
Abstract
Port-wine stains are a type of capillary malformation affecting 0.3% to 0.5% of the population. Port-wine stains present at birth as pink to erythematous patches on the skin and/or mucosa. Without treatment, the patches typically darken with age and may eventually develop nodular thickening or associated pyogenic granuloma. Laser and light treatments provide improvement through selective destruction of vasculature. A variety of vascular-selective lasers may be employed, with the pulsed dye laser being the most common and well studied. Early treatment produces more optimal results. Advances in imaging and laser treatment technologies demonstrate potential to further improve clinical outcomes.
Introduction
Capillary malformations (CMs), also called port-wine stains, appear as congenital pink to erythematous patches affecting 0.3%–0.5% of the population.Citation1 There is no sex predilection, and the inheritance pattern is generally sporadic. The most common locations are the head and neck, particularly the V1 and V2 dermatomes. The trunk and extremities are also frequently affected. The color change results from an increased hemoglobin content in the skin, due to dilated capillaries and postcapillary venules in the affected regions.Citation1 A somatic activating mutation in the GNAQ gene (c.548G → A, p.R183Q), encoding the guanine nucleotide binding protein G-alpha-q subunit, has been discovered in port-wine stain lesions.Citation2 This appears to produce activation of extracellular signal-regulated kinase (ERK), c-Jun N-terminal kinase, and P70 ribosomal S6 kinase.Citation3 Dysregulation of angiogenic signaling has been observed to underlie CM pathology.Citation4 Unlike vascular tumors, CMs do not exhibit proliferation, but rather demonstrate chronic progressive vascular dilatation over the course of years.
Laser treatment of CMs reduces the likelihood and severity of unwanted associated effects, including cutaneous hypertrophy, disfigurement of the normal tissue architecture (), development of associated pyogenic granuloma, and psychosocial morbidity.Citation5 When treatment is sought, vascular-selective lasers represent the treatment of choice (). Using the principle of selective photothermolysis, the affected cutaneous blood vessels can be destroyed with effective and durable results while protecting the remainder of the skin.Citation6 In this article, we review the diagnosis and medical evaluation of port-wine stains and discuss both classic and recent research findings relating to lasers and lights in producing optimal treatment outcomes.
Figure 1 An untreated facial capillary malformation (port-wine stain) in a 60-year-old man who presented with a complaint of progressive darkening and development of nodularity in his adult years.

Table 1 Vascular-selective lasers for treatment of CMs (also called port-wine stains)
Medical evaluation of CMs
CMs are diagnosed clinically by physical examination revealing a pink to erythematous patch or series of patches along with a confirmatory history of presence at birth and possible gradual darkening and thickening over the course of many years. Pink patches presenting in a neonate must be observed for signs of growth during infancy, which may suggest an alternative diagnosis of infantile hemangioma rather than CM.Citation7
Medical evaluation of CMs includes screening for glaucoma when the V1 distribution of the facial nerve is affected, as up to 10% of patients may have the condition.Citation8 Additionally, when the V1 dermatome is affected, screening for Sturge–Weber syndrome is warranted. Sturge–Weber syndrome risk is 7%–28% in reported studies of children with V1 CMs.Citation9 Magnetic resonance imaging is a preferred screening modality.Citation9 Sturge–Weber syndrome consists of a constellation of findings including facial CM, vascular involvement of the leptomeninges, possible glaucoma of the ipsilateral eye, and possible seizures or mental retardation.Citation2 The diagnosis may be made by imaging showing classic tram-like calcifications in the brain, which may not appear until later infancy.
