
Abstract
Background
Dexlansoprazole is a proton pump inhibitor (PPI) approved for use in dual delayed-release capsule and orally disintegrating tablet (ODT) formulations.
Aim
To assess effects of food, water, and route of administration on the bioavailability of dexlansoprazole 30-mg ODT.
Methods
Two separate open-label, phase 1, single-dose crossover studies were conducted in healthy adults. In study 1, pharmacokinetic parameters were analyzed in participants receiving dexlansoprazole ODT in a fed or fasted state with and without water. In study 2, the bioavailability of dexlansoprazole after administration via oral syringe or nasogastric (NG) tube, or after swallowing intact with water was compared to ODT administration in the fasted state, swallowed without water. Blood samples for determining dexlansoprazole plasma concentrations and pharmacokinetic parameter estimates were collected before and after dosing.
Results
Equivalent values for area under the plasma concentration–time curve (AUC) were observed in the fed and fasted states, but the maximum observed plasma concentration (Cmax) was 38% lower in the fed state; therefore, bioequivalence was not achieved. A water rinse following standard ODT administration decreased dexlansoprazole bioavailability, with lower Cmax and AUC values than when ODT was administered without a water rinse. Bioequivalence was demonstrated when comparing the alternative routes of administration, including via oral syringe or NG tube with standard ODT administration. Unlike with a water rinse, bioequivalence to standard ODT administration (i.e., without water) was demonstrated when swallowing the ODT intact with water. Rates of adverse events were comparable irrespective of administration route in the fasted state (6.7%–9.3%) and were 12% higher in the fed state than in the fasted state.
Conclusion
The AUC from the dexlansoprazole ODT was equivalent when administered in the fed and fasted states. Equivalent systemic exposure to dexlansoprazole was achieved regardless of the administration route.
Introduction
Gastroesophageal reflux disease (GERD) is a common digestive acid-related disorder, most notably associated with symptoms of heartburn and acid regurgitation with a prevalence of up to 20% in North American adults.Citation1,Citation2 Options for drug therapy include acid-suppressing agents, such as antacids, histamine 2-receptor antagonists, and proton pump inhibitors (PPIs). PPIs are the treatment of choice for GERD symptom relief and healing of esophageal erosions.Citation1
Dexlansoprazole is a PPI that suppresses gastric acid secretion by inhibiting the hydrogen-potassium adenosine triphosphatase pump in the gastric parietal cell; the final step of acid production is blocked by the specific action on this gastric proton pump.Citation3 Dexlansoprazole dual delayed-release capsules are indicated for the healing of erosive esophagitis (EE), maintenance of healed EE and relief of heartburn, and the treatment of heartburn associated with symptomatic nonerosive GERD in patients ≥12 years of age.Citation3 The pharmacokinetic, pharmacodynamic, efficacy, and safety profiles following administration of dexlansoprazole 30-, 60-, and 90-mg capsules have been studied extensively.Citation4–Citation8 With the dual delayed-release formulation, the initial release of dexlansoprazole occurs 1–2 hours after dosing followed by a second release 4–5 hours after dosing, allowing 24-hour control of intragastric acidity.Citation8
The capsule and tablet formulations of most PPIs are intended to be swallowed, and thus, are not ideal for patients with difficulty swallowing. Difficulty swallowing is often present in patients who suffer from neurologic or muscular disorders, such as post-polio syndrome, multiple sclerosis, muscular dystrophy, Parkinson’s disease, Alzheimer’s disease, myasthenia gravis, scleroderma, and eosinophilic esophagitis, and other disorders that might restrict movement of the esophagus.Citation9–Citation13 Although epidemiologic data regarding reflux symptoms in neuromuscular disorders are scarce, GERD has a high prevalence (26.5%) in a group of patients with Parkinson’s disease and has also been associated with dysphagia in a general population study.Citation14,Citation15 In a population-based survey of 7640 patients, GERD was the most common diagnosis among those who reported difficulty swallowing.Citation16 Furthermore, in patients with severe dysphasia, especially the elderly with inadequate food intake and malnutrition, short-term use of a nasogastric (NG) tube is indicated.Citation17 Consequently, a 30-mg orally disintegrating tablet (ODT) formulation of dexlansoprazole was developed for dosing flexibility, providing an alternative option for patients unable or unwilling to swallow capsules. The bioequivalence between 30-mg formulations of dexlansoprazole ODT and capsule was demonstrated in a phase 1 crossover study.Citation18 Dexlansoprazole 30-mg ODT has recently been approved in the USA in patients ≥12 years of age for the treatment of heartburn associated with symptomatic nonerosive GERD, maintenance of healed EE, and relief of heartburn, the same indications for which the dexlansoprazole 30-mg capsule is approved. A 60-mg daily dose of the capsule is also approved for the healing of EE.Citation3
Herein, we describe the results from two separate studies conducted in healthy adults that assessed the effects of food, water, and alternative routes of administration on the bioavailability of 30-mg dexlansoprazole ODT. Study 1 measured the bioavailability of dexlansoprazole ODT in the fed and fasted states and with and without water in the fasted state. Study 2 compared the bioavailability of dexlansoprazole ODT administration directly on the tongue without water vs administration via oral syringe or NG tube after the tablet was allowed to disintegrate in water or after swallowing the ODT intact with water.
