Abstract
Background:
The aim of the current study is to report on a new form of treatment for cellulite based on a novel physiological hypothesis.
Methods:
A novel treatment for cellulite was evaluated in 14 patients aged 19–36 (mean 27.5) years. The only inclusion criterion was clinically diagnosed cellulite, and the exclusion criteria were history of edema, obesity, or any other disease diagnosed during the physical examination. Perimetry was performed at the gluteal fold, at 5 cm and 10 cm below the gluteal fold for both legs, and 5 cm and 10 cm below the navel. Additionally, standard photographs were taken and a questionnaire of satisfaction was applied. The patients were submitted to a treatment regimen of 1.5 hours per day adapted for the treatment of cellulite, consisting of manual and mechanical lymph drainage and cervical stimulation using the Godoy and Godoy technique. After 10 sessions over two weeks, the patients were evaluated again.
Results:
Reductions were identified at both points below the navel, the points on the thighs, and at the gluteal fold (P < 0.0001).
Conclusion:
This technique of lymphatic system stimulation is efficacious in the treatment of cellulite.
Keywords:
Introduction
The presence of cellulite is an esthetically unacceptable cosmetic problem for most postadolescent women.Citation1 Cellulite, or so-called “orange peel” skin affects 80%–90% of all females. It is not considered as a pathological condition but as esthetically disturbing dimpling of the skin, seen most commonly on the thighs and buttocks.Citation2
Cellulite is an alteration of the topography of the skin that occurs in body areas where fat deposits seem to be under the influence of estrogen, mainly the hips, buttocks, thighs, and abdomen. There is currently no cure or consistently effective treatment for cellulite.Citation3 In fact, no treatment is completely successful, and none are more than mildly and temporarily effective.Citation4
This condition is not specific to overweight women, although increased adipogenicity will exacerbate the condition. It is a complex problem involving the microcirculatory system and lymphatics, the extracellular matrix, and the presence of excess subcutaneous fat that bulges into the dermis.Citation1
There are glaring discrepancies regarding the microanatomical descriptions of this condition in the literature,Citation5 and the pathophysiological aspects of cellulite are still not clear.Citation6 Only a limited number of studies on cellulite have been published in the international literature, and many of them reach somewhat antithetical conclusions. Consequently, it is not yet possible to reconcile the extreme differences of opinion which have lingered for years concerning the nature of this disorder, as well as its origin and even the most basic aspects of its histopathological classification.Citation7
There is no consensus in respect to the anatomical changes in cellulite and even less on a pathophysiological basis that can guide treatment. However, a series of proposals have been published.Citation8–Citation12
This suggests that cellulite is a consequence of alterations that develop in the lymphatic system and lead to an accumulation of substances in subcutaneous tissue, in particular in the cellular interstice. These alterations may be influenced by hormones or by any other mechanism that predisposes the individual to an accumulation of fluids and other substances in the cellular interstice. Thus stimulation, using appropriate techniques may be efficacious in the reduction of cellulite.Citation13
The objective of the current study is to report on a novel form of treatment for cellulite based on a new pathophysiological hypothesis.
Methods
A novel form of treatment for cellulite was evaluated in 14 patients aged 19–36 (mean 27.5) years. On acceptance, consecutive patients were enrolled in this study. The only inclusion criterion was clinically diagnosed cellulite, and the exclusion criteria were history of edema, obesity, or any other disease diagnosed during the physical examination. Perimetry was performed at the gluteal fold, at 5 cm and 10 cm below the gluteal fold for both legs, and 5 cm and 10 cm below the navel. Standard photographs were taken. The patients were submitted to a treatment regimen for 1.5 hours per day adapted for cellulite, consisting of manual and mechanical lymph drainage and cervical stimulation using the Godoy and Godoy technique. Thus, the treatment employed was an association of three techniques. Mechanical lymph drainage consists of the utilization of a device that causes passive plantar/dorsiflexion movements.Citation14 The cervical stimulation technique was performed for 20 minutes per day.Citation15,Citation16 Manual lymph drainage was performed using manual compression of 30–40 mmHg. This subjectively determined pressure, as with conventional lymph drainage, is exerted with a sliding motion over the course of lymphatic collectors up to the corresponding lymph node regions.Citation17,Citation18
After 10 sessions over two weeks, the patients again underwent physical examination, including perimetry. Standard photographs were taken, and an investigation was made of the satisfaction of patients with the treatment results. The photographs were evaluated by two examiners who identified the differences between photographs. The greatest variation in the thigh and abdomen regions was considered for each patient.