CMs associated with significant tissue hypertrophy or with bony hypertrophy may have increased vascular flow (Klippel–Trenaunay syndrome).Citation10 An associated arteriovenous malformation may further be present (Klippel– Trenaunay–Weber syndrome). Patients with a CM located in a midline lumbar location should also be screened for an underlying arteriovenous malformation as seen in Cobb syndrome.Citation11
Visual examination of CM thickness and of patient skin type aids in preoperative assessment for laser treatment. Modern imaging technologies including optimal coherence tomography can aid in assessment of target vessel depth and diameters.Citation12 Three-dimensional photography and reflectance spectrophotometry can provide objective quantification of pre- and post-procedure volume and color, respectively.Citation13,Citation14 In pediatric patients, an assessment of the child’s ability to tolerate laser treatment in the office using topical anesthesia as needed and staff assistance, or the need for general anesthesia, is also important for preoperative preparation and planning.
Treatment principles
Laser treatment of CMs is based on selective photothermolysis of the affected vessels. Selective photothermolysis is the process by which a pigmented target absorbs photons, becoming heated and ultimately destroyed, while surrounding structures are relatively spared.Citation6 In the case of CM, the desired targets are 10–500 μm dilated capillaries and postcapillary venules in the papillary and reticular dermis.Citation12 The endothelium is indirectly destroyed through targeting of the chromophore in its interior, hemoglobin. Hemoglobin absorbs light strongly at 400–600 nm and displays reduced absorption at 700–1,100 nm. Vascular-selective laser wavelengths are absorbed by hemoglobin, producing heat, photocoagulation and aggregation of erythrocytes, and, ultimately, necrosis of the endothelial cells.Citation15 The vessel may rupture, producing purpura.Citation16 In order to limit damage to surrounding structures, the pulse duration should be set at less than or equal to the target vessels’ thermal relaxation time (TRT; for CM vessels, TRT is estimated at 0.45–10 ms).Citation6,Citation17
After laser treatment produces thermolysis of the vessel walls, a neutrophilic and lymphocytic infiltrate with vasculitis-like karyorrhexis appears by 24 hours. Vascular remodeling occurs during the healing process, with a resulting reduction in the number and size of CM vessels.Citation18,Citation19 Vessels that are not sufficiently damaged may recover. Antiangiogenic agents such as topical rapamycin applied after laser treatment have been shown to reduce angiogenic signals and have shown potential to improve clinical outcomes.Citation20
Laser treatment should be initiated early in infancy, if possible, when better outcomes are produced.Citation21 The young dermis allows for more optimal targeting of vessels, as dermal thickness and scatter increase with age. The goal clinical endpoint during laser therapy is a transient gray to blue discoloration of the skin that evolves into purpura. Laser treatment is generally continued every 2 to 4 weeks until a plateau is reached, so that further improvement is not seen.Citation7 The majority of patients will have more than 50% lightening of their CMs.Citation7 Suboptimal response remains a significant obstacle observed in 20%–46% of patients, and 14%–40% have been reported to show minimal to no response, for diverse reasons.Citation22 Multiple treatments are the norm, and most patients require eight to ten treatments or more for optimal results.Citation7 Some anatomic sites respond more than others, with distal or acral and centrofacial sites showing less response.Citation23 In addition, smaller CMs generally show more complete clearance than large CMs.Citation24
Laser types and treatment
The pulsed dye laser (PDL) represents the most commonly used laser for treatment of CMs and has the most published literature supporting its use. First-generation PDLs introduced in the 1980s produced light at 577 nm, while modern-generation PDLs produce 595–600 nm light that has a greater depth of penetration.Citation22 There is absorption by oxyhemoglobin and deoxyhemoglobin, as well as by melanin. Common initial fluences are 8–9 J/cmCitation2 with increases until the clinical endpoint is reached. Pulse durations can be varied from 0.45 to 40 ms and spot sizes also come in wide variations, from 2 to 12 mm, with circular and elliptical shape options. Cryogen spray cooling provides epidermal protection and has aided in the excellent safety record in the published literature.Citation25 Studies show 50%–90% overall clearance, with approximately 10% improvement per treatment session ().Citation26 Improved fading is visualized when treatment is begun at an earlier age.Citation7,Citation21 Pigmentary changes have been reported at rates of 1.4%, atrophic scarring at 4.3%, and hypertrophic scarring at 0.7%, generally in appropriately selected patients.Citation7 PDL has been utilized with an excellent safety profile in skin phototypes I–III. In a study of 75 subjects of skin phototypes IV and V, PDL demonstrated improvement in CMs with frequent transient hyperpigmentation (30%, typically lasting 6–8 weeks) and two cases of scarring that were felt to be related to pulse stacking.Citation27 Very small and deep vessels are less likely to respond to PDL treatment.Citation28 While PDL represents the standard initial laser treatment for CMs, a reported 20%–30% of CMs show resistance.Citation28 Resistant or deep CMs are sometimes treated with alternative lasers in an effort to enhance clearance.
