
Abstract
Dissecting cellulitis (DC) of the scalp or perifolliculitis capitis abscedens et suffodiens is a rare chronic inflammatory condition of the scalp manifested by perifollicular pustules, nodules, abscesses and sinuses that result into scarring alopecia. Treatment of DC is challenging and often disappointing. We report a 38-year-old male patient with DC for 5 years, and multiple topical and systemic therapies had shown poor effect. This patient achieved excellent response to adalimumab with hair regrowth.
Introduction
Dissecting cellulitis (DC) of the scalp, also known as perifolliculitis capitis abscedens et suffodiens, is a rare chronic inflammatory condition that results in scarring alopecia. It commonly affects young African-American men. It presents as firm or fluctuant tender nodules usually over the posterior vertex and upper occiput, with possible formation of interconnecting draining sinuses and abscesses.Citation1 Spontaneous drainage of purulent foul-smelling discharge is commonly seen as well.Citation2 Finally, scarring alopecia of the overlying skin and keloids develop.
The pathogenesis of this disorder is linked to the occlusion of the pilosebaceous unit and follicular hyperkeratosis with subsequent follicular dilatation and rupture that result in neutrophilic and granulomatous inflammatory response. Additionally, bacterial infections have been implicated in the pathogenesis of DC, with Staphylococcus epidermidis, Propionibacterium acnes, Staphylococcus aureus being the most commonly isolated.Citation1
Treatment of DC is challenging and often disappointing. There are multiple treatment options for DC with varying response and efficacy. The commonly used agents are systemic antibiotics, oral isotretinoin, dapsone, zinc sulphate, and intralesional triamcinolone acetate. Photodynamic therapy and surgical excision have been used in resistant cases.Citation3,Citation4 Recently, few reports have been published about the use of tumor necrosis factor (TNF-α) inhibitors in DC with promising results.Citation5 Herein, we report a case of recalcitrant dissecting cellulitis of the scalp successfully treated with adalimumab.
Case Report
A 38-year-old male patient presented with 5-year history of inflammatory, boggy, fluctuant nodules over the upper occiput with recurrent foul-smelling discharge (). A scalp punch biopsy showed epidermal hyperkeratosis, marked neutrophilic infiltrate of the hair follicles and deep dermis, and focal areas with multinucleated giant cells and histocytes (foreign body giant cell reaction) (). A diagnosis of DC was made based on the findings of the clinical and histopathological examinations. The patient was initially treated with several topical and systemic antibiotics (clindamycin, doxycycline, and amoxicillin/clavulanic acid) with no improvement. After that, he was started on isotretinoin for 17 months, with dose escalation to 1 mg/kg (80 mg/day). His disease activity was partially controlled with isotretinoin, but it was discontinued because he could not tolerate the side effect of severe dryness. After stopping isotretinoin, his disease relapsed again. The patient had purified protein derivative skin test, hepatitis serology, chemistry and chest X-ray, which all were within normal. After that, adalimumab was started 80 mg on day 0, then 40 mg on day 7, and 40 mg weekly thereafter. Excellent response was noted after 1 month of therapy. The patient reported less pain and no more discharge. At 2 months follow-up, decreased swelling and areas of hair regrowth were noted which is unusual in the primary cicatricial alopecias (). The patient continues to receive 40 mg adalimumab weekly.
Figure 1 The patient with fluctuant, tender nodules with overlying alopecia. (A and B) Posterior and lateral views to show enlarged nodules in the scalp.

Figure 2 The scalp biopsy showing marked neutrophilic infiltrate of the hair follicles and deep dermis at low (A) and high (B) maginification.
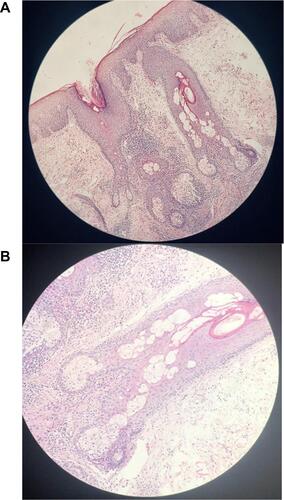
Figure 3 (A) Before treatment. (B) After 2 months of therapy showing partial hair regrowth.

