
Abstract
Purpose
Different immunohistochemical stains are used in dermatopathology to stain melanocytes and diagnose benign and malignant melanocytic lesions.
Methods
SOX-10, HMB-45, and Melan-A immunohistochemical stains were used to assess 32 biopsy specimens with a histologic diagnosis of lentigo. The total number of melanocytes stained with each immunohistochemical stain was counted and an average count was obtained from two readings.
Results
Analysis of the data revealed a significant difference in staining melanocytes between these three immunostains (p=0.0010, ANOVA). SOX-10 stained 0.195 more melanocytes than HMB-45 (p=0.0026). Similarly, Melan-A stained 0.195 more melanocytes than HMB-45 (p=0.0011). However, the difference between SOX-10 and Melan-A was not statistically significant (p=0.9810).
Conclusion
SOX-10 and Melan-A immunostaining stain more melanocytes than HMB-45. No significant difference was noted between Melan-A and SOX-10.
Introduction
Early melanoma in situ can be difficult to distinguish from lentigo senilis, particularly in sun-damaged skin, which can result in a significant delay in diagnosis.Citation1,Citation2 Efforts to identify additional prognostic biomarkers in melanocytic lesions continue to be a challenge. Hematoxylin and eosin (H&E) staining in conjunction with immunohistochemistry has remained the gold standard for dermatopathologists to confirm their diagnoses.Citation3 The choice of immunohistochemical stains may depend on the pathologists’ personal preferences; however, data on comparison between different immunostains are scarce.
Widely used immunohistochemical markers for the diagnosis of melanocytic lesions include Sry-related HMG-BOX gene 10 (SOX-10), human melanoma black-45 (HMB-45), and Melan-A/MART-1. These three immunohistochemical stains are used to visualize melanocytes in melanocytic lesions expressed in the epidermis and dermo-epidermal junction. SOX-10 is a nuclear transcription factor involved in the differentiation of neural crest cells to melanocytes.Citation2 Its nuclear pattern differentiates itself from the other commonly used melanocytic markers. It has been shown to be both a sensitive and specific marker in staining melanomas.Citation4 HMB-45 is a monoclonal cytoplasmic marker of the premelanosome complex, glycoprotein gp100. The HMB-45 stain is less sensitive, but fairly specific for melanocytic differentiation.Citation5 Melan-A/MART-1, also known as melanoma antigen, recognized by T cells, is a cytoplasmic protein.Citation6 In addition to staining melanocytes, Melan-A has been reported to stain melanophages. The Melan-A immunostain has an equal sensitivity and specificity for melanoma; however, it has been shown to stain melanoma more intensely and may appear to show more epidermal melanocytes than what is actually present.Citation3 Since there has not been a single antigen identified that stains with maximum sensitivity and specificity, immunohistochemical markers are typically used in combination.
Although immunohistochemistry has been the gold standard to distinguish melanocytic lesions, including benign versus malignant, histological diagnosis can be difficult, which has led to an increasing interest in finding a marker that is most beneficial in staining melanocytes. To date, there are no studies comparing the staining patterns of SOX-10, HMB-45, and Melan-A of melanocytes in lentigo senilis or benign melanocytic lesions. The objective of our study is to compare SOX-10, HMB-45, and Melan-A to determine the relative degree of immunohistochemical staining in lentigo senilis.
Methods
Thirty-two biopsy specimens with a histologic diagnosis of lentigo were randomly selected from the database at Pinkus Dermatopathology Lab, Monroe, MI. Lesions were chosen based on a clinical suspicion of lentigo maligna (melanoma in situ) but were histologically lentigo senilis or lentigo with focal melanocytic hyperplasia.