Figure 2 An adult woman with a previously untreated capillary malformation at the left temple that had developed darkening and nodularity.

Frequency-doubled neodymium-doped yttrium aluminum garnet (Nd:YAG) and potassium titanyl phosphate lasers produce 532 nm green light.Citation29 Because of absorption by melanin, use is primarily in skin phototypes I–III and, sometimes, skin phototype IV.Citation29 With a limited penetration depth due to the shorter wavelength, these lasers have been primarily successful in treating superficial vascular lesions including some CMs;Citation29 532 nm lasers have demonstrated improvement when treating both previously untreated and treatment-resistant CMs ().Citation30 A prospective study confirmed up to 75% improvement in color and histologic destruction of vessels in flat, nonhypertrophic CMs using a frequency-doubled 532 nm laser.Citation18 In a study of 30 treatment-resistant CMs treated with one to four sessions of 532 nm laser, 53% showed greater than 25% improvement and 17% showed more than 50% improvement.Citation31 Pençe et al studied 89 patients with CMs who were treated with 532 nm frequency-doubled Nd:YAG laser and found 13% to have an excellent response, 38% a good response, 44% a moderate response, and 5% mild improvement.Citation32 Some studies report slightly reduced efficacy per session when compared with PDL and an increased rate of side effects, including crusting.Citation33
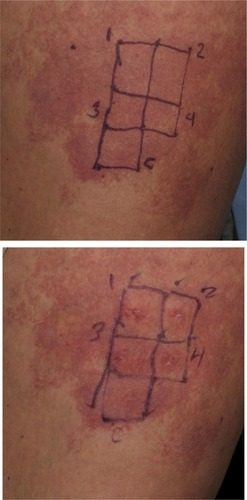
Figure 3 A previously untreated capillary malformation (port-wine stain) at the right thigh.
Alexandrite lasers fall in the near-infrared category, having a 755 nm wavelength. With a 50%–75% increased depth of penetration, near-infrared laser use for CMs is primarily for dark or resistant lesions.Citation34 A retrospective study of 20 patients with either hypertrophic or PDL-resistant CMs treated with alexandrite laser alone or in combination with other lasers such as PDL showed most had a moderate response, while some had mild or no response.Citation35 Diode lasers (800–940 nm) may similarly be used to treat CMs, though they are more often used for venous lakes or for endovenous ablation.Citation36,Citation37
Nd:YAG lasers have the highest depth of penetration of the vascular-selective lasers and the lowest epidermal melanin absorption. Because higher fluences are generally required, rates of pigmentary change and scarring are higher than with PDL in published studies (0%–4.3%).Citation38 Epidermal cooling is typically by cryogen spray cooling and provides an important measure of protection. Nd:YAG lasers are typically reserved for CMs in patients with skin phototypes V–VI or for hypertrophied or resistant CMs. In addition, they have shown efficacy in treating vascular blebs associated with CM.Citation39 In a retrospective study of 130 CM patients treated with long-pulsed 1,064 nm Nd:YAG laser, 2%, 15%, 64%, and 19% of patients experienced <25%, 25%–49%, 50%–75%, and >75% lesion clearance, respectively.Citation40 Darker CMs showed more response than lighter CMs.Citation40 Nd:YAG laser treatment at 1,064 nm has also been demonstrated to improve hypertrophy, with good-to-excellent improvements seen in the majority of the 32 studied patients. Adverse effects were more frequent, however, with hypopigmentation seen in 14 and scars in seven of the 32 subjects.Citation41
