Abstract
Background
Epidemiologic information regarding the prevalence of “fragile skin” in different adult populations is currently limited. The objective of the current survey was to assess the occurrence of perceived “fragile skin” across different skin types in the general adult population.
Methods
Individuals aged 15–65 years from five representative geographic regions (France, Spain, Sweden, Japan, and the US) were interviewed and grouped into the following skin types: Caucasian North skin (n=1,218), Caucasian South skin (n=1,695), Asian skin (n=1,500), and Black skin (n=500). The main survey question was “In your opinion, do you have fragile skin?” Concepts relating to the nature and appearance of an individual’s skin were also evaluated.
Results
A total of 4,913 individuals were interviewed. Subjects in the Caucasian North, Caucasian South, Asian, and Black skin type groups responded positively to the question “In your opinion, do you have fragile skin?” in the following proportions: 24.44%, 29.71%, 52.67%, and 42.20%, respectively. With the exception of individuals in the Black skin group, “fragile skin” was prevalent in significantly more women than men (P<0.0001). Compared with other age categories, the prevalence of “fragile skin” was significantly higher in individuals aged 15–34 years (P<0.0001), regardless of skin type. In general, individuals reporting “fragile skin” were 2–3-fold more likely to respond positively to a series of questions relating to the nature and appearance of their skin. The prevalence of “fragile skin” was also higher in individuals who experienced dermatosis (skin lesions of any type) in the previous 12 months.
Conclusion
Whilst these findings need to be confirmed through objective evaluation, the current survey demonstrated that “fragile skin” is perceived to occur in a substantial proportion of individuals from any given country, particularly in the age range of 15–34 years, regardless of skin type.
Introduction
The skin is the largest organ of the body, providing a protective barrier against bacteria, chemicals, and physical insults while maintaining homeostasis in the internal environment.Citation1,Citation2 Such a barrier function encompasses protection against excessive water loss and limitation of the deleterious influences of sunlight. The skin’s immune defense consists of several facets, including immediate, nonspecific mechanisms (innate immunity), and delayed, stimulus-specific responses (adaptive immunity), which contribute to fending off a wide range of potentially invasive microorganisms. Injury or weakening of the skin barrier can result in local and systemic infection, increased morbidity, negative psychosocial implications associated with skin disorders, and increased cost of care, eg, in neonates and the elderly.Citation3
The main epidermal permeability barrier is localized to the uppermost epidermal layer, ie, the stratum corneum; however, a second line of protection is provided by the sealing effect of tight junctions situated in the granular layer.Citation4–Citation6 Often referred to as the “rivets” of the stratum corneum, corneodesmosomes serve to anchor the corneocytes at the skin surface and are mostly composed of three major specialized proteins (desmoglein-1, desmocollin-1, and corneodesmosin).Citation7 The primary function of corneodesmosomes is to maintain a cohesive force between adjacent corneocytes until the junctions are degraded by proteolytic enzymes involved in physiologic desquamation.Citation8,Citation9 Intercellular lipids, structured in several bilayers, constitute the extracellular matrix of the stratum corneum and are responsible for the regulation of tissue permeability.Citation10 Changes in lipid composition and epidermal differentiation lead to disturbances in the skin barrier,Citation11 allowing the entry of environmental allergens, immunological reaction, and inflammation. Indeed, a disturbed skin barrier is an important component in the pathogenesis of contact dermatitis, ichthyosis, psoriasis, and atopic dermatitis.Citation12–Citation15
The concept of “fragile skin” is a subjective (experienced) and objective (clinically evaluated) perception of the skin’s condition that is based on constitutional factors relating to the structure and function of the epidermal barrier.
Despite extensive research on the physiologic and pathologic mechanisms leading to skin barrier dysfunction, which may result in perceived skin fragility, there is limited epidemiologic information regarding the prevalence of “fragile skin” in different adult populations. Such a subjective perception of “having fragile skin” should be clearly differentiated from “skin fragility”, a well documented disorder, occurring mostly in newborn infants and elderly individuals, leading to skin tears of mechanical origin.Citation16–Citation19
All kinds of “fragile skin” are characterized by a lower constitutional resistance threshold to minor environmental aggression and, consequently, require appropriate management, including the use of skin care products that allow the skin to strengthen its natural protective qualities. Skin that is temporarily weakened by major environmental aggression, local or systemic treatments, or by skin disease, can also benefit from skin care products designed for “fragile skin”.
