Abstract
Background:
An interactive software program (HOYS) has been developed utilizing a database of digital images depicting various aspects and degrees of aging of exposed skin across seven geographic regions, representing a total of 35 facial and extrafacial subregions. A five-point photonumeric rating scale, which portrays age-related skin changes across five decades for each of these subregions, underpins this patient-based interactive self-assessment program. Based on the resulting outputs from this program, an individualized treatment prioritization list is generated for each region where significant differences between the patient’s chronological and esthetic ages exist. This provides guidance for the patient and the treating physician on treatment options.
Methods:
To evaluate the utility of HOYS in the clinic, relative to education programs currently used in Australian private esthetic clinics, a total of 95 esthetically-orientated patients were enrolled in a prospective, randomized, controlled, multicenter study.
Results:
Compared with a prospective cohort of patients completing a standard education program commonly utilized in Australian esthetic clinics, patients receiving the HOYS education program reported greater empowerment through improved knowledge of specific age-related skin changes. This was associated with a clearer understanding of treatment options available to them, and a perceived ability to participate in the selection of the treatments potentially administered to improve their appearance. These differences between the two education groups were highly significant.
Conclusion:
Patients completing the HOYS patient education program have an improved understanding of age-related changes to exposed skin of their face, neck, décolletage, and hands. Due to the patient-specific nature of the program, these patients perceive a greater role in the deciding which esthetic treatments should be subsequently administered to enhance their appearance, through an improved understanding of the rationale for these treatments and indeed how they should be prioritized to achieve the best outcome for them.
Introduction
A new patient education software program (“Home Of Younger Skin”, HOYS) has been developed by an Australian dermatologist. The program has been designed to provide a structured analysis of the exposed areas of the face, neck, décolletage, and hands via a photographic grading scale, reflecting age-related skin changes through the decades. Seven geographic regions are considered in this program, specifically; the upper face (divided into two regions, ie, forehead/temple and periorbital), mid-face, lower face/perioral, neck, décolletage, and hands. These regions are further divided into a total of 35 “subregions”. Each subregion is represented by a five-point photonumeric scale, utilizing representative images from a typical patient at the ages of 25, 35, 45, 55, or 65 years, to reflect five grades of aging or “severity”. The initial program was designed for Caucasian females.
While viewing themselves in a mirror, patients participating in the HOYS program are asked to select the image that most appropriately depicted their current appearance for each subregion in question, with the associated score entered. This process is repeated until all 35 subregions were scored by the patient. The HOYS program software subsequently calculated the patient’s skin age based on these scores, utilizing a proprietary algorithm. There was also a calculated skin age for each of the seven regions described above. Utilizing this information, a treatment prioritization list was generated, based on the degree of divergence between the patient’s chronological age and esthetic age, if any, for the seven geographical regions. This formed the basis of a clinic treatment plan, focused on skin rejuvenation by region.
The HOYS program is a departure from what is the current practice for education of patients on age-related skin changes in most plastic surgery, medical esthetics, and dermatology clinics throughout Australia and probably in many other parts of the world. Currently, the esthetic consultation process may vary according to the specialty of the physician involved, the particular interests and experience of the practitioner, as well as the expertise and service provided in each clinic. Due to a number of factors, including the lack of universally accepted methods for evaluating skin surface and structural changes associated with aging, as well as the potential for treatment biases, there may be significant variability in what patients are told about their appearance, what treatments may be offered, and indeed what treatment is administered from one clinic to the next.
A formalized and reproducible consultation procedure, which empowers patients to make informed treatment decisions based on an education intervention which is individualized to them, would address the above scenario. Ultimately, the motivation to adopt such a program in a clinic would be based on clear evidence of an efficient and targeted esthetic treatment strategy, leading to an overall improvement in patient satisfaction and an enduring relationship between clinic and patient. It is believed that the HOYS education program might offer such an approach, although the patient’s perception of such a program would need to be formally evaluated in the clinic, which is the primary objective of this study.