Argon lasers were the earliest common vascular laser, used frequently in the 1970s and 1980s.Citation42 However, they have fallen out of use with the development of more modern and safe laser systems. Argon laser light is blue-green with a 488–514 nm wavelength. Oxyhemoglobin absorbs well at this range.Citation42 A small spot size limits the depth of penetration to 1–2 mm and is inconvenient for treatment. There is a high rate of hypertrophic scarring due to the continuous wave or quasi-continuous wave nature, and reports of 20% or more risk of hyper- or hypopigmentation, due to competitive absorption by epidermal melanin.Citation42
Copper vapor and copper bromide lasers produce yellow 578 nm light. Krypton lasers produce green, quasi-continuous 520–530 nm light or yellow 568 nm light. The copper and krypton lasers are also early-generation vascular lasers that are largely unused due to similar complications of quasi-continuous laser exposure and absorption by melanin.Citation43
Intense pulsed light does not meet the definition of a laser and instead produces non-coherent, broadband light between 390 and 1,200 nm using a xenon flashlamp.Citation44 A low fluence output is produced. When laser treatment is not available or when non-purpuric treatment with limited side effects is desired, and with the understanding that there is typically significantly reduced efficacy in comparison to laser treatment, intense pulsed light may be considered as an alternative treatment method. Cutoff filters are available to modulate the wavelength range applied.Citation7 Spot sizes vary from 8×15 mm to 15×35 mm and can be further modified using opaque white paper. Typical settings may include a 550 nm filter, 50–75 J/cmCitation2 fluence, and 40–60 ms pulse delay. Despite the low fluence, significant pigmentary changes and adverse effects can occur, and similar cautions must be applied as with laser treatment.Citation7
Photodynamic therapy (PDT) represents an alternative and advancing treatment option for port-wine stains.Citation22 A chemical photosensitizer is introduced, typically via intravenous injection, and the affected area is irradiated with light of a wavelength absorbed by the photosensitizer. In the presence of oxygen, free radical damage results, with subsequent destruction of endothelial cells.Citation22 One significant drawback is the side effect of generalized photosensitivity requiring photoprotection for days to weeks, depending on the half-life of the photosensitizer used.Citation45 PDT treatment has been used alone or has been combined with other laser and light therapies in small studies.Citation46 In general, studies have suggested an equivalent or possibly superior efficacy when compared to the standard PDL treatment.Citation22 Indocyanine green photosensitizer activated by diode laser demonstrated efficacy in a study of 15 patients as an alternative to PDL.Citation46 PDT treatment using hemoporfin and copper laser was recently studied in children 3 to 10 years of age and showed a higher rate of excellent response than the traditional PDL treatment (25% versus 11%).Citation47 A more significant difference was seen in violaceous lesions than in those that were erythematous.Citation47 PDT treatment of port-wine stains represents an emerging arena, and investigators continue to explore optimization of treatment protocols.Citation48
Side effects and potential complications
The most common side effects of laser treatment of CMs are redness, swelling, and bruising. Erythema (redness) and swelling persist for hours, and sometimes up to days or weeks. CMs are usually treated at settings which induce purpura (bruising) for more effective results. Purpura typically fades over 1–2 weeks. Blistering and crusting can also develop, more commonly after overlapping or double pulses. Crusted or blistered areas should be treated gently with liberal petroleum jelly and moist bandaging until healed.