Materials and methods
The effects of various dexlansoprazole ODT dosing regimens and multiple routes of administration on bioavailability were assessed in two phase 1, randomized, open-label, single-center, single-dose crossover studies conducted in healthy adults in the USA. Study 1 assessed the bioavailability of dexlansoprazole in the fed and fasted states and with and without consumption of water in the fasted state. Study 2 evaluated bioavailability after using different routes of delivering the dexlansoprazole ODT in fasting participants. Study 1 was conducted at the Covance Madison Clinical Research Unit in Madison, Wisconsin, from April to August 2012 and study 2 was conducted at Celerion in Neptune, NJ, USA from August to December 2012. Both studies were designed according to the Food and Drug Administration of the United States (FDA) Guidance for Industry: Bioavailability and Bioequivalence Studies for Orally Administered Drug Products – General Considerations.Citation19 Study 1 was also performed with consideration to the FDA Guidance for Industry: Food-Effect Bioavailability and Fed Bioequivalence Studies.Citation20 Trial protocols met the principles within the Declaration of HelsinkiCitation21 and the International Conference on Harmonisation (ICH) Harmonised Tripartite Guideline for Good Clinical Practice,Citation22 and were approved by the Independent Investigational Review Boards at each site (Chesapeake Research Review, Inc., Columbia, Maryland, USA and Independent Investigational Review Board INC, Plantation, FL, USA). Trial registration was not required for either study at the time of conduct, as phase 1 drug trials are excluded from US Food and Drug Administration Amendments Act 801 registration requirements.Citation23 All participants gave written informed consent before beginning the study.
Study participants
Eligible participants were healthy adults between the age of 18 and 55 years and weighed ≥50 kg with a body mass index ≥18 and ≤30 kg/m2. Participants with any clinically significant hematologic, neurologic, cardiovascular, pulmonary, hepatic, renal, metabolic, gastrointestinal, urological, immunologic, endocrine, or psychiatric disorder, or history of malignant disease were ineligible for enrollment. Participants were also considered ineligible if they had recently received agents that could alter hepatic or renal clearance, or contained nicotine, caffeine, xanthine, or grapefruit products, or if they had evidence of either drug or alcohol consumption. A known hypersensitivity to any component of dexlansoprazole ODT, dexlansoprazole capsules, or other PPIs, or prior use of dexlansoprazole, lansoprazole, or any investigational compound for any indication within 30 days before check-in (day –1 of the first treatment period) were grounds for study exclusion. In addition, both non-sterilized male participants and female participants of childbearing potential had to agree to routine contraception use for the duration of the study and for the 30 days after the last dose. If participants did not meet any of the entry criteria after randomization, they were removed at the discretion of the investigator and not replaced. Participants could also be discontinued because of adverse events.
