
Abstract
Pyoderma gangrenosum (PG) is a rare autoinflammatory skin disorder, which is characterised by rapidly developing and tender cutaneous ulcers. The treatment of PG is challenging. Palmoplantar pustulosis (PPP) is also an autoinflammatory dermatosis with sterile pustules on the palms and/or the soles. We demonstrated a 68-year-old patient with coexisting autoinflammatory diseases including PG, 1-year history of plaque psoriasis and PPP, recovered after treatment with adalimumab. We also reviewed published reports of PG-associated autoinflammatory syndromes with adalimumab.
Introduction
Pyoderma gangrenosum (PG) represents a neutrophilic dermatosis characterized by painful, sharply marginated with violaceous ulcers commonly on the lower extremities, especially the pretibial area.Citation1 PG is a rapidly evolving and debilitating disease with severe physical and psychosocial burden.Citation2 The pathophysiology of PG is still not clear.Citation3 PG may be a cutaneous consequence of autoinflammation.Citation4 PG is often associated with immune-mediated diseases that involve inflammatory bowel disease and rheumatoid arthritis.Citation2
Palmoplantar pustulosis (PPP), a chronic and relapsing disease, is characterized by sterile and erupting pustules on the palms and/or the soles.Citation5
Plaque psoriasis is a chronic, immune-mediated skin disease characterized by erythematous scaly patches or plaques that occur commonly on extensor surfaces.9
Severe PG is defined as a patient having multiple ulcers, or a single ulcer of 3 cm or greater, or involvement of the face.2 Patients with mild disease are initially treated with a low-dose immunosuppressive agent (such as prednisone and cyclosporine) and/or localized (topical or intralesional) therapy.2 Adverse effects may occur in patients treated with prednisone or cyclosporine, including infection, hyperglycaemia, renal dysfunction, gastrointestinal disturbance and hypertension.Citation6
It has been suggested that imbalance of the congenital immunity including some common cytokines such as Tumor necrosis factor (TNF)-α, interleukin (IL)-17 and IL-23 may play a crucial role in the progress of both PGCitation7 and PPPCitation8 in recent research. Adalimumab, an anti-TNF-α antibody, was approved for the therapy of psoriasis.Citation9 It has been showed to be effective and generally well tolerated for Japanese patients with active ulcers of PG.Citation10
Herein, we report our successful experience of a patient of PG, plaque psoriasis and PPP with adalimumab.
Case Report
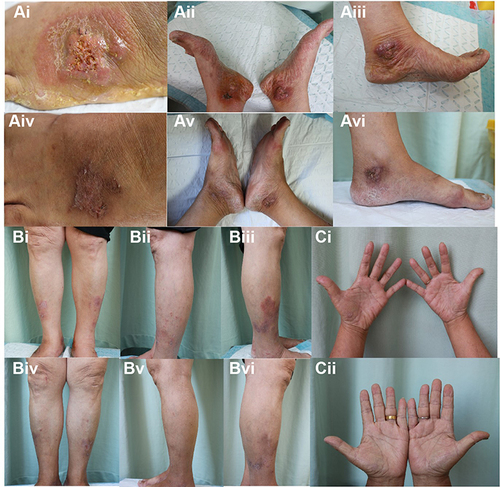
A 68-year-old female attended to our outpatient clinic with a 2-month history of persistent, rapidly developing and aching ulcers affecting her feet () and 1-year history of plaque psoriatic lesions symmetrically distributed on the lower extremities (). Pustules were found on her palms (). She denied history of lesions on her face and joint symptoms.
Figure 1 A female patient with pyoderma gangrenosum, plaque psoriasis and palmoplantar pustulosis who is treated with adalimumab. Lesions of (Ai–Aiii) pyoderma gangrenosum, (Bi–Biii) plaque psoriasis and (Ci) palmoplantar pustulosis were significantly improved (Aiv–Avi, Biv–Bvi and Cii) after 3 months by treating with adalimumab.
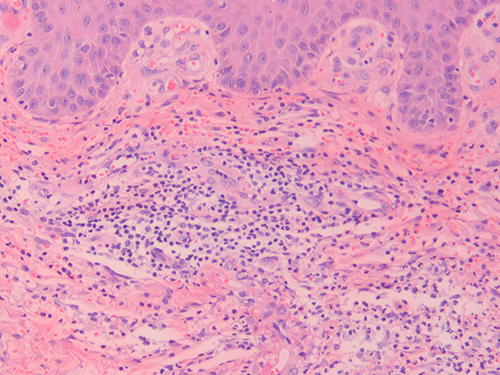
Laboratory investigations revealed elevated levels of C-reactive protein (14.1 mg/L; normal, <8 mg/L) and erythrocyte sedimentation rate (74 mm/H; normal, <20 mm/H). The outcome of syphilis antibody and T cell spot test for tuberculosis infection was negative. We have scraped some flakes for fungal culture to rule out fungal infections. Other laboratory investigations, including complete blood count, liver functions and renal functions were unremarkable. Histopathology of the ulcer near the right medial malleolus showed dense neutrophils which confined to the dermis (), with no indication of cutaneous vasculitis, mycobacterium tuberculosis, parasitic infections or fungal infections. The clinical and histopathological findings above were consistent with PG. Based on the erythematous scaly plaques distributed on the lower extremities, diagnosis of plaque psoriasis was made. The patient also had pustules on her palms leading to the clinical diagnosis of PPP.