More permanent effects can occur as well. Alopecia can occur when using lasers that also target melanin in areas that have pigmented hairs. Hyperpigmentation and hypopigmentation can occur from damage to melanosomes and/or due to postinflammatory changes. Selection of the appropriate laser wavelength matched to the patient skin type, use of epidermal cooling, more conservative fluences and pulse durations, and test spots, along with photoprotection before and after treatments, reduce the incidence of pigmentary changes. Scarring is uncommon, but must be carefully guarded against. Special attention should be paid to any areas of erosions, blisters, or necrotic skin that can develop into scars.
Ocular risks, which include corneal burns or retinal pigment loss resulting in blindness, are rare when diligent safety procedures are practiced. Appropriate eye protection includes the routine use of external eye shields. Nd:YAG and other deep-penetrating lasers may induce retinal damage in the periorbital area and are utilized most safely outside of the orbital rim.Citation49 When lasers are used inside of the orbital rim, intraocular eye protection is paramount.Citation49
Flammability is also a risk with the use of lasers.Citation50 Water-based lubricants protect hairs from being singed. When treating patients under anesthesia or requiring supplemental oxygen, use of a laryngeal mask airway with clear tubing and wet draping is preferred to reduce the risk of ignition.Citation50
Conclusion and future directions
Modern laser treatments, at wavelengths and settings matched well to individual patient and lesional characteristics, are able to produce significant diminution of CMs. Improvements of 80%–90% are frequently seen with early and optimal treatment. Adjuvant and novel treatments have been briefly explored in the literature and are likely to expand in coming years. The use of antiangiogenic drugs, photodynamic therapy, and other methods of targeting dilated capillaries and of limiting revascularization after laser treatment are likely to produce further improvements. Enhancements in laser technology and epidermal protection methods will also allow more complete results to be obtained while reducing risks of pigmentary changes or scarring. Importantly, an improved understanding of the molecular, genetic, and cellular changes causing this localized capillary and venular dilatation may provide a permanent cure or preventive solution.
Disclosure
Drs Reddy and Brightman have served as investigators for Syneron/Candela, Cutera, and Cynosure. Dr Brightman serves on the medical advisory board of Cynosure and has received honoraria from Syneron/Candela. Dr Geronemus has served on the medical advisory boards for Zeltiq, Syneron/Candela, and Cynosure; as an investigator for Syneron/Candela, Cynosure, Cutera, Medicis, Allergan, Dusa, Myoscience, MoMelan, Lithera, Kythera, Miramar, Pfizer, and Cytrellis; and has been a stockholder of Zeltiq and OnLight Sciences. The authors report no other conflicts of interest in this work.
References
- CordoroKMSpeetzenLSKoerperMAFriedenIJPhysiologic changes in vascular birthmarks during early infancy: mechanisms and clinical implicationsJ Am Acad Dermatol200960466967519167781
- ShirleyMDTangHGallioneCJSturge-Weber syndrome and port-wine stains caused by somatic mutation in GNAQN Engl J Med2013368211971197923656586
- TanWChernovaMGaoLSustained activation of c-Jun N-terminal and extracellular signal-regulated kinases in port-wine stain blood vesselsJ Am Acad Dermatol20147196496825135651
- LaquerVTHeveziPAAlbrechtHChenTSZlotnikAKellyKMMicroarray analysis of port wine stains before and after pulsed dye laser treatmentLasers Surg Med2013452677523440713
