
Abstract
Atopic dermatitis (AD) is a common, chronic, relapsing–remitting inflammatory disease that can be challenging to treat. Patients with mild disease are usually managed well with good skin care practices including moisturization and appropriate bathing along with intermittent use of topical therapies such as topical corticosteroids and/or topical calcineurin inhibitors during flares. Patients with frequent flares may benefit from proactive application of topical therapies twice a week to the most troublesome areas. Patients with severe disease often present significant treatment challenges. Systemic therapies are usually required for severe AD but have varying degrees of success and can be associated with side-effect profiles that require counseling and close monitoring. Phototherapy has been shown to have success in treating moderate-to-severe AD, but several factors can limit its utility and efficacy including cost and access. New therapies are in development targeting specific pathways relevant for AD. Dupilumab was the first biologic treatment approved in North America, Europe, and Japan for adults with moderate-to-severe AD. Although this treatment can lead to rapid improvement in the majority of patients, there are inadequate responders. In this review, we discuss the clinical challenges and treatment options for moderate-to-severe refractory AD.
Introduction
Atopic dermatitis (AD) is a pruritic, inflammatory skin disorder that frequently presents in childhood but is also common in adults.Citation1 The pathogenesis of AD is due to a multitude of factors including skin barrier defects, dysregulation of innate immune responses, defects in adaptive immune response with development of strong type 2 immunity, and altered skin microbiome.Citation2,Citation3 Two of the major risk factors that predispose a person to developing AD include a positive family history of atopy and loss-of-function mutations in the filaggrin gene.Citation4 In most cases, AD is successfully managed through elimination of exacerbating factors, good skin care practices, and topical therapies as defined by the most recent AD treatment guidelines such as those set forth by the European Academy of Dermatology and Venereology in April 2018.Citation5 Patients with moderate-to-severe disease who fail to improve with this first-line, conventional therapy may benefit from second-line therapies such as phototherapy and systemic medications, including dupilumab. Even after employing these systemic treatments, there is a subset of patients who continue to suffer from extensive skin lesions and intense pruritus resulting in both physical and emotional disability. In cases of treatment resistance, factors such as poor compliance or incorrect medication use, lack of access to appropriate medications, hypersensitivity reactions to topical treatments, skin infections, and other exacerbating environmental triggers need to be considered. If these factors can be ruled out, one or several skin biopsies may be needed to rule out the possibility of other diagnoses such as cutaneous T-cell lymphoma (CTCL). In this article, we review the current treatment guidelines and the systemic therapies that are in late-stage clinical development (Phase III) that may help AD patients whose disease is recalcitrant to the currently employed systemic therapies.
Clinical presentation and diagnosis
The onset of AD classically occurs during early childhood. In infants, AD typically presents with red, scaly, pruritic lesions involving the face, scalp, trunk, and extensor surfaces of the extremities. Although AD can have a more generalized distribution, it typically involves the flexural aspects of the extremities in later childhood and adulthood.Citation6 AD can be categorized as acute (erythema, vesicles, bullae, weeping, crusting), subacute (scaly plaques, papules, erosions, and crusts), and chronic (lichenification, scaling, and hyperpigmentation or hypopigmentation) based on appearance.Citation7 Diagnosis of AD is largely based on clinical history and physical exam features.Citation8 Core features that must be present to establish a diagnosis of AD include the following: 1) pruritis; 2) acute, subacute, or chronic eczema; 3) representative morphology to include agespecific patterns and distribution; and 4) chronic or relapsing time course.Citation8 Features that help to support a diagnosis of AD include the following: 1) early age of onset, although adult onset is possible; 2) xerosis; and 3) personal or family history of atopy. Areas that are typically spared in AD include the axillary, gluteal, and perineal regions. If these areas are involved, other diagnoses such as allergic or irritant contact dermatitis, psoriasis, scabies, tinea, and erythroderma due to other causes should be considered.Citation8 In cases where a diagnosis is in doubt, skin biopsy or a more detailed history may be necessary to rule out other AD-like conditions that have distinctive histology such as nummular dermatitis, stasis dermatitis, seborrheic dermatitis, Id reaction, lichen simplex chronicus, prurigo nodularis, irritant contact dermatitis, allergic contact dermatitis, and dyshidrosis.
Treatments
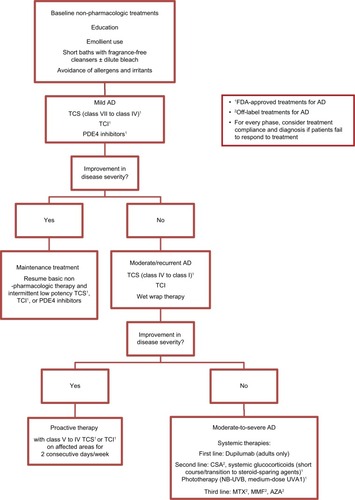
Careful environmental history and education are part of the management of all AD patients including education on the pathophysiology of AD, identification of patient-specific allergens, and avoidance of or reduced exposure to relevant allergens (where possible) as this often improves AD.Citation5 In this review, we outline a therapeutic ladder to consider based on disease severity ().
Figure 1 Therapeutic ladder for the treatment of AD.
Basic non-pharmacologic treatment
There are several known deficiencies in the skin barrier of patients with AD. These include filaggrin deficiency, decreased intercellular lipids, altered ratios of ceramides, fatty acids, and cholesterol, as well as reduced expression of tight junction proteins which individually or collectively are likely contributing to the increased transepidermal water loss characteristically observed in this disease.Citation9 Research suggests that barrier disruption enables the penetration of allergens, irritants, and potentially pathogenic microbes into the skin, resulting in inflammation.Citation10,Citation11 Because of this, patients with AD must be selective about the products they use on their skin, as they are at a greater risk for adverse reactions to known irritants and allergens.
In general, patients should be advised to choose skin care and laundry products (eg, cleansers, moisturizers, shampoo/conditioner, makeup, and laundry detergents) that are “fragrance free” and hypoallergenic.Citation5 It is important to note that even “scent-free” products may be made with fragrances and thus may still be allergenic or irritating. Patients should also avoid certain fabrics, such as wool and wool mixes, which may be bothersome because of the lanolin or simply by virtue of the texture which causes skin friction and may, therefore, worsen the itch–scratch cycle.Citation5 When bathing, patients should use warm (not hot) water and make sure to apply moisturizers immediately within 5 minutes to prevent the skin from drying out.Citation5
It is recommended that patients bathe for short durations of 5–10 minutes in warm water up to once daily with non-soap, hypoallergenic, and nonirritant cleansers or solutions to remove any allergens or irritants and to hydrate the skin.Citation5 While most patients with AD typically choose to shower, there is some evidence that soaking in a bathtub with dilute sodium hypochlorite (“bleach baths”) may be beneficial in reducing disease severity; however, studies are conflicting and bleach baths may not be any more effective than regular water baths.Citation12–Citation14 It is not known whether this bleach water should be rinsed off afterwards. As noted earlier, all bathing should be immediately followed by moisturizing.