Figure 2 Histopathology of the ulcer near the right medial malleolus. (40×) H & E stain showing dense neutrophilic infiltrate in the dermis.
She was treated with adalimumab with 80 mg subcutaneously at week 0 and then 40 mg every 2 weeks. In the third month, the lesions of PG (), psoriasis () and PPP () improved markedly. The Psoriasis Area Severity Index score improved from 2.4 to 0.2. The body surface area of psoriasis reduced from 1.5% to 0.5%. She did not report any adverse effects during the period of therapy.
Discussion
The coexistance of PG and PPP is rarely reported in literature. Only six cases in Japanese populationCitation8 and one case from NepalCitation11 have been reported till date. To our knowledge, our case firstly described the coexistence of plaque psoriasis, PPP and PG.
PPP is a kind of inflammatory disease that affects the palms and/or the soles with sterile pustules, which are debilitating and usually resistant to treatment.Citation5 PPP is a limited form of pustular psoriasis and presents both in isolation and in patients with a history of plaque psoriasis .Citation12
Case series and case reports may have revealed the efficacy and safety of adalimumab for the treatment of pyoderma gangrenosum-associated autoinflammatory syndromes (Supplementary Table 1). Adalimumab was successful for treating 3 patients with PAPA (pyogenic arthritis, pyoderma gangrenosum and acne), 3 patients with PASS (pyoderma gangrenosum, acne, suppurative hidradenitis and ankylosing spondylitis), 3 patients with PsAPASH (psoriatic arthritis, pyoderma gangrenosum, acne, suppurative hidradenitis), 1 patient with PAPASH (pyoderma gangrenosum, acne, psoriasis, arthritis and suppurative hidradenitis) and 6 patients with PASH (pyoderma gangrenosum, acne, suppurative hidradenitis). On a pathogenetic basis, these conditions share the common pathway, which involves the imbalance of the innate immunity that results in increased levels of IL-1 family, induction of TNF-α and subsequent sterile neutrophilic infiltration in the skin.2 The involvement of TNF-α could justify the treatment of blocking TNF-α in these patients.
It has been reported that PG responds well to biologics against IL-1β,Citation13 IL-12,Citation14 IL-17,Citation15 IL-23,Citation16 IL-1 receptor,Citation17 IL-6 receptorCitation18 and most commonly TNF.Citation19 The T helper (Th)17/TNF-α axis leading to neutrophil infiltration has been shown in the pathogenetic basis of psoriasis,Citation20 PPPCitation8 and PG.Citation2 It is shown in recent studies that TNF‐α, IL‐17 and IL‐23 are increased in lesional skin of PG and PPP. IL-17-positive lymphocytes were observed in biopsy samples obtained from a leg ulcer and plantar pustule.Citation8 These findings indicate that the Th 17/TNF-α axis may perform key roles in both PG and PPP.
Physicians need to consider the presence of coexisting diseases when they are selecting the treatment. Methotrexate, cyclosporine and biologics are potential therapeutic modalities for this patient. However, the possibility of therapeutic failures and side-effects of methotrexate and cyclosporine make the clinicians to shift them to alternative long-term therapies. Cyclosporine can cause significant side effects, such as hypertension and nephrotoxicity, while methotrexate can lead to hepatic and hematological toxicities, limiting their long-term use.Citation5 Therefore, we tried treating this patient with adalimumab and the outcome was satisfactory.
In summary, we reported a case of PG, plaque psoriasis and PPP successfully treated with adalimumab. Further clinical observations will be necessary to assess the prevalance of this clinical entity and the efficacy of adalimumb.
Consent for Publication
Informed consent for publication of the case details and connected images was gained from the patient. Institutional approval from the Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine has been obtained to publish the case details (Approved number: IIT-2022-004).
Disclosure
The authors report no conflicts of interest.