Treatment regimens
Participants were randomized to one of three (study 1) or four (study 2) treatment sequences; each comprised three (study 1) or four (study 2) treatment periods (Tables S1 and S2). For each treatment period, participants were confined to the study site from the day before dose administration until all study procedures had been completed on day 2. A single dose of dexlansoprazole 30-mg ODT was administered on day 1 of each treatment period according to the dosing regimen dictated by the treatment sequence. Participants were discharged from the study site for a washout interval of at least 5 days between subsequent treatment periods. A follow-up phone call was made 5–10 days after the final dose of study drug to monitor for any ongoing or emergent adverse events.
Reference regimen
The reference regimen in both studies required administering dexlansoprazole ODT directly on the tongue without water. Participants were instructed to allow the tablet to disintegrate and to swallow the granules without chewing. Participants could drink water at any time outside of the 2-hour window ranging from 1 hour before and after receiving the drug. Participants receiving the reference regimen were to have fasted for ≥10 hours before dosing and remained fasting for 4 hours postdose.
Study 1 (effects of food and water) test regimens
In this study, participants were randomized in a 1:1:1 ratio to three possible treatment sequences, each including a period where they received tests 1A, 1B, or the reference regimen (Table S1). With test regimen 1A, the bioavailability of dexlansoprazole ODT when administered in the fed state without water was examined. Participants fasted overnight for ≥10 hours and were served a high-fat breakfast 30 minutes before the scheduled dose. The tablet was then administered without water as in the reference regimen. In test regimen 1B, the bioavailability of dexlansoprazole ODT when administered with water was examined. A single dose of dexlansoprazole ODT was administered after a minimum 10-hour fast according to the reference regimen, but was then followed by consumption of 240 mL of water (the recommended volume of administration stated by the FDA Guidance for Industry: Bioavailability and Bioequivalence Studies Submitted in NDAs or INDs—General Considerations)Citation19 after the tablet was disintegrated on the tongue and swallowed. All participants were limited to the standardized meals and snacks provided by the site. Breakfast was only served during the treatment period for test regimen 1A, and all groups received lunch and dinner.
Study 2 (alternative routes of administration) test regimens
In this study, participants were randomized in a 1:1:1:1 ratio to four possible treatment sequences, each including a treatment period for the tests 2A, 2B, 2C, or reference regimen (Table S2). With test regimens 2A and 2B, the bioavailability of dexlansoprazole ODT was examined when administered orally via syringe or an 8 French NG tube directly to the stomach, respectively. In both regimens, the intact tablet was placed into a syringe and allowed to disintegrate in 15–20 mL of water. After initial administration in each regimen, an additional 10 mL of water was used to rinse the dosing syringe. This rinse was performed twice, and the water used for the rinse was administered to participants after each rinse. With test regimen 2C, a single dose of dexlansoprazole ODT was administered orally with direction to swallow the tablet intact with 240 mL of water.
Evaluations
In both studies, blood samples (3 mL) were collected from a peripheral vein at ≤30 minutes before treatment and at 0.5, 1, 1.5, 2, 3, 4, 5, 6, 7, 8, 10, 12, 16, and 24 hours after dose administration. Plasma concentrations of dexlansoprazole were measured by a proprietary validated liquid chromatography tandem mass spectrometry assay at PPD Development in Middleton, WI, USA. During assay validation, the accuracy (percent difference from theoretical concentrations) and precision (percent coefficient of variation) for dexlansoprazole quality control samples were determined to be −3.83% to 1.07% and 2.45% to 4.56%, respectively. The validated concentration range for dexlansoprazole was 2.00–2000 ng/mL; values below this range were set to zero for pharmacokinetic analysis. In addition, because dexlansoprazole is metabolized by the cytochrome P450 (CYP) 2C19 enzyme, increased plasma concentrations of dexlansoprazole may be observed in CYP2C19 poor metabolizers; therefore, a single blood sample was collected from all participants for the determination of CYP2C19 metabolizer status.
Primary endpoints for both studies included the maximum observed drug concentration in the plasma (Cmax) and the amount of systemic drug exposure, determined by the area under the plasma concentration–time curve (AUC). The AUC values presented were measured from time 0 extrapolated to infinity (AUC∞). The rate of absorption (Tmax), defined as the time to reach Cmax, was a primary endpoint in study 1 and a secondary endpoint in study 2. The apparent clearance after extravascular administration (CL/F), the terminal elimination half-life (T1/2), and the apparent volume of distribution after extravascular administration (Vz/F) were also included as secondary endpoints in study 2.
