Abstract
Minocycline is a tetracycline derivative antibiotic commonly prescribed for acne, rosacea, and other inflammatory skin disorders. Minocycline turns black when oxidized, leading to discoloration of the skin, nails, bulbar conjunctiva, oral mucosa, teeth, bones, and thyroid gland. Hyperpigmentation has been reported after long-term minocycline therapy with at least 100 mg/day. Three types of minocycline-induced cutaneous hyperpigmentation can result. Type I is the most common, and is associated with blue-black discoloration in areas of previous inflammation and scarring. Type II most commonly affects the legs and is characterized by blue-gray pigmentation of previously normal skin. Type III is the least common and is characterized by diffuse muddy-brown discoloration predominantly on sun exposed skin. Minocycline-induced hyperpigmentation may be cosmetically disfiguring and prompt identification is essential. Without treatment, symptoms may take several months, to years to resolve, after discontinuation of the drug. However, the pigmentation may never completely disappear. In fact, there have been few reports of complete resolution associated with any therapeutic intervention. We report a case of a patient on long-term minocycline therapy utilized as an anti-inflammatory agent to control symptoms of rheumatoid arthritis, which led to minocycline-induced hyperpigmentation of the face. To remove the blue-gray cutaneous deposits, 3 Q-switched lasers (Neodymium: yttrium aluminum garnet (Nd:YAG) 1064 nm, Alexandrite 755 nm, and Ruby 694 nm) were used in test areas. The Alexandrite 755 nm laser proved to provide effective clearing of the minocycline hyperpigmentation requiring just 2 treatments, with minimal treatment discomfort and down time.
Introduction
Diffuse blue-gray skin discoloration has been reported in several conditions such as Addison’s disease, argyria, hemochromatosis and polycythemia vera.Citation1 Riehl melanosis is characterized by brown-violet pigmentation on sun-exposed areas, erythema, and pruritus.Citation2 Erythema dyschromicum perstans is either idiopathic or acquired, typically occurs in those younger than 40 years, and first presents with erythematous macules that slowly turn slate gray resulting in gray-blue hypermelanosis.Citation2 Finally, end-stage metastatic melanoma can produce a blue-gray to brown hue to the body.Citation2 In addition, drugs including minocycline, amiodarone, zidovudine, and bleomycin have been reported to cause cutaneous darkening ().
Table 1 Drugs associated with cutaneous darkening and special attributes
Minocycline is a semi-synthetic tetracycline antibiotic that turns black when oxidized, and can produce discoloration of the skin, nails, oral mucosa, conjunctiva, teeth, bones, and thyroid gland.Citation3 Three types of minocycline-induced cutaneous hyperpigmentation have been described:Citation3
Type I is the most common, and is associated with blue-black discoloration in areas of previous inflammation and scarring.
Type II most commonly affects the legs and is characterized by blue-gray pigmentation of previously normal skin.
Type III is the least common and is characterized by diffuse muddy-brown discoloration predominantly on sun-exposed skin.
Minocycline-induced hyperpigmentation is associated with long-term use of this drug. Any patient receiving more than 100 grams of minocycline can develop discoloration.Citation4 The pigment deposition is the result of a drug metabolite-protein complex chelated with calcium, or an insoluble minocycline-melanin complex.Citation5 Minocycline hyperpigmentation occurs in 2.4% to 14.8% of patients on chronic treatment, most commonly for acne and rosacea.Citation5 In a study of 700 patients on high-dose long-term minocycline treatment for acne (100 mg daily, 100/200 mg on alternate days, or 200 mg daily for 10.5 months), the only side effect that was significantly greater in patients taking higher doses (cumulative dose greater than 70 g) compared with lower doses was pigmentation (P < 0.01).Citation6 Its anti-inflammatory effects are helpful for rheumatoid arthritis, immunobullous disease and other inflammatory diseases.Citation3 The incidence of minocycline pigmentation is higher in patients treated for autoimmune diseases and may be more common with increasing age.Citation3
Q-switched lasers use high energy, nanosecond pulsing and are available in 3 wavelengths for drug-induced pigmentation, including the Ruby 694 nm, the Alexandrite 755 nm, and the Nd:YAG infrared 1064 nm.Citation7 There have been reports of the Alexandrite laser leading to the resolution of Type II minocycline induced hyperpigmentation.Citation6 Other reports have shown efficacy of the Ruby laser for minocycline facial and leg pigmentation.Citation8,Citation9 A single study compared the YAG and Ruby lasers in the treatment of minocycline pigmentation and the Ruby laser was found to be more effective.Citation9 However, there are no studies comparing the 3 Q-switched lasers for effectiveness and patient comfort in the treatment of minocycline-induced hyperpigmentation.