The application of moisturizers is an integral part of managing AD as their consistent use reduces disease severity and likely lessens the need for pharmacologic interventions.Citation15 Moisturizers should contain emollients as well as occlusive and/or humectant agents to optimize skin hydration and be free of fragrances and additives.Citation16,Citation17 Moisturizers should be applied liberally and frequently to help mitigate xerosis. The most effective moisturizers are often ointments; however, some patients may find ointments too greasy for their day-to-day activities as they do not rub in and can stain clothing and bed linens.Citation18,Citation19 The next most effective vehicle is a thick or “emollient” cream that ideally is available in a large size so it has sufficient quantities to use as suggested (454 g per 1 pound in the US).Citation19 Creams may be better tolerated than ointments which may lead to better compliance. The pros/cons to these two vehicles should be discussed with the patient. Of note, some patients with many fissures or erosions may find that many topicals “sting” or “burn” due to the addition of preservatives such as propylene glycol, sorbitan sesquioleate, parabens, lanolin, fragrance, methylisothiazolinone, and formaldehyde-releasing preservatives.Citation20 Changing the vehicle to an ointment may reduce these symptoms as they often do not contain preservatives or other potential irritating ingredients.Citation18
Flare-directed (reactive) treatment
Due to the relapsing and remitting course of AD, many patients have achieved success in treating their disease more intensively during flares and scaling back treatment when their disease is better controlled. The optimal treatment modality for reactive treatment depends on the severity of disease, the location of the AD, and patient and physician preference. Additionally, it is important to consider whether AD flares are associated with secondary skin infections, which may require additional treatment.
Topical therapy
Topical corticosteroids
Topical corticosteroids (TCSs) are the first-line treatment for an acute flare of AD as they provide more rapid effects that lead to decreased inflammation and pruritus.Citation18,Citation19 The potency and vehicle of the TCSs should be tailored based on the age of the patient, disease severity, lesion location, patient preference, and cost.Citation18
Low-potency TCSs are best for mild disease and for sensitive areas such as the face, groin, or axilla.Citation19 Mid-potency TCSs are appropriate for most other body surfaces.Citation21 High-potency TCSs are best reserved for thick/lichenified skin such as the palms/soles of the feet and ankles, and for significant flares.Citation21 Although high-potency TCSs are more effective, they have a higher risk of local and rarely even systemic adverse effects (AEs).
Wet wrap therapy with an ointment moisturizer or a medium-potency TCS (ointment) can be considered during a flare.Citation24,Citation25
Topical calcineurin inhibitors
Topical calcineurin inhibitors (TCIs), including tacrolimus 0.1% ointment, tacrolimus 0.03% ointment, and pimecro-limus 1% cream, are considered second-line agents for the management of AD flares.Citation18,Citation22 TCIs are products of the bacteria, Streptomyces, which inhibit calcineurin-dependent T-cell activation by binding to FKBP-12, which inhibits calcineurin leading to a blockade in the signal transduction in the T-lymphocyte pathway and ultimately blocking the production of pro-inflammatory cytokines.Citation18,Citation23 There is conflicting evidence on the interaction between TCIs and the skin barrier in AD patients. Some studies suggest that TCIs decrease synthesis of epidermal lipids and antimicrobial peptides leading to increased permeability of the skin barrier and decreased antimicrobial function, while others suggest that TCIs can improve clinical and biophysical properties of the barrier function.Citation24,Citation25 TCIs are steroid sparing, which is an important consideration for patients who may need long-term treatment with TCSs and are therefore at a greater risk for the aforementioned side effects. TCIs decrease inflammation, with an effectiveness similar to that of a mid-potency TCS.Citation26,Citation27 TCIs can be an appropriate choice for patients with AD on the eyelids, face, groin, or armpits. While only tacrolimus 0.03% ointment is approved by the US Food and Drug Administration (FDA) for children aged 2–15 years with moderate-to-severe AD, both tacrolimus 0.03% and the stronger 0.1% ointment are approved for patients older than 15 years with moderate-to-severe AD.Citation18 Pimecrolimus 1% cream is approved for patients with mild-to-moderate AD aged 2 years and up.Citation18
Of note, TCIs come with an FDA Black Box Warning based on the theoretical risk of malignancy from systemic calcineurin inhibitors in animal studies and transplant patients. However, clinical trials, post-marketing surveillance, and pharmacokinetic and toxicology studies have found that the overall rate of malignancy in patients treated with TCIs is no more than the general population.Citation28 The most common side effect reported from TCIs is skin “burning” or “stinging” which may lead some patients to prematurely discontinue the use of TCIs. However, this sensation typically resolves within a week of use. Additionally, pre-cooling the TCI tube may reduce the burning sensation.Citation29
Topical PDE4 inhibitors
In December 2016, the first topical PDE4 inhibitor, crisaborole 2% ointment, was approved for the treatment of mild-to-moderate AD in patients aged 2 years and up.Citation30,Citation31 PDE4 inhibitors suppress the production of cytokines and ROS, which have been shown to play a role in perpetuating the skin barrier defect and inflammation associated with AD.Citation32 This drug has been shown to be safe and effective in randomized controlled trials (RCTs) for up to 1 year of treatment. The most common treatment-related AE experienced was skin burning.Citation30,Citation33
Proactive (maintenance) therapy
In cases of moderate or recurrent AD, proactive treatment is usually recommended as it has been shown to reduce the risk of relapse.Citation34 Proactive therapy is defined as the use of a topical anti-inflammatory agent usually twice a week for 2 consecutive days (weekend therapy) to previously affected areas of skin in combination with the daily, liberal use of moisturizers over entire body for an undefined but long-term period of time.Citation35 Classically, medium-potency TCSs or TCIs are recommended as the topical anti-inflammatory agents of choice.Citation19 Proactive therapy can decrease the frequency of AD flares while minimizing potential side effects typically associated with medium- or high-potency TCSs.
Systemic therapy
In cases of severe AD with inadequate control despite optimized topical treatment, systemic therapy may be considered. The only two FDA-approved systemic treatments in the US at the time of submission are dupilumab and systemic steroids. Cyclosporine (CsA) is approved in some European countries and Japan.Citation36
Dupilumab
Dupilumab is a fully humanized monoclonal antibody against the shared alpha subunit of IL-4 and IL-13 receptors, which blocks the actions of these two canonical T-helper type 2 (Th2) cytokines that are commonly found in the skin of AD patients.Citation37 Dupilumab was FDA approved in March 2017 for the treatment of moderate-to-severe AD in adults and is now considered a first-line systemic treatment. Two large (n=671 and n=708), long-term (16 weeks), randomized, double-blind, placebo-controlled trials (RDBPCTs) with subcutaneous dupilumab showed a rapid and significant improvement in disease severity (Eczema Area and Severity Index, EASI) and extent of involvement (body surface area, BSA).Citation38 The addition of TCSs to dupilumab treatment resulted in even greater improvement of AD signs and symptoms compared to dupilumab alone.Citation39 The most common side effects associated with dupilumab include a range of ocular complaints commonly reported as dry eye, noninfectious conjunctivitis, and blepharitis. Dupilumab does not require lab monitoring or screening for tuberculosis or hepatitis B/C. Additionally, there appears to be no increased infection risk in those treated with dupilumab.Citation39
Recommendation
Dupilumab is recommended as a first-line treatment choice for moderate-to-severe AD given the efficacy and safety demonstrated in two large, long-term RCTs. TCS, TCI, and crisaborole can be used in conjunction with dupilumab to address an AD flare.