Methods
In this prospective, randomized, controlled, multicenter study, eligible patients were randomized (1:1) to either the HOYS education program (HOYS group) or a standard patient education program (standard group) at one of six private suburban clinics in Australia. A computer-generated randomization code was used, based on the method of randomly permuted blocks.
Eligible patients were females aged 25–54 years, who provided written informed consent before any study-related procedure. All were required to be existing clients at the investigational site during the preceding 12 months, receiving at least one esthetic treatment during this period. Subjects treated with a dermal filler, botulinum toxin, and/or plastic surgery to their face during the preceding 3 months were excluded, as were subjects who had any condition which might affect their ability to complete the HOYS-based evaluation adequately, such as connective tissue disease, scarring, or inflammation at one or more of the seven regions of interest. Study patients had to agree that the enrolling clinic would be their principal provider of esthetic treatments for the duration of the study and that they intended to receive one or more such treatments while on study. Individuals who were pregnant or lactating, or who planned to become pregnant, during the study were also excluded, as were those with a history of adverse events or hypersensitivity to medical esthetic treatments, including dermal fillers, botulinum toxin, intense pulsed light, or laser therapy.
Prior to initiation of their randomized education program, all patients had their baseline characteristics documented, including their age, ethnicity, esthetic medical history, Fitzpatrick skin phototype and Glogau photoaging classification scores. Each patient also completed a series of Likert scales on their perception of their facial appearance.
Patients randomized to the HOYS group completed their education program on a designated computer. They were guided through each step by the study coordinator, who was instructed not to provide the patient with any advice that would aid in image selection. As each subregion was presented, the patients were asked to select one of the five images which best matched their appearance while looking in a mirror, as described above. and are examples of five-point photonumeric scales of two subregions (naso-labial folds and upper lip atrophy, respectively) from the HOYS education program. The HOYS consultation continued until all 35 subregions, representing the seven regions of the program, were scored by the patient. The entire procedure took approximately 30–40 minutes for each patient.
Figure 1 Five-point photonumeric scale used for nasolabial folds.

Figure 2 Five-point photonumeric scale used for upper lip atrophy.

At the conclusion of the program, each patient was informed of their total skin age score, as well as the skin age score for the seven regions across the face, hands, chest, and neck. They were also shown a treatment prioritization list, related to the differences between their chronological and esthetic ages for each subregion, with the subregion having the largest difference listed first. They were also shown a list of treatment options for these subregions derived from an existing database in the program. This information was printed out for the patient for subsequent discussion with their treating physician.
For the standard education group, each patient was given a five-page information sheet on age-related skin changes, based on materials commonly given to patients at esthetic, plastic surgery, or dermatology clinics throughout Australia (see the attached Appendix). This information sheet provided details of skin changes expected to occur with age, based on the same seven skin regions defined in the HOYS program. The patients were given as much time as they required reviewing this information sheet.
Immediately after completion of the assigned education program, each patient was asked to complete a program evaluation questionnaire. This questionnaire was based on a five-point Likert scale, with an additional “yes/no” question on whether the patient would recommend the assigned education program to a friend. The questionnaire was identical for both groups, except that patients in the HOYS group were asked to answer two additional questions on the relevance of skin age scores. A series of questions related to their knowledge of age-related skin changes of their face before their assigned education program and whether this improved both generally and at specific areas of their face after the program. There were also questions on the impact of the program in terms of their sense of empowerment in defining treatment plans/priorities with their treating physician. Finally, there were questions about whether the program was interactive, engaging, and easy to follow. At the completion of the questionnaire, all patients (in both groups) met with the treating physician to discuss their treatment options.
The primary endpoint for this study was patient satisfaction with their assigned education program, based on results of the patient program evaluation questionnaires, with the Fisher’s Exact test used to identify statistical differences between the two groups for each of the questions in this questionnaire. The secondary endpoint was the responses of the HOYS group to the skin age score questions, with the one-way Chi-square test used to analyze this outcome. P values < 0.05 were considered statistically significant.
