Abstract
Pancreatic enzyme replacement therapy is currently the mainstay of treatment for nutrient malabsorption secondary to pancreatic insufficiency. This treatment is safe and has few side effects. Data demonstrate efficacy in reducing steatorrhea and fat malabsorption. Effective therapy has been limited by the ability to replicate the physiologic process of enzyme delivery to the appropriate site, in general the duodenum, at the appropriate time. The challenges include enzyme destruction in the stomach, lack of adequate mixing with the chyme in the duodenum, and failing to deliver and activate at the appropriate time. Treatment is begun when clinically significant malabsorption occurs resulting in steatorrhea and weight loss. Treatment failure is addressed in a sequential fashion. Current research is aimed at studying new enzymes and delivery systems to improve the efficiency of action in the duodenum along with developing better means to monitor therapy.
Introduction
Normal pancreatic function ensures effective digestion and absorption of nutrients. Clinical exocrine pancreatic insufficiency occurs when secretions of the pancreas do not maintain normal digestive function, resulting in nutrient malabsorption and other symptoms such as diarrhea, which in turn affect quality of life and eventually result in malnutrition.Citation1–Citation3 The leading cause of pancreatic insufficiency is chronic pancreatitis, which is estimated to affect 0.4% to 5% of the world population.Citation4 In children, however, the most common cause of pancreatic insufficiency is cystic fibrosis. The reported prevalence of exocrine pancreatic insufficiency in chronic pancreatitis and cystic fibrosis is 30% to 40% and 80% to 90% respectively.Citation5 The use of oral therapy pre-dates the creation of the US Food and Drug Administration (FDA) in 1938, and currently enzyme replacement is the mainstay of therapy in patients diagnosed with malabsorption secondary to pancreatic insufficiency.
In order to manage patients effectively with malabsorption related to exocrine pancreatic insufficiency, an understanding of normal pancreatic physiology and pathophysiology is required. This review provides an overview of normal pancreatic function and the biochemistry of lipid digestion, along with the pathophysiologic mechanisms of disease that lead to malabsorption. Enzyme replacement therapy is reviewed including the pharmacokinetics, various preparations, dosing, and side effects. The inadequacy of current therapy has led to ongoing research, which is reviewed in detail to examine how this has improved our understanding of lipid digestion and also the therapy we have to offer.
Normal exocrine pancreatic physiology
Composition and regulation of pancreatic fluid secretion
The exocrine pancreas plays a key role in the digestive function through the secretion of pancreatic juice consisting of numerous enzymes and of aqueous solution rich in sodium bicarbonate. Postprandial secretion can increase up to 1 to 2 L per day.Citation6–Citation8 Three main types of enzymes are secreted to digest the ingested macronutrients: proteins (trypsinogen 1, 2, and 3, chymotrypsinogen, proelastase 1 and 2, protease E, kallikreinogen, procarboxypeptidase A1, A2, B1, and B2), starchy foods (α-amylase), and lipids ().Citation9–Citation21 While lipases and amylase are secreted in the active form, proteases are secreted as pro-enzymes. Trypsinogen is converted to its active form trypsin in the duodenum by enterokinase, a protease secreted by the enterocytes, and trypsin in turn activates the other pancreatic proteases.
Table 1 Human pancreatic enzymes involved in lipid digestion
Enzyme content of pancreatic fluid changes according to different factors including age, gender, and diet. The pancreas reaches mature function by 2 years of age,Citation22 and enzyme secretion is lower in full-term newborns and young infants than in adults.Citation22–Citation25 Pancreatic secretion in the elderly is decreased, with as little as 56% of young adult function maintained, but the clinical impact is controversial.Citation26,Citation27 Men may have higher levels of secretion than women but the physiological relevance is not documented.Citation27 Pancreatic fluid composition varies highly among individuals.Citation7,Citation28–Citation31 Amount and type of lipids consumed might explain in part this individual variability. Indeed, a 2-week high-fat/low-carbohydrate diet is associated with a 4-fold higher pancreatic enzyme output in healthy humans compared with a diet rich in carbohydrates or proteins.Citation32 Pancreatic lipase levels in the human duodenum vary with the quantity and the type of lipids ingested during a single meal.Citation29,Citation30,Citation33–Citation36 The rate of pancreatic enzyme degradation in the small intestinal lumen also varies among individuals.Citation37 As a result of these variables, determining the exact enzyme level secreted by the normal human pancreas is difficult. Furthermore, varying methods used for collection and measurement of activity result in data that are not directly comparable. Pancreatic or duodenal juice is collected using solid or liquid meal,Citation7,Citation24,Citation28,Citation30,Citation31,Citation34–Citation36,Citation38,Citation39 or after direct hormonal stimulationCitation8,Citation22,Citation23,Citation40,Citation41 or through baseline.Citation24,Citation39,Citation42,Citation43 Enzyme activity measurements are in general done under optimized assay conditions and do not indicate the real activity in vivo.Citation28,Citation38 Data are available as enzyme activities or output expressed as Units (U) per minute or U per hour, U per milliliter, or as milligrams of secreted enzymes ( and ).Citation7,Citation8,Citation22–Citation24,Citation29–Citation31,Citation34–Citation36,Citation40–Citation45 To make the comparisons easier, enzyme activities are generally expressed as International Units (IU). One IU is defined as the amount of enzyme required to release 1 μmole of product from the used substrate per mL per min under the standard assay conditions.
Table 2 Baseline and postprandial activity of the main pancreatic enzymes in healthy humansTable Footnotea
Table 3 Postprandial output expressed as amount of the main pancreatic enzymes in the duodenal lumen in healthy adult humansTable Footnotea
There is a specif ic orchestration of the pancreatic fluid secretion during the fed state leading to appropriate enzyme delivery on demand in the duodenum. During the cephalic phase, orosensory perception of lipids seems to increase pancreatic secretion.Citation46–Citation49 During the gastric phase, digestion of proteins by pepsin and of triglycerides by gastric lipase generates amino acids and free fatty acids, respectively.Citation50,Citation51 When delivered through the pylorus, they become powerful stimulants of the cholecystokinin hormone (CCK) produced by the duodenal endocrine cells which stimulates pancreatic enzymes secretion and controls the gastric emptying rate.Citation49 The acidic pH of the chyme entering the duodenum stimulates the release of secretin, which increases the secretion of water and bicarbonate ions from the pancreas.Citation49 This gastric phase of digestion represents an important aspect in the overall postprandial regulation of pancreatic secretion that becomes abnormal after gastric surgery when gastric digestion and emptying are altered.Citation52,Citation53 During the intestinal phase, enterohormones, such as CCK, together with neurotransmitters and neuropeptides further stimulate pancreatic secretion.Citation49,Citation54 Thus, digestive pancreatic enzyme response to a meal follows a specific pattern in which the degree and duration depend on nutrient composition, caloric content, and physical properties of the meal through hormonal and neural regulations; enzyme secretion into the duodenum increases quickly reaching peak output within the first 20 to 60 minutes postprandially, then decreasing to a stable level before reaching an interdigestive level at the end of the digestive period, ie, about 4 hours after meal intake.Citation27
Role of pancreatic enzymes in lipid bioavailability
Pancreatic juice plays a key role in the digestion of all macronutrients, but is most crucial for lipid digestion. Protein digestion begins in the stomach with the concomitant action of hydrochloric acid and pepsin, continues with pancreatic proteases in the duodenum, and finishes with numerous brush border peptidases located all over the small intestine.Citation50 Starch digestion begins in the mouth with salivary amylase, continues with pancreatic amylase, and ends with several intestinal brush border oligosaccharidases.Citation50 In contrast, the majority of lipid digestion and absorption occurs between the pylorus and the ligament of Treitz. Prior to this step, 5% to 40% of the dietary triglyceride acyl chains are released in the stomach by gastric lipase,Citation29,Citation30,Citation34,Citation51,Citation55,Citation56 which continues its action in the duodenum together with pancreatic lipase until these enzymes are degraded by pancreatic proteases.Citation34 The human pancreatic lipase (HPL) specifically cleaves the outer sn-1 and sn-3 esters on the triglyceride molecules and generates two free fatty acids and a 2-monoglyceride.Citation10,Citation19 This lipase needs a specific cofactor, colipase, to anchor at the lipid–droplet surface containing phospholipids and surrounded by bile lipids (bile salts and phospholipids).Citation16,Citation58 Although a pH of 8 to 9 appears to be optimal for this lipase activity in vitro, bile salts allow the enzyme to work efficiently at a pH of 6 to 6.5 in vivo.Citation10,Citation29,Citation35 HPL is responsible for the hydrolysis of 40% to 70% of triglycerides.Citation29,Citation30,Citation34 The pancreatic lipase related 1 protein (hPLRP1) has no known lipolytic activityCitation11,Citation12,Citation16 but inhibits to some extent lipolysis of milk triglycerides by HPL.Citation9 The pancreatic lipase-related 2 protein (hPLRP2) exhibits a broad substrate specificity hydrolyzing milk triglycerides in a synergistic effect with HPL,Citation9 phospholipids,Citation15,Citation16,Citation19 galactolipids,Citation13,Citation18 and esters of lipid-soluble vitamins.Citation17 Carboxyl ester lipase (CEL) (also secreted by mammary gland cells as bile salt-stimulated lipase, (BSSL)) will hydrolyze triglycerides, diglycerides, phospholipids, and esters of lipid-soluble vitamins and of cholesterol.Citation14 Of note, hPLRP2, which is highly expressed in early life, plays an important role in lipid digestion in infants fed human milk,Citation59,Citation60 along with BSSL.Citation59 Phospholipase A2 hydrolyzes phospholipids to lysophospholipidsCitation20 which is essential for an optimal absorption of lipid nutrients.Citation61 Products generated during lipolysis are solubilized in bile salts–mixed micelles and liposomes (vesicles) which allow absorption across the intestinal villi.Citation62 Once absorbed, the digested lipids are converted back to triglycerides, phospholipids, and esters of cholesterol and of lipid-soluble vitamins, then packaged as chylomicrons and transported through the thoracic duct into the systemic circulation for delivery to various sites throughout the body.Citation61,Citation63
Exocrine pancreatic insufficiency
Clinical presentation and diagnosis
Exocrine pancreatic insufficiency (EPI) is largely a clinical diagnosis. A patient with a known cause of pancreatic insufficiency who presents with weight loss and fatty diarrhea is usually begun on treatment without extensive testing. As up to 20% of patients with chronic pancreatitis resulting in insufficiency will present with no history of pain suggestive of pancreatitis, steatorrhea may be the presenting complaint.Citation64 The diagnostic options include indirect measures (ie, 72-hour fecal fat and fecal elastase) or direct measures (ie, secretin–cerulein or secretin–pancreozymin tests). Steatorrhea is classically defined as at least 7 g of fecal fat over 24 hours, in the context of a 72-hour stool test while on 100 g of fat daily;Citation65 however, quantification of fecal fat is inconvenient and difficult. With reasonable clinical suspicion, a positive spot stool test may be adequate to detect steatorrheaCitation66 but will not allow monitoring of response to therapy. Fecal elastase testing may be used to demonstrate a lack of endogenous enzyme. It has been found that fecal elastase is 72% sensitive for severe pancreatic insufficiency and 90% specific. It does have lower sensitivity with milder steatorrhea, and is not as useful in diabetics, as fecal elastase decreases with increased duration of diabetes.Citation67–Citation69 In contrast to the above indirect measurements of pancreatic function, direct measurements with the secretin–cerulein or secretin–pancreozymin tests are the gold standard for accurate assessment of the exocrine function of the pancreas.Citation69,Citation70 However, the limitations of the direct functional tests are that they are usually performed only at specialized centers, and they are time consuming and expensive.Citation69