Systemic glucocorticoids
Glucocorticoids, while being both FDA approved and nearly universally effective, should be used rarely and only as a bridge to a more sustainable treatment plan. There are no high-quality RCTs evaluating the safety and efficacy of systemic glucocorticoids in AD. A systematic review on the safety and efficacy of systemic corticosteroids in AD recommended that their use should be limited to short courses when other options are unavailable, for the immediate relief of acute flares, as a transition to a steroid-sparing treatment, or in the most severe, treatment-refractory cases.Citation40,Citation41 The most recent guidelines set forth by the European Task Force on Atopic Dermatitis suggest an initial dose of 0.5 mg/kg/day for 1–2 weeks which should be tapered over 1 month to decrease the risk of rebound.Citation5 The taper should overlap with a steroid-sparing agent. Special consideration should be made with pediatric patients due to potential concern of delayed or reduced bone growth.Citation42
Recommendation
Systemic glucocorticoids should be used very rarely and only for a short duration with slow taper off due to the serious side effects with long-term treatment even with low-dose corticosteroids (≤15 mg/day prednisone-equivalent) or recurrent courses because of the high risk of serious side effects including fractures, gastrointestinal (GI) hemorrhages, cataracts, obesity, growth delay/reduction, and infections.Citation43
Cyclosporine
CsA is approved for the treatment of adults (ie, ≥16 years) with AD in at least 15 European countries, Australia, and Japan. CsA is an oral calcineurin inhibitor, which suppresses the activation of the T-cell transcription factor, NF-AT, and thereby prevents the transcription of a number of cytokines including IL-2, thus diminishing inflammation.Citation42,Citation44 A 2013 systematic review found that CsA successfully improved AD with a mean improvement of 50%–95% as assessed by various clinical severity scores after 10 days to 8 weeks of treatment.Citation45 The head-to-head trials included in this review showed that CsA was more effective than intravenous immu-noglobulin, prednisolone, and phototherapy.Citation45 The most recent American Academy of Dermatology (AAD) guidelines recommend an initial dose of 3–6 mg/kg/day, citing that higher initial doses lead to quicker control of the disease and improvement in quality-of-life measures.Citation42 A dose of 5 mg/kg/day is usually considered maximum in dermatology. CsA has been viewed as a short-term or temporizing treatment for uncontrolled AD and should be used to transition (albeit more slowly than systemic glucocorticoids) to a safer, longer-term treatment. There is general consensus that continuous treatment with CsA beyond 1–2 years is not recommended primarily because of the risk of irreversible renal disease.Citation42 Most common side effects of CsA include hypertension and nephrotoxicity which are both dose and duration dependent.Citation45 Other side effects include hypertrichosis, headaches, nausea, diarrhea, gingival hyperplasia, and low serum magnesium.Citation45
Recommendation
CsA can be recommended as an effective second-line or shorter-term treatment for moderate-to-severe AD based on several high-quality RCTs.Citation45 Larger long-term studies are needed to fully clarify best practices to monitor for nephrotoxicity in the AD population before being recommended for greater than 1–2 years of treatment.
Phototherapy
Ultraviolet (UV) radiation has been shown to be an effective treatment modality in moderate-to-severe AD due to its proposed ability to decrease Staphylococcus aureus colonization, improve skin barrier function, reduce pruritis, and decrease tissue inflammation associated with AD.Citation46,Citation47 Four hundred and twenty-eight studies and 19 RCTs that enrolled over 900 subjects found medium-dose UVA1 phototherapy and narrowband (NB)-UVB phototherapy to be the safest and most effective phototherapies for moderate-to-severe AD subjects, with similar efficacy.Citation48–Citation51 NB-UVB has also been shown to be safe and effective in children as young as 3 years old; however, it is generally recommended for older children.Citation48 Phototherapy is usually well tolerated by patients. Potential side effects include xerosis, pruritus, erythema, and burning of the skin.Citation43,Citation49 The potential for photocarcinogenesis with both UVA1 and NB-UVB phototherapy has not been determined.Citation46,Citation46 NB-UVB is the most commonly employed phototherapy approach in the US to treat AD.
Recommendation
Phototherapy, especially NB-UVB and medium-dose UVA1, is recommended as a second-line treatment modality for both short- and long-term management of moderate-to-severe AD in children and adults given its safety and efficacy profile from numerous high-quality RCTs. Phototherapy can be used in conjunction with emollients and TCSs to reduce flare ups. Phototherapy is not typically recommended for infants or young children until they can dependably stand still in the unit and wear appropriate eye protection.
Methotrexate
Methotrexate (MTX) is a chemotherapeutic agent that blocks the synthesis of DNA, RNA, and purines, by inhibiting dihydrofolate reductase which, in turn, inhibits lymphocyte functions.Citation42 In a small (n=42), 12-week RCT, MTX (10–22.5 mg/week) was found to have similar efficacy to azathioprine (AZA) (1.5–2.5 mg/kg/day) as found using the SCORing Atopic Dermatitis (SCORAD) severity score with reductions of ~40% in both treatment groups of adults with severe AD.Citation52 The frequency of AEs was similar in both treatment arms, and most of the AEs were classified as mild. In another small (n=40), 12-week RCT, low-dose MTX (7.5 mg/week) was compared with low-dose CsA (2.5 mg/kg/day) in children aged 8–14 years with severe AD.Citation53 After 12 weeks, both groups showed similar reductions in SCORAD score, with a 49% reduction in the MTX group compared to 45% in the CsA group.Citation53 In this study, CsA showed a rapid onset of action (2–3 weeks) compared to a slightly slower onset with MTX (3–5 weeks), but upon discontinuation, MTX was associated with a longer time to relapse (20 weeks) compared to CsA (14 weeks).Citation53 The most recent AAD guidelines recommend starting doses of MTX between 7.5 and 25 mg weekly in conjunction with 1 mg folic acid daily to help mitigate MTX toxicities.Citation42 When clearance or near-clearance is achieved and maintained, MTX should be tapered or discontinued, using emollients and topical agents to maintain the remission. If there is no response after 12–16 weeks, an alternative therapy should be considered.Citation42 The most common side effects are nausea, other GI symptoms, and stomatitis. The most serious side effects are bone marrow suppression, pulmonary fibrosis, and hepatotoxicity.Citation42 The risk of these potentially serious side effects is thought to be lower in the AD population compared to those with psoriasis, possibly due to lower rates of obesity, alcoholism, metabolic syndrome, and polypharmacy.Citation42
Recommendation
MTX is recommended as a third-line option for the long-term treatment of children (≥8 years) and adults with moderate-to-severe AD based on two small, long-term RCTs. This treatment may be especially useful in patients who are not candidates for CsA.