The purpose of the current survey was to assess the prevalence of perceived “fragile skin” across different skin types in the general adult population.
Patients and methods
Data collection
The survey was conducted by the CSA Health Institute, Puteaux, France, on samples of recruited individuals that were representative of the French, Spanish, Swedish, and Japanese populations. A representative sample of individuals with Black skin was also formed in the US. All recruited individuals were aged ≥15 years. The objective of the survey was to interview a total of 5,000 subjects. Since this study was designed as a survey and did not include manipulation of the subject or the subject’s environment, submission to the institutional review board was waived.
Participants were interviewed by telephone between June 2012 and May 2013, and selected according to the national quota method (sex, age, occupation of head of family, geographic density, and region). In order to reduce potential errors and assessor bias, interviews were double-checked by follow-up calls to 20% of the interviewees, and if this procedure revealed any abnormal finding in even a single questionnaire, all interviews conducted by the interviewer concerned were reassessed. No abnormal findings were observed.
Depending on skin type and the geographic location of the individual, the following four “skin type” groups were formed:
Caucasian North skin (Swedish subjects and French subjects living in northern France)
Caucasian South skin (Spanish subjects and French subjects living in southern France)
Asian skin (Japanese subjects)
Black skin (US subjects)
Participants responded to questions about “fragile skin”, with the main question being “In your opinion, do you have fragile skin?”. In addition, the survey covered a series of other questions, relating to the concepts of “transparent”, “translucent”, “thin”, and “fine textured” skin, and skin with a “velvety” appearance. To determine the presence of eczema or acne, participants answered the survey questions “Do you currently have eczema?” and “Do you currently have acne?”. Participants were also asked to respond to the question “In your childhood, have you suffered from atopic dermatitis?”. Medical history and socioeconomic data were also recorded.
Statistical analysis
Qualitative variables were compared using the χ2 test, or Fisher’s exact test if conditions for application were not met. Statistical analyses were performed using SAS software (version 8.2; SAS Institute, Cary, NC, USA).
Results
A total of 4,913 individuals from the five geographic regions were interviewed and grouped into the following skin types: Caucasian North (n=1,218), Caucasian South (n=1,695), Asian (n=1,500), and Black (n=500). The overall survey response rate was 100% (any subject that did not answer the questions was replaced by an identical individual in terms of the quota method [sex, age, occupation of head of family, geographic density and region]).
shows demographic data for all included individuals. With the exception of the Caucasian North group, numerically more females than males were included in each group. Groups were evenly balanced with regard to age range categories, although there were numerically more younger individuals, aged 15–34 years, in the Black skin group, and a slightly higher proportion of individuals aged 35–54 years in the Caucasian South group. The reported prevalence of acne and eczema was consistent with data reported in the literature.Citation20,Citation21 The prevalence of both diseases was highest in the group of Northern Americans with Black skin (). The breakdown of acne and eczema by age and sex is presented in .
Table 1 Demographic characteristics of individuals included in the “fragile skin” survey
Table 2 Prevalence of acne and eczema by sex and age group
In response to the question “In your opinion, do you have fragile skin?”, 24.44%, 29.71%, 52.67%, and 42.20% of subjects in the Caucasian North, Caucasian South, Asian, and Black skin type groups, respectively, responded positively. Of the subjects responding positively, most were females; at least one in three women consistently provided a positive response (). With the exception of the Black skin group, this sex-related difference in self-assessment was statistically significant in all skin type groups (P<0.0001). Analysis of positive responses by age category showed that the perception of “fragile skin” was significantly (P<0.0001) higher in individuals aged 15–34 years, regardless of skin type ().
Table 3 Proportion of patients responding positively to the question “In your opinion, do you have fragile skin?”
As shown in , with the exception of the Asian skin type group, individuals reporting “fragile skin” were 2–3 times more likely to respond positively to a series of questions relating to the nature and appearance of their skin. Individuals in the Black skin group who reported “fragile skin” were seven times more likely to respond positively to the question “In your opinion, do you have thin skin?” than individuals in the same group who did not report “fragile skin” ().