Patients usually will present for evaluation when <10% of exocrine pancreatic function remains, which results in lipid malabsorption.Citation3,Citation71 Steatorrhea (frothy, foul smelling, buoyant stools), weight loss, abdominal discomfort, and abdominal swelling are the common presenting symptoms and are related to the inadequate lipid digestion. Even with significant pancreatic insufficiency, protein and starch digestion are usually maintained at a normal physiologic level. However, once pancreatic insufficiency progresses, lipid malabsorption becomes the overriding problem and cause of many of the clinical symptoms and nutritional deficiencies. Consequences of abnormal lipid digestion lead to malnutrition, with malabsorption of lipid-soluble vitamins (A, D, E, K), depleted micronutrients, and decreased circulating lipoproteins.Citation3,Citation72–Citation74 Exocrine pancreatic insufficiency itself can cause or exacerbate motility disorders. There are alterations in neurohormonal regulation in gastrointestinal motility; specifically, the production of CCK and of pancreatic polypeptide are adversely affected by undigested food in the intestines, which can lead to rapid gastric emptying and altered antroduodenal and gallbladder motility. In untreated EPI, patients are noted to have shorter fed patterns, and a faster small intestinal transit that is largely reversed with enzyme therapy.Citation71 The severity of such motility disorders is often related to the severity of the pancreatic insufficiency, and this can often be corrected with enzyme replacement therapy.Citation75–Citation80
Causes of lipid maldigestion and malabsorption
There are various causes of pancreatic insufficiency resulting in malabsorption (), and for some the status of pancreatic enzyme levels has been documented ().Citation23,Citation24,Citation35,Citation40,Citation42,Citation44,Citation45,Citation71 Chronic pancreatitis (CP) and cystic fibrosis (CF) are the most common causes of irreversible pancreatic insufficiency. Diabetes may also result in exocrine insufficiency.Citation81 In contrast, decreased production of pancreatic lipase without glandular destruction is associated with Celiac sprue, Crohn’s disease, and Shwachman–Diamond syndrome.Citation2,Citation71 Reversible pancreatic insufficiency has been reported in premature infants due to developmental immaturity.Citation22–Citation25 The pancreas will gain complete function in infants at 2 years of age.Citation22 Other causes of lipid maldigestion are blockage of the pancreatic duct, and surgical resection.Citation2,Citation5,Citation71
Table 4 Etiologies of exocrine pancreatic insufficiency
Table 5 Baseline or postprandial activity of the main pancreatic enzymes in transitory or irreversible pancreatic insufficiencyTable Footnotea
Motility disorders that result in rapid gastric emptying and decreased small intestinal transit time may also be associated with malabsorption due to inadequate lipid digestion. Rapid transit causes poor mixing of food together with bile and pancreatic enzymes, further reduces contact time with the small intestine leading to impaired digestion and absorption, and affects the stimulation of pancreatic function.Citation5,Citation71 For instance, gastrectomy alters gastric emptying, which reduces lipase production because chyme rapidly bypasses the duodenum resulting in reduced stimulation of duodenal hormones that normally stimulate the pancreas to release enzymes.Citation5 Of note, some studies of steatorrhea after gastrectomy have not demonstrated a benefit of pancreatic enzyme supplementation.Citation82
It is also important to be aware that diabetic patients may also suffer from exocrine insufficiency as a result of endocrine failure, presenting as either classic steatorrhea or more subtly as brittle diabetes.Citation81 Studies have reported that exocrine dysfunction occurs in up to 43% of insulin-dependent diabetics, but its severity is typically mild to moderate, and only 1% of these patients require therapy.Citation83,Citation84 Mild to moderate exocrine insufficiency was reported in 30% of type 2 diabetics, 19% of whom were suffering from severe insufficiency.Citation85 These studies raised the question of the clinical significance of EPI in diabetic patients, which would potentially raise health care costs to these patients if expensive enzyme replacement therapy were required. A thorough investigation studied pancreatic function in type 1 diabetic patients with a secretin–cerulein test, fecal fat stimulation, and 2 fecal elastase tests to determine the accuracy of previous studies and define the clinical significance. In this study, 33% of type 1 diabetics were found to have mild to moderate pancreatic insufficiency, but none of the patients had lipase levels <10% of normal, which would necessitate enzyme replacement. It was concluded that fecal elastase or fecal fat levels were not reliable diagnostic tools for diabetes. Moreover, the majority of these patients had steatorrhea not related to pancreatic function, but rather to bacterial overgrowth.Citation69 Although diarrhea and steatorrhea are often multifactorial in diabetics, and the significance of exocrine insufficiency in diabetics is still under study, physicians should be aware of the association and have a low threshold to test for this entity in diabetics.Citation81
The pathophysiology of EPI caused by glandular destruction in CP and CF
Irreversible pancreatic insufficiency is mainly observed in CP and CF.Citation4,Citation5 In CP, long-standing inflammation with fibrosis results in destruction of acinar cells. A variety of proposed pathogenic mechanisms has been described. Alcohol is a common cause of chronic pancreatitis, and it has been shown to be directly toxic to the pancreatic acinar cells. It produces cytoplasmic lipid accumulation ultimately leading to fibrosis and gland failure.Citation57 Moreover, chronic use of alcohol can cause pancreatic secretions to be more lithogenic, which results in stone formation and pancreatic duct obstruction. The contact of stones with the duct lumen will ultimately lead to a cascade of events, which includes ulceration, scarring, stasis, further stone formation with eventual atrophy, and fibrosis.Citation86,Citation87 In contrast to de novo stone formation as a result of alcohol consumption, repeated attacks of acute pancreatitis from various causes including alcohol will result in peri-ductular scarring, which leads to duct obstruction with stasis and a similar cascade of events that will lead to glandular fibrosis.Citation88,Citation89 Oxidized byproducts of metabolism are produced in the liver and secreted in bile, and it is proposed that this results in oxidative stress as the bile is refluxed into the pancreatic ducts. Oxidative stress has also been attributed to high levels of dietary lipids or alcohol.Citation90–Citation92 Also described is an immunologic response that results in an attack on the ductal epithelium, an autoimmune-like reaction, resulting in scarring and fibrosis.Citation93 A recently proposed theory, the SAPE (sentinel acute pancreatitis event) hypothesis, combines a number of the above-described pathogenic mechanisms leading to chronic pancreatitis. It suggests an initial event of acute pancreatitis that leads to an inflammatory response secondary to an insult such as alcohol or oxidative stress. If this insult is removed, tissue repair occurs. If the insult is not removed, proinflammatory cytokines activate pancreatic stellate cells resulting in chronic pancreatitis with fibrosis and tissue destruction. This ultimately leads to reduced secretion of adequate amounts of lipase, giving rise to pancreatic insufficiency.Citation94,Citation95
In CF, the mutation of the CFTR (cystic f ibrosis transmembrane conductance regulator) protein results in abnormal sodium and chloride transport. Normally, luminal chloride is exchanged for bicarbonate, which allows for an alkaline environment within the lumen, allowing highly concentrated proteins to remain in the soluble state. With mutant CFTR protein, the net result is abnormally viscous secretions and an acidic lumen, resulting in ductal obstruction. Prolonged obstruction results in tissue destruction by retained proteolytic enzymes, f ibrosis, fatty replacement, cyst formation, and eventual exocrine insufficiency.Citation3,Citation96
The initial effect of acinar destruction is decreased pancreatic enzyme production (). However, lipid digestion can be maintained to reach an absorption rate of 20% to 80% due to the action of gastric lipase secreted by the fundic mucosa of the stomach;Citation51 indeed this lipase output is normal or higher in CP and CF patients,Citation35,Citation51,Citation97 and its action take place both in the stomach and in the duodenum, being favored by a low level of pancreatic proteases and low intraduodenal pH.Citation51 But the lipolysis rate reached by the gastric lipase is not always sufficient to make up for the lack of pancreatic lipase.Citation5 As continued glandular destruction occurs in CP and CF, the ductules are affected causing inadequate bicarbonate production and resulting in an inability to neutralize acidic chyme.Citation3 Along with decreased pancreatic bicarbonate secretion, gastric acid production is increased in certain conditions associated with pancreatic insufficiency, notably advanced CP and CF.Citation5,Citation35,Citation97–Citation100 Consequently the intraduodenal pH will be acidic (3 to 5)Citation35,Citation98 and will lead to enzyme inactivation and bile salt denaturation.Citation5,Citation71,Citation98 The bile salt pool is even more reduced by decreased enterohepatic circulation of bile secondary to impaired ileal mucosa absorption.Citation101 As bile salts are required to solubilize the lipolytic products within the intestinal lumen, this process further impairs lipid digestion and absorption.Citation3,Citation61
Pancreatic enzyme replacement therapy
Formulations and pharmacokinetics
The goal of supplemental enzyme therapy in EPI is to minimize nutrient malabsorption, especially of lipids, and to do this it is important to achieve an adequate concentration of active pancreatic enzymes in the duodenum at the same time that food is delivered.Citation3,Citation71 Attempting to replicate this physiologic process requires resistance to gastric inactivation and delivery of active enzyme at the site where digestion is required, the duodenum. The composition and various formulations of pancreatin and pancrelipase affect their use and ability to deliver appropriate amounts of active enzyme to the duodenum. Pancreatin, a crude mixture, is derived from swine or ox pancreas, and each milligram contains no less than 2 USP (United States Pharmacopeia) units of lipase and 25 USP units of amylase and protease activity. Pancrelipase is obtained from swine pancreas and is a more concentrated and purified enzyme preparation. Each milligram contains no less than 24 USP units of lipase and 100 USP units of amylase and protease activity. Because of its higher enzyme content, pancrelipase formulations are favored over pancreatin preparations.Citation3 A variety of delivery agents has been developed in attempts to increase resistance to destruction, and enable delivery to sites where lipid digestion is physiologic, ie, the duodenum. The uncoated formulations are susceptible to acidic breakdown in the stomach and are currently used largely in clinical practice to treat the pain of chronic pancreatitis and not malabsorption.Citation102 Enteric-coated preparations were designed to avoid inactivation in the stomach, as the enzyme is protected from the acidic environment by the coating, and then dissolves in the duodenum when pH exceeds 5 to 5.5.Citation3 A wide range of polymers, natural (carboxylmethyl or succinate high amylose starch) or synthetic (methacrylate copolymers, polymer cellulose acetate phtalate, hydroxyl propyl methyl cellulose phtalate), with different pH sensitivity, have been examined as excipients to circumvent the gastric inactivation of enzymes and to control the timing and location of their release in enteric-coated preparations.Citation103,Citation104 They are supposed to allow uniform mixing in the stomach without releasing their content and timely delivery to the duodenum for digestion to proceed. But effective delivery and release are difficult to achieve because the pH in the stomach can fluctuate from 6, owing to the buffering capacity of the meal, down to 2 during the fed state,Citation98 and the duodenal pH ranges from 4 to 6,Citation35,Citation105 with high individual variability. In fact, dissolution characteristics of excipients are quite different in terms of optimum pH (5 or 5.8 for example) and time (49 to 71 minutes for the half-time of release).Citation106–Citation108 As a result, enteric-coated microspheres are not bioequivalent in vitro, and probably not in vivo, depending on the pH of the duodenal content.Citation106–Citation108
Early enteric-coated formulations did not empty into the duodenum as quickly as smaller food particles, impairing their ability to aid in digestion. Newer formulations use the enteric-coated microsphere technology that allows a smaller, yet stable delivery system. Studies have demonstrated that the size of the particles or the microspheres affect the delivery to the duodenum, and that particles of smaller size empty more quickly, with 1.4 mm being the optimal size.Citation109 In theory, along with delivering adequate amounts of lipase to the duodenum at the same time as the ingested food, microsphere technology should allow more adequate mixture with the postprandial chyme.Citation3 Studies of labeled capsules suggest that even with varying sizes of microspheres, the ingested lipid may enter the duodenum in advance of the pancreatic enzyme. When, where and at how much enzyme is released is not very well studied in humans.Citation110 The new FDA rules in terms of pancreatic enzyme replacement therapy (PERT) have instructed companies to set up clinical trials in order to fill this gap. The results of recent studies of delivery of pancrelipase should be informative and could help to ameliorate coating materials (ClinicalTrials.gov NCT00676702, Pancrease MT, Johnson & Johnson Pharmaceutical, NJ, USA; NCT00744250, Pancrecarb MS16, Digestive Care, PA, USA; NCT00559052, Viokase 16, Axcan Pharma, Canada).