The study was approved by a central institutional review board and conducted at the six investigational sites in accordance with the applicable Good Clinical Practice regulations and guidelines. All patients were required to provide written informed consent prior to study-related procedures. This study is listed on the Australian New Zealand Clinical Trial Registry (ACTRN12611000476932).
Results
A total of 95 patients were enrolled, 51 of whom were randomized to the HOYS group and 44 to the standard group. The slight imbalance between the two groups related to the exclusion from the analysis of an initial series of patients randomized to the standard group at one investigational site where protocol-defined procedures were not conducted.
At baseline, there were no significant differences between the groups in terms of age, ethnicity, esthetic treatment history, or Fitzpatrick or Glogau scores (). There were also no significant differences in how the cohorts perceived their facial appearance (). Further, the patient’s assumed knowledge of age-related skin changes before administration of the two education programs was not significantly different between the two groups (Q.1, ).
Table 1 Patient demographics and other characteristics at screening
Table 2 Patient’s facial appearance evaluation (prior to assigned education program)
Table 3 Education program evaluation questionnaire
Based on the analysis of the results from the questionnaire following the administration of the allocated program, the HOYS program was highly regarded, as documented by a statistically greater proportion of patients in the HOYS group classifying it positively or very positively, relative to the standard group (–, ). This was particularly relevant for issues of prioritization, treatment selection, and empowerment (–). Consistent with this, patient’s apparent knowledge of their facial/skin aging features after their assigned education program, compared with before, was substantially improved following the education in the HOYS group (84% vs 50%; P = 0.0006, see ). The HOYS group also highly valued the total overall skin age score and regional skin age scores which were generated by the HOYS program (). Furthermore, 91% of patients in the HOYS group vs 61% in the standard group were satisfied or very satisfied with their education program (P = 0.0001, see ), while 92% of patients in the HOYS group vs 57% in the standard group documented that they would recommend the program to a friend (P < 0.0001, see ).
Figures 3 Patient education evaluation questionnaire. Do you feel that the consultation helped you to prioritize the facial areas you would like to improve?
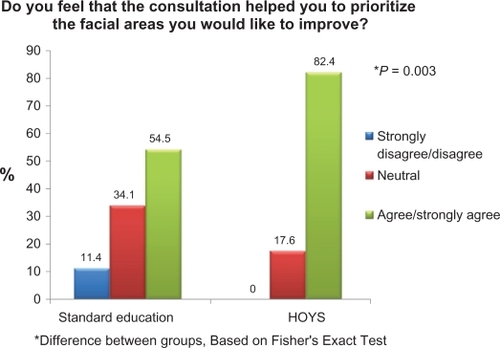
Figure 4 Patient education evaluation questionnaire. Do you feel that the program helped you to better define your treatment options/plans with your clinician?
Note: *Difference between groups, based on Fisher’s Exact Test.
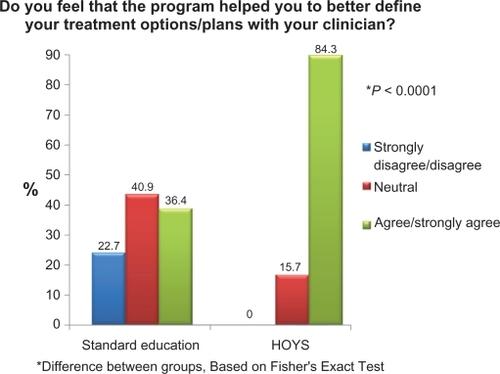
Figure 5 Patient education evaluation questionnaire. Do you feel empowered or more confident in making decisions regarding treatment options?