The paired t-test was used for statistical analysis, with an alpha level of 5% (P < 0.05) being considered significant. This study was approved by the research ethics committee of FAMERP.
Results
The mean circumferences at the points 5 cm and 10 cm below the navel were 98.9 cm and 95.6 cm before and after treatment, respectively. Thus, the mean reduction with treatment was 3.3 cm (paired t-test: P < 0.0001, ). There were no significant differences between the initial measurements of the right and left thighs (P = 0.6). On the other hand, differences were seen between the measurements before (54.4 cm) and after (51.2 cm) treatment of the right thigh, with a mean loss of 3.2 cm (P < 0.000, ). Moreover, a significant difference of 3.5 cm was seen between pretreatment (54.5 cm) and post-treatment (51.2 cm) of the left leg (P < 0.0001, ). The circumferences at the gluteal fold before and after treatment were 58.4 cm and 54.9 cm, respectively, with a mean reduction of 3.5 cm (P < 0.0001, ). All the patients reported that they liked the results, and in the analysis of the photographs, both examiners were in agreement that the cellulite improved for 13 of the 14 patients ( and ).
Figure 1A and 1B. Pretreatment and post-treatment of the gluteal fold and thighs.
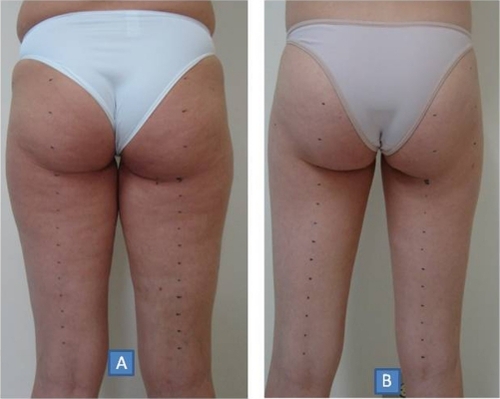
Figure 2A and 2B. Pretreatment and post-treatment 5 cm and 10 cm below the navel.

Table 1 Pre- and post-treatment measurements 5 and 10 cm below the navel
Table 2 Pretreatment and post-treatment measurements of the right thigh 5 cm and 10 cm below the gluteal fold
Table 3 Pretreatment and post-treatment measurements of the left thigh 5 cm and 10 cm below the gluteal fold
Table 4 Pretreatment and post-treatment measurements at the gluteal fold
Discussion
The current study demonstrates reductions in body measurements of regions in which the presence of clinical cellulite was detected. The satisfaction of the patient in respect to treatment, regional volumetric reductions, and improvement in the clinical evaluation, all substantiate the efficacy of this new option of treatment for cellulite.
This novel approach was developed from clinical observations that cellulite normalized with lymphedema treatment that utilizes specific techniques of manual and mechanical lymph drainage. From these findings, studies of the pathophysiological basis of the condition were made in an attempt to explain the results.Citation13 However, there is no consensus in the literature about the pathophysiology of cellulite.Citation19–Citation21 Subsequently, published histological data were analyzed which also did not demonstrate a consensus. However, modifications of the interstice matrix suggest that a physiological hypothesis should explain these changes in the lymphatic system.Citation20,Citation21
Only lean women with cellulite were enrolled in this study to eliminate any interference of obesity. Another precaution was to exclude patients with idiopathic cyclic edema and other forms of clinically evident edema. Thus, two important causes of accumulation of fluids and other substances in the subcutaneous tissue were excluded.
The three conditions, ie, edema, cellulite, and obesity, can occur simultaneously. However, the treatment should be specific for each condition; if not, the objective of treatment will not be reached. This association of conditions leads to increases in alterations of subcutaneous tissue, and so has a synergic effect, both to aggravate the symptoms and improve the treatment. This we denominated the cellulitic complex to facilitate the diagnosis and guide the therapeutic conduct.
The basis of treatment in this study was to stimulate both the deep and superficial lymphatic system. This approach included cervical stimulation which, the authors believe, stimulates contraction and motility of lymphatic vessels.Citation15,Citation16 This drainage technique was developed by the authors, and is based on physiology, anatomy, pathophysiology, and hydrodynamic concepts consistent with reproducible scientific principles both in vitro and in vivo. Hence, all the movements utilized in this lymph drainage technique follow scientific principles based on hemodynamic concepts for fluid drainage in collectors. An in vivo study can be reproduced using dyes while draining the lymphatic collectors of animals or by using lymphoscintigraphy.