Mycophenolate mofetil (MMF)
MMF and mycophenolate sodium inhibit purine synthesis in B and T lymphocytes by directly inhibiting inosine monophosphate dehydrogenase.Citation54 The overall efficacy of MMF is dependent on a UGT1A9 polymorphism that ultimately affects the metabolism of MMF.Citation55 In a 2017 study assessing UGT1A9 enzyme activity and MMF bioavailability, 85% of subjects who carried the UGT1A9 polymorphism were MMF nonresponders, presumably due to a suboptimal exposure to MMF.Citation55 Studies assessing the efficacy of MMF in AD are extremely limited. One small (n=55), 36-week RCT compared enteric-coated mycophenolate sodium (EC-MPS) with CsA in adult AD patients who failed treatment with potent TCSs.Citation56 Patients were initially treated with CsA 5 mg/kg/day for 6 weeks and then randomized to CsA 3 mg/kg/day or EC-MPS 1,440 mg/day for 30 weeks. After the first 10 weeks, the reduction in SCORAD score was greater in the CsA treatment group; however, by the end of the maintenance phase, disease activity was similar in both groups.Citation56 Once treatment was discontinued, relapse occurred faster in the CsA group compared to the EC-MPS group.Citation56 AEs were mild and transient within both groups. Two small (n=14, n=12) retrospective case series have been conducted on the use of MMF as a monotherapy in children (age 2–17 years), and the results showed a significant improvement in disease severity.Citation57,Citation58 Recommended starting doses for MMF are 1,000–1,500 mg twice a day for adults and 20–50 mg/kg/day in children.Citation59
Recommendation
MMF or EC-MPS may be promising third-line agents in patients with moderate-to-severe AD who fail or are not candidates for the other off-label immunosuppressants. Larger, long-term RCTs are needed to make any further recommendations on dosing, monitoring, and long-term therapy for moderate-to-severe AD. Screening for UGT1A9 polymorphisms prior to the initiation of treatment could be considered to identify potential nonresponders to MMF.
Azathioprine
AZA works by inhibiting purine synthesis and therefore inhibits RNA and DNA production especially in highly proliferative cells such as white blood cells commonly found in many inflammatory diseases.Citation42 It is FDA approved for the treatment of rheumatoid arthritis (RA) and prophylaxis against renal transplant rejection but is used off-label in refractory AD. The efficacy of AZA in the treatment of AD has been evaluated in several studies. Two adult RCTs have shown AZA to be more effective than placebo over 12 weeks.Citation60,Citation61 The Six Area Six Sign Atopic Dermatitis (SASSAD) score fell by 37% vs 20% in adults with moderate-to-severe AD treated with either 1 or 2.5 mg/kg/day based on thiopurine methyltransferase (TPMT) activity over placebo.Citation61 Knowing a patient’s TMPT level prior to treatment is important as low or absent enzyme activity increases the risk of AZA toxicity such as myelosuppression.Citation45 In a small, crossover trial testing 2.5 mg/kg/day in patients with severe AD, the treatment reduced SASSAD score by 26% compared to 3% in the placebo group.Citation60 AZA at doses of 1.5–2.5 mg/kg/day and MTX at doses of 10–22.5 mg/week were found to be equally efficacious over a 12-week regimen in a comparative study with similar reductions in SCORAD score.Citation52 The most recent dosing guidelines established by the AAD recommend a dose range between 1 and 3 mg/kg/day.Citation42 A delayed therapeutic effect may be noted with AZA requiring upwards of 12 weeks of medication to achieve full clinical benefit. Once clearance of AD has been obtained, AZA should be tapered to discontinuation with the use of TCSs, TCIs, and emollients for maintenance. Most common side effects of AZA include nausea and vomiting.Citation42,Citation52,Citation53 Long-term use has been associated with lymphopenia, progressive anemia, nonmelanoma skin cancer, and transient elevation of liver enzymes.Citation42,Citation45 Additionally, there is evidence that AZA treatment is associated with a dose- and duration-dependent increased risk of non-Hodgkin’s lymphoma and hepatosplenic T-cell lymphoma.Citation62–Citation65
Recommendation
AZA is recommended as a third-line treatment for moderate-to-severe AD given its modest level of effectiveness as seen in a few small studies. AZA is usually reserved for patients who are not candidates for other third-line agents given its safety profile.
Treatment failure
If patients fail to respond to any of the aforementioned available treatments for AD, factors such as poor compliance and incorrect use of the prescribed therapy need to be explored. Given the magnitude of misinformation available to patients and/or their caregivers about AD therapies, it is imperative that physicians provide clear and easy-to-understand instructions so that patients understand and are comfortable with the prescribed treatment regimen. Additionally, a strong emphasis needs to be placed on the chronic relapsing and remitting nature of this disease and appropriate care must continue despite improvement in disease severity with the prescribed treatment regimen. If poor compliance and incorrect medication use are determined not to be contributing to treatment failure, other factors that need to be explored include hypersensitivity reactions to topical treatments, skin infections, and other exacerbating environmental triggers. If these factors can be ruled out, it is then necessary to rule out AD mimickers including but not limited to allergic contact dermatitis, irritant contact dermatitis, seborrheic dermatitis, psoriasis, scabies, and tinea. Additionally, serial biopsies may be warranted to rule out CTCL.
Emerging therapies currently in Phase III clinical trials
Tofacitinib
Tofacitinib is a JAK inhibitor, currently FDA approved for the treatment of RA as an oral agent. Tofacitinib reduces the production of pro-inflammatory cytokines by interfering with the signaling of multiple cytokines relevant for allergic diseases including IL-4, IL-5, IL-13, IL-31, IL-33, and thymic stromal lymphopoietin.Citation66 A topical formulation of tofacitinib 2% ointment for the treatment of mild-to-moderate AD was evaluated in a small (n=69) 4-week Phase IIa RCT, which showed a significant change from baseline in the EASI score in patients treated with tofacitinib (–81.7% change) compared to placebo (−29.9% change).Citation67 Additionally, 73% of subjects treated with tofacitinib had an Investigator Global Assessment (IGA) score indicating clearance or near-clearance at the end of the 4-week study compared to 22% of the subjects treated with placebo.Citation67 The overall incidence of AEs was lower in the treatment group vs the placebo group, and AEs were classified as mild.Citation67 Long-term and comparative trials with other topical treatments are recommended to further assess long-term safety and efficacy.