Statistical analysis
Within each study, individual pharmacokinetic parameters were generated using Phoenix WinNonlin Version 6.3 (Certara, Princeton, NJ, USA) and analyzed with SAS (Statistical Analysis System) Version 9.2 software (SAS Institute, Cary, NC, USA). Actual sampling times were used over scheduled sampling times in all pharmacokinetic parameter calculations. Values for Tmax and log-transformed Cmax and AUC were analyzed using the analysis of variance model with sequence, period, and regimen as fixed effects and the study participant nested within sequence as a random effect. Pharmacokinetic parameters from participants who had data for the reference regimen and at least one of the test regimens were included in the statistical analyses.
Statistical comparisons evaluated the point estimate and 90% confidence intervals (CIs) for the Cmax and AUC central value ratios of the test and reference regimens. Bioequivalence between regimens was declared if the CIs fell within the range of 0.80–1.25.Citation20
A sample size of 72 (24 per treatment sequence) and 80 (20 per treatment sequence) participants was used in studies 1 and 2, respectively. These sample sizes allowed for dropout rates of ~8% (study 1) and 20% (study 2) and provided at least 88% probability of concluding equivalence on dexlansoprazole Cmax between 2 regimens if the true difference between dexlansoprazole Cmax central values from 2 regimens was not >5%. The power for concluding equivalence on dexlansoprazole AUCs between 2 regimens was expected to be >95% for both studies.
Genetic variations between individuals, including CYP polymorphisms, could potentially affect bioavailability estimates. However, CYP2C19 genotype was not expected to affect the assessment of bioavailability because each participant received both treatment regimens, serving as his or her own control in the crossover study design employed. Consequently, no formal statistical analyses were conducted based on CYP2C19 genotype.
Results
Study participants
In total, 72 and 77 participants were randomized in studies 1 and 2, respectively (Tables S1 and S2). Participant demographics were comparable across treatment sequences within each study ().
Table 1 Demographic and baseline characteristics
Pharmacokinetic parameter estimates of dexlansoprazole ODT administration with and without food or water
Pharmacokinetic parameter estimates following dexlansoprazole ODT administration in the fed and fasted states with and without water are summarized for each regimen in . The absorption of dexlansoprazole ODT was slower in the fed state with a median Tmax of 6 vs 4 hours in the fasted state (). Furthermore, the mean Cmax was lower in the fed state (445 ng/mL) than in the fasted state (688 ng/mL; ). The mean AUC, which measures systemic exposure, was similar between the fed and fasted states (); similar values for mean T1/2, CL/F, and Vz/F between the two regimens were also observed (). When statistically comparing ODT administration in fed and fasted states, the 90% CIs of dexlansoprazole AUC values (0.8776–1.0242) were contained within the predetermined range of bioequivalence – that is, within 0.80–1.25 (; ). The 90% CI for Cmax did not meet bioequivalence criteria (0.5568–0.6908) and the point estimate suggests that the peak concentration was ~38% lower in the fed state (; ).
Figure 1 Study 1: statistical comparisons of pharmacokinetic parameter estimates after administration of dexlansoprazole ODT with or without food or water.
Abbreviations: AUC∞, area under the plasma concentration–time curve from time 0 to infinity; Cmax, maximum observed plasma concentration.
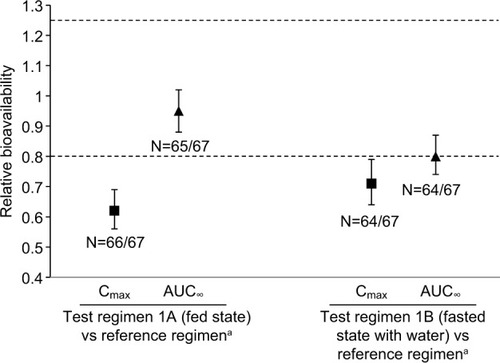
Table 2 Study 1: pharmacokinetic parameter estimates after administration of dexlansoprazole ODT with or without food or water
Table 3 Study 1: statistical comparisons of pharmacokinetic parameter estimates after administration of dexlansoprazole ODT with or without food or water
When comparing dexlansoprazole ODT administration with and without water (test regimen 1B and reference regimen, respectively) similar rates of absorption were observed with median Tmax of 4 hours each (). Participants receiving the ODT with water had a 26% lower mean Cmax than those receiving the reference regimen (508 ng/mL vs 688 ng/mL, respectively; ). Mean AUC was also 15% lower when administration of the ODT was followed with water (). The 90% CIs for both Cmax and AUC values were not in the prespecified range for bioequivalence (; ). Mean T1/2 values were similar between the two regimens ().