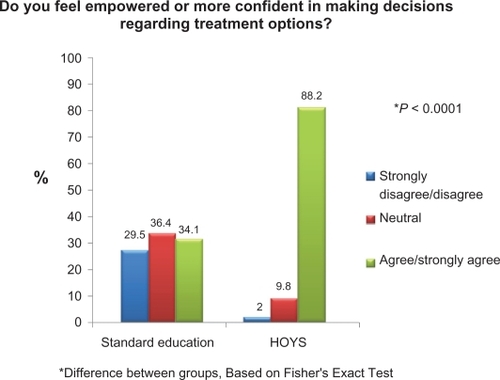
Figure 6 Patient education evaluation questionnaire. Change in the patient’s perceived knowledge of facial/skin aging after completing allocated education program vs before the program.
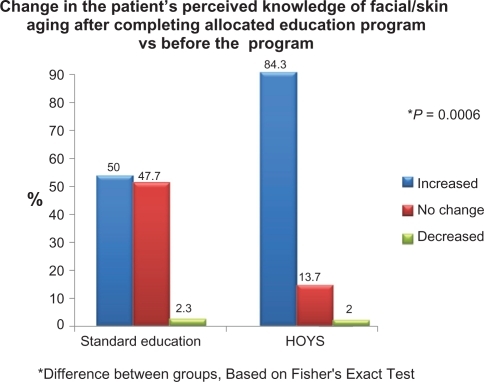
Figure 7 Patient education evaluation questionnaire. Overall, how do rate your level of satisfaction with the education program?
Note: *Difference between groups, based on Fisher’s Exact Test.
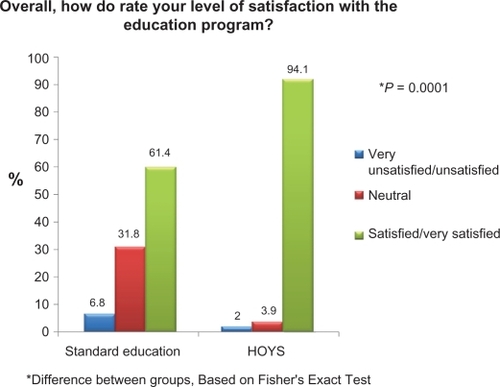
Figure 8 Patient education evaluation questionnaire. Would you recommend this facial consultation to a friend?
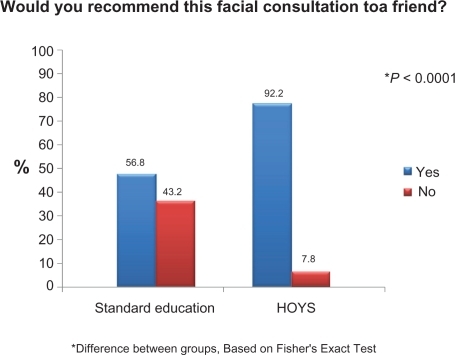
Table 4 Supplementary questions for HOYS group only
Discussion
Loss of bone and soft tissue volume, redistribution of fat, and decreased dermal elasticity and thickness contribute to the formation of wrinkles and folds, which characterize signs of the aging process in the skin.Citation1,Citation2 These changes may be accentuated by diet, movement, environmental stress (such as photodamageCitation3), self-care (ie, maintaining or enhancing their appearance), and/or the genotype of the individual.Citation4 Age-related changes are clearly not consistent for women of similar age, nor are they symmetrical on the facial or extrafacial regions of an individual woman. Many women have distinct areas (subregions) of the face, chest, neck, or hands which may make them look older than they are chronologically. Conversely, they may have other subregions which are perceived to be more consistent with their actual age. This situation may be compounded by the absence of universally applied methodologies for the total evaluation of skin surface and structural changes associated with aging.
The HOYS education program allows for a personalized, effective, and efficient methodology for assessing seven important facial or extrafacial regions which are commonly visible and exposed. Differences from one region to another can be quickly identified, with a score recorded, quantifying any divergence between esthetic and chronological age. Using HOYS, the patient drives the consultation rather than a physician or practice consultant. As a result, the patient is likely to feel that the information gained is less biased, and this self-generated knowledge of her own age-related changes leads to a sense of empowerment. Further, because the HOYS program lists treatment options offered by that clinic, which are predicated on the self-assessment during the preceding consultation, the patients are likely to see the specific logic behind this treatment listing, so that they can contribute actively to a discussion with their practitioners on which treatments are ultimately administered.