Discussion
Dissecting cellulitis is neutrophilic scarring alopecia with chronic and relapsing course. Treatment of DC is often challenging. Oral antibiotics are typically used as initial management and have variable outcomes. The commonly used antibiotics are doxycycline, azithromycin, ciprofloxacin and the combination of rifampin with clindamycin. Their efficacy is hypothesized to be secondary to their anti-inflammatory properties.Citation3 Isotretinoin is a frequently used option. In one systematic review of refractory DC, isotretinoin was prescribed for 53% of the cases with significant response seen in 54% of the case. However, relapse was common with relapse rate of 19%.Citation4 The usual dose of isotretinoin is 0.5–1mg/kg, and the response is typically seen within 3 months; however, the duration of therapy is still controversial. Several antibiotics were used for our patient but with no significant improvement. However, he had good response with isotretinoin, although he relapsed after discontinuation.
Adalimumab is TNF-α inhibitor that has been increasingly used in various dermatological conditions, like psoriasis, and more recently in hidradenitis suppurativa (HS) and pyoderma gangrenosum with promising results.Citation6 HS shares similar pathogenesis to DC, therefore providing a justification to use adalimumab in DC. Few cases of DC treated with TNF- α inhibitors have been reported with good outcome in majority of the cases.Citation5,Citation7 Sukhatme et al reported a case of DC which had excellent response to adalimumab with hair regrowth.Citation8 Likewise, our patient had hair regrowth after 2 months of therapy. The hair regrowth is unusual result to be seen after treatment of this type of primary scarring alopecia. Given these promising results of adalimumab in DC, larger controlled studies are needed to support these observations.
Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. Patient gave written informed consent for publication of clinical information and photographs. Institutional approval is not required for this case study.
Disclosure
The authors report no conflicts of interest in this work.
References
- Badaoui A, Reygagne P, Cavelier-Balloy B, et al. Dissecting cellulitis of the scalp: a retrospective study of 51 patients and review of literature. Br J Dermatol. 2016;174(2):421–423. doi:10.1111/bjd.13999
- Whiting DA. Cicatricial alopecia: clinico-pathological findings and treatment. Clin Dermatol. 2001;19(2):211–225. doi:10.1016/S0738-081X(00)00132-2
- Scheinfeld N. Dissecting cellulitis (Perifolliculitis Capitis Abscedens et Suffodiens): a comprehensive review focusing on new treatments and findings of the last decade with commentary comparing the therapies and causes of dissecting cellulitis to hidradenitis suppurativa. Dermatol Online J. 2014;20(5):22692.
- Thomas J, Aguh C. Approach to treatment of refractory dissecting cellulitis of the scalp: a systematic review. J Dermatolog Treat. 2019;1–6.
- Takahashi T, Yamasaki K, Terui H, et al. Perifolliculitis capitis abscedens et suffodiens treatment with tumor necrosis factor inhibitors: a case report and review of published cases. J Dermatol. 2019;46(9):802–807. doi:10.1111/1346-8138.14998
- Traczewski P, Rudnicka L. Adalimumab in dermatology. Br J Clin Pharmacol. 2008;66(5):618–625. doi:10.1111/j.1365-2125.2008.03263.x
- Brandt HR, Malheiros AP, Teixeira MG, et al. Perifolliculitis capitis abscedens et suffodiens successfully controlled with infliximab. Br J Dermatol. 2008;159(2):506–507. doi:10.1111/j.1365-2133.2008.08674.x
- Sukhatme SV, Lenzy YM, Gottlieb AB. Refractory dissecting cellulitis of the scalp treated with adalimumab. J Drugs Dermatol. 2008;7(10):981–983.