThe relationship between duration of psoriasis, vascular inflammation, and cardiovascular eventsJ Am Acad Dermatol2017774650656.e65328826925
- FurueMTsujiGChibaTKadonoTCardiovascular and metabolic diseases comorbid with psoriasis: beyond the skinIntern Med201756131613161928674347
- HuSCLanCEPsoriasis and cardiovascular comorbidities: focusing on severe vascular events, cardiovascular risk factors and implications for treatmentInt J Mol Sci20171810E221129065479
- GisondiPFostiniACFossaIGirolomoniGTargherGPsoriasis and the metabolic syndromeClin Dermatol2018361212829241748
- GuiXYYuXLJinHZZuoYGWuCPrevalence of metabolic syndrome in Chinese psoriasis patients: a hospital-based cross-sectional studyJ Diabetes Investig2018913943
- Rodriguez-ZunigaMJMGarcia-PerdomoHASystematic review and meta-analysis of the association between psoriasis and metabolic syndromeJ Am Acad Dermatol2017774657666.e65828917453
- SalunkeASNagargojeMVBelgaumkarVATolatSNChavanRBAssociation of metabolic syndrome in chronic plaque psoriasis patients and their correlation with disease severity, duration and age: a Case Control Study from Western MaharashtraJ Clin Diagn Res2017118WC06WC10
- SinghSYoungPArmstrongAWAn update on psoriasis and metabolic syndrome: a meta-analysis of observational studiesPLoS One2017127e018103928719618
- ZuoYGWuCDescalzoMAPsoriasis, metabolic syndrome, and systematic reviewsJ Diabetes Investig2017108323
- CarubbiFChimentiMSBlasettiGAssociation of psoriasis and/or psoriatic arthritis with autoimmune diseases: the experience of two Italian integrated Dermatology/Rheumatology outpatient clinicsJ Eur Acad Dermatol Venereol201529112160216825882399
- ModyEHusniMESchurPQureshiAAMultidisciplinary evaluation of patients with psoriasis presenting with musculoskeletal pain: a dermatology: rheumatology clinic experienceBr J Dermatol200715751050105117725678
- Di MeglioPVillanovaFNestleFOPsoriasisCold Spring Harb Perspect Med201448A01535425085957
- SaracGKocaTTBaglanTA brief summary of clinical types of psoriasisNorth Clin Istanb201631798228058392
- De RosaGMignognaCThe histopathology of psoriasisReumatismo200759Suppl 1464817828343
- MiyoshiHKanekuraTAokiTKanzakiTBeneficial effects of tissue inhibitor of metalloproteinases-2 (TIMP-2) on chronic dermatitisJ Dermatol200532534635316043896
- LeTKSchalkwijkJvan de KerkhofPCvan HaelstUvan der ValkPGA histological and immunohistochemical study on chronic irritant contact dermatitisAm J Contact Dermat19989123289471983
- Kamyab-HesariKSafaei-NaraghiZGhanadanANikooASabaghiMPalmoplantar psoriasis versus eczema: major histopathologic clues for diagnosisIran J Pathol201494251256
- AydinOEnginBOguzOIlvanSDemirkesenCNon-pustular palmoplantar psoriasis: is histologic differentiation from eczematous dermatitis possible?J Cutan Pathol200835216917318300385
- MehtaSSingalASinghNBhattacharyaSNA study of clinicohistopathological correlation in patients of psoriasis and psoriasiform dermatitisIndian J Dermatol Venereol Leprol2009751100