Pharmacokinetic parameter estimates of dexlansoprazole after using alternative routes of administration
Pharmacokinetic parameter estimates after using alternative routes of dexlansoprazole ODT administration were summarized for each regimen (). The absorption of dexlansoprazole was similar irrespective of the method of delivery, with all regimens reaching maximum plasma concentrations at 4 hours (). Similarly, mean Cmax and AUC values were consistent for all routes of administration, ranging from 744 to 786 ng/mL and from 3043 to 3340 ng·h/mL, respectively (). No differences were observed for the secondary endpoints of T1/2, CL/F, and Vz/F (). All point estimates of relative bioavailability for Cmax and AUC had 90% CIs that fell within the range for bioequivalence (0.80–1.25), indicating equivalent pharmacokinetic profiles between dexlansoprazole ODT administered via oral syringe, via an NG tube, or as an intact tablet swallowed with water and the reference regimen (i.e., administered intact on the tongue without water; ; ).
Figure 2 Study 2: statistical comparisons of pharmacokinetic parameter estimates for dexlansoprazole ODT after using different routes of administration.
Abbreviations: AUC∞, area under the plasma concentration–time curve from time 0 to infinity; Cmax, maximum observed plasma concentration; ODT, orally disintegrating tablet; PK, pharmacokinetic.
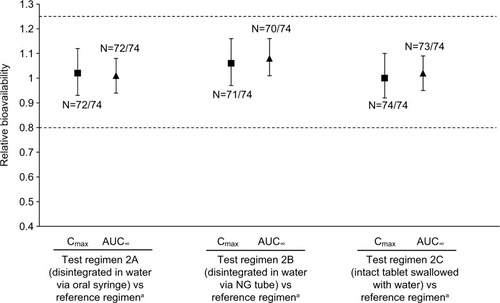
Table 4 Study 2: pharmacokinetic parameter estimates for dexlansoprazole ODT after using different routes of administration
Table 5 Study 2: statistical comparisons of pharmacokinetic parameter estimates for dexlansoprazole ODT after using different routes of administration
Summary of adverse events
The majority of events in both studies were classified by the investigator as of mild intensity and unrelated to study drug. In study 1, there was a higher rate of treatment-emergent adverse events among those who received a high-fat meal for breakfast (test regimen 1A; 21.2%) than among those who had fasted (test regimen 1B; 8.8% or reference regimen; 13.2%). Adverse events that occurred in 2 or more of the study 1 participants with any treatment regimen were headache, arthropod bite, and vessel puncture site pain, occurring at rates of 6.9% (n=5), 4.2% (n=3), and 4.2% (n=3), respectively. Three participants discontinued study 1 because of adverse events, including 1 case of pressured speech and agitation, 1 case of anxiety-related symptoms, and 1 case of worsening of anemia; all were attributed to preexisting conditions.
In study 2, treatment-emergent adverse events occurred with comparable rates (6.7%–9.3%), irrespective of the route of administration. Headache (n=6; 7.8%) was the only adverse event that occurred in 2 or more study 2 participants with any treatment regimen. Two participants discontinued study 2 because of adverse events, including one participant who was unable to tolerate placement of the NG tube, and one participant who had elevated creatine kinase levels before NG tube regimen dosing at the treatment period 4 check-in visit. The latter participant had creatine kinase levels return to normal after being withdrawn from the study medication. No serious adverse events or deaths were reported in either of the studies.