Reduction in cellulite can be total, and no further reduction in the circumferences occurs. Moreover, reductions were only observed in the regions where cellulite was detected; the worse the cellulite, the better the results. It is possible to reduce the perimeter at the point of greatest diameter in 10 sessions without the patient losing weight. Thus, these results show that cellulite (regional cutaneous lymphostasis) has its own physiopathology which is totally different from that for obesity and edema.
We have been studying this technique for 10 years, and have seen that results can be maintained for years, as long as the patient does not put on weight or present with edema, so the results are long-lasting. This technique is a novel approach to the treatment of cellulite, involving stimulation of the physiological processes of the body, and so it is the body itself that re-establishes its equilibrium. In conclusion, this lymphatic system simulation technique is efficacious in the treatment of cellulite.
Disclosure
The authors report no conflicts of interest in this work.
References
- RawlingsAVCellulite and its treatmentInt J Cosmet Sci20062817519018489274
- PavicicTBorelliCKortingHCCellulite – the greatest skin problem in healthy people? An approachJ Dtsch Dermatol Ges20064861870 German.17010177
- GoldmanAGotkinRHSarnoffDSPratiCRossatoFCellulite: A new treatment approach combining subdermal Nd:YAG laser lipolysis and autologous fat transplantationAesthet Surg J20082865666219083594
- WannerMAvramMAn evidence-based assessment of treatments for celluliteJ Drugs Dermatol2008734134518459514
- QuatresoozPXhauflaire-UhodaEPiérard-FranchimontCPiérardGECellulite histopathology and related mechanobiologyInt J Cosmet Sci20062820721018489276
- RonaCCarreraMBerardescaETesting anticellulite productsInt J Cosmet Sci20062816917318489273
- TerranovaFBerardescaEMaibachHCellulite: Nature and aetio-pathogenesisInt J Cosmet Sci20062815716718489272
- Van der LugtCRomeroCAnconaDAl-ZarouniMPereraJTrellesMAA multicenter study of cellulite treatment with a variable emission radio frequency systemDermatol Ther200922748419222519
- LachEReduction of subcutaneous fat and improvement in cellulite appearance by dual-wavelength, low-level laser energy combined with vacuum and massageJ Cosmet Laser Ther20081020220919093288
- SasakiGHComparison of results of wire subcision performed alone, with fills, and/or with adjacent surgical proceduresAesthet Surg J20082861962619083589
- ChristCBrenkeRSattlerGSiemsWNovakPDaserAImprovement in skin elasticity in the treatment of cellulite and connective tissue weakness by means of extracorporeal pulse activation therapyAesthet Surg J20082853854419083577
- Pires-de-CamposMSLeonardiGRChorilliMSpadari-BratfischRCPolacowMLGrassi-KassisseDMThe effect of topical caffeine on the morphology of swine hypodermis as measured by ultrasoundJ Cosmet Dermatol2008723223718789063
- De GodoyJMde GodoyM de FPhysiopathological hypothesis of celluliteOpen Cardiovasc Med J20093969719756187
- GodoyJMPGodoyMFGDevelopment and evaluation of a new apparatus for lymph drainage: Preliminary resultsLymphology200437626415328758
- GodoyJMPGodoyMFGGodoy and Godoy technique of cervical stimulation in the reduction of edema of the face after cancer treatmentQJM200810132532618287110
- de GodoyJM PereiraSilvaSHToninatoMCGodoyM de FCervical stimulation for volumetric reduction of limbs in the treatment of lymphedemaIndian J Med Sci20086242342519008619
- GodoyJMFGodoyMFGBatigaliaFPreliminary evaluation of a new, more simplified physiotherapy technique for lymphatic drainageLymphology200235919312081057
- GodoyJMPGodoyMFGManual lymph drainage: A new conceptJ Vasc Br200437780
- AlquierLCe qu’est la cellulite. Comment la traiterMonde Med19495934415400736
- SegersAMAbulafiaJKrinerJCortodonoOCellulitis. Histopathologic and histochemical study of 100 cases. [Article in Spanish]Méd Cutan Ibero Lat Am198412167172
- FernandézGCurriSBVenous stasis and panniculopathy: a semiologic studyAngiologia [Article in Spanish]1990421271322248419