Currently, the main formulations are immediate-release, enteric-coated microspheres and minimicrospheres, enteric-coated microtablets, and enteric-coated microspheres with a bicarbonate buffer. A comprehensive table of these medications has been summarized in other reviews.Citation3,Citation76 A major focus of regulation of these products has been on the active enzyme content and accuracy of packaging. While instability of the enzymes results in delivery medications that contain less than the packaged amount of enzyme, the practice of “overfilling” in an effort to address enzyme degradation may result in excess enzyme content, resulting in formulations that deliver inadequate or excess amounts of enzyme. In Europe, historically these products have been regulated, resulting in more standard enzyme content. In the United States, until recently, because of lack of stringent regulation, studies showed marked variation in the enzyme content of the various formulations, generic products being of greatest concern.Citation111 The marketing of products containing pancreatic enzymes extracted from animal tissue preceded the creation of the FDA in 1938, so that these products were historically not regulated by the FDA. In 2004, in response to concerns FDA issued a statement requiring that all manufacturers of PERT submit New Drug Applications. Eventually, the FDA set a deadline of April 28, 2010 for approval of all pancreatic enzyme products, and at the time of submission of this article, only 3 pancrelipase preparations have been approved for use in the United States:Citation112 Creon (Abbott, IL, USA), EUR-1008 or Zenpep (Eurand, Milan, Italy), and Pancreaze (Johnson & Johnson, NJ, USA). All these formulations have been demonstrated to be safe and effective in improving lipid malabsorption and the symptoms of maldigestion. The most studied of the approved enzymes, Creon, is an enteric-coated formulation of pancrelipase delivered in the form of minimicrospheres.Citation113–Citation115 Zenpep is an enteric-coated bead preparation.Citation116 To counteract the problem of non-uniform drug delivery raised by the FDA, this formulation of pancrelipase enteric-coated microtablet is manufactured with label-claimed lipase content being zero-overfilled.Citation116 Clinical Phase III trials demonstrated an improvement in coefficient of fecal fat absorption (CFA) (88.3% vs 62.8% in placebo group) and lipid-soluble vitamin levels.Citation116 Pancreaze is an enteric-coated microtablet.Citation112
In Europe availability of preparations varies by country and they are regulated nationally and not by the European Medicines Agency. Many regulatory agencies provide information on their website and information on available enzyme preparations may be sought through the national regulatory agency, the pharmaceuticals, or pharmacy references. In products in which the enzyme content has been standardized, there is still a marked variability in particle size, release, and, for some, acid stability, which may result in differences in clinical effect.Citation106,Citation117,Citation118
Dosing and schedule of administration
The typical indications for starting enzyme replacement therapy are progressive weight loss and steatorrhea, defined as at least 7 to 15 g of fecal fat per day, but there are no substantial data to support these guidelines. Since steatorrhea does not typically occur until >90% of pancreatic lipase activity is lost, 10% enzyme activity is the initial goal for therapy. Dosing is adjusted based on the amount of lipase in the supplements, and the initial dose aims at supplying 40 to 60 IU/minute of lipase activity within the duodenal lumen. To achieve this goal in adults, approximately 25,000 to 40,000 IU of lipase is required to digest a typical meal, and about 5000 to 25,000 IU of lipase per snack. However, is not recommended to exceed 10,000 IU of lipase per kg of body weight per meal.Citation3,Citation5,Citation71,Citation76 Pediatric dosing is detailed in the products’ respective package inserts. Ultimately 50,000, 100,000 and 150,000 IU of lipase per day will decrease steatorrhea by 45%, 60%, and 70%, respectively.Citation119 Ideally the correct amount of lipase should be divided and administered through the course of a meal or immediately after a meal, and dose adjustments made after several days to allow for sufficient time for the enzymes to work.Citation5 A recent study compared three different administration schedules using enzyme replacement before meals, during meals, or after meals. It was found that lipid digestion was better when giving enzymes during or after meals, and patient preference did not differ.Citation120 Currently, none of the approved enzyme supplements are specifically designed for administration via percutaneous gastrostomy tubes. In patients who cannot swallow large capsules, and infants, opening the capsules into a small amount of acidic food (ie, apple sauce) is an acceptable way to administer the medication.
Monitoring therapy
Currently there are no guidelines in clinical practice for monitoring the efficacy of enzyme replacement therapy and determining a need for dose adjustment. In research studies, a commonly used method to monitor therapy is the use of the CFA and coefficient of nitrogen absorption. The CFA uses a 72-hour stool collection comparing the amount of lipid ingested with that excreted.Citation121–Citation123 The cumbersome nature of stool studies limits their use in the outpatient setting. Commonly, determining the efficacy of therapy is performed by clinically assessing the patient’s weight loss or gain and diarrhea. Unfortunately, clinical assessment correlates poorly with the patient’s nutritional status.Citation124,Citation125 In a recent study, approximately two-thirds of the study subjects, when asymptomatic, had evidence of nutritional deficiencies as measured by retinol-binding protein, ferritin, and pre-albumin. The authors concluded that monitoring of weight loss and diarrhea is an inadequate measure of nutritional deficiencies in EPI.Citation126 Various breath tests have been developed, using various substrates labeled with 13C including mixed triglycerides, triolein, and cholesteryl octanoate.Citation127–Citation129 As an example, the 13C-labeled mixed triglyceride breath test uses a labeled substrate with two molecules of stearic acid and octanoic acid. Lipolysis is associated with measured release of labeled carbon dioxide.Citation130 This test was shown to be accurate in estimating pancreatic exocrine function and has been shown to correlate with nutritional markers when estimating response to enzyme supplementation.Citation131,Citation132 Because stool collection is often time consuming and difficult, and breath tests are not readily available in all locations or fully validated as a clinical tool, following patients clinically is the common approach in determining the efficacy of PERT. As the degree of symptoms and symptom improvement do not always correlate with the patient’s nutritional status, in the future we would hope for more clinically relevant and widely available tests to monitor therapy, most likely in the form of a breath test or a spot stool test.Citation124–Citation126
Efficacy
Although the efficacy of enzyme replacement therapy is presumed, the data are not as robust as one might hope. Although numerous studies have evaluated the response to treatment for outcomes such as steatorrhea and fecal fat, surprisingly few have studied improvement in nutritional status, even in weight gain.Citation2,Citation113–Citation116,Citation122,Citation133 Enzyme supplements have been found to improve lipid malabsorption compared with placebo in numerous trials, for both adults and children younger than 7 years old.Citation2,Citation113–Citation116,Citation122,Citation133 They have also been shown to improve symptoms related to pancreatic insufficiency such as abdominal pain, flatulence, stool consistency, and improve overall global impression of disease symptoms.Citation113 A systematic review of the randomized trials of PERT identified only two studies that evaluated weight as an outcome, and the difference was not significant.Citation134 It has been reported that in patients who were considered to be on acceptable replacement therapy, with reduction in steatorrhea, markers of significant malnutrition still persisted as measured by retinol-binding protein, transferring, and prealbumin.Citation126 In a prospective, non-placebo controlled study, this group has also reported that increasing enzyme therapy to normalize 13C-mixed triglyceride breath test did significantly improve key markers of nutritional status at 1 year.Citation132 As such, although it is presumed, the reduction in stool fat achieved by PERT has not been proven by rigorous research to be correlated with a complete correction of nutritional deficiency in patients with pancreatic insufficiency, preventing our overall assessment of the efficacy of this therapy. In the future, demonstration of long-term outcomes would also be of interest.
Safety and side effects
In general, PERT is regarded as safe with few side effects, and adverse events are comparable to those with placebo.Citation2 Supplemental enzymes act within the lumen of the intestine, and this is considered an intraluminal and not a systemic therapy. The most commonly reported side effects for recently approved enzymes are headache (6%), dizziness (6%), abdominal pain (9%), and flatulence (www.micromedex.com). Historically, hyperuricemia, and hyperuricosuria, which leads to dysuria and uric acid crystaluria, have been reported in cystic fibrosis patients with older formulations.Citation135 Folic acid deficiency has been associated with use of pancreatin extracts which may form insoluble complexes with folate.Citation76 Irritation of the oral mucosa may be avoided by not chewing the medications, or mixing them in foods with a pH > 4.5 (package inserts). A theoretical risk exists of xenotic viral infections, although such cases have not been reported. As more concern is focused on the effect of pthalates, which are commonly present in the polymer coating, the impact of this component will likely be evaluated further.Citation136 The most concerning adverse effect associated with enzyme replacement is fibrosing colonopathy, which has been described in cystic fibrosis patients receiving <24,000 IU of lipase/kg daily.Citation137,Citation138 It results in submucosal collagen deposition with fibrosis and varying degrees of stricturing. Some studies suggest that the acid-resistant coating of enzyme preparations may be responsible for the fibrosing colonopathy, as it has also been demonstrated with other medications that use the same methacrylic copolymer coating.Citation76,Citation139–Citation143 In addition, as these cases largely occurred with high-dose enzyme therapy (>50,000 IU/kg daily), limits are suggested for maximum dosage and delivery. Caution should be used when doses exceed 2500 IU/kg per meal. Most formulations are considered pregnancy class C, as there are insufficient data to evaluate their safety, and no data are available on their secretion in breast milk.