Each tissue section was formalin fixed (Thermo Scientific, Waltham, MA), embedded in paraffin (Cardinal Health, Dublin, OH), and cut at 4 µm thick. They were mounted onto charged slides and placed in a drying oven for 45 minutes at 60°C. The sections were immunostained with anti-SOX-10 antibody (prediluted RTU, Cell Marque, Rocklin, CA), anti-HMB-45 antibody (pre-diluted RTU, Leica Biosystems, Buffalo Grove, IL), and anti-Melan-A antibody (pre-diluted RTU, Leica Biosystems, Buffalo Grove, IL), using an automated Leica Bond-Max Polymer Refine Detection Kit (Leica Biosystems, Buffalo Grove, IL). The total number of melanocytes stained with each immunohistochemical stain was counted by two independent observers (DRM and TH). An average count was obtained from the two independent readings.
ANOVA test was used to analyze the significance of difference between three immunohistochemical stains. A linear mixed effects model was also employed to test the difference in the count of melanocytes. A p-value less than 0.05 was considered statistically significant.
Results
The study included a total of 32 benign melanocytic lesions from 32 biopsy specimens with lentigo senilis or mild junctional proliferation (). In all of the cases, the melanocytes stained positive for SOX-10, HMB-45, and Melan-A. Specimens stained more intensely with Melan-A and SOX-10 at the dermo-epidermal junction compared to HMB-45; however, the difference between SOX-10 and Melan-A was not statistically significant (p=0.9810, and ). The difference in the number of stained melanocytes was highly significant between HMB-45 and SOX-10 (p=0.0031) and between HMB-45 and Melan-A (p=0.0042) based on a pairwise comparison. Using a logarithmic scale, SOX-10 stained 0.195 more melanocytes/mm, or 1.215 times more, than HMB-45 (p=0.0026). Similarly, Melan-A stained 0.195 more melanocytes/mm, or 1.214 times more, than HMB-45 (p=0.0011, ). Overall, the three markers have a significantly different ability to stain melanocytes (p=0.0010, ANOVA).
Table 1 Clinical Data and Staining Results of Patients with a Diagnosis of Lentigo Senilis or Lentigo with Mild Junctional Proliferation
Figure 1 Mild atypical junctional proliferation. (A) H&E stain, (B) HMB-45 stain, (C) Melan-A stain, (D) SOX-10 stain. More intense staining noted for Melan-A and SOX-10 at the dermo-epidermal junction. Scale bar = 50 µm.
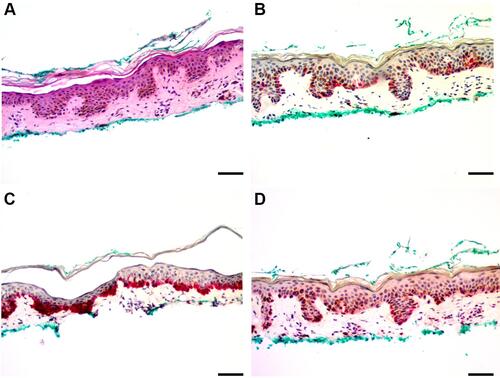
Figure 2 Lentigo with focal junctional melanocytic hyperplasia. (A) H&E stain, (B) HMB-45 stain, (C) Melan-A stain, (D) SOX-10 stain. Melan-A and SOX-10 showed increased staining at the dermo-epidermal junction. Scale bar = 50 µm.