- GeronemusRGAshinoffRThe medical necessity of evaluation and treatment of port-wine stainsJ Dermatol Surg Oncol199117176791991884
- AndersonRRParrishJASelective photothermolysis: precise microsurgery by selective absorption of pulsed radiationScience198322045965245276836297
- AstnerSAndersonRRTreating vascular lesionsDermatol Ther200518326728116229727
- IwachAGHoskinsHDJrHetheringtonJJrShafferRNAnalysis of surgical and medical management of glaucoma in Sturge-Weber syndromeOphthalmology19909779049092381705
- MelanconJMDohilMAEichenfieldLFFacial port-wine stain: when to worry?Pediatr Dermatol201229113113322256997
- StierMFGlickSAHirschRJLaser treatment of pediatric vascular lesions: port wine stains and hemangiomasJ Am Acad Dermatol200858226128518068263
- JessenRTThompsonSSmithEBCobb syndromeArch Dermatol19771131115871590931402
- LiuGJiaWNelsonJSChenZIn vivo, high-resolution, three-dimensional imaging of port wine stain microvasculature in human skinLasers Surg Med2013451062863224155140
- FrigerioABhamaPKTanOTQuantitative three-dimensional assessment of port-wine stain clearance after laser treatmentsLasers Surg Med2013451063363824339253
- HalachmiSAzariaRInbarRAd-ElDLapidothMUse of reflectance spectrophotometry to predict the response of port wine stains to pulsed dye laserLasers Med Sci201429122523023609559
- HegerMBeekJFMoldovanNIvan der HorstCMvan GemertMJTowards optimization of selective photothermolysis: prothrombotic pharmaceutical agents as potential adjuvants in laser treatment of port wine stains. A theoretical studyThromb Haemost200593224225615711739
- SuthamjariyaKFarinelliWAKohWAndersonRRMechanisms of microvascular response to laser pulsesJ Invest Dermatol2004122251852515009739
- ShafirsteinGBäumlerWLapidothMFergusonSNorthPEWanerMA new mathematical approach to the diffusion approximation theory for selective photothermolysis modeling and its implication in laser treatment of port-wine stainsLasers Surg Med200434433534715083495
- ReddyKKBrauerJAIdrissMHTreatment of port-wine stains with a short pulse width 532-nm Nd:YAG laserJ Drugs Dermatol2013121667123377330
- JiaWSunVTranNLong-term blood vessel removal with combined laser and topical rapamycin antiangiogenic therapy: implications for effective port wine stain treatmentLasers Surg Med201042210511220166161
- GaoLPhanSNadoraDMTopical rapamycin systematically suppresses the early stages of pulsed dye laser-induced angiogenesis pathwaysLasers Surg Med201446967968825270513
- AshinoffRGeronemusRGFlashlamp-pumped pulsed dye laser for port-wine stains in infancy: earlier versus later treatmentJ Am Acad Dermatol19912434674722061448
- ChenJKGhasriPAguilarGAn overview of clinical and experimental treatment modalities for port wine stainsJ Am Acad Dermatol201267228930422305042
- LaniganSWPort wine stains on the lower limb: response to pulsed dye laser therapyClin Exp Dermatol199621288928759191
- YohnJJHuffJCAelingJLWalshPMorelliJGLesion size is a factor for determining the rate of port-wine stain clearing following pulsed dye laser treatment in adultsCutis19975952672709169268
- SeukeranDCCollinsPSheehan-DareRAAdverse reactions following pulsed tunable dye laser treatment of port wine stains in 701 patientsBr J Dermatol199713657257299205506
- KosterPHvan der HorstCMBossuytPMvan GemertMJPrediction of portwine stain clearance and required number of flashlamp pumped pulsed dye laser treatmentsLasers Surg Med200129215115511553903
- ThajudheenCPJyothyKPriyadarshiniATreatment of port-wine stains with flash lamp pumped pulsed dye laser on Indian skin: a six year studyJ Cutan Aesthet Surg201471323624761097
- SavasJALedonJAFrancaKChaconANouriKPulsed dye laser-resistant port-wine stains: mechanisms of resistance and implications for treatmentBr J Dermatol2013168594195323290045