Treatment failure
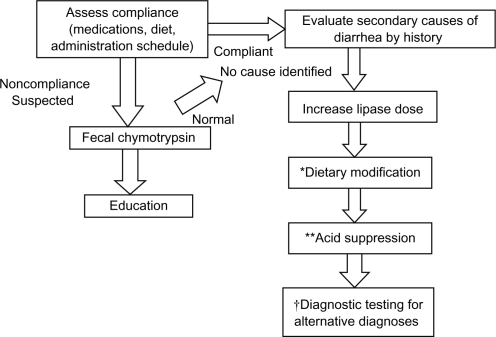
Despite optimal dosing of enzymes and clinical assessment, treatment failures are common. A systematic approach is beneficial in determining the reason for treatment failure (). The first step is to assess compliance, diet, and timing of administration. Studies have demonstrated that efficacy is maximum if medications are taken during and after a meal, and such a schedule may need to be detailed with the patient.Citation5,Citation120 Although wide variation has been noted between products,Citation106,Citation107,Citation111 at this point there is inadequate information to recommend changing formulation if the medication is not working, although this is not an unreasonable practice, given the fact that there are documented differences in delivery and release among the marketed products.Citation117,Citation118 Certainly, in areas in which generic medications are available, if the medication loses its clinical effect in an individual, it should be determined if the medication has been changed to a generic form, and changed to brand name medication if appropriate. If compliance is in question, a fecal chymotrypsin test can be performed to confirm compliance. If these possibilities are eliminated as primary causes of loss of clinical effect, and secondary causes of diarrhea are less likely by history and exam, the first option is to increase the amount of lipase given to see if response improves. If this is not successful, dietary habits may need modification, in particular, a reduction in lipid intake to 50 to 75 g per day.Citation71 Other treatment modifications may include reduction in fiber intake, avoidance of alcohol, and minimizing calcium- and magnesium-containing antacids, as these can all increase steatorrhea. The next step is usually to administer acid-suppressing medications, either histamine-2 receptor blockers or proton pump inhibitors. Studies have shown improved lipid digestion and absorption with administration of acid-suppressing medications to nonenteric-coated formulations.Citation144–Citation146 Furthermore, it has been shown that acid suppression in addition to enteric-coated formulations will improve steatorrhea, and may enable the use of lower amounts of lipase.Citation147 Finally, if all the above steps fail, diagnostic evaluation for other etiologies for continued steatorrhea is warranted, including small intestinal bacterial overgrowth, giardiasis, blind loop syndrome, and other absorptive problems.Citation37,Citation71,Citation76
Figure 1 Failure of pancreatic enzyme therapy: a systematic approach.
Future developments for an optimal therapy
The challenges of current obstacles to effective therapy
Optimal lipid digestion and absorption is not always reached in EPI patients, which is assumed to be due largely to problems with delivery of active lipases at the appropriate intestinal site (duodenum) and time of delivery. Also, the amount and the type of enzymes administered fails to mimic normal human pancreatic secretion that is specific to age and to each individual. Treatment requires intake of multiple capsules and is expensive. Problems of allergy to porcine proteins and religious or other cultural concerns with the use of pork products also have to be taken into account. To address these issues, ongoing research is focusing on identifying new enzyme sources, more efficacious lipases, and strategies to enable improved delivery throughout the digestive process. Standardized, rapid, in vitro test systems to measure the efficacy of such lipases in near physiologic conditions need to be set up for screening and to help create more accurate PERT product labeling.
Supplementation of duodenal bicarbonate
Acidic degradation of exogenous pancreatic lipase and the discrepancy between an optimal pH for enzyme action and the actual intra-duodenal pH in EPI patients are major factors that prevent complete correction of steatorrhea.Citation71 One answer is to increase the local duodenal pH. The use of sodium bicarbonate (1.34 g per test meal) with enteric-coated tablets of pancreatic enzymes combined with desiccated ox bile (50 mg per test meal) considerably improved lipid digestion as measured by breath-test in patients with chronic pancreatitis, without concurrent acid-suppressive therapy.Citation148 More recently, the effect of administering enteric-coated buffered pancrelipase microspheres (Pancrecarb MS-8, Digestive Care Inc, PA, USA) containing 2.5 mEqCitation149 or 1.5 mEqCitation150 of bicarbonate per capsule was tested on CFA in CF patients. In both studies, the number of patients, lipid consumption, stated lipases units/kg per day (about 4400 USP) were similar, and patients were their own controls. A significant increase in CFA (9%) was observed only in the study providing the higher amount of sodium bicarbonate (about 6.9 g daily versus 3.1 g daily).Citation149 The results of these studies are difficult to interpret, as individual responses to the buffered PERT varied widely, probably because CF patients can secrete either normal or high levels of gastric acid postprandially.Citation98,Citation151 As a result, there would be marked individual variability in duodenal pH as a response to the amount of bicarbonate provided.
Alternative sources of lipases
In order to avoid the short half-life of lipolytic enzymes of pancreatic origin for replacement therapy, a variety of lipases have been tested from sources as diverse as animal gastric lipase and microbial or plant lipases.
Supplementation with gastric lipase has been evaluated because of the natural acid-resistant properties and broad pH of action (3 to 6) of the enzyme.Citation51,Citation152 A dog recombinant lipase, rGL, was produced to test this conceptCitation153 and was developed by the French company Meristem Therapeutics SA, Clermont-Ferrand (Merispase), that went out of business in September 2008. This approach is problematic for several reasons: gastric lipase specific activity is about 10 times lower than that of pancreatic lipase (measured on tributyrin);Citation51 it is highly sensitive to trypsin proteolysis;Citation154 and endogenous secretion of gastric lipase can be increased in patients with pancreatic insufficiencyCitation28 because of possible nutritional adaptation.Citation98,Citation155 However, gastric lipase supplements may still be a viable option. Indeed, during gastric lipolysis, endogenous human gastric lipase is rapidly trapped within fatty acid-rich particles generated at the surface of the lipid droplet and is no longer able to access its substrate.Citation156 The addition of an extra dose of gastric lipase through supplementation will allow lipolysis to continue.Citation156 Also, in vivo specific activity of gastric lipase can be close to that of pancreatic lipase especially on a solid food matrix.Citation38 Two clinical trials conducted in CF patients showed that rGL is well tolerated and efficient when administered at the dose of 600 mg alone, or when associated with pancreatic extract (PE) (≥300,000 UPS total per day). This combination led to a significantly increased CFA compared with PE alone (84% vs 71%) in 7 of 11 patients.Citation157 Another study showed that 250 mg rGL combined with a low dose of pancreatic extract led to at least equal CFA compared with a high dose of PE.Citation158 Furthermore, there was a greater benefit in CF patients with low CFA, which also improved quality of life.Citation158
Microbial lipases of fungal or bacterial origin are of potential interest because of their acid and protease-stable properties and their activity at pH 3 to 10. Rhizopus arrhizus,Citation159 Candida cylindacea, Aspergillus niger,Citation160,Citation161 and Yarrowia lipolyticaCitation162,Citation163 are some examples of the most tested fungi. The Aspergillus and Yarrowia species have better survival in the duodenal environment as shown in vitro and in rats, while the others appeared very sensitive to trypsin and to the detergent action of bile salts. Lipases derived from bacteria are more promising as they are highly resistant to both acid and alkaline inactivation, stable in the presence of both proteolytic enzymes and bile salts, and active without the need for bile salts and colipase.Citation164 A novel, experimental type of enzyme supplement containing bacterial lipase, fungal protease, and amylase (TheraCLEC-Total or ALTU-135, Altus Pharmaceuticals, MA, USA) has demonstrated good tolerance and efficacy (20% increase in CFA).Citation164 A Phase II clinical trial showed that a moderate dose (25,000 USP of lipase per meal) resulted in a 35% to 40% increase in the CFA of cystic fibrosis patients with 0% to 40% CFA at baseline, and that a high dose (100,000 USP lipase per meal) was necessary for a 10% increase in the CFA of patients with 41% to 80% baseline CFA, after 1 month’s treatment.Citation165 A 1-year, multi-center, Phase III clinical trial was completed in 2009 (ClinicalTrials.gov NCT00500084) and results are pending.Citation166 Thus, Liprotamase (formerly known as ALTU-135 and Trizytek), for which a pediatric formulation is in progress, is the first porcine-free PERT developed since the end of 2008 (Alnara Pharmaceuticals, MA, USA, acquired by Eli Lilly, IN, USA).Citation167 A better knowledge of the microbial lipases structure and modes of action will probably help to select and design much more active enzymes in the near future.Citation168,Citation169
Plant acid-stable lipase, as in oats,Citation170 and plant latex lipase extracts from euphorbia characias, fruit of babaco, or carica papayaCitation171,Citation172 are potential sources of lipases. At this point, kinetics have been studied only in vitro and scientific data are needed on their digestive function in physiological conditions.
Recombinant human lipases
Recombinant human lipases would be expected to offer superior safety by decreasing the risk of allergic reactions. Progress in protein engineeringCitation173 and a detailed knowledge of human lipasesCitation174 will enable large-scale production and the ability to apply directed mutagenesis if necessary for improving lipase stability and activity in acidic conditions. Of note, the use of recombinant human lipases may be limited by the fact that changes in glycosylation (rates and type) and other post-translational modifications in proteins produced in the non-eukaryotic cell system used for large-scale production may interfere with enzymatic activity.Citation175,Citation176
A promising candidate for the treatment of lipid malabsorption is a recombinant human bile salt-stimulated lipase (rBSSL). This enzyme is naturally acid resistant and able to hydrolyze triglycerides and phospholipids.Citation59 Two preparations dedicated to cystic fibrosis patients and preterm infants, Exinalda and Kiobrina, respectively, are currently under development (Biovitrum AB, Stockholm, Sweden). A Phase I clinical trial was conducted in 9 CF patients with EPI, measuring lipid uptake through breath-test.Citation177 The addition of rBSSL (0.2 or 1 g) to standard pancrelipase (Creon) enabled a dose reduction of pancrelipase to 25% of normal dose.Citation177 Plasma chylomicron level was significantly higher with the addition of rBSSL (34% to 48%), a clear secretion peak being reached at 3 hours after the meal,Citation177 which is similar to the pattern found in normal subjects,Citation30 while no real peak was observed with pancrelipase dosing alone. This can be explained by the ability of BSSL to generate lysophospholipids necessary for an efficient lipid absorption rate by the small intestine,Citation61 and to participate in chylomicron assembly and secretion through its ceramidase activity.Citation14 Another study was conducted through 2009 with Exinalda in 18 CF patients with EPI in Poland and the Netherlands, but the results have not yet been published (ClinicalTrials. gov NCT00743483). Two Phase II clinical trials have been conducted in Italy and France with Kiobrina administered at a dose physiologically found in human milk (0.15 g/L) for 1 week to premature infants in formula (ClinicalTrials.gov NCT00658905) or in pasteurized breast milk (ClinicalTrials.gov NCT00659243), but results are not yet available.