Upadacitinib
Upadacitinib is an oral JAK1 inhibitor that is being investigated for use in moderate-to-severe AD.Citation68 In a small (n=166), Phase II RCT, adult patients were randomized to placebo, or 7.5, 15, or 30 mg upadacitinib administered once daily for 16 weeks. All doses produced a statistically significant improvement in EASI and IGA scores compared to placebo.Citation68 Significant reductions in itch were seen as early as 1 week with reductions in disease severity revealed by EASI and IGA scores by 2 weeks for all doses.Citation68 The 30 mg dose led to a 74% mean reduction in EASI score at 16 weeks compared to 23% reduction in the placebo group (P<0.001). The most common AEs were upper respiratory tract infections and acne.Citation68 Long-term RCTs are necessary to further explore the safety profile of upadacitinib.
PF-04965842
PF-04965842 is an oral JAK1 inhibitor that is being investigated for use in moderate-to-severe AD.Citation69 In a Phase II (n=269) RCT, adult patients were randomized to placebo, or 10, 30, 100, or 200 mg PF-04965842 once daily for 12 weeks.Citation70 A statistically significant improvement in IGA score was seen with the 200 mg dose compared to placebo, and statistically significant improvements in the EASI score were observed in the 100 and 200 mg dosing groups compared to placebo group.Citation70 The most common AEs were headache, nausea, diarrhea, and upper respiratory tract infections across all dosing groups and placebo group.Citation70 Larger, long-term RCTs are needed to further explore the efficacy and safety of PF-04965842.
Baricitinib
Baricitinib is an oral JAK1 and JAK2 inhibitor currently approved for RA in Europe and Japan.Citation71 In a small (n=124) Phase II RDBPCT, patients were randomized to once-daily placebo, or 2 or 4 mg baricitinib for 16 weeks after a 4-week run-in of daily TCS use. More patients receiving 4 mg of baricitinib achieved a 50% reduction in their EASI score compared to those receiving placebo (61% vs 37%) at week 16, and baricitinib also significantly improved pruritus and sleep loss.Citation71 AEs were dose dependent, and the most common ones in the baricitinib 4 mg group included headache, increased creatinine phosphokinase, and nasopharyngitis.Citation71 Larger, long-term trials to assess the safety and efficacy of baricitinib as a monotherapy are needed.Citation72
Tradipitant
Tradipitant is an NK-1R antagonist that is being developed to reduce itch in patients with AD.Citation69 NK-1R and SP are postulated to regulate both neurogenic inflammation and pain perception.Citation69 NK-1R and SP are also expressed by endothelial and immune cells, and high levels of SP are strongly associated with pruritus in chronic inflammatory dermatoses.Citation73,Citation74 In a Phase II proof-of-concept study, 69 adult patients with treatment-resistant pruritus associated with AD were randomized to receive either 100 mg of tradipitant once daily or placebo for 4 weeks. Tradipitant-treated patients had a significant improvement in the VAS score compared to baseline; however, there was not a statistically significant difference between the tradipitant and placebo groups in the VAS, SCORAD, or EASI score. Larger, long-term RCTs with different dosing regimens are needed to truly determine whether this drug is an effective treatment for AD-associated pruritus.
Nemolizumab
Nemolizumab is a humanized monoclonal antibody targeted against IL-31 receptor. IL-31 is a cytokine associated with pruritis and chronic skin inflammation.Citation76 A 12-week, Phase II RCT evaluated the efficacy of nemolizumab in the treatment of adult subjects with moderate-to-severe AD. This medium-sized (n=264) RCT demonstrated that nemolizumab at three different doses (0.1, 0.5, and 2 mg/kg) was superior to placebo at reducing pruritis. Additionally, modest improvements in EASI scores and BSA affected were also observed but only at the two highest doses (0.5 and 2 mg/kg) compared to placebo.Citation77 The overall incidence of AEs was similar to that observed in the placebo group, and AEs were classified as mild with the most frequent AEs being AD exacerbation and respiratory tract infections.Citation77 Long-term and comparative trials with other treatments are recommended to better assess long-term safety and efficacy.
Lebrikizumab
Lebrikizumab is a monoclonal antibody directed against IL-13, a Th2 cytokine that has been shown to play a key role in barrier dysfunction, defects in innate immunity, allergen sensitization, and inflammation associated with AD.Citation78 In a 12-week, medium-sized (n=209), Phase II RCT in adult patients with moderate-to-severe AD, 82.4% of patients treated with 125 or 250 mg doses of lebrikizumab (every 4 weeks) in conjunction with a TCS achieved the primary end point of a 50% reduction in the EASI score compared to 62.3% in the placebo group (P=0.026).Citation79 AEs were similar between treatment and placebo groups and were mostly mild to moderate.Citation79 While this trial shows promising results for lebrikizumab as a concomitant therapy in the treatment of moderate-to-severe AD, trials assessing its efficacy as a monotherapy are needed as well as long-term and comparative trials with other systemic therapies.
Tralokinumab
Tralokinumab is a humanized monoclonal antibody that targets and inhibits IL-13, a Th2 cytokine strongly linked to AD pathogenesis.Citation80 A 12-week, medium-sized (n=204), Phase IIb RCT of adult patients with moderate-to-severe AD evaluated several doses of tralokinumab (45, 150, or 300 mg) given every 2 weeks for 12 weeks vs placebo. More patients receiving the 300 mg dose reached an IGA score of 0 or 1 (26.7%) compared to the placebo group (11.8%).Citation81 AEs were similar between treatment and placebo groups with the most common AEs being upper respiratory infections.Citation81 Larger, long-term trials are recommended to more completely assess long-term safety and efficacy. Studies assessing the efficacy of tralokinumab as a monotherapy are ongoing.
