
Abstract
Cutaneous pili migrans is a rare condition caused by embedded hair shafts or fragments which presents as a mobile black linear rash and is easily confused with cutaneous larva migrans. “Ingrowing hair”, in which the hair shaft grows inside the skin and burrows into the uppermost dermis rather than exiting the skin, is much rarer, and only 8 cases have been reported thus far, all in Asian men. We report a case of a 22-year-old Chinese male with a 4 cm-long black linear rash that migrated from the anterior abdomen to the left lower abdomen. The black lines represented hair shafts with follicular structures. The lesion disappeared immediately after hair removal. No recurrence occurred in 4 weeks of follow-up. To our knowledge, this is the first description of ingrowing hair occurring in the abdomen.
Introduction
Cutaneous pili migrans (CPM) is a rare condition caused by the movement of a hair shaft or fragment within the shallow epidermis or dermis, causing an eruption resembling cutaneous larva migrans.Citation1 To date, no more than 30 cases have been reported, with a high prevalence in Asian men.Citation2 However, in 2006, Sakai et al reported four Japanese cases classified as ingrown hair, in which the causative hair shaft grew inside the skin and burrowed into the uppermost dermis rather than exiting the skin.Citation3 In 2016, Luo et alCitation2 renamed this condition “ingrowing hair” because they believed it to be better than “ingrown hair” to describe the condition. In addition, Liu et al suggested that “ingrown hair” and “ingrowing hair” could easily be confused and thought that intradermal growing hair (IGH) may be a more appropriate term to describe this condition,Citation4 which is seen even more rarely. To our knowledge, only eight cases, including four JapaneseCitation3 and four ChineseCitation5 cases, have been reported to date. In this study, we added another new case.
Case Report
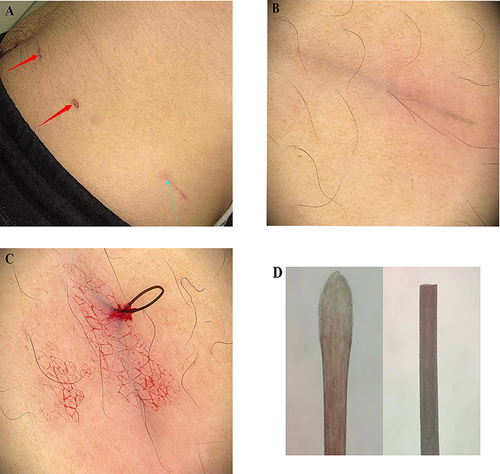
A 22-year-old Chinese male discovered a black line under the skin of the anterior abdomen one week before presentation. He felt a crawling sensation under the skin without any other symptoms and denied any history of trauma or recent travel abroad. There was no similar condition among his family members. A dermatologist suspected cutaneous larva migrans; however, no larva was found after carbon dioxide laser treatment, leaving pigmentation on the anterior abdominal skin (, red arrow). On re-evaluation, the next day, the black linear lesion had further migrated, and the eruption extended to the left lower abdomen. Physical examination revealed a 4 cm long, slightly elevated, black linear eruption in the skin of the left lower abdomen, with inflammatory erythema surrounding the lesion (, blue arrow). A black lesion was observed on the upper skin. Dermoscopy revealed a thick black line below the skin resembling a hair shaft without vasodilation (). Subsequently, we pierced the skin over one-third of the lesion using a sterile syringe and clamped the black line with forceps, pulling it out with minor bleeding (). The black line was identified as a hair shaft with intact follicles under a light microscope (). The diagnosis of “ingrowing hair” was made. After the hair shaft had been removed, the lesion disappeared immediately, leaving slight pigmentation. No recurrence was observed at the follow-up 4 weeks after treatment.
Figure 1 The presentations of ingrowing hair. The anterior abdominal shows pigmentation after carbon dioxide laser treatment (red arrow); a 4-cm-long black linear lesion beneath the skin located on the left lower abdomen associated with inflammatory erythema around (blue arrow) (A). The dermoscopy shows a black line under the skin without vasodilation (×20, polarized light) (B). A hair is pulled out with the association of bleeding by the forceps (C). The microscope shows a hair shaft with follicles (D).