Table 4 Proportion of patients with/without “fragile” skin responding to questions relating to appearance of their skin
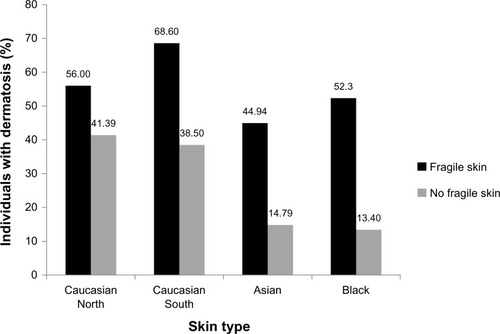
Regardless of skin type, among patients with perceived “fragile skin” there was a consistently larger number of individuals who reported having experienced a skin disease in the last 12 months; in fact, 56%, 68.6%, 44.9%, and 52.1% of individuals in the Caucasian North (P=0.007), Caucasian South (P<0.001), Asian (P<0.001), and Black (P<0.001) skin type groups declaring “fragile” skin, respectively, also claimed to have experienced dermatitis in the last 12 months ().
Figure 1 Proportion of individuals with skin disease in the last 12 months who reported having “fragile skin”.
Discussion
Although the concept of “sensitive skin” is often addressed by dermatologists,Citation22 the current survey evaluated the perception of “fragile skin” among representative populations of adults with different skin types. In this context, it is important to differentiate between the distinct concepts of “fragile” and “sensitive” skin. Sensitive skin is generally defined as skin (often facial) that has a reduced tolerance to cosmetics and toiletries.Citation23 One of its characteristics is improper protection of the epidermal nerve endings and the resulting sensation of itching, with a tendency toward blushing. Our survey participants were not given precise clues permitting them to distinguish between the two concepts and no particular skin territory of interest was suggested. Conducted in nearly 5,000 individuals, our study provides a series of previously unprecedented responses in terms of the subjective perception of “fragile skin” and the notions of thin, translucent, and transparent skin, and skin with a velvety appearance.
Nevertheless, there may well be some common underlying etiologic factors between sensitive and fragile skin among individuals with different skin types.Citation24 For example, baseline transepidermal water loss, a functional descriptor of the permeability barrier, has been shown to be elevated in subjects with sensitive skin and higher in people with Black skin than in Caucasians and Asians.Citation25 This observation could explain the higher proportion of individuals in our Black skin group with perceived “fragile skin” who responded positively to questions relating to the thinness, fine texture, and velvety appearance of their skin. Large, well designed studies are warranted in order to establish objective evaluation criteria and to explore the findings of the present survey in greater depth.
The current study also provides a different perspective regarding the age-related prevalence of “fragile skin”. We focused on different groups of adults, deliberately dismissing very young and elderly subjects. Indeed, at full-term gestation, the barrier function of newborn skin is not fully mature and, although the skin is structurally similar to that of adults, the thickness of the epidermal and dermal layers is ≤60% compared with that of adult skin.Citation26–Citation28 Thereafter, skin maturation continues until adult age and seamlessly evolves towards ageing.Citation29 At the other end of the age spectrum, the breakdown of dermal tissue, flattening of the dermal-epidermal junction, epidermal thinning, and xerosis contribute to an increased risk of skin tears and to itchy conditions in elderly individuals.Citation30,Citation31
Interestingly, our survey shows that, amongst the age categories evaluated in the general adult population, the prevalence of “fragile skin” was consistently and significantly higher in individuals aged 15–34 years. Indeed, although the proportions differed between the different skin type groups, the higher prevalence of “fragile skin” in the age category of 15–34 years occurred regardless of skin type. The reason for this observation is not clear, although one can speculate that it could possibly relate to hormonal changes in the age category of 15–34 years linked to a perception of fragile skin. Psychologic factors reflecting societal evolution and tendency towards narcissism and depression in the so-called “generation me” also cannot be excluded.Citation32 Psychologic stress alters epidermal barrier function and may contribute to the picture of “fragile skin”.Citation33,Citation34 An interesting clue is provided by the fact that subjects having experienced dermatosis during the year preceding the survey were more prone to describe their skin as “fragile” when compared with those who had no history of skin disorders. The prevalence of acne vulgaris is highest during adolescence, resulting from changes in the body’s hormonal milieu.Citation35 Although occurrence of acne decreases with age, it often continues into early adulthood, and current evidence suggests that the prevalence of post-adolescent acne in women is increasing.Citation36 However, whilst the overall prevalence of acne (and eczema) across the geographic skin type groups in the current survey was in concordance with previous literature,Citation20,Citation21 age category-specific analyses of potential systemic changes that may explain the higher prevalence of fragile skin in the age category of 15–34 years were not conducted. Indeed, a number of systemic diseases or physiologic changes may affect the maintenance of homeostasis of the skin barrier;Citation37 further studies are warranted to explore our findings in an objective manner.