Fezakinumab
Fezakinumab is a monoclonal antibody that targets IL-22, which is thought to have a unique role in some of the epithelial abnormalities associated with AD.Citation82 In a small (n=60) Phase II RCT, adult patients with moderate-to-severe AD were treated with intravenous fezakinumab or placebo every 2 weeks for 10 weeks. Reductions in SCORAD score were observed in all treatment arms, but the decline was only significantly different in patients with severe AD.Citation82 AEs were similar between treatment and placebo group and were classified as mild with the most common AE being upper respiratory infections.Citation82 Future studies evaluating the benefits of fezakinumab may demonstrate greater efficacy if enrollment targeted AD patients with high tissue expression of IL-22.Citation83–Citation85
Ustekinumab
Ustekinumab is a human monoclonal antibody that binds to the shared p40 protein subunit of human IL-12 and IL-23, thereby preventing interaction with their shared receptor.Citation86 It is currently approved for Crohn’s disease, plaque psoriasis, and psoriatic arthritis. In a systematic review of ustekinumab in the treatment of AD including eight cases and two RCTs (n=107), a total of 58% of patients showed improvement in their AD.Citation86 While ustekinumab was well tolerated, it is likely that it may only be effective for a subset of AD patients such as those with early-onset AD and possibly AD subjects of Asian descent.Citation87,Citation88
Conclusion
The foundation of AD treatment is gentle skin care and frequent moisturization use. A graded, reactive approach with low- to mid-potency TCS, TCI, or crisaborole should be added for flares of mild AD. For patients with moderate AD, the use of mid- to high-potency TCS is typically warranted until treatment can be de-escalated. For those with frequent relapses, proactive mid- to high-potency TCS or TCI should be used on the previously affected areas. If these treatment options do not result in sufficient improvement, systemic therapies are the next step in the therapeutic ladder. Dupilumab is the current first-line systemic agent for adults with moderate-to-severe, treatment-resistant eczema. If treatment with dupilumab is not successful, second-line treatments should be considered including CsA or phototherapy (NB-UVB or UVA1). Short-term systemic glucocorticoids should only be used as a bridge to a more sustainable treatment or for the most severe, refractory cases. Third-line treatment options include MTX, MMF, and AZA. For patients who fail to respond to any of the currently approved treatments for AD, factors such as poor compliance or incorrect medication use, hypersensitivity reactions to topical treatments, skin infections, and other exacerbating environmental triggers need to be considered. If these factors can be excluded, one or several skin biopsies may be warranted to rule out AD mimickers such as CTCL. There are several new therapies currently in Phase III clinical trials with strong evidence of efficacy for mild-to-moderate and moderate-to-severe AD. If FDA approval is granted, these additional therapies will provide additional options for treatment-resistant disease and may enable a more individualized approach to refractory AD.
Key points
An accurate diagnosis is imperative to establish an effective treatment regimen.
Good skin care with the use of moisturizers and gentle skin cleansers, and avoidance of triggers is a necessary first step, regardless of disease severity.
A systematic approach with topical anti-inflammatory therapies should be used in mild-to-severe AD and during flares of all degrees of severity.
Dupilumab and phototherapy are the next steps if good skin care and topical anti-inflammatory agents are not sufficient.
For patients who do not have access to dupilumab or phototherapy, are incomplete responders or nonresponders, or have significant side effects, systemic therapy with cyclosporine, mycophenolate, azathioprine, or methotrexate is recommended. Combination therapy such as dupilumab plus another systemic immunomodulatory agent and/or phototherapy has not been adequately studied.
For the subset of patients who fail to respond to several systemic treatments, it is necessary to rule out AD mimickers including but not limited to allergic contact dermatitis, irritant contact dermatitis, seborrheic dermatitis, psoriasis, scabies, and tinea. Additionally, serial biopsies may be warranted to rule out cutaneous T-cell lymphoma.
Disclosure
Brian B Johnson serves as an investigator for Regeneron Pharmaceuticals, Inc., Eli Lilly, and Pfizer. Abigail I Franco serves as an investigator for Regeneron Pharmaceuticals, Inc., Eli Lilly, and Pfizer. Lisa A Beck serves as an investigator for Regeneron Pharmaceuticals, Inc., AbbVie, Realm Therapeutics, and Pfizer, and as a consultant for Allakos, Astra-Zeneca, Boehringer-Ingelheim, Celgene, GSK, Leo Pharma, Eli Lilly, Novan, Novartis, and Sanofi-Genzyme, and owns stock in Pfizer and Medtronic. James C Prezzano serves as an investigator for AbbVie, Realm Therapeutics, Pfizer, and Regeneron Pharmaceuticals, Inc. The authors report no other conflicts of interest in this work.
References
- KangKPolsterAMNedorostSTAtopic Dermatitis Dermatology2New YorkMosby2003199
- KuoIHYoshidaTDe BenedettoABeckLAThe cutaneous innate immune response in patients with atopic dermatitisJ Allergy Clin Immunol2013131226627823374259
- BoguniewiczMLeungDYMAtopic dermatitis: a disease of altered skin barrier and immune dysregulationImmunol Rev2011242123324621682749
- IrvineADMcleanWHILeungDYMFilaggrin mutations associated with skin and allergic diseasesN Engl J Med2011365141315132721991953
- WollenbergABarbarotSBieberTGlobal Allergy and Asthma European Network (GA2LEN) and the European Union of Medical Specialists (UEMS)Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: Part IJ Eur Acad Dermatol Venereol201832565768229676534
- PugliarelloSCozziAGisondiPGirolomoniGPhenotypes of atopic dermatitisJDDG: Journal der Deutschen Dermatologischen Gesellschaft201191122021054785
- RudikoffDLebwohlMAtopic dermatitisThe Lancet1998351911717151721
- EichenfieldLFTomTWChamlinSLGuidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitisJ Am Acad Dermatol201470233835124290431
- WeidingerSBeckLABieberTKabashimaKIrvineADAtopic dermatitisNat Rev Dis Primers201841:129930242
- KuboANagaoKAmagaiMEpidermal barrier dysfunction and cutaneous sensitization in atopic diseasesJ Clin Invest2012122244044722293182
- OuchiTKuboAYokouchiMLangerhans cell antigen capture through tight junctions confers preemptive immunity in experimental staphylococcal scalded skin syndromeJ Exp Med2011208132607261322143886