From analysis of the responses from the study questionnaire, the HOYS education program was positively identified by the majority of patients randomized to this program. These patients scored their assigned education program consistently higher than did the standard group. This was most evident for scales relating to sense of empowerment, knowledge of the age-related skin changes, as well as their perceived degree of participation in the selection of the administered treatments.
As many patients currently engage in a consultation with a preconceived notion of their esthetic “issue” or “issues” and even what treatments they want administered with only a minimal understanding of age-related skin changes, the HOYS program gives patients an opportunity to learn more about their appearance, as well as about these specific changes in exposed facial and exfacial regions over their lifetime. For patients with a limited budget or those uncertain about what aspect of their appearance might be an “esthetic priority” to address, the HOYS program provides a structured, nonthreatening, patient-directed approach, which is quantitative. For the practitioner, HOYS offers the chance to educate patients more comprehensively and allows a foundation for further discussion on treatment prioritization and planning. This may result in logic-based decision by the patient, because their treatment decisions are no longer based on a particular bias that a patient or physician may have. The end result of this might be better treatment outcomes for patients, as evidenced by improved patient satisfaction and greater fiscal investment in enhancing their appearance.
In summary, the results from this study demonstrate that, relative to a prospective control group who received a standard education program commonly utilized at private clinics in Australia, patients receiving the HOYS education program perceive themselves to have greater empowerment through a significant improvement in their understanding of the age-related skin changes by specific facial/extrafacial region. This translates into a clearer understanding of treatment prioritization and the subsequent regimens which may be employed to improve their appearance.
Acknowledgements
Data management and statistical analysis for this study was conducted independently by Datapharm Australia Pty Ltd, Five Dock, Australia. On-site study management was performed independently by Hanya Oversby, Specialist Consulting, Hawthorn, Australia.
Disclosure
JR and MH are employees of Allergan Australia, which sponsored the study. GG developed the HOYS program, however, did not enroll patients into the study and had no involvement in the data analysis. The other authors report no conflicts of interest in this work.
References
- DonofrioLMFat distribution: a morphologic study of the ageing faceDermatol Surg2000261107111211134986
- MonheitGDColemanKMHyaluronic acid fillersDermatol Ther20061914115016784513
- WidgerowADGrekinSKEffecting skin renewal: a multifaceted approachJ Cosmet Dermatol20111012613021649818
- DavisECCallenderVDAesthetic dermatology for aging ethnic skinDermatol Surg20113790190721585594
Appendix
Standard patient education intervention
Introduction
This information sheet is on the normal aging processes occurring in our skin and supporting tissues. It will possibly aid you in understanding how your own skin is aging and potentially assist you in making decisions about future esthetic therapies, if you require these treatments.
The information in this sheet is similar to that given to patients by many Australian clinics providing esthetic advice and treatment and is focused on the face, neck, chest and hands.

The forehead

In our 20s, the forehead and frown area has a smooth, unlined appearance. In our mid-30s we see the beginning of expression lines formed by repeated muscle movements. The intensity of these lines increases through our 40s and 50s, until frown and horizontal lines become etched into our skin and are present with or without these muscle movements, giving one an angry appearance. The structural support (bone, muscle, collagen and fat) for the skin in our forehead, which is present in out 20s, is lost over time.
Surface changes include widespread sun damage, observed as sun spots and pigmentation changes and a variety of lumps and bumps which are often due to blocked oil glands.
The eye region

In our mid-30s, We start to see expression lines around our eyes formed by repeated muscle movements. The intensity of these lines increases through our 40s and 50s, until they are present at rest.
Some of the most noticeable changes in this area due to the surface quality of the skin where very fine to medium wrinkling and even more subtle textural changes can create an aged appearance.