Case
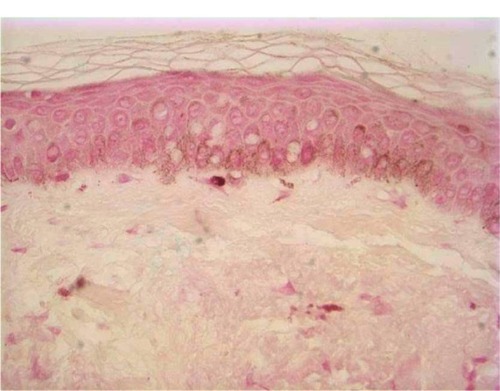
A 70-year-old caucasian male presented with a one-year history of progressive worsening blue-gray discoloration of the face. There were no associated symptoms and no history of previous gold therapy. Physical examination revealed macular, non-blanching, diffuse blue-gray hyperpigmentation on the forehead, temples, cheeks, nose, and chin sparing the oral mucosa. The patient was taking 100 mg of minocycline orally twice daily for 3 years (total 219 grams) to suppress symptoms of rheumatoid arthritis. The patient noticed increased darkening of the face over the past year. Minocycline was discontinued to prevent further pigmentation. A 0.4 × 0.3 × 0.3 cm punch biopsy demonstrated mild perivascular lymphocytic infiltrates with increased pigment deposition in the basal layers of the epidermis (). Iron stain was negative ().
Figure 1 Minocycline-induced hyperpigmentation.
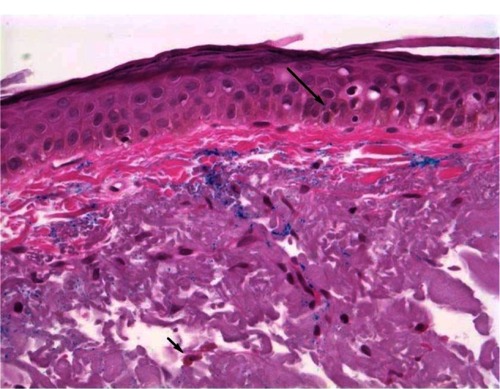
Figure 2 Iron stain.
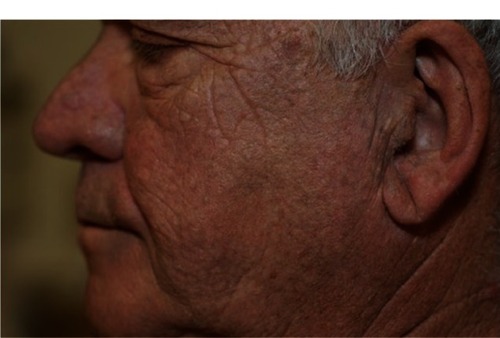
The patient was spot-treated with 3 Q-switched lasers (1064 nm, [Palomar Spectrum RD1200] 755 nm, and 694 nm [both Syneron-Candela Alex Trivantage]) to evaluate which laser would achieve the best results in removing pigmentation with minimal discomfort. No topical anesthetic was used. The 1064 nm laser was set at 1.6 joules (J) with a 5 mm spot size. The 755 nm laser used a fluence of 5.5 J with a 4 mm spot size. The 694 nm was set at 4 J with a 6.5 mm spot size. The results of the trial therapy after 1 week are shown in . The 1064 nm revealed minimal to no change in pigment. The 755 nm showed a 50% improvement with minimal discomfort. The 694 nm showed 90% improvement, however was uncomfortable for the patient. We chose the 755 nm laser for treatment based on its significant improvement with minimal pain, discomfort, and downtime for the patient. The patient received two full-face treatments spaced 2 weeks apart with the 755 nm at 5.5 J and 4 mm spot size and one follow-up spot treatment. These treatments led to complete resolution of hyperpigmentation and the patient was completely satisfied with the result (). Sun protection was encouraged following treatments.