Various differences were noted between the skin type groups in responses to questions about “fragile skin” and some of these differences may reflect limitations in maintaining question uniformity (eg, cultural and language differences) between countries.Citation38 It must also be noted that between-country differences may reflect inherent biases of the database samples used in the survey. There are potential advantages of telephone-based surveys versus face-to-face interviews for conducting qualitative research, including decreased cost and travel, and ability to reach geographically dispersed respondents. However, the requirement for a short interview duration, and the absence of visual or nonverbal cues are potential limiting factors.Citation39,Citation40
Conclusion
In summary, the current survey demonstrates that “fragile skin” was perceived to occur in a substantial proportion of individuals from any given country, particularly in individuals in the age range of 15–34 years, regardless of skin type. These findings need to be confirmed through objective evaluation on the basis of relevant and specific assessments. Meanwhile, preventive strategies for individuals with “fragile skin” may already be available.
Disclosure
MH declares no conflicts of interest in this work. CT is an employee of Pierre Fabre SA, Paris, France. CC is an employee of Laboratoires Dermatologiques A-Derma. The authors thank David P Figgitt of Content Ed Net for providing medical writing and editorial assistance in the preparation of this manuscript, funding for which was provided by Pierre Fabre SA.
References
- ProkschEBrandnerJMJensenJMThe skin: an indispensable barrierExp Dermatol200817121063107219043850
- BaroniABuomminoEDe GregorioVRuoccoERuoccoVWolfRStructure and function of the epidermis related to barrier propertiesClin Dermatol201230325726222507037
- SchindlerCAMikhailovTAKuhnEMProtecting fragile skin: nursing interventions to decrease development of pressure ulcers in pediatric intensive careAm J Crit Care2011201263421196569
- Del RossoJQLevinJThe clinical relevance of maintaining the functional integrity of the stratum corneum in both healthy and disease-affected skinJ Clin Aesthet Dermatol201149224221938268
- HaftekMCallejonSSandjeuYCompartmentalization of the human stratum corneum by persistent tight junction-like structuresExp Dermatol201120861762121672033
- YoshidaKYokouchiMNagaoKIshiiKAmagaiMKuboAFunctional tight junction barrier localizes in the second layer of the stratum granulosum of human epidermisJ Dermatol Sci2013712899923712060
- HaftekMSimonMSerreGCorneodesmosomes: pivotal actors in the stratum corneum cohesion and desquamationEliasPMFeingoldKRSkin BarrierNew York, NYTaylor and Francis Group2006
- HaftekMTeillonMHSchmittDStratum corneum, corneodesmosomes and ex vivo percutaneous penetrationMicrosc Res Tech19984332422499840802
- CaubetCJoncaNBrattsandMDegradation of corneodesmosome proteins by two serine proteases of the kallikrein family, SCTE/KLK5/hK5 and SCCE/KLK7/hK7J Invest Dermatol200412251235124415140227
- BouwstraJAHoneywell-NguyenPLGoorisGSPonecMStructure of the skin barrier and its modulation by vesicular formulationsProg Lipid Res200342113612467638
- HaftekMThe stratum corneumAnn Dermatol Venereol20021291 Pt 2117122 French11976538
- RoelandtTGiddeloCHeughebaertCThe “caveolae brake hypothesis” and the epidermal barrierJ Invest Dermatol2009129492793619005485
- EliasPMArbiserJBrownBEEpidermal vascular endothelial growth factor production is required for permeability barrier homeostasis, dermal angiogenesis, and the development of epidermal hyperplasia: implications for the pathogenesis of psoriasisAm J Pathol2008173368969918688025
- EliasPMSchmuthMAbnormal skin barrier in the etiopathogenesis of atopic dermatitisCurr Opin Allergy Clin Immunol20099543744619550302