Discussion
Cutaneous pili migrans (CPM) has been described by other authors with multiple terms, such as embedded hair, bristle migrans, burrowing hair, moving hair, creeping hair, and ingrowing hair.Citation3,Citation5 Some scholars believe that “ingrown hair”,Citation3,Citation6 “ingrowing hair”,Citation2 and “intradermal growing hair”Citation4 can all be used to describe one type of cutaneous pili migrans. Based on the aetiology and the presence of hair follicles, CPM can be divided into two categories. One category involves an exogenous hair fragment or hair shaft embedded in the skin that has no hair follicles at either end of the skin lesion. The other category is “ingrowing hair”, which has intact follicles and involves hair growing inside the skin, but the exact mechanisms for ingrowing hair remain unknown. Luo et al suggested that actions such as friction, pulling, or extruding the beard might play an important role in the pathogenesis of ingrowing hair by causing localized inflammation and oedema around the hair follicle or by changing the growth direction of the hair, leading to the possibility of hair growth inside the skin.Citation2 To date, eight cases of “ingrowing hair” have been reported, all of which were observed on the neck and face of the affected individuals.Citation2–5 These studies suggest that ingrowing hair always occurs in beard growth areas and is prevalent among Asian men. This may be because Asian hairs have a larger diameter with a circular geometry that are harder and straighter, making it easier for hairs to grow and extend inside the skin.Citation7
In our case, a black linear eruption was present on the abdomen, and the follicle structure was obvious under the microscope. When the skin was punctured, the hair was easily removed with forceps. We were also unsure how the black linear eruption occurred on the abdomen. Sakai et alCitation3 reported that a hair shaft released from the hair follicle in the catagenic period has dried connective tissue at the lower end. It is highly unlikely that the released hair shaft repenetrated the skin; rather, an ingrown hair in the pubic area continued moving forward from the lower end after being released from the hair follicle. Since the structure of pubic hair is similar to that of the beard, we speculate that the ingrowing hair in the pubic area migrated with the movement of the body, growing inside the skin and slowly extending from the pubic area to the anterior abdomen and the left lower abdomen, which caused the patient to seek medical attention. The erythema may be an inflammatory response caused by the hair, since the reaction disappeared after the hair was removed. However, when we pulled out the hair, we observed that the hair was hard, much harder than pubic hair, so there were some flaws in our speculation. In general, this case is different from other cases reported in the past and offers a new perspective on the further understanding of the disease.
To our knowledge, ingrowing hair that occurs in the pubic or inguinal areas has not yet been reported. This case provides new insights that ingrowing hair can occur anywhere in the body. Ingrowing hair is easily underestimated, misdiagnosed, or neglected because hairs growing inside the skin are primarily asymptomatic and are often unnoticed. Dermoscopy and biopsy are valuable diagnostic tools for ingrowing hair. The limitation of this case is that we did not perform a biopsy on this patient and lack histopathology results. In summary, when ingrowing hair is diagnosed, a minimally invasive removal technique using forceps and dermoscopy can reduce pain, bleeding, procedure time, and secondary infection risk, as dermoscopy can be used to locate the openings of the punctured skin to promote this process.
Consent Statement
Oral and written consent was obtained from the patient for publication of the article images, and the patient was shown the content of the article to be published. Institutional approval was not required to publish the case details.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Cascais M, Folques C, Pinho A, Rodrigues F. Cutaneous pili migrans, a creeping eruption. J Pediatr. 2022. doi:10.1016/j.jpeds.2022.09.058
- Luo DQ, Liang YH, Li XQ, Zhao YK, Wang F, Sarkar R. Ingrowing hair: a case report. Medicine. 2016;95(19):e3660. doi:10.1097/md.0000000000003660
- Sakai R, Higashi K, Ohta M, Sugimoto Y, Ikoma Y, Horiguchi Y. Creeping hair: an isolated hair burrowing in the uppermost dermis resembling larva migrans. Dermatology. 2006;213(3):242–244. doi:10.1159/000095045
- Liu JH, Zhao YK, Wu HH, Wang F, Luo DQ, Huang YB. Intradermal growing hair: two case reports. Am J Mens Health. 2019;13(1):1557988319825774. doi:10.1177/1557988319825774
- Liu X, Yao ZY. Cutaneous pili migrans: a case confirmed by dermoscopy and reflectance confocal microscopy. Indian J Dermatol Venereol Leprol. 2021;87(2):244–246. doi:10.25259/ijdvl_199_19
- Panchaprateep R, Tanus A, Tosti A. Clinical, dermoscopic, and histopathologic features of body hair disorders. J Am Acad Dermatol. 2015;72(5):890–900. doi:10.1016/j.jaad.2015.01.024
- Franbourg A, Hallegot P, Baltenneck F, Toutain C, Leroy F. Current research on ethnic hair. J Am Acad Dermatol. 2003;48(6 Suppl):S115–S119. doi:10.1067/mjd.2003.277