Crow’s feet may occur due to the dual effects of sun damage and the localised muscle movement associated with smiling, squinting frowning or grimacing. At first they are only noticeable with this movement, however by our 40s they tend to become visible at rest.
Our temples may also become sunken as we age and there is less support for the eyebrows and of the upper eyelids and they may tend droop as a result.
Loss of volume over time in the area below our eyes or the eye hollows can also lead to the formation of dark circles or bags (‘tear troughs’), giving one a very tired appearance.
The cheek and nose region
The volume loss caused by diminishing structural tissue (fat, muscles, collagen and/or bone) as we age allows the cheeks to drop and lose definition. This may lead to the formation of jowls (skin folds) at the jaw line and increases the heaviness of the fold that travels from the corner of the nose to the corner of the mouth (the nasolabial fold).
Sun exposure can amplify this loss of volume and is often responsible for the secondary smile lines and mid-facial wrinkling.
Fine and medium wrinkling is also common, as are sun and age spots. Hormonal pigmentation is often at its most obvious in this area, especially high on the cheekbones and this might be intensified by sun exposure. Scarring, predominantly from acne, is also common on the cheeks and temples. These age-related changes in the cheek area are often observed in our 50s. An increased prominence of blood vessels are also common in this area due to sun damage and this may lead to redness and bumps on the skin (rosacea).
Wrinkles radiating from our nose (‘bunny lines’) may also develop due to squinting, frowning or smiling over many years, which with sun exposure, can become permanent. Also, as we age, our nose seems to drop downwards.
The lower face region

The main focal point in this region is, of course, the lips.
The youthful fullness of the lips and the surrounding tissue decreases with age due to the loss of the supporting structure (volume). The lips also appear to lengthen. This loss of volume is also a major cause of the vertical wrinkling of and around the lips. Although this wrinkling is primarily inherited, it is also exacerbated by sun damage and smoking, as well as muscle movement related to talking, eating and drinking. This wrinkling may also lead to lip bleeding lipstick application.
The area in front of the developing jowl deepens with our increasing years and begins to merge with the evolving groove at the angle of the mouth, potentially causing mouth frowns (‘accordion lines’) and/or marionette lines. The chin may also loose definition and appear to project further due to loss of structural tissue with age.
The neck region

In our 20s, the neck is very well defined, free of horizontal and vertical neck wrinkling (banding). The jawline angle at the chin is also tight due to predominant structural muscles. In our 30s, some of this definition is lost. The vertical and horizontal bands also become visible. In our 40s, these events progress with the neck, often showing advanced signs of aging when compared with the face. Surface pigmentation and redness are often an issue and can be exacerbated by perfume use and sun exposure, which may be observed in our 50s and 60s. Our neck can also take on a goose-like flesh appearance.
The décolletage (chest region)
The décolletage, or chest area, is affected by the environment, particularly the sun, which can be exacerbated by the use of perfume or perfumed creams.
These elements can cause redness and enlarged blood vessels, blotchy brown pigmentation, age and sun spots and a leathery appearance. This leads to a multitude of vertical wrinkles in the centre of the chest and between the breasts. These changes are usually first observed in our 30s, depending on individual sun habits, becoming more prominent in our 40s, with the appearance of this vertical wrinkling, the pigmentation changes and leather-like look in our 50s. Eventually, all these changes may result in skin folding in our chest region in our 60s.
The hands
Our hands, or more specifically the back of our hands, age as the consequence of genetic and environmental factors. Loss of support structure (volume) under the skin commences in our 30s, with the appearance of veins. By our 40s, tendons are often observed and, in our 50s and 60s, these changes become more pronounced with an associated loss of elasticity. The skin becomes very thin and brittle in our 60s with bruising occurring from minimal or no trauma. All these events can be exacerbated by the sun, which also contributes to extreme dryness, blotchy colouring and a myriad of spots observed on our hands, especially in our later years.