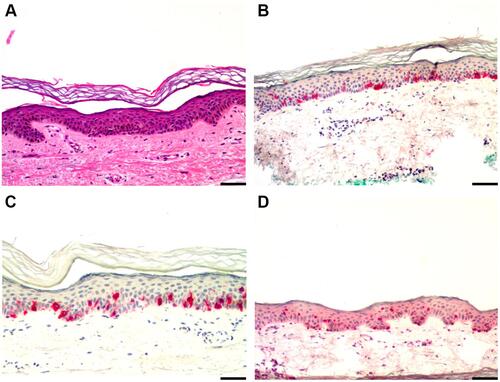
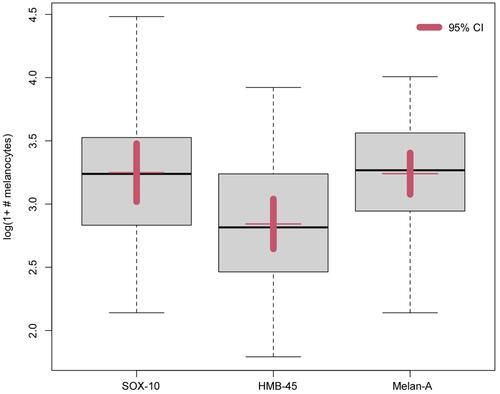
Figure 3 In a logarithmic scale, SOX-10 stained 1.215 times more melanocytes than HMB-45 (p=0.0026) and Melan-A stained 1.214 times more melanocytes than HMB-45 (p=0.0011) with a 95% confidence interval.
Discussion
Immunohistochemistry remains the most common aid used by dermatopathologists to assist in the distinction between benign and malignant melanocytic lesions. The S100 marker has historically been used as a melanocytic marker; however, it is highly sensitive but not specific for melanocytes as it is also expressed in epidermal Langerhans cells. Unfortunately, there still is not a single immunohistochemical marker that can achieve this distinction with certainty.Citation7 Often a subtle melanocytic proliferation can be easily missed. In particular, an early melanoma in situ may be difficult to differentiate from a lentigo senilis. Often this may lead to descriptive diagnoses such as “lentigo with junctional melanocytic hyperplasia” or “atypical junctional melanocytic proliferation”. All of the cases studied were submitted to rule out melanoma in situ but showed histologic findings of a lentigo senilis or mild atypical junctional proliferation. No cases showed definitive features of a melanoma such as pagetoid scatter of melanocytes or melanocytic nest formation. SOX-10, HMB-45, and Melan-A are highly specific for melanocytic cell types. However, our findings show that the choice of immunohistochemical stain may result in different sensitivity for melanocytes. In our study, Melan-A and SOX-10 both had a significant increase in staining compared with HMB-45, however, there was no significant difference in staining between Melan-A and SOX-10. As in , there was a prominent difference in staining of melanocyte dendrites between Melan-A and SOX-10. Even though there was not a statistical difference in the number of melanocytes stained, it was easier for the investigators to visualize melanocytes stained with SOX-10 compared to Melan-A. This is most obvious in , however also visible in .
HMB-45 and Melan-A have been previously compared in both benign and malignant melanocytic lesions.Citation8,Citation9 HMB-45 was found to be more specific, with greater staining at the dermo-epidermal junction, but lacking sensitivity. Moreover, Melan-A showed a diffuse staining of melanocytes in benign melanocytic lesions, being more sensitive overall. Melan-A was also found to stain heavily melanized keratinocytes and melanophages. This finding is consistent with what was seen in our stained biopsy specimens. Although HMB-45 did not stain as many melanocytes as SOX-10 and Melan-A, HMB-45 may be helpful in distinguishing between lentigo senilis and early melanoma in situ. This has been successfully demonstrated with staining of HMB-45 to differentiate pigmented actinic keratosis from lentigo maligna due to the reaction of HMB-45 in lesions with cytologic atypia and confluence of growth.Citation10
A more recent study directly compared Melan-A and SOX-10 immunostaining.Citation3 It was found that Melan-A stained significantly more melanocytes than SOX-10 in actinic keratoses; however, there was no difference in detecting melanocytic proliferations. Their results also showed that SOX-10 was more specific than Melan-A in identifying epidermal melanocytes on sun-damaged skin.Citation4 In our study, we did not find a difference between Melan-A and SOX-10 staining. Some authors argue that melanocytic cells can easily be overlooked in H&E-stained sections and Melan-A should be the primary biomarker. With this in mind, Drabeni et al stained with Melan-A after initially staining with H&E. Their findings resulted in 33% of in situ melanoma cases being reclassified as invasive melanoma.Citation11 In an opposing study, they found an increased number of melanocytes in the epidermis confirmed by a strong positivity for Melan-A in single cells and in small nests located at the dermo-epidermal junction. However, their histopathology showed the presence of a lichenoid dermatitis, not melanoma in situ. These results suggest that immunohistochemical investigations performed with Melan-A alone may lead to confusing and potentially disastrous results in analyzing pigmented lesions.Citation12