- HonKLTsangYCLeeVWEfficacy of sodium hypochlorite (bleach) baths to reduce Staphylococcus aureus colonization in childhood onset moderate-to-severe eczema: a randomized, placebo-controlled cross-over trialJ Dermatol Treat2016272156162
- HuangJTRademakerAPallerASDilute bleach baths for Staphylococcus aureus colonization in atopic dermatitis to decrease disease severityArch Dermatol2011147224624721339459
- ChopraRVakhariaPPSacotteRSilverbergJIEfficacy of bleach baths in reducing severity of atopic dermatitis: A systematic review and meta-analysisAnn Allergy Asthma Immunol2017119543544029150071
- EichenfieldLFTomWLBergerTGGuidelines of care for the management of atopic dermatitisJ Am Acad Dermatol201471111613224813302
- ElmariahSBLernerEATopical therapies for pruritusSemin Cutan Med Surg201130211812621767774
- GiamYCHebertAADizonMVA review on the role of moisturizers for atopic dermatitisAsia Pac Allergy20166212012827141486
- EichenfieldLFTomWLBergerTGGuidelines of care for the management of atopic dermatitis: Section 2. Management and treatment of atopic dermatitis with topical therapiesJ Am Acad Dermatol201471111613224813302
- KapurSWatsonWCarrSAtopic dermatitisAllergy Asthma Clin immunol201814Suppl 2525230275844
- ColoeJZirwasMJAllergens in corticosteroid vehiclesDermatitis: Contact, Atopic, occupational, Drug20081913842
- RathiSKD’SouzaPRational and ethical use of topical corticosteroids based on safety and efficacyIndian J Dermatol201257425125922837556
- GutfreundKBieniasWSzewczykAKaszubaATopical calcineurin inhibitors in dermatology. Part I: properties, method and effectiveness of drug usePostepy Dermatol Alergol201330316516924278069
- NghiemPPearsonGLangleyRGTacrolimus and pimecrolimus: from clever prokaryotes to inhibiting calcineurin and treating atopic dermatitisJ Am Acad Dermatol200246222824111807435
- KimMJungMHongSPTopical calcineurin inhibitors compromise stratum corneum integrity, epidermal permeability and antimicrobial barrier functionExp Dermatol201019650151019703225
- Valdman-GrinshpounYBen-AmitaiDZvulunovABarrier-restoring therapies in atopic dermatitis: current approaches and future perspectivesDermatol Res Pract2012201292313422956938
- El-BatawyMMBosseilaMAMashalyHMHafezVSTopical calcineurin inhibitors in atopic dermatitis: a systematic review and meta-analysisJ Dermatol Sci2009542768719303745
- Ruer-MulardMAbererWGunstoneATwice-daily versus once-daily applications of pimecrolimus cream 1% for the prevention of disease relapse in pediatric patients with atopic dermatitisPediatr Dermatol200926555155819840309
- LebwohlMGowerTA safety assessment of topical calcineurin inhibitors in the treatment of atopic dermatitisMedGenMed20068488
- Al-KhenaizanSPractical tip: Precooling topical calcineurin inhibitors tube; reduces burning sensationDermatol Online J201016416
- PapierAStrowdLCAtopic dermatitis: a review of topical nonsteroid therapyDrugs in Context2018721252129632548
- PallerASTomWLLebwohlMGEfficacy and safety of crisaborole ointment, a novel, nonsteroidal phosphodiesterase 4 (PDE4) inhibitor for the topical treatment of atopic dermatitis (AD) in children and adultsJ Am Acad Dermatol2016753494503.e627417017
- SivaranjaniNRaoSVRajeevGRole of reactive oxygen species and antioxidants in atopic dermatitisJ Clin Diagn Res20137122683268524551611
- EichenfieldLFCallRSForshaDWLong-term safety of crisaborole ointment 2% in children and adults with mild to moderate atopic dermatitisJ Am Acad Dermatol2017774641649.e528823881
- Berth-JonesJDamstraRJGolschSTwice Weekly fluticasone propionate added to emollient maintenance treatment to reduce risk of relapse in atopic dermatitis: randomised, double blind, parallel group studyBMJ20033267403136712816824
- WollenbergABieberTProactive therapy of atopic dermatitis – an emerging conceptAllergy200964227627819076538
- DehesaLAbucharANuno-GonzalezAVitielloMKerdelFAThe use of cyclosporine in dermatologyJ Drugs Dermatol201211897998722859244
- SimpsonELBieberTGuttman-YasskyETwo phase 3 trials of Dupilumab versus placebo in atopic dermatitisN Engl J Med2016375242335234827690741
- BeckLAThaçiDHamiltonJDDupilumab treatment in adults with moderate-to-severe atopic dermatitisN Engl J Med2014371213013925006719
- BlauveltAde Bruin-WellerMGooderhamMLong-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (liberty AD CHRONOS): a 1-year, randomised, double-blinded, placebo-controlled, phase 3 trialLancet2017389100862287230328478972
- YuSHDruckerAMLebwohlMSilverbergJIA systematic review of the safety and efficacy of systemic corticosteroids in atopic dermatitisJ Am Acad Dermatol2018784733740.e71129032119
- DruckerAMEyerichKde Bruin-WellerMSUse of systemic corticosteroids for atopic dermatitis: international eczema Council consensus statementBritish J Dermatol20181783768775
- SidburyRDavisDMCohenDEGuidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic agentsJ Am Acad Dermatol201471232734924813298
- SaagKGKoehnkeRCaldwellJRLow dose long-term corticosteroid therapy in rheumatoid arthritis: An analysis of serious adverse eventsAm J Med19949621151238109596
- KirkupMEBirchallNMWeinbergEGHelmKKennedyCTAcute and maintenance treatment of atopic dermatitis in children - two comparative studies with fluticasone propionate (0.05%) creamJ Dermatol Treat2003143141148
- RoekevischESpulsPIKuesterDLimpensJSchmittJEfficacy and safety of systemic treatments for moderate-to-severe atopic dermatitis: a systematic reviewJ Allergy Clin Immunol2014133242943824269258
- PatriziARaoneBRavaioliGMManagement of atopic dermatitis: safety and efficacy of phototherapyClin Cosmet Invest Dermatol20158511520
- El SamahyMHAttiaEASaadAAMahmoudEYCirculating CD4(+) CD25(high) FoxP3(+) T-regulatory cells in patients with atopic dermatitis after narrowband-ultraviolet B phototherapyInt J Dermatol20155410e42442926219909
- DograSMahajanRPhototherapy for atopic dermatitisIndian J Dermatol Venereol20158111015
- GarritsenFMBrouwerMWLimpensJPhoto (chemo)therapy in the management of atopic dermatitis: an updated systematic review with implications for practice and researchBr J Dermatol2014170350151324116934
- GambichlerTOthlinghausNTomiNSMedium-dose ultraviolet (UV) A1 vs. narrowband UVB phototherapy in atopic eczema: a randomized crossover studyBr J Dermatol2009160365265819120333
- MajoieIMOldhoffJMvan WeeldenHNarrowband ultraviolet B and medium-dose ultraviolet A1 are equally effective in the treatment of moderate to severe atopic dermatitisJ Am Acad Dermatol2009601778419103360
- SchramMERoekevischELeeflangMMBosJDSchmittJSpulsPIA randomized trial of methotrexate versus azathioprine for severe atopic eczemaJ Allergy Clin Immunol2011128235335921514637