Directional mutagenesis and use of electrostatic computations has also allowed generation of a human pancreatic lipase with modified pH of action (pH 4–5).Citation178 Pancreatic lipase is irreversibly inactivated by gastric acid at a pH of 4.0 and below and its activity is very low at pH 5.0.Citation10 Several variants of the recombinant human pancreatic lipase were generated by error-prone PCR and screened for stability and activity at a pH of 5 in vitro.Citation179 Although these enzymes were more acid stable, their activity on physiologic substrates was not enhanced compared to native human pancreatic lipase.
Delivery system strategies
Bacterial engineering and gene transfer techniques could revolutionize the delivery of pancreatic enzymes by producing the enzymes within the host. Strains of bacteria such as Lactococcus lactis, genetically modified to highly express bacterial lipases, have been derived.Citation180 Colonization of pigs with experimentally induced pancreatic insufficiency with lipase-producing L. lactis demonstrated increased CFA under a high-fat diet.Citation181 The treatment occurs as the bacteria release their cellular content in response to contact with proteolytic secretions and bile acids.Citation181 A gene therapy approach could be envisioned as an alternative therapeutic strategy to improve lipid digestion and absorption in EPI patients by mediating enzyme production by transduced cells within the treated patient. Indeed, the human pancreatic lipase gene has been successfully expressed in the biliary tract in rats using recombinant adenovirus.Citation182
Strategies through substrate physicochemical properties and lipase activators
As an alternative, creating functional dietary lipids that are more effectively digested is another frontier of treatment for pancreatic insufficiency. Triglyceride digestion is more efficient when the substrate is emulsified, ie, dispersed, in aqueous medium as lipid droplets which consist in a core of triglycerides stabilized by a layer of phospholipids or other emulsifiers. The process of emulsification creates a lipid–water interface allowing optimal action of lipases.Citation183 The physicochemical properties of such an interface can modulate the rate of lipolysis.Citation183,Citation184 Thus, structuring food emulsions is a new concept that should improve lipid digestion and absorption in EPI patients by selecting the best lipid physicochemical properties for optimal action of lipases.Citation28,Citation30,Citation185,Citation186
Lipid droplet size is one of the key physicochemical parameters of triglyceride digestion by gastric and pancreatic lipases, as it governs the lipid–water interface area.Citation29,Citation30,Citation155 Droplet size is inversely related to the lipid interface area, and, theoretically, small-sized droplets should be more efficiently digested in the digestive tract offering a larger interface area that will allow the binding of more lipase molecules at the interface. Indeed, it was shown in healthy humans that the triglycerides from small-sized droplets (0.7 μm) are more efficiently digested in the stomach and in the duodenum than from larger droplets.Citation30 Even though this has a potential for health, it has not been tested yet in EPI patients.
Another physicochemical key factor involved in lipid digestion is the ultrastructure, ie, droplet surface layer composition (phospholipid classes, phospholipid fatty acid profile, adsorbed proteins).Citation184 Lipases bind to such a surface layer to access to triglycerides contained in the core of the droplet. The composition of the droplet surface layer plays a key role in vivo as it was shown that native human milk droplets of about 4 μm (three phospholipid layers) were more efficiently lipolyzed in the stomach of premature babies than small-sized droplets (0.5 μm) from a formula (single layer).Citation56 It was shown in vitro that specific classes of phospholipids will prevent pancreatic lipase activity,Citation187 or enhance dramatically gastric lipase, pancreatic lipase, and BSSL activity in conditions that mimic physiology.Citation188,Citation189 Also, the dietary protein interaction within the droplet surface can improve or diminish the triglycerides lipolysis rates.Citation190
A third physicochemical property of lipids that is of particular importance in patients suffering from digestive and absorptive disorders is the triglyceride structure, ie, the nature of fatty acid esterified at positions sn-1, sn-2, and sn-3 of the glycerol backbone.Citation191–Citation194 Indeed, this structure influences digestion, as the lipolysis rate depends on the type of fatty acid present at the sn-1 and sn-3 positions,Citation195 and the lipid droplet size can differ depending on the triglyceride structure.Citation196 Triglyceride structure also affects i) the absorption step, as the fatty acid is better absorbed when it is present as a 2-monoglyceride;Citation193,Citation197,Citation198 ii) the enterocyte re-synthesis step and the secretion of chylomicrons by the enterocyte, as the fatty acid of the sn-2 position is retained in chylomicron lipid particles; and iii) the lipid metabolism.Citation198,Citation199 So, the structure of triglycerides is particularly important to improve absorption of essential and very-long chain fatty acids.Citation193,Citation200 In contrast, absorption of long-chain saturated fatty acids can be dramatically decreased when present at the sn-1 and sn-2 positions of the triglyceride molecule and in the presence of high concentration of calcium or magnesium, because they form insoluble soaps.Citation197 Except for Betapol (Lipid Nutrition, Hogeweg, the Netherlands) used in several milk substitutes because it is a source of structured triglycerides with long-chain saturated fatty acids in sn-2 position, as in human milk,Citation192,Citation193 other kinds of structured triglycerides are not often used, probably because of their cost.Citation193
Functional foods are a new area of research for clinical nutrition. For EPI patients, specific, more digestible or absorbable lipid sources could be designed. The addition of specific phospholipids able to enhance lipase activity in enzyme supplements or in formula would both increase lipase activity and, in parallel, enhance lipid nutrient absorption.
Conclusion
Exocrine pancreatic insufficiency results from a wide range of medical and surgical conditions. PERT is the standard treatment for the resultant malabsorption. Therapy is in general well tolerated and efficacy is satisfactory. Although progress has been made in standardizing therapy and improving enzyme formulations, there is still room to improve in terms of fully resolving the symptoms and malnutrition related to EPI, along with convenient and accurate means for monitoring therapy. In the clinical setting, a basic understanding of the physiology of enzyme delivery assists in choosing, monitoring, and adjusting therapy. Currently the most common monitoring strategy is clinical response, as stool fat and breath testing are cumbersome and less clinically available. Dose adjustments can be made according to the amount of steatorrhea and the patient’s weight loss or gain. The common problem of incomplete response to therapy might also indicate that the mechanism of malabsorption in pancreatic insufficiency is more complex than simply a lack of pancreatic enzymes and electrolyte secretions, and further study in this area is warranted. In the future, with the advent of new technology, we look forward to delivering even better tolerated replacement therapy, which replicates more accurately the function of the native pancreas or delivers nutrition more effectively, and more convenient or available means of monitoring therapy.
Disclosure
The authors declare no conflict of interest.
References
- PezzilliRMorselli LabateAMCeciliatoRQuality of life in patients with chronic pancreatitisDig Liver Dis200537318118915888283
- WhitcombDCLehmanGAVasilevaGPancrelipase delayed-release capsules (CREON) for exocrine pancreatic insufficiency due to chronic pancreatitis or pancreatic surgery: A double-blind randomized trialAm J Gastroenterol2010105102276228620502447
- Fer roneMRaimondoMScolapioJSPancreatic enzyme pharmacotherapyPharmacotherapy200727691092017542772
- YamadaTTextbook of GastroenterologyFourth edLippincott Williams & Wilkins2003
- BrunoMJHaverkortEBTytgatGNvan LeeuwenDJMaldigestion associated with exocrine pancreatic insufficiency: implications of gastrointestinal physiology and properties of enzyme preparations for a cause-related and patient-tailored treatmentAm J Gastroenterol1995909138313937661155
- AdlerGMullenhoffAKoopIStimulation of pancreatic secretion in man by a protease inhibitor (camostate)Eur J Clin Invest1988181981043130267
- BraganzaJMHermanKHinePKayGSandleGIPancreatic enzymes in human duodenal juice–a comparison of responses in secretin pancreozymin and Lundh Borgstrom testsGut1978195358366658764
- EscourrouJFrexinosJRibetABiochemical studies of pancreatic juice collected by duodenal aspiration and endoscopic cannulation of the main pancreatic ductAm J Dig Dis197823217317723675
- BertonASebban-KreuzerCRouvellacSLopezCCrenonIIndividual and combined action of pancreatic lipase and pancreatic lipase-related proteins 1 and 2 on native versus homogenized milk fat globulesMol Nutr Food Res200953121592160219824014
- BorgstromBInfluence of bile salt, pH, and time on the action of pancreatic lipaseJournal of Lipid Research1964552253114221095
- CrenonIFoglizzoEKerfelecBPancreatic lipase-related protein type I: a specialized lipase or an inactive enzymeProtein Eng19981121351429605548
- De CaroJCarrièreFBarboniPGillerTVergerRDe CaroAPancreatic lipase-related protein 1 (PLRP1) is present in the pancreatic juice of several speciesBiochim Biophys Acta199813871–23313419748646
- EydouxCAloulouADe CaroJHuman pancreatic lipase-related protein 2: tissular localization along the digestive tract and quantification in pancreatic juice using a specific ELISABiochim Biophys Acta20061760101497150416887271
- HuiDYHowlesPNCarboxyl ester lipase: structure-function relationship and physiological role in lipoprotein metabolism and atherosclerosisJ Lipid Res200243122017203012454261