This is particularly important for dermatologic surgeons and pathologists in distinguishing the subtle features of melanoma in situ in the background of atypical junctional melanocytic hyperplasia. Due to overlapping features of sun-damaged skin, reading the surgical margins after an excision can be challenging as there is often melanocytic hyperplasia with or without an associated pigmented lesion and variability in melanocyte density adjacent to melanoma and nonmelanoma skin cancers.Citation13 Although melanocytic hyperplasia can be expected surrounding a melanoma on chronically sun-damaged skin, the progression of the melanocytic hyperplasia is still unclear.Citation14 Histologic discrimination of early melanoma in situ from benign melanocytic lesions can be challenging. Immunohistochemical studies of microphthalmia-associated transcription factor (MITF), a key component of the signal transduction pathway for the development of and differentiation of melanocytes, showed increased melanocyte density and nuclear diameter in melanoma in situ compared to a benign solar lentigo.Citation15,Citation16 This demonstrates the importance in using a stain with a high specificity for melanocytes. The lack of specificity of Melan-A immunostaining, as stated previously, may result in false-positive margins for surgical excision of melanoma in situ. In our study, Melan-A did not stain with clear, defined margins, possibly yielding more stained melanocytes than what was actually present. In addition, some authors have proposed that there is a continuum between solar lentigo and lentigo maligna. They have described it as a solar lentigo with melanocytic hyperplasia not extending past the margin of the lesion. Although distinguishing criteria for the diagnosis of melanoma in situ compared to melanocytic hyperplasia has been identified, there is uncertainty as to whether or not a solar lentigo may be a precursor lesion to lentigo maligna.Citation17 This highlights the important role immunohistochemistry plays in the histopathological identification of benign melanocytic lesions from early malignancy.
Overall, we found a significant increase in staining with Melan-A and SOX-10 at the dermo-epidermal junction, compared to HMB-45. However, no significant difference was noted between Melan-A and SOX-10. A potential limitation to our study is the limited sample size. Although a difference in melanocyte count was not observed between Melan-A and SOX-10, our results show an apparent trend approaching significance. Melan-A or SOX-10 may be superior in staining melanocytes in melanocytic lesions, however SOX-10 may be more specific. Immunohistochemistry itself carries a few obstacles including its small biopsy size with a limited number of melanocytes and its differing sensitivity and specificity of antibodies to differentiate between melanocytes and keratinocytes.Citation12 Pathologists need to consider the relative sensitivity of the stains utilized when interpreting results of staining in subtle melanocytic proliferations.
In conclusion, immunohistochemical stains are commonly used to quantify melanocytic proliferation, especially in the differential diagnosis of lentigo senilis and early melanoma in situ. Our study shows that the choice of immunohistochemical stain may result in different sensitivity for melanocytic proliferation.