- EliasPMWilliamsMLFeingoldKRAbnormal barrier function in the pathogenesis of ichthyosis: therapeutic implications for lipid metabolic disordersClin Dermatol201230331132222507046
- XuXLauKTairaBRSingerAJThe current management of skin tearsAm J Emerg Med200927672973319751631
- FernandesJDMachadoMCOliveiraZNChildren and newborn skin care and preventionAn Bras Dermatol201186110211021437530
- LeBlancKBaranoskiSHollowaySLangemoDValidation of a new classification system for skin tearsAdv Skin Wound Care201326626326523685526
- Stephen-HaynesJSkin tears: achieving positive clinical and financial outcomesBr J Community Nurs2012SupplS6S8S10 passim22584188
- SchäferTNienhausAVielufDBergerJRingJEpidemiology of acne in the general population: the risk of smokingBr J Dermatol2001145110010411453915
- HanifinJMReedMLEczema Prevalence and Impact Working GroupA population-based survey of eczema prevalence in the United StatesDermatitis2007182829117498413
- MiseryLSibaudVMerial-KienyCTaiebCSensitive skin in the American population: prevalence, clinical data, and role of the dermatologistInt J Dermatol201150896196721781068
- BerardescaEFarageMMaibachHSensitive skin: an overviewInt J Cosmet Sci20133512822928591
- FarageMAPerceptions of sensitive skin: changes in perceived severity and associations with environmental causesContact Dermatitis200859422623218844698
- FarageMAMaibachHISensitive skin: closing in on a physiological causeContact Dermatitis201062313714920565500
- LeBlancKBaranoskiSSkin Tear Consensus Panel MembersSkin tears: state of the science: consensus statements for the prevention, prediction, assessment, and treatment of skin tearsAdv Skin Wound Care201124Suppl 921521876389
- Garcia BartelsNMleczkoASchinkTProquittéHWauerRRBlume-PeytaviUInfluence of bathing or washing on skin barrier function in newborns during the first four weeks of lifeSkin Pharmacol Physiol200922524825719690450
- Blume-PeytaviUHauserMStamatasGNPathiranaDGarcia BartelsNSkin care practices for newborns and infants: review of the clinical evidence for best practicesPediatr Dermatol201229111422011065
- KottnerJLichterfeldABlume-PeytaviUTransepidermal water loss in young and aged healthy humans: a systematic review and meta-analysisArch Dermatol Res2013305431532323341028
- Ramos-e-SilvaMBozaJCCestariTFEffects of age (neonates and elderly) on skin barrier functionClin Dermatol201230327427622507040
- SimonMBernardDMinondoAMPersistence of both peripheral and non-peripheral corneodesmosomes in the upper stratum corneum of winter xerosis skin versus only peripheral in normal skinJ Invest Dermatol20011161233011168794
- TwengeJMCampbellWKThe Narcissism EpidemicsNew York, NYSimon and Schuster2009
- GargAChrenMMSandsLPPsychological stress perturbs epidermal permeability barrier homeostasis: implications for the pathogenesis of stress-associated skin disordersArch Dermatol20011371535911176661
- ChoiEHBrownBECrumrineDMechanisms by which psychologic stress alters cutaneous permeability barrier homeostasis and stratum corneum integrityJ Invest Dermatol2005124358759515737200
- Knutsen-LarsonSDawsonALDunnickCADellavalleRPAcne vulgaris: pathogenesis, treatment, and needs assessmentDermatol Clin20123019910622117871
- KimGKMichaelsBBPost-adolescent acne in women: more common and more clinical considerationsJ Drugs Dermatol201211670871322648217
- Ramos-e-SilvaMJacquesCDEpidermal barrier function and systemic diseasesClin Dermatol201230327727922507041
- DolnicarSGrünBCross-cultural differences in survey response patternsInt Market Rev2007242127143
- BowlingAMode of questionnaire administration can have serious effects on data qualityJ Public Health (Oxf)200527328129115870099
- NovickGIs there a bias against telephone interviews in qualitative research?Res Nurs Health200831439139818203128