- JayneSKerfelecBFoglizzoEChapusCCrenonIHigh expression in adult horse of PLRP2 displaying a low phospholipase activityBiochim Biophys Acta20021594425526511904221
- LoweMEThe triglyceride lipases of the pancreasJ Lipid Res200243122007201612454260
- ReboulEBertonAMoussaMKreuzerCCrenonIBorelPPancreatic lipase and pancreatic lipase-related protein 2, but not pancreatic lipase-related protein 1, hydrolyze retinyl palmitate in physiological conditionsBiochim Biophys Acta20061761141016497549
- SiasBFerratoFGrandvalPHuman pancreatic lipase-related protein 2 is a galactolipaseBiochemistry20044331101381014815287741
- ThirstrupKVergerRCarrièreFEvidence for a pancreatic lipase subfamily with new kinetic propertiesBiochemistry19943310274827568130186
- VerheijMHWestermanJSternbyBde HaasGHThe complete primary structure of phospholipase A2 from human pancreasBiochim Biophys Acta19837471–293996349696
- LoweMEThe structure and function of pancreatic enzymesJohnsonLRAlpersDHChristensenJJacobsonEDWalshJHPhysiology of the Gastrointestinal Tract2New YorkRaven Press199415311542
- LebenthalELeePCDevelopment of functional responses in human exocrine pancreasPediatrics19806645565606159567
- ZoppiGAndreottiGPajno-FerraraFNjaiDMGaburroDExocrine pancreas function in premature and full term neonatesPediatr Res19726128808864678558
- FredrikzonBOlivecronaTDecrease of lipase and esterase activities in intestinal contents of newborn infants during test mealsPediatr Res1978125631634662468
- TrackNSCreutzfeldtCBokermannMEnzymatic, functional and ultrastructural development of the exocrine pancreas–II. The human pancreasComp Biochem Physiol A Comp Physiol1975511A95100236895
- LaugierRBernardJPBerthezenePDupuyPChanges in pancreatic exocrine secretion with age: pancreatic exocrine secretion does decrease in the elderlyDigestion1991503–42022111812045
- KellerJLayerPHuman pancreatic exocrine response to nutrients in health and diseaseGut200554Suppl 6vi1vi2815951527
- ArmandMLipases and lipolysis in the human digestive tract: where do we stand?Curr Opin Clin Nutr Metab Care200710215616417285003
- ArmandMBorelPPasquierBPhysicochemical characteristics of emulsions during fat digestion in human stomach and duodenumAm J Physiol19962711 Pt 1G172G1838760121
- ArmandMPasquierBAndreMDigestion and absorption of 2 fat emulsions with different droplet sizes in the human digestive tractAm J Clin Nutr19997061096110610584056
- SchwizerWAsalKKreissCRole of lipase in the regulation of upper gastrointestinal function in humansAm J Physiol19972733 Pt 1G612G6209316463
- BoivinMLanspaSJZinsmeisterARGoVLDiMagnoEPAre diets associated with different rates of human interdigestive and post-prandial pancreatic enzyme secretion?Gastroenterology1990996176317712227289
- BorovickaJSchwizerWMettrauxCRegulation of gastric and pancreatic lipase secretion by CCK and cholinergic mechanisms in humansAm J Physiol19972732 Pt 1G374G3809277416
- CarrièreFBarrowmanJAVergerRLaugierRSecretion and contribution to lipolysis of gastric and pancreatic lipases during a test meal in humansGastroenterology199310538768888359655
- CarrièreFGrandvalPRenouCQuantitative study of digestive enzyme secretion and gastrointestinal lipolysis in chronic pancreatitisClin Gastroenterol Hepatol200531283815645402
- YagoMDGonzalezMVMartinez-VictoriaEPancreatic enzyme secretion in response to test meals differing in the quality of dietary fat (olive and sunflowerseed oils) in human subjectsBr J Nutr199778127399292757
- LayerPKellerJPancreatic enzymes: secretion and luminal nutrient digestion in health and diseaseJ Clin Gastroenterol19992813109916657
- CarrièreFRenouCLopezVThe specific activities of human digestive lipases measured from the in vivo and in vitro lipolysis of test mealsGastroenterology2000119494996011040182
- KellerJRunziMGoebellHLayerPDuodenal and ileal nutrient deliveries regulate human intestinal motor and pancreatic responses to a mealAm J Physiol19972723 Pt 1G632G6379124585
- MoreauHSaunièreJFGargouriYPieroniGVergerRSarlesHHuman gastric lipase: variations induced by gastrointestinal hormones and by pathologyScand J Gastroenterol1988239104410483247586
- PalascianoGSaunièresJFLaugierRSarlesHPancreatic response to secretin+CCK-PZ in European and North African adults and childrenGut1979201210631065527879
- BoehmGBorteMMullerHMoroGMinoliIActivities of trypsin and lipase in duodenal aspirates of preterm infants: influence of dietary protein and fat compositionAm J Clin Nutr19956135245277872215
- MottCSarlesHTiscorniaOGulloLInhibitory action of alcohol on human exocrine pancreatic secretionAm J Dig Dis197217109029105073678
- BozkurtTAdlerGKoopIKoopHTurmerWArnoldRPlasma CCK levels in patients with pancreatic insufficiencyDig Dis Sci19883332762813342719
- Nouri-SorkhabiMHChapmanBEKuchelPWGrucaMAGaskinKJParallel secretion of pancreatic phospholipase A(2), phospholipase A(1), lipase, and colipase in children with exocrine pancreatic dysfunctionPediatr Res200048673574011102539
- ArmandMMilk fat digestibilitySciences des Aliments2008281–28498
- MattesRDFat taste and lipid metabolism in humansPhysiol Behav200586569169716249011
- SarlesHDaniRPrezelinGSouvilleCFigarellaCCephalic phase of pancreatic secretion in manGut1968922142215655031
- SolomonTControl of exocrine pancreas secretionLRJPhysiology of the Gastrointestinal Tract2New YorkRaven Press199414991529
- AlpersDDigestion and absorption of carbohydrates and proteinsLRJPhysiology of the Gastrointestinal Tract2New YorkRaven Press199417231749
- HamoshMLingual and gastric lipasesNutrition1990664214282134569
- MacGregorIParentJMeyerJHGastric emptying of liquid meals and pancreatic and biliary secretion after subtotal gastrectomy or truncal vagotomy and pyloroplasty in manGastroenterology1977722195205830568
- MayerEAThompsonJBJehnDReedyTElashoffJMeyerJHGastric emptying and sieving of solid food and pancreatic and biliary secretion after solid meals in patients with truncal vagotomy and antrectomyGastroenterology1982831 Pt 21841926919504
- CheyWYChangTNeural hormonal regulation of exocrine pancreatic secretionPancreatology20011432033512120211
- ArmandMBorelPDuboisCCharacterization of emulsions and lipolysis of dietary lipids in the human stomachAm J Physiol19942663 Pt 1G372G3818166277
- ArmandMHamoshMMehtaNREffect of human milk or formula on gastric function and fat digestion in the premature infantPediatr Res19964034294378865280
- BordaloOGoncalvesDNoronhaMCristinaMLSalgadinhoADreilingDANewer concept for the pathogenesis of chronic alcoholic pancreatitisAm J Gastroenterol1977683278285596358
- DahimMBrockmanHHow colipase-fatty acid interactions mediate adsorption of pancreatic lipase to interfacesBiochemistry19983723836983779622488
- LindquistSHernellOLipid digestion and absorption in early life: an updateCurr Opin Clin Nutr Metab Care201013331432020179589
- LoweMEKaplanMHJackson-GrusbyLD’AgostinoDGrusbyMJDecreased neonatal dietary fat absorption and T cell cytotoxicity in pancreatic lipase-related protein 2-deficient miceJ Biol Chem19982734731215312219813028
- TsoPIntestinal lipid absorptionLRJPhysiology of the Gastrointestinal Tract2New YorkRaven Press199418671908
- HernellOStaggersJECareyMCPhysical-chemical behavior of dietary and biliary lipids during intestinal digestion and absorption. 2. Phase analysis and aggregation states of luminal lipids during duodenal fat digestion in healthy adult human beingsBiochemistry1990298204120562328238
- MuHHoyCEThe digestion of dietary triacylglycerolsProg Lipid Res200443210513314654090
- LayerPYamamotoHKalthoffLClainJEBakkenLJDiMagnoEPThe different courses of early- and late-onset idiopathic and alcoholic chronic pancreatitisGastroenterology19941075148114877926511
- RobertsIMPoturichCWaldAUtility of fecal fat concentrations as screening test in pancreatic insufficiencyDig Dis Sci19863110102110243757718
- FineKDSchillerLRAGA technical review on the evaluation and management of chronic diarrheaGastroenterology199911661464148610348832
- EwaldNRaspeAKaufmannCBretzelRGKloerHUHardtPDDeterminants of exocrine pancreatic function as measured by fecal elastase-1 concentrations (FEC) in patients with diabetes mellitusEur J Med Res200914311812219380282
- NaruseSIshiguroHKoSBFecal pancreatic elastase: a reproducible marker for severe exocrine pancreatic insufficiencyJ Gastroenterol200641990190817048055
- HahnJUKernerWMaisonneuvePLowenfelsABLankischPGLow fecal elastase 1 levels do not indicate exocrine pancreatic insufficiency in type-1 diabetes mellitusPancreas200836327427818362841
- LankischPGSchmidtIKonigHFaecal elastase 1: not helpful in diagnosing chronic pancreatitis associated with mild to moderate exocrine pancreatic insufficiencyGut19984245515549616319
- LayerPKellerJLipase supplementation therapy: standards, alternatives, and perspectivesPancreas20032611712499909
- Dominguez-MunozJEPancreatic enzyme therapy for pancreatic exocrine insufficiencyCurr Gastroenterol Rep20079211612217418056
- MontaltoGSoresiMCarroccioALipoproteins and chronic pancreatitisPancreas1994911371388108368
- PezzilliRChronic pancreatitis: maldigestion, intestinal ecology and intestinal inflammationWorld J Gastroenterol200915141673167619360910
- GielkensHAEddesEHVechtJvan OostayenJALamersCBMascleeAAGallbladder motility and cholecystokinin secretion in chronic pancreatitis: relationship with exocrine pancreatic functionJ Hepatol19972723063129288605
- KrishnamurtyDMRabieeAJagannathSBAndersenDKDelayed release pancrelipase for treatment of pancreatic exocrine insufficiency associated with chronic pancreatitisTher Clin Risk Manag20095350752019707261
- LongWBWeissJBRapid gastric emptying of fatty meals in pancreatic insufficiencyGastroenterology19746759209254609827
- MizushimaTOchiKIchimuraMKiuraKHaradaHKoideNPancreatic enzyme supplement improves dysmotility in chronic pancreatitis patientsJ Gastroenterol Hepatol20041991005100915304117
- NustedeRKohlerHFolschURSchafmayerAPlasma concentrations of neurotensin and CCK in patients with chronic pancreatitis with and without enzyme substitutionPancreas1991632602651713670
- VuMKVechtJEddesEHBiemondILamersCBMascleeAAAntroduodenal motility in chronic pancreatitis: are abnormalities related to exocrine insufficiency?Am J Physiol Gastrointest Liver Physiol20002783G458G46610712266
- CzakoLHegyiPRakonczayZJrWittmannTOtsukiMInteractions between the endocrine and exocrine pancreas and their clinical relevancePancreatology20099435135919454837