Discussion
The studies described were designed to assess the effect of food, water, and alternative routes of administration on the pharmacokinetic parameters of dexlansoprazole derived from the novel 30-mg ODT formulation. Approved in 2009, the dual delayed-release dexlansoprazole capsule formulation has proven efficacyCitation3,Citation8; however, swallowing the capsule whole may prove difficult for some patients.
In general, patients who have difficulty in swallowing have been found to be less compliant.Citation24 Other options for patients who have trouble in swallowing dexlansoprazole capsules include opening the capsule and administering the granules mixed with water in an oral syringe, via a size 16 French or larger NG tube, or by sprinkling the granules on applesauce.Citation3,Citation25 However, greater adherence has been reported with ODT administration, and dysphagic patients have reported a preference for ODT delivery.Citation24,Citation26 Dexlansoprazole ODT, which is formulated to disintegrate in the mouth without water when placed on the tongue, provides dosing flexibility for these patients.
Hospitalized patients may require a NG tube for severe dysphagia and for traumatic medical events, severe malnutrition, or a range of neurologic disorders.Citation17 Oral syringes are the preferred apparatus for dispensing oral liquid medications in inpatient settings.Citation27 The microgranules contained in the dexlansoprazole ODT are smaller than the granules in the capsule formulation and therefore much easier to disperse in water and administer in an oral syringe or a smaller NG tube (e.g., size 8 French). The results reported here demonstrate that similar systemic exposure to dexlansoprazole was achieved when swallowed intact with water or disintegrated in water and administered orally via a syringe or directly to the stomach via NG tube vs the ODT being swallowed without water after disintegration on the tongue. Bioequivalence between the alternative routes of administration evaluated suggests that the dispersal of ODT in water can be a suitable alternative for patients unable to receive oral therapy.
Compared with the consistent bioavailability observed for the dexlansoprazole ODT after using the different routes of administration in study 2 (including the administration of an intact ODT with water), a moderate decrease in dexlansoprazole bioavailability was observed when dexlansoprazole ODT was placed on the tongue, allowed to disintegrate, swallowed, and then followed with a 240-mL water rinse in study 1. These unexpected results are somewhat contradictory, and the cause of the decrease in bioavailability when a water rinse is used after standard ODT administration is not readily apparent. The difference in Cmax with the water rinse is not considered to negatively affect the overall pharmacodynamic profiles of the ODT formulation, because previous studies have confirmed that the pharmacodynamic effect (increase in intragastric pH) of PPIs is associated with AUC and not Cmax.Citation28–Citation30 In one of these studies, Vakily et al performed pharmacokinetic/pharmacodynamic modeling of the exposure–response relationship between dexlansoprazole AUC and the percent of time pH >4 over a 24-hour period following multiple doses of the dexlansoprazole capsule.Citation30 The relationship between pharmacologic response and dexlansoprazole AUC was described using a simple maximum effect (Emax) model: E=Emax × AUCt/EC50 + AUCt, where E is the predicted pharmacologic response, Emax is the maximum predicted pharmacologic response, and EC50 is the AUCt (AUC from time 0 to the last measurable concentration) that produces 50% of the Emax. Using this model and a dexlan-soprazole Emax of 71% and dexlansoprazole EC50 on day 5 of 642 ng·h/mL, as reported by Vakily et al for the percent of time pH >4, we assessed the effect of the decreased AUC on overall pH control.Citation30 The mean AUCt for the 30-mg ODT administered on the tongue without water followed by a water rinse (2351 ng·h/mL) would be predicted to result in a pH >4 for 55.8% of a 24-hour period, whereas the mean AUCt for the 30-mg ODT administered on the tongue without water (2789 ng·h/mL) would result in a pH >4 for 57.7% of the time. The predicted 1.9% decrease in the percent of time pH >4 is not expected to have a substantial effect on the ability of dexlansoprazole to increase intragastric pH, despite a 20% decrease in AUC when the ODT was administered with a water rinse.