Additional information
Funding
References
- Ashchyan HJ, Nelson CA, Stephen S, et al. Neutrophilic dermatoses: pyoderma gangrenosum and other bowel- and arthritis-associated neutrophilic dermatoses. J Am Acad Dermatol. 2018;79:1009–1022. doi:10.1016/j.jaad.2017.11.063
- Maverakis E, Marzano AV, Le ST, et al. Pyoderma gangrenosum. Nat Rev Dis Primers. 2020;6(81). doi:10.1038/s41572-020-0213-x
- Saternus R, Schwingel J, Muller CSL, Vogt T, Reichrath J. Ancient friends, revisited: systematic review and case report of pyoderma gangrenosum-associated autoinflammatory syndromes. J Transl Autoimmun. 2020;3:100071. doi:10.1016/j.jtauto.2020.100071
- Satoh TK, Mellett M, Contassot E, French LE. Are neutrophilic dermatoses autoinflammatory disorders? Br J Dermatol. 2018;178:603–613. doi:10.1111/bjd.15105
- Freitas E, Rodrigues MA, Torres T. Diagnosis, screening and treatment of Patients with Palmoplantar Pustulosis (PPP): a review of current practices and recommendations. Clin Cosmet Investig Dermatol. 2020;13:561–578. doi:10.2147/CCID.S240607
- Ormerod AD, Thomas KS, Craig FE, et al. Comparison of the two most commonly used treatments for pyoderma gangrenosum: results of the STOP GAP randomised controlled trial. BMJ. 2015;350:h2958–h2958. doi:10.1136/bmj.h2958
- Fischer-Stabauer M, Boehner A, Eyerich S, et al. Differential in situ expression of IL-17 in skin diseases. Eur J Dermatol. 2012;22:781–784. doi:10.1684/ejd.2012.1854
- Ohtsuka M, Yamamoto T. Rare association of pyoderma gangrenosum and palmoplantar pustulosis: a case report and review of the previous works. J Dermatol. 2014;41:732–735. doi:10.1111/1346-8138.12543
- Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323:1945–1960. doi:10.1001/jama.2020.4006
- Yamasaki K, Yamanaka K, Zhao Y, et al. Adalimumab in Japanese patients with active ulcers of pyoderma gangrenosum: twenty-six-week Phase 3 open-label study. J Dermatol. 2020;47:1383–1390. doi:10.1111/1346-8138.15533
- Pukar C, Sudha A, Punam P. Simultaneous occurrence of pyoderma gangrenosum and palmoplantar pustular psoriasis: is it an association or coincidental findings? Clin Case Rep. 2021;9(1):410–415. doi:10.1002/ccr3.3544
- Noe MH, Wan MT, Mostaghimi A, et al. Evaluation of a case series of patients with palmoplantar pustulosis in the United States. JAMA Dermatol. 2022;158:68–72. doi:10.1001/jamadermatol.2021.4635
- Kolios AG, Maul J-T, Meier B, et al. Canakinumab in adults with steroid-refractory pyoderma gangrenosum. Br J Dermatol. 2015;173:1216–1223. doi:10.1111/bjd.14037
- Goldminz AM, Botto NC, Gottlieb AB. Severely recalcitrant pyoderma gangrenosum successfully treated with ustekinumab. J Am Acad Dermatol. 2012;67:e237–e238. doi:10.1016/j.jaad.2012.04.045
- McPhie ML, Kirchhof MG. Pyoderma gangrenosum treated with secukinumab: a case report. SAGE Open Med Case Rep. 2020;8:2050313X20940430. doi:10.1177/2050313X20940430
- John JM, Sinclair RD. Tildrakizumab for treatment of refractory pyoderma gangrenosum of the penis and polymyalgia rheumatica: killing two birds with one stone. Australas J Dermatol. 2020;61:170–171. doi:10.1111/ajd.13196
- Brenner M, Ruzicka T, Plewig G, Thomas P, Herzer P. Targeted treatment of pyoderma gangrenosum in PAPA (pyogenic arthritis, pyoderma gangrenosum and acne) syndrome with the recombinant human interleukin-1 receptor antagonist anakinra. Br J Dermatol. 2009;161:1199–1201. doi:10.1111/j.1365-2133.2009.09404.x
- Solovan C, Nicula Proca A, Ursoniu S. Pros and cons of biological therapy in psoriasis. J Eur Acad Dermatol Venereol. 2017;31(2):e74–e75. doi:10.1111/jdv.13735
- Patel F, Fitzmaurice S, Duong C, et al. Effective strategies for the management of pyoderma gangrenosum: a comprehensive review. Acta Derm Venereol. 2015;95:525–531. doi:10.2340/00015555-2008
- Martin DA, Towne JE, Kricorian G, et al. The emerging role of IL-17 in the pathogenesis of psoriasis: preclinical and clinical findings. J Invest Dermatol. 2013;133:17–26. doi:10.1038/jid.2012.194