- BragelmannRArmbrechtURosemeyerDSchneiderBZillyWStockbruggerRWThe effect of pancreatic enzyme supplementation in patients with steatorrhoea after total gastrectomyEur J Gastroenterol Hepatol199911323123710333193
- CreutzfeldtWGleichmannDOttoJStockmannFMaisonneuvePLankischPGFollow-up of exocrine pancreatic function in type-1 diabetes mellitusDigestion2005722–3717516113545
- LankischPGMantheyGOttoJExocrine pancreatic function in insulin-dependent diabetes mellitusDigestion19822532112166186557
- HardtPDHauenschildANalopJHigh prevalence of exocrine pancreatic insufficiency in diabetes mellitus. A multicenter study screening fecal elastase 1 concentrations in 1,021 diabetic patientsPancreatology20033539540214526149
- SarlesHEtiopathogenesis and definition of chronic pancreatitisDig Dis Sci1986319 Suppl91S107S3525051
- SarlesHBernardJPGulloLPathogenesis of chronic pancreatitisGut19903166296322199345
- ComfortMWGambrillEEBaggenstossAHChronic relapsing pancreatitis. A study of twenty-nine cases without associated disease of the biliary or gastro-intestinal tractGastroenterology196854(4) Suppl7607655659821
- KloppelGMailletBChronic pancreatitis: evolution of the diseaseHepatogastroenterology19913854084121765357
- BraganzaJMPancreatic disease: a casualty of hepatic “detoxification”?Lancet198328357100010036138545
- EkstromGIngelman-SundbergMRat liver microsomal NADPH-supported oxidase activity and lipid peroxidation dependent on ethanol-inducible cytochrome P-450 (P-450IIE1)Biochem Pharmacol1989388131313192495801
- MarshallWJMcLeanAEA requirement for dietary lipids for induction of cytochrome P-450 by phenobarbitone in rat liver microsomal fractionBiochem J197112245695735123890
- CavalliniGIs chronic pancreatitis a primary disease of the pancreatic ducts? A new pathogenetic hypothesisItal J Gastroenterol19932573913968280902
- DiMagnoMJDiMagnoEPChronic pancreatitisCurr Opin Gastroenterol200521554455416093768
- StevensTConwellDLZuccaroGPathogenesis of chronic pancreatitis: an evidence-based review of past theories and recent developmentsAm J Gastroenterol200499112256227015555009
- WilschanskiMDuriePRPatterns of GI disease in adulthood associated with mutations in the CFTR geneGut20075681153116317446304
- ArmandMHamoshMPhilpottJRGastric function in children with cystic fibrosis: effect of diet on gastric lipase levels and fat digestionPediatr Res200455345746514681491
- AndersenJRBendtsenFOvesenLPedersenNTRuneSJTage-JensenUPancreatic insufficiency. Duodenal and jejunal pH, bile acid activity, and micellar lipid solubilizationInt J Pancreatol1990642632702212745
- DuttaSKRussellRMIberFLInfluence of exocrine pancreatic insufficiency on the intraluminal pH of the proximal small intestineDig Dis Sci197924752953437059
- DuttaSKRussellRMIberFLImpaired acid neutralization in the duodenum in pancreatic insufficiencyDig Dis Sci1979241077578039715
- BrunoMJRauwsEAHoekFJTytgatGNComparative effects of adjuvant cimetidine and omeprazole during pancreatic enzyme replacement therapyDig Dis Sci19943959889928174440
- ChauhanSForsmarkCEPain management in chronic pancreatitis: A treatment algorithmBest Pract Res Clin Gastroenterol201024332333520510832
- MassicotteLPBailleWEMateescuMACarboxylated high amylose starch as pharmaceutical excipients. Structural insights and formulation of pancreatic enzymesInt J Pharm20083561–221222318403141
- NaikwadeSRMeshramRNBajajANPreparation and in vivo efficacy study of pancreatin microparticles as an enzyme replacement therapy for pancreatitisDrug Dev Ind Pharm200935441743218850362
- RobinsonPJSmithALSlyPDDuodenal pH in cystic fibrosis and its relationship to fat malabsorptionDig Dis Sci19903510129913042120019
- AloulouAPuccinelliDSarlesJLaugierRLeblondYCarrièreFIn vitro comparative study of three pancreatic enzyme preparations: dissolution profiles, active enzyme release and acid stabilityAliment Pharmacol Ther200827328329217973644
- KraisingerMHochhausGStecenkoABowserEHendelesLClinical pharmacology of pancreatic enzymes in patients with cystic fibrosis and in vitro performance of microencapsulated formulationsJ Clin Pharmacol19943421581668163716
- CaseCLHennigesFBarkinJSEnzyme content and acid stability of enteric-coated pancreatic enzyme products in vitroPancreas200530218018315714141
- MeyerJHElashoffJPorter-FinkVDressmanJAmidonGLHuman postprandial gastric emptying of 1–3-millimeter spheresGastroenterology1988946131513253360258
- MeyerJHLakeRMismatch of duodenal deliveries of dietary fat and pancreatin from enterically coated microspheresPancreas19971532262359336785
- HendelesLDorfAStecenkoAWeinbergerMTreatment failure after substitution of generic pancrelipase capsules. Correlation with in vitro lipase activityJAMA199026318245924612329633
- TraynorKFDA approves third pancrelipase product: Unapproved products illegal to market after April 28Am J Health Syst Pharm2010671077620479094
- GraffGRMaguinessKMcNamaraJEfficacy and tolerability of a new formulation of pancrelipase delayed-release capsules in children aged 7 to 11 years with exocrine pancreatic insufficiency and cystic fibrosis: a multicenter, randomized, double-blind, placebo-controlled, two-period crossover, superiority studyClin Ther20103218910320171415
- GraffGRMcNamaraJRoyallJCarasSForssmannKSafety and tolerability of a new formulation of pancrelipase delayed-release capsules (CREON) in children under seven years of age with exocrine pancreatic insufficiency due to cystic fibrosis: an open-label, multicentre, single-treatment-arm studyClin Drug Investig2010306351364
- TrapnellBCMaguinessKGraffGRBoydDBeckmannKCarasSEfficacy and safety of Creon 24,000 in subjects with exocrine pancreatic insufficiency due to cystic fibrosisJ Cyst Fibros20098637037719815466
- WooldridgeJLHeubiJEAmaro-GalvezREUR-1008 pancreatic enzyme replacement is safe and effective in patients with cystic fibrosis and pancreatic insufficiencyJ Cyst Fibros20098640541719683970
- LohrJMHummelFMPirilisKTSteinkampGKornerAHennigesFProperties of different pancreatin preparations used in pancreatic exocrine insufficiencyEur J Gastroenterol Hepatol20092191024103119352190
- WaltersMPLittlewoodJMPancreatin preparations used in the treatment of cystic fibrosis – lipase content and in vitro releaseAliment Pharmacol Ther19961034334408791974
- KolbelCLayerPHotzJGoebellHEffect of an acid protected, microencapsulated pancreatin preparation on pancreatogenic steatorrheaMed Klin (Munich)198681385863641037
- Dominguez-MunozJEIglesias-GarciaJIglesias-ReyMFigueirasAVilarino-InsuaMEffect of the administration schedule on the therapeutic efficacy of oral pancreatic enzyme supplements in patients with exocrine pancreatic insufficiency: a randomized, three-way crossover studyAliment Pharmacol Ther2005218993100015813835
- O’KeefeSJCariemAKLevyMThe exacerbation of pancreatic endocrine dysfunction by potent pancreatic exocrine supplements in patients with chronic pancreatitisJ Clin Gastroenterol200132431932311276275
- SafdiMBekalPKMartinSSaeedZABurtonFToskesPPThe effects of oral pancreatic enzymes (Creon 10 capsule) on steatorrhea: a multicenter, placebo-controlled, parallel group trial in subjects with chronic pancreatitisPancreas200633215616216868481
- SternRCEisenbergJDWagenerJSA comparison of the efficacy and tolerance of pancrelipase and placebo in the treatment of steatorrhea in cystic fibrosis patients with clinical exocrine pancreatic insufficiencyAm J Gastroenterol20009581932193810950038
- BakerSSDelayed release pancrelipase for the treatment of pancreatic exocrine insufficiency associated with cystic fibrosisTher Clin Risk Manag2008451079108419209287
- BakerSSBorowitzDDuffyLFitzpatrickLGyamfiJBakerRDPancreatic enzyme therapy and clinical outcomes in patients with cystic fibrosisJ Pediatr2005146218919315689904
- Dominguez-MunozJEIglesias-GarciaJOral pancreatic enzyme substitution therapy in chronic pancreatitis: is clinical response an appropriate marker for evaluation of therapeutic efficacy?JOP201011215816220208327
- LembckeBBradenBCasparyWFExocrine pancreatic insufficiency: accuracy and clinical value of the uniformLy labelled 13C-Hiolein breath testGut19963956686749026480
- RitzMAFraserRJDi MatteoACEvaluation of the 13C-triolein breath test for fat malabsorption in adult patients with cystic fibrosisJ Gastroenterol Hepatol200419444845315012784
- VentrucciMCipollaAUbalducciGMRodaARodaE13C labelled cholesteryl octanoate breath test for assessing pancreatic exocrine insufficiencyGut199842181879505890
- VantrappenGRRutgeertsPJGhoosYFHieleMIMixed triglyceride breath test: a noninvasive test of pancreatic lipase activity in the duodenumGastroenterology1989964112611342494097
- NakamuraHMorifujiMMurakamiYUsefulness of a 13C-labeled mixed triglyceride breath test for assessing pancreatic exocrine function after pancreatic surgerySurgery2009145216817519167971
- Dominguez-MunozJEIglesias-GarciaJVilarino-InsuaMIglesias-ReyM13C-mixed triglyceride breath test to assess oral enzyme substitution therapy in patients with chronic pancreatitisClin Gastroenterol Hepatol20075448448817445754
- ColomboCFredellaCRussoMCEfficacy and tolerability of Creon for Children in infants and toddlers with pancreatic exocrine insufficiency caused by cystic fibrosis: an open-label, single-arm, multicenter studyPancreas200938669369919531972
- ShafiqNRanaSBhasinDPancreatic enzymes for chronic pancreatitisCochrane Database Syst Rev20094CD00630219821359
- StapletonFBKennedyJNousia-ArvanitakisSLinshawMAHyperuricosuria due to high-dose pancreatic extract therapy in cystic fibrosisN Engl J Med19762955246248934188
- HauserRDutySGodfrey-BaileyLCalafatAMMedications as a source of human exposure to phthalatesEnviron Health Perspect2004112675175315121520
- FitzSimmonsSCBurkhartGABorowitzDHigh-dose pancreatic-enzyme supplements and fibrosing colonopathy in children with cystic fibrosisN Engl J Med199733618128312899113931
- BansiDSPriceARussellCSarnerMFibrosing colonopathy in an adult owing to over use of pancreatic enzyme supplementsGut200046228328510644326
- Van VelzenDBallLMDezfulianARSouthgateAHowardCVComparative and experimental pathology of fibrosing colonopathyPostgrad Med J199672Suppl 2S39S48 discussionS49S518869182
- SmythRLAshbyDO’HeaUFibrosing colonopathy in cystic fibrosis: results of a case-control studyLancet19953468985124712517475715