The 90% CIs for the central value ratios of dexlansoprazole AUC between the ODT administered in the fed condition relative to the fasted state were contained within the bioequivalence range of 0.80–1.25. However, administration of the ODT with food resulted in a 38% reduction in dexlansoprazole Cmax. Literature suggests that the antisecretory effect of PPIs is generally acknowledged to be proportional to the AUC,Citation28,Citation29 and in light of these studies, the demonstrated pharmacokinetic equivalence of the AUC values achieved with the ODT administered with or without food suggests that the pharmacodynamic response would be similar following administration of the 30 mg ODT in the fed condition or in the fasted state. The reduced Cmax in the fed condition may not be expected to affect the efficacy or safety profiles of dexlansoprazole ODT. However, due to the reduced Cmax value observed in the fed state, the prescribing information for the dexlansoprazole 30-mg ODT indicates that it should be administered at least 30 minutes before a meal.Citation3
The dexlansoprazole capsule has been available for many years as a safe and effective treatment option for patients with heartburn, GERD, or EE but options for patients with difficulty swallowing were limited to the administration via oral syringe, NG tube, or applesauce. The dual delayed-release of 30-mg dexlansoprazole ODT formulation offers advantages in convenience and compliance for patients with swallowing difficulty. Both dexlansoprazole ODT and capsule are approved in 30-mg doses for the treatment of heartburn in symptomatic nonerosive GERD and for the maintenance of healed EE and relief of heartburn.Citation3 Dexlansoprazole ODT is a promising treatment option for patients ≥12 years of age seeking the efficacy of the dual delayed-release of 30-mg dexlansoprazole capsule with the flexibility in dosing options that the ODT provides.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
Medical writing assistance was provided by Nafis Islam, PharmD, and Bomina Yu, PhD, CMPP, of inVentiv Medical Communications, which was supported by Takeda Pharmaceuticals USA, Inc. The authors thank both Dr. Michael Cwik, an employee of Takeda and the staff of PPD, Middleton, WI, for conducting the bioanalytical portion of the study. The authors also thank Ms. Angela Gamble and Ms. Kelly Hanna for managing the conduct of studies 1 and 2, respectively.
All authors had access to the data and vouch for the veracity and completeness of the data and the data analysis. Funding for this study was provided by Takeda Development Center Americas, Inc.
Supplementary materials
Table S1 Study 1 treatment sequences
Table S2 Study 2 treatment sequences
Disclosure
All authors are employees of Takeda Development Center Americas, Inc., a wholly owned subsidiary of Takeda Pharmaceuticals America, Inc. The authors report no other conflicts of interest in this work.
References
- KatzPOGersonLBVelaMFGuidelines for the diagnosis and management of gastroesophageal reflux diseaseAm J Gastroenterol20131083308328 quiz 32923419381
- DentJEl-SeragHBWallanderMAJohanssonSEpidemiology of gastro-oesophageal reflux disease: a systematic reviewGut200554571071715831922
- Dexilant and Dexilant SoluTab [package insert]Deerfield, ILTakeda Pharmaceuticals America Inc2016
- SharmaPShaheenNJPerezMCClinical trials: healing of erosive oesophagitis with dexlansoprazole MR, a proton pump inhibitor with a novel dual delayed-release formulation – results from two randomized controlled studiesAliment Pharmacol Ther200929773174119183157
- MetzDCHowdenCWPerezMCLarsenLO’NeilJAtkinsonSNClinical trial: dexlansoprazole MR, a proton pump inhibitor with dual delayed-release technology, effectively controls symptoms and prevents relapse in patients with healed erosive oesophagitisAliment Pharmacol Ther200929774275419210298
- PeuraDAMetzDCDabholkarAHParisMMYuPAtkinsonSNSafety profile of dexlansoprazole MR, a proton pump inhibitor with a novel dual delayed release formulation: global clinical trial experienceAliment Pharmacol Ther200930101010102119735233
- DabholkarAHHanCParisMMPerezMCAtkinsonSNPeuraDAThe 12-month safety profile of dexlansoprazole, a proton pump inhibitor with a dual delayed release formulation, in patients with gastro-oesophageal reflux diseaseAliment Pharmacol Ther201133336637721118280