Figure 3 Diffuse blue-black darkening after prolonged minocycline use.
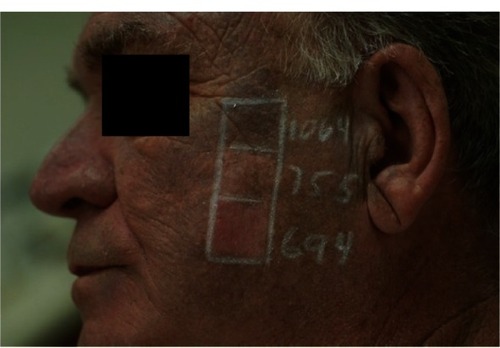
Figure 4 Results after 2 sessions with the Q-switched Alexandrite (755 nm) laser.
Discussion
This patient had Type III minocycline-induced hyperpigmentation on the sun-exposed skin of the face after taking 219 grams of minocycline over 3 years. Of the 3 Q-switched lasers tested, the 755 nm laser was effective in reversing pigmentation with minimal patient discomfort after 2 treatments. Type III minocycline-induced hyperpigmentation is less likely to respond than Types I and II.Citation3 It is not known exactly how laser therapy removes the pigment associated with minocycline use, but is thought to result from fragmentation of the intracellular and extracellular pigmentation and drainage through the lymphatic system.Citation2
The recommended minocycline dose for acne is 100–200 mg daily. Many patients treated for a year or two will reach a cumulative dose of over 100 g. According to the US Food and Drug Administration (FDA), there is a manufacturing delay of tetracycline leading to a shortage of the drug.Citation10 As a result, physicians are forced to use alternative medications such as doxycycline.Citation10 Therefore, we may see a greater incidence of minocycline-induced hyperpigmentation as minocycline prescribing increases. Fortunately, we can utilize the Alexandrite 755 nm laser to remove pigmentation associated with the use of this drug. A recent case reported successful treatment with the Alexandrite laser, with the patient deciding to continue minocycline therapy and returning 3 years later with recurrence to receive another laser treatment.Citation11
Disclosure
The authors report no conflicts of interest in this work.
References
- MerchantFCarpenterTBlue-gray discoloration of the skinAm Fam Physician1012011847821822222010621
- KaliaSAdamsSPDermcase. Minocycline-induced pigmentationCan Family Physician5200652595596
- PecinaJLPittelkowMRHyperpigmentation – a case studyAust Fam Physician9201140970170221894278
- EisenDHakimMDMinocycline-induced pigmentation: Incidence, prevention, and managementDrug Saf619981864314409638388
- MoutonRWJordaanHFSchneiderJWA new type of minocycline-induced cutaneous hyperpigmentationClin Exp Dermatol1200429181414723711
- GreenDFriedmanKJTreatment of minocycline-induced cutaneous pigmentation with the Q-switched Alexandrite laser and a review of the literatureJ Am Acad Dermatol2200144Suppl 234234711174411
- GouldenVGlassDCunliffeWJSafety of long-term high-dose minocycline in the treatment of acneBr J Dermatol4199613446936958733373
- KnoellKAMilgraumSSKutenplonMQ-switched ruby laser treatment of minocycline-induced cutaneous hyperpigmentationArch Dermatol10199613210125112538859046
- TsaoHBusamKBarnhillRLDoverJSTreatment of minocycline-induced hyperpigmentation with the Q-switched ruby laserArch Dermatol10199613210125012518859045
- RuthCRunning on empty. FDA, Congress working to mitigate drug shortagesDerm World72012
- SamalonisLBQ-switched lasers effective for treating drug-induced hyperpigmentationDermatology Times312012
- HolmANNelsonWKImages in clinical medicine. Minocycline-induced hyperpigmentationN Engl J Med1116200635520e2317108338
- WiperARobertsDHSchmittMAmiodarone-induced skin pigmentation: Q-switched laser therapy, an effective treatment optionHeart120079311517170336
- GuptaLKTanwarRKKhareAKJainSKBleomycin induced flagellate pigmentationIndian J Dermatol Venereol LeprolMay-Jun200268315815917656922
- GreenbergRGBergerTGNail and mucocutaneous hyperpigmentation with azidothymidine therapyJ Am Acad Dermatol21990222 Pt 23273302303586