- PrescottPBakowskiMTPathogenesis of fibrosing colonopathy: the role of methacrylic acid copolymerPharmacoepidemiol Drug Saf19998637738415073899
- PrescottPPancreatic enzymes and fibrosing colonopathyLancet19993549174250 author reply25110421323
- GaiaESambatoroADe GiuliPAngeliAAdult f ibrosing colonopathy associated with mesalazine treatmentAm J Gastroenterol20019682508250911513205
- ReganPTMalageladaJRDimagnoEPGoVLRationale for the use of cimetidine in pancreatic insufficiencyMayo Clin Proc19785327983340805
- DuriePRBellLLintonWCoreyMLForstnerGGEffect of cimetidine and sodium bicarbonate on pancreatic replacement therapy in cystic fibrosisGut19802197787867429342
- CarroccioAPardoFMontaltoGUse of famotidine in severe exocrine pancreatic insufficiency with persistent maldigestion on enzymatic replacement therapy. A long-term study in cystic fibrosisDig Dis Sci1992379144114461505293
- VechtJSymerskyTLamersCBMascleeAAEfficacy of lower than standard doses of pancreatic enzyme supplementation therapy during acid inhibition in patients with pancreatic exocrine insufficiencyJ Clin Gastroenterol200640872172516940886
- VukovicMJojicNEffect of enteric coated sodium bicarbonate, enzymes and bile combination on the absorption of fat in chronic pancreatitisAnn Gastroenterol2000132113117
- BradyMSGarsonJLKrugSKAn enteric-coated high-buffered pancrelipase reduces steatorrhea in patients with cystic fibrosis: a prospective, randomized studyJ Am Diet Assoc200610681181118616863712
- KalninsDEllisLCoreyMEnteric-coated pancreatic enzyme with bicarbonate is equal to standard enteric-coated enzyme in treating malabsorption in cystic fibrosisJ Pediatr Gastroenterol Nutr200642325626116540792
- BarracloughMTaylorCJTwenty-four hour ambulatory gastric and duodenal pH profiles in cystic fibrosis: effect of duodenal hyperacidity on pancreatic enzyme function and fat absorptionJ Pediatr Gastroenterol Nutr199623145508811523
- AloulouACarrièreFGastric lipase: an extremophilic interfacial enzyme with medical applicationsCell Mol Life Sci200865685185418213443
- GruberVBernaPArnaudTLarge-scale production of a therapeutic protein in transgenic tobacco plants: effect of subcellular targeting on quality of a recombinant dog gastric lipaseMol Breed20017329340
- BernbackSBlackbergLHuman gastric lipase. The N-terminal tetrapeptide is essential for lipid binding and lipase activityEur J Biochem198918234954992753032
- ArmandMHamoshMDiPalmaJSDietary fat modulates gastric lipase activity in healthy humansAm J Clin Nutr199562174807598069
- PafumiYLaironDde la PortePLMechanisms of inhibition of triacylglycerol hydrolysis by human gastric lipaseJ Biol Chem200227731280702807911940604
- LenoirGRKnoopCDurieuIEfficacy and safety of a recombinant gastric lipase produced in corn for the treatment of fat malabsorption in cystic fibrosis. [abstract]Pediatr Pulmonol2006Suppl 29293
- LenoirGDubrayCChironRRecombinant gastric lipase (RGL) for the treatment of fat malabsorption. [abstract]Pediatr Pulmonol2008Suppl 31306
- MoreauJBouissonMSaint-Marc-GirardinMFPignalFBommelaerGRibetAComparison of fungal lipase and pancreatic lipase in exocrine pancreatic insufficiency in man. Study of their in vitro properties and intraduodenal bioavailabilityGastroenterol Clin Biol198812117877923220231
- GriffinSMAldersonDFarndonJRAcid resistant lipase as replacement therapy in chronic pancreatic exocrine insufficiency: a study in dogsGut1989307101210152759481
- Zentler-MunroPLAssoufiBABalasubramanianKTherapeutic potential and clinical efficacy of acid-resistant fungal lipase in the treatment of pancreatic steatorrhoea due to cystic fibrosisPancreas1992733113191594552
- AloulouAPuccinelliDDe CaroALeblondYCarrièreFA comparative study on two fungal lipases from Thermomyces lanuginosus and Yarrowia lipolytica shows the combined effects of detergents and pH on lipase absorption and activityBiochim Biophys Acta20071771121446145618022403
- TurkiSAyedAChalghoumiNWeekersFThonartPKallelHAn enhanced process for the production of a highly purif ied extracellular lipase in the non-conventional yeast Yarrowia lipolyticaAppl Biochem Biotechnol201016051371138519333561
- BorowitzDGossCHLimauroSStudy of a novel pancreatic enzyme replacement therapy in pancreatic insufficient subjects with cystic fibrosisJ Pediatr2006149565866217095338
- BorowitzDGossCHStevensCSafety and preliminary clinical activity of a novel pancreatic enzyme preparation in pancreatic insufficient cystic fibrosis patientsPancreas200632325826316628080
- BorowitzDFalzoneRPFratazziCA phase 3 study of the efficacy and safety of ALTU-135 (Trizytek) for treatment of pancreatic insufficiency in CF. [abstract]Pediatr Pulmonol2008Suppl 31423
- AldridgeSLilly snaps up AlnaraNat Biotechnol201028882
- HasanFShahAAHameedAMethods for detection and characterization of lipases: A comprehensive reviewBiotechnol Adv200927678279819539743
- MalaJGTakeuchiSUnderstanding structural features of microbial lipases–an overviewAnal Chem Insights2008391919609386
- TursiJMPhairPGBarnesGLPlant sources of acid stable lipases: potential therapy for cystic fibrosisJ Paediatr Child Health19943065395437865271
- CambonERodriguezJAPinaMCharacterization of typo-, regio-, and stereo-selectivities of babaco latex lipase in aqueous and organic mediaBiotechnol Lett200830476977418038267
- MoulinATeissereMBernardCPieroniGLipases of the euphorbiaceae family: purification of a lipase from Euphorbia characias latex and structure-function relationships with the B chain of ricinProc Natl Acad Sci U S A1994912411328113327972058
- QuianZFieldsCJYuYLutzSRecent progress in engineering alpha/beta hydrolase-fold family membersBiotechnol J20072219220017183507
- AloulouARodriguezJAFernandezSExploring the specific features of interfacial enzymology based on lipase studiesBiochim Biophys Acta200617619995101316931141
- MertenOWMattanovichDLangCRecombinant Protein Production with Prokaryotic and Eukaryotic Cells. A Comparative View on Host PhysiologyThe NetherlandsKluwer Academic Publishers2001
- VitaleAPedrazziniERecombinant pharmaceuticals from plants: the plant endomembrane system as bioreactorMol Interv20055421622516123536
- StrandvikBHanssonLHernellORecombinant human bile salt-stimulates lipase improves lipid uptake and reduces the pancreatic enzyme supplementation in patients with cystic fibrosis. [abstract]Pediatr Pulmonol2004Suppl 27333
- Neves-PetersenMTPetersenEIFojanPNoronhaMMadsenRGPetersenSBEngineering the pH-optimum of a triglyceride lipase: from predictions based on electrostatic computations to experimental resultsJ Biotechnol200187322525411334666
- ColinDYDeprez-BeauclairPSilvaNInfantesLKerfelecBModification of pancreatic lipase properties by directed molecular evolutionProtein Eng Des Sel201023536537320150178
- DrouaultSCorthierGEhrlichSDRenaultPExpression of the Staphylococcus hyicus lipase in Lactococcus lactisAppl Environ Microbiol200066258859810653722
- DrouaultSJusteCMarteauPRenaultPCorthierGOral treatment with Lactococcus lactis expressing Staphylococcus hyicus lipase enhances lipid digestion in pigs with induced pancreatic insufficiencyAppl Environ Microbiol20026863166316812039786
- KuhelDGZhengSTsoPHuiDYAdenovirus-mediated human pancreatic lipase gene transfer to rat bile: gene therapy of fat malabsorptionAm J Physiol Gastrointest Liver Physiol20002795G1031G103611053001
- BrockmanHGeneral Features of Lipolysis: Reaction Scheme, Interfacial Structure and Experimental ApproachesElsevier1984
- FavéGCosteTCArmandMPhysicochemical properties of lipids: new strategies to manage fatty acid bioavailabilityCell Mol Biol (Noisy-le-grand)200450781583115672466
- GoldingMWoosterTJThe influence of emulsion structure and stability on lipid digestionCurr Opin Colloid Interface Sci20101590101
- SinghHYeAHorneDStructuring food emulsions in the gastrointestinal tract to modify lipid digestionProg Lipid Res20094829210019116160
- TsuzukiWUeANagaoAEndoMAbeMInhibitory effect of lysophosatidylcholine on pancreatic lipase-mediated hydrolysis in lipid emulsionBiochim Biophys Acta200416841–31715450204
- ArmandMPieroniG Inventors; Innovation Santé des Lipides (I.S.L.)/I.N.S.E.R.M., assignee. Foodstuff composition to improve digestibility of Foodstuff lipids. French patent WO 2009/037398, International Application No.: PCT/FR2008/001062.
- FavéGLévêqueCPeyrotJPieroniGCosteTCArmandMModulation of gastric lipolysis by the phospholipid specie: link to specific lipase-phospholipid interaction at the lipid/water interface? [abstract]FASEB Journal200721 A1010-a.
- MunSDeckerEAMcClementsDJInfluence of emulsifier type on in vitro digestibility of lipid droplets by pancreatic lipaseFood Res Intern2007406770781
- HubbardVSMcKennaMCAbsorption of safflower oil and structured lipid preparations in patients with cystic fibrosisLipids19872264244283613873
- LucasAQuinlanPAbramsSRyanSMeahSLucasPJRandomised controlled trial of a synthetic triglyceride milk formula for preterm infantsArch Dis Child Fetal Neonatal Ed1997773F178F1849462186
- MuHPorsgaardTThe metabolism of structured triacylglycerolsProg Lipid Res200544643044816269186
- TsoPLeeTDemicheleSJLymphatic absorption of structured triglycerides vs physical mix in a rat model of fat malabsorptionAm J Physiol19992772 Pt 1G333G34010444447
- JandacekRJWhitesideJAHolcombeBNVolpenheinRATaulbeeJDThe rapid hydrolysis and efficient absorption of triglycerides with octanoic acid in the 1 and 3 positions and long-chain fatty acid in the 2 positionAm J Clin Nutr19874559409453578095
- KimuraMShizukiMMiyoshiKRelationship between the molecular structures and emulsification properties of edible oilsBiosci Biotechnol Biochem19945812581261
- BraccoUEffect of triglyceride structure on fat absorptionAm J Clin Nutr1994606 Suppl1002S1009S7977140
- InnisSMDyerRALienELFormula containing randomized fats with palmitic acid (16:0) in the 2-position increases 16:0 in the 2-position of plasma and chylomicron triglycerides in formula-fed piglets to levels approaching those of piglets fed sow’s milkJ Nutr19971277136213709202092
- KritchevskyDFatty acids, triglyceride structure, and lipid metabolismJ Nutr Biochem1995127713621370
- ChristensenMSHoyCEBeckerCCRedgraveTGIntestinal absorption and lymphatic transport of eicosapentaenoic (EPA), docosahexaenoic (DHA), and decanoic acids: dependence on intramolecular triacylglycerol structureAm J Clin Nutr199561156617825539