- BecherGLCameronHMoseleyHTreatment of superficial vascular lesions with the KTP 532-nm laser: experience with 647 patientsLasers Med Sci201429126727124401943
- WooWKJasimZFHandleyJMEvaluating the efficacy of treatment of resistant port-wine stains with variable-pulse 595-nm pulsed dye and 532-nm Nd:YAG lasersDermatol Surg2004302 Pt 1158162 discussion 16214756643
- ChowdhuryMMHarrisSLaniganSWPotassium titanyl phosphate laser treatment of resistant port-wine stainsBr J Dermatol2001144481481711298542
- PençeBAybeyBErgenekonGOutcomes of 532 nm frequency-doubled Nd:YAG laser use in the treatment of port-wine stainsDermatol Surg200531550951715962732
- LandthalerMHohenleutnerULaser therapy of vascular lesionsPhotodermatol Photoimmunol Photomed200622632433217100741
- IziksonLAndersonRRTreatment endpoints for resistant port wine stains with a 755 nm laserJ Cosmet Laser Ther2009111525519012069
- IziksonLNelsonJSAndersonRRTreatment of hypertrophic and resistant port wine stains with a 755 nm laser: a case series of 20 patientsLasers Surg Med200941642743219588532
- WallTLGrassiAMAvramMMClearance of multiple venous lakes with an 800-nm diode laser: a novel approachDermatol Surg200733110010317214688
- Van Den BosRRNeumannMDe RoosKPNijstenTEndovenous laser ablation-induced complications: review of the literature and new casesDermatol Surg20093581206121419469796
- McGillDJMacLarenWMackayIRA direct comparison of pulsed dye, alexandrite, KTP and Nd:YAG lasers and IPL in patients with previously treated capillary malformationsLasers Surg Med200840639039818649379
- BrauerJAGeronemusRGSingle-treatment resolution of vascular blebs within port wine stains using a novel 1,064-nm neodymium-doped yttrium aluminum garnet laserDermatol Surg20133971113111523560945
- ZhongSXLiuYYYaoLClinical analysis of port-wine stain in 130 Chinese patients treated by long-pulsed 1064-nm Nd: YAG laserJ Cosmet Laser Ther201416627928325060356
- van DroogeAMBosveldBvan der VeenJPde RieMAWolkerstorferALong-pulsed 1064 nm Nd:YAG laser improves hypertrophic port-wine stainsJ Eur Acad Dermatol Venereol201327111381138623094931
- GeronemusRGArgon laser for the treatment of cutaneous lesionsClin Dermatol199513155587704856
- NouriKAlsterTChoudharySFalto-AizpuruaLABallardCJVejjabhinantaVLaser Treatment of Acquired and Congenital Vascular Lesions [webpage on the Internet]New York, NYMedscape [updated October 9, 2013]. Available from: http://emedicine.medscape.com/article/1120509-overviewAccessed October 1, 2014
- PiccoloDDi MarcantonioDCrismanGUnconventional use of intense pulsed lightBiomed Res Int2014201461820625276803
- KimelSSvaasandLOKellyKMNelsonJSSynergistic photodynamic and photothermal treatment of port-wine stain?Lasers Surg Med2004342808215004815
- KleinABäumlerWBuschmannMLandthalerMBabilasPA randomized controlled trial to optimize indocyanine green-augmented diode laser therapy of capillary malformationsLasers Surg Med210345421622423619901
- ZhangBZhangTHHuangZLiQYuanKHHuZQComparison of pulsed dye laser (PDL) and photodynamic therapy (PDT) for treatment of facial port-wine stain (PWS) birthmarks in pediatric patientsPhotodiagnosis Photodyn Ther Epub6252014
- WangYZuoZLiaoXGuYQiuHZengJInvestigation of photodynamic therapy optimization for port wine stain using modulation of photosensitizer administration methodsExp Biol Med (Maywood)2013238121344134924157585
- HammesSAugustinARaulinCOckenfelsHMFischerEPupil damage after periorbital laser treatment of a port-wine stainArch Dermatol2007143339239417372105
- WaldorfHAKauvarNBGeronemusRGLeffelDJRemote fire with the pulsed dye laser: risk and preventionJ Am Acad Dermatol19963435035068609266