- LeeRDVakilyMMulfordDWuJAtkinsonSNClinical trial: the effect and timing of food on the pharmacokinetics and pharmacodynamics of dexlansoprazole MR, a novel Dual Delayed Release formulation of a proton pump inhibitor – evidence for dosing flexibilityAliment Pharmacol Ther200929882483319243357
- SoniesBCDalakasMCDysphagia in patients with the post-polio syndromeN Engl J Med199132417116211672011159
- DanielsSKNeurological disorders affecting oral, pharyngeal swallowingGI Motility Online2006 http://www.nature.com/gimo/contents/pt1/full/gimo34.htmlAccessed January 1, 2017
- JaradehSMuscle disorders affecting oral and pharyngeal swallowingGI Motility Online2006 http://www.nature.com/gimo/contents/pt1/full/gimo35.htmlAccessed January 1, 2017
- SheehanNJDysphagia and other manifestations of oesophageal involvement in the musculoskeletal diseasesRheumatology (Oxford)200847674675218326539
- YanBMShafferEAEosinophilic esophagitis: a newly established cause of dysphagiaWorld J Gastroenterol200612152328233416688820
- MaedaTNagataKSatohYYamazakiTTakanoDHigh prevalence of gastroesophageal reflux disease in Parkinson’s disease: a questionnaire-based studyParkinsons Dis2013201374212823476890
- LockeGR3rdTalleyNJFettSLZinsmeisterARMeltonLJ3rdPrevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, MinnesotaGastroenterology19971125144814569136821
- ChoSYChoungRSSaitoYAPrevalence and risk factors for dysphagia: a USA community studyNeurogastroenterol Motil201527221221925376877
- CioconJOIndications for tube feedings in elderly patientsDysphagia199051152118023
- KukulkaMNudurupatiSPerezMCPharmacokinetics and pharmacodynamics of an orally disintegrating tablet formulation of dexlansoprazoleTherap Adv Gastroenterol201696759769
- Food and Drug Administration Center for Drug Evaluation and Research (CDER), US Department of Health and Human ServicesGuidance for Industry: Bioavailability and Bioequivalence Studies Submitted in NDAs or INDs—General ConsiderationsRockville, MDFood and Drug Administration32014 Available from: http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm389370.pdfAccessed January 1, 2017
- Food and Drug Administration Center for Drug Evaluation and Research (CDER), US Department of Health and Human ServicesGuidance for Industry: Food-Effect Bioavailability and Fed Bioequivalence StudiesRockville, MDFood and Drug Administration122002 Available from: http://www.fda.gov/downloads/RegulatoryInformation/Guidances/UCM126833.pdfAccessed January 1, 2017
- World Medical AssociationWorld Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjectsJAMA2013310202191219424141714
- International Conference on Harmonisation of technical requirements for registration of pharmaceuticals for human u. ICH harmonized tripartite guideline: guideline for Good Clinical PracticeJ Postgrad Med2001471455011590294
- FDAAA 801 Requirements ClinicalTrials.gov website [Updated November 2015]. Available from: https://clinicaltrials.gov/ct2/managerecs/fdaaaAccessed June 22, 2016
- Carnaby-MannGCraryMPill swallowing by adults with dysphagiaArch Otolaryngol Head Neck Surg20051311197097516301368
- CzerniakRVakilyMWuJTAK-390MR, a novel dual delayed release formulation of a PPI, is bioequivalent when administered as granules sprinkled over applesauce or as an intact capsuleAm J Gastroenterol2008103S4S5 Abstract 12
- MaaloufNDeveloping patient-centric drug formulations to meet patient needsBusiness Dev Licensing J20132014
- GrissingerMOral syringes: making better use of a crucial and economical risk-reduction strategyP T20133815623599662
- HuntRHArmstrongDJamesCEffect on intragastric pH of a PPI with a prolonged plasma half-life: comparison between tenatoprazole and esomeprazole on the duration of acid suppression in healthy male volunteersAm J Gastroenterol200510091949195616128938
- LindTRydbergLKylebackAEsomeprazole provides improved acid control vs. omeprazole in patients with symptoms of gastro-oesophageal reflux diseaseAliment Pharmacol Ther200014786186710886041
- VakilyMZhangWWuJAtkinsonSNMulfordDPharmacokinetics and pharmacodynamics of a known active PPI with a novel Dual Delayed Release technology, dexlansoprazole MR: a combined analysis of randomized controlled clinical trialsCurr Med Res Opin200925362763819232037