Statement of Ethics
This study was performed in accordance with ethical guidelines of the Declaration of Helsinki. Ethical approval to conduct this study was obtained from the Institutional Review Board (IRB) of Wayne State University, Detroit, MI. Consent requirement was waived as unidentified archived pathology materials were used in this study.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Okamura JM, Barr RJ, Cantos KA, et al. Benign atypical junctional melanocytic hyperplasia associated with intradermal nevi: a common finding that may be confused with melanoma in situ. Modern Pathol. 2000;13(8):857–860. doi:10.1038/modpathol.3880152
- Muzumdar S, Argraves M, Kristjansson A, et al. A Quantitative comparison between SOX10 and MART-1 immunostaining to detect melanocytic hyperplasia in chronically sun-damaged skin. J Cutan Pathol. 2018;45(4):263–268. doi:10.1111/cup.13115
- Kasprzak JM, Yaohui GX. Diagnosis and management of lentigo maligna: a review. Drugs Context. 2015;4:212281. doi:10.7573/dic.212281
- Prieto VG, Shea RC. Immunohistochemistry of melanocytic proliferations. Arch Pathol Lab Med. 2011;135:7. doi:10.5858/2009-0717-RAR.1
- Ohsie SJ, Sarantopoulos GP, Cochran AJ, et al. Immunohistochemical characteristics of melanoma. J Cutan Pathol. 2008;35(5):433–444. doi:10.1111/j.1600-0560.2007.00891.x
- Shabrawi-Caelen LE, Kerl H, Cerroni L. Melan-A: not a helpful marker in distinction between melanoma in situ on sun-damaged skin and pigmented actinic keratosis. Am J Dermatopathol. 2004;26(5):364–366. doi:10.1097/00000372-200410000-00003
- Koh SS, Cassarino DS. Immunohistochemical expression of p16 in melanocytic lesions: an updated review and meta-analysis. Arch Pathol Lab Med. 2018;142(7):815–828. doi:10.5858/arpa.2017-0435-RA
- Willis BC, Johnson G, Wang J, et al. SOX10: a Useful marker for identifying metastatic melanoma in sentinel lymph nodes. Appl Immunohistochem Mol Morphol. 2015;23(2):109–112. doi:10.1097/PAI.0000000000000097
- Clarkson K, Sturdgess I, Molyneux A. The usefulness of tyrosinase in the immunohistochemical assessment of melanocytic lesions: a comparison of the novel T311 antibody (anti-tyrosinase) with S-100, HMB45, and A103 (anti-Melan-A). J Clin Pathol. 2001;54(3):196–200. doi:10.1136/jcp.54.3.196
- Ribé A, McNutt NS. S100A protein expression in the distinction between lentigo maligna and pigmented actinic keratosis. Am J Dermatopathol. 2003;25(2):93–99. doi:10.1097/00000372-200304000-00001
- Drabeni M, Lopez-Vilaró L, Barranco C, et al. Differences in tumor thickness between hematoxylin and eosin and Melan-A immunohistochemically stained primary cutaneous melanomas. Am J Dermatopathol. 2013;35(1):56–63. doi:10.1097/DAD.0b013e31825ba933
- Beltraminelli H, Shabrawi-Caelen LE, Kerl H, et al. Melan-a-positive “pseudomelanocytic nests”: a pitfall in the histopathologic and immunohistochemical diagnosis of pigmented lesions on sun-damaged skin. Am J Dermatopathol. 2009;31(3):305–308. doi:10.1097/DAD.0b013e31819d3769
- Barlow J, Maize J, Lang P. The density and distribution of melanocytes adjacent to melanoma and nonmelanoma skin cancers. Dermatologic Surg. 2007;33(2):199–207.
- Johnson TM, Smith JW, Nelson BR, et al. Current therapy for cutaneous melanoma. J Am Acad Dermatol. 1995;32:689–707. doi:10.1016/0190-9622(95)91443-9
- Bertolotto C, Abbe P, Hemesath TJ, et al. Microphthalmia gene product as a signal transducer in cAMP-induced differentiation of melanocytes. J Cell Biol. 1998;142:827–835. doi:10.1083/jcb.142.3.827
- Black WH, Thareja SK, Blake BP, et al. Distinction of melanoma in situ from solar lentigo on sun-damaged skin using morphometrics and MITF immunohistochemistry. Am J Dermatopathol. 2011;33(6):573–578. doi:10.1097/DAD.0b013e3182093b13
- Byrom L, Barksdale S, Weedon D, et al. Unstable solar lentigo: a defined separate entity. Australas J Dermatol. 2016;57(3):229–234. doi:10.1111/ajd.12447