- El-KhalawanyMAHassanHShaabanDGhonaimNEassaBMethotrexate versus cyclosporine in the treatment of severe atopic dermatitis in children: a multicenter experience from EgyptEur J Pediatr2013172335135623229188
- Grundmann-KollmannMPoddaMOchsendorfFBoehnckeWHKaufmannRZollnerTMMycophenolate mofetil is effective in the treatment of atopic dermatitisArch Dermatol2001137787087311453805
- ThijsJLVan Der GeestBAMVan Der SchaftJPredicting therapy response to mycophenolic acid using UGT1A9 genotyping: towards personalized medicine in atopic dermatitisJ Dermatol Treat2017283242245
- HaeckIMKnolMJTen BergeOvan VelsenSGde Bruin-WellerMSBruijnzeel-KoomenCAEnteric-coated mycophenolate sodium versus cyclosporin A as long-term treatment in adult patients with severe atopic dermatitis: a randomized controlled trialJ Am Acad Dermatol20116461074108421458107
- HellerMShinHTOrlowSJSchafferJVMycophenolate mofetil for severe childhood atopic dermatitis: experience in 14 patientsBr J Dermatol2007157112713217489974
- WaxweilerWTAgansRMorrellDSSystemic treatment of pediatric atopic dermatitis with azathioprine and mycophenolate mofetilPediatr Dermatol201128668969421967657
- SlaterNAMorrellDSSystemic therapy of childhood atopic dermatitisClin Dermatol201533328929925889129
- Berth-JonesJTakwaleATanEAzathioprine in severe adult atopic dermatitis: a double-blind, placebo-controlled, crossover trialBr J Dermatol2002147232433012174106
- MeggittSJGrayJCReynoldsNJAzathioprine dosed by thiopurine methyltransferase activity for moderate-to-severe atopic eczema: a double-blind, randomised controlled trialLancet2006367951383984616530578
- BodoSSvrcekMSourrouilleIAzathioprine induction of tumors with microsatellite instability: risk evaluation using a mouse modelOncotarget2015628249692497726327213
- KotlyarDSOstermanMTDiamondRHA systematic review of factors that contribute to hepatosplenic T-cell lymphoma in patients with inflammatory bowel diseaseClin Gastroenterol Hepatol2011913641.e3120888436
- KotlyarDSLewisJDBeaugerieLRisk of lymphoma in patients with inflammatory bowel disease treated with azathioprine and 6-mercaptopurine: a meta-analysisClin Gastroenterol Hepatol2015135847858.e424879926
- WolvertonSEComprehensive dermatologic drug therapy2013 Available from: http://www.clinicalkey.com/dura/browse/bookChapter/3-s2.0-C20091567366Accessed November 4th, 2018
- HodgeJAKawabataTTKrishnaswamiSThe mechanism of action of tofacitinib - an oral Janus kinase inhibitor for the treatment of rheumatoid arthritisClin Exp Rheumatol201634231832826966791
- BissonnetteRPappKAPoulinYTopical tofacitinib for atopic dermatitis: a phase IIa randomized trialBrit J Dermatol2016175590291127423107
- AbbVieA study to evaluate ABT-494 in adult subjects with moderate to severe atopic dermatitis Available from: https://news.abbvie.com/news/abbvies-upadacitinib-abt-494-meets-primary-endpoint-in-phase-2b-study-in-atopic-dermatitis.htmAccessed November 30, 2018
- NygaardUVestergaardCDeleuranMEmerging treatment options in atopic dermatitis: systemic therapiesDermatology2017233534435729320765
- Study to evaluate PF-04965842 in subjects with moderate to severe atopic dermatitis Available from: https://clinicaltrials.gov/ct2/show/study/NCT02780167?sect=X4301256#studydesignAccessed November 3, 2018
- Guttman-YasskyESilverbergJINemotoOBaricitinib in adult patients with moderate-to-severe atopic dermatitis: a phase 2 parallel, double-blinded, randomized placebo-controlled multiple-dose studyJ Am Acad Dermatol Epub201821
- YamaokaKBenefit and risk of tofacitinib in the treatment of rheumatoid arthritis: a focus on herpes zosterDrug Safety201639982384027193610
- ParkAYSpergelJMPathophysiology of Nocturnal Scratching in Childhood Atopic Dermatitis: The Role of Brain-Derived Neurotrophic Factor and Substance PPediatrics2008122Supplement 4S197S197
- ToyodaMNakamuraMMakinoTHinoTKagouraMMorohashiMNerve growth factor and substance P are useful plasma markers of disease activity in atopic dermatitisBr J Dermatol20021471717912100187
- Vanda Pharmaceuticals Inc.Vanda Pharmaceuticals Announces Tradipitant Phase II Proof of Concept Study Results for Chronic Pruritus in Atopic DermatitisPR News Wire2015 Available from: https://www.prnewswire.com/news-releases/vanda-pharmaceuticals-announces-tra-dipitant-phase-ii-proof-of-concept-study-results-for-chronic-pruritus-in-atopic-dermatitis-300045700.htmlAccessed November 2nd, 2018
- SaleemMDOussedikED’AmberVFeldmanSRInterleukin-31 pathway and its role in atopic dermatitis: a systematic reviewJ Dermatolog Treat201728759159928145790
- RuzickaTHanifinJMFurueMAnti-interleukin-31 receptor a antibody for atopic dermatitisN Eng J Med20173769826835
- HamannCRThyssenJPMonoclonal antibodies against interleukin 13 and interleukin 31RA in development for atopic dermatitisJ Am Acad Dermatol2018783S1S37S4229248521
- SimpsonELFlohrCEichenfieldLFEfficacy and safety of lebrikizumab (an anti-IL-13 monoclonal antibody) in adults with moderate-to-severe atopic dermatitis inadequately controlled by topical corticosteroids: a randomized, placebo-controlled phase II trial (TREBLE)J Am Acad Dermatol2018785863871.e1129353026
- FabbrociniGNapolitanoMMegnaMBalatoNPatrunoCTreatment of atopic dermatitis with biologic drugsDermatol Ther2018
- WollenbergAHowellMDGuttman-YasskyETreatment of atopic dermatitis with tralokinumab, an anti-IL-13 mAbThe Journal of Allergy and Clinical Immunology2019143113514129906525
- Guttman-YasskyEBrunnerPMNeumannAUEfficacy and safety of fezakinumab (an IL-22 monoclonal antibody) in adults with moderate-to-severe atopic dermatitis inadequately controlled by conventional treatments: a randomized, double-blind, phase 2a trialJ Am Acad Dermatol2018785872881.e87629353025
- BrunnerPMPavelABKhattriSBaseline IL-22 expression in patients with atopic dermatitis stratifies tissue responses to fezakinumabJ Allergy Clin Immunol2019143114215430121291
- SanyalRDPavelABGlickmanJAtopic dermatitis in African American patients is TH2/TH22-skewed with TH1/TH17 attenuationAnn Allergy Asthma Immunol201912219911030223113
- CzarnowickiTEsakiHGonzalezJEarly pediatric atopic dermatitis shows only a cutaneous lymphocyte antigen (CLA)(+) TH2/TH1 cell imbalance, whereas adults acquire CLA(+) TH22/TC22 cell subsetsJ Allergy Clin immunol20151364941951.e94326242300
- PanYXuLQiaoJFangHA systematic review of ustekinumab in the treatment of atopic dermatitisJ Dermatol Treat2018296539541
- BrunnerPMIsraelAZhangNEarly-onset pediatric atopic dermatitis is characterized by TH2/TH17/TH22-centered inflammation and lipid alterationsJ Allergy Clin Immunol201814162094210629731129
- NodaSSuárez-FariñasMUngarBThe Asian atopic dermatitis phenotype combines features of atopic dermatitis and psoriasis with increased TH17 polarizationJ Allergy Clin Immunol201513651254126426428954