
Abstract
Enterolithiasis, also known as gastro-intestinal concretions, is an uncommon medical disorder that arises from intestinal stasis. Enteroliths are commonly caused by tuberculosis-related constriction and arise from intestinal diverticula. Small bowel obstruction caused by an enterolith is extremely uncommon and might be difficult to diagnose. The mortality rate of uncomplicated enterolithiasis is relatively low, but it rises to 3% in patients who have background comorbid illness, have significant bowel obstruction, and are diagnosed late. We present a rare case of an uncomplicated partial intestinal obstruction caused by an enterolith in an elderly male patient with small bowel diverticular disease who was treated nonoperatively and did not develop further symptoms in the six-month follow-up and discuss the difficulty in diagnosis and its management.
Introduction
Enterolithiasis is an uncommon pathological condition in which calculi or concretion formation occurs in the intestines and has a prevalence ranging from 0.3 to 10%.Citation1 The mortality rate for uncomplicated primary enterolithiasis is very low, but it rises to 3% in poorly conditioned patients with significant obstruction and a late diagnosis. Enteroliths can cause bowel obstruction, haemorrhage, or perforation, but the vast majority are cleared asymptomatically. Although one-third of enteroliths are radiolucent, a CT scan of the abdomen can detect radiolucent stones as well as their underlying bowel pathology. If nonoperative therapeutic management fails, surgical exploration is indicated.Citation2 We present a case of small bowel diverticular disease with primary enterolith formation resulting in symptoms of partial bowel obstruction that were relieved spontaneously with the passage of the enterolith and highlight the rarity of the condition, which should be considered in elderly patients with sudden onset of intestinal obstruction. Written informed consent was obtained from the patient for the publication of this report and accompanying images.
Case Presentation
A 72-year-old man with diabetes mellitus and hypertension, both controlled on medication, presented to the emergency department with a 7-day history of diffuse central abdominal pain that was gradual in onset and was followed by abdominal distention and vomiting. He gave a history of constipation for 7 days for which he was being treated non-operatively in an outside medical facility for 5 days. But for the last 2 days, he started passing flatus infrequently, and abdominal distention and vomiting had also decreased. He denied any prior history of similar complaints or abdominal surgery. He was afebrile; his heart rate was 88/minute; his blood pressure was 100/72 mmHg; his respiratory rate was 22/minute, and his oxygen saturation was 98% in room air. His abdomen was distended but was soft and non-tender on palpation. Intestinal sounds were present, although sluggish. His haematological and biochemical investigations were unremarkable.
Dilated small bowel loops were observed in the abdominal X-rays. A contrast-enhanced computed tomography (CECT) scan of the abdomen with oral negative contrast revealed multiple dilated small bowel loops measuring 4 cm in maximum calibre with air-fluid levels and a suspected transition zone at mid/distal jejunal loops along with an enterolith measuring 1.5×2.2 cm floating in the bowel lumen near the transition zone (). Multiple small intestinal diverticula were also noted. There were, however, no pneumobilia or gallstones, and the gallbladder was unremarkable. A diagnosis of partial small bowel obstruction due to an enterolith arising out of small bowel diverticulosis was made, and he was admitted and treated with intravenous crystalloids, analgesics, and a liquid diet as tolerated. He passed stool after one day of non-operative management, and his abdominal distention and vomiting abated in the next two days, following which he was discharged. Interestingly, a repeat CECT scan of the abdomen after one month of follow-up did not reveal any enterolith, indicating its spontaneous passage. A follow-up barium meal follow-through did not reveal any bowel stenosis, but multiple jejunal and ileal diverticulosis were noted ().
Figure 1 CT scan of the abdomen showing enterolith in a dilated small bowel segment (yellow arrowhead). Multiple small bowel diverticula are also seen (red arrowhead).
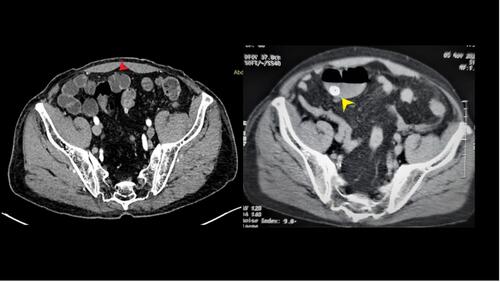
Figure 2 Barium meal follow-through in the follow-up period indicates no evidence of bowel obstruction and absence of enterolith. Multiple small bowel diverticula are noted (Orange arrowhead).

Discussion
Enterolithiasis (gastro-intestinal concretions) is primarily an adult disease. Enteroliths range in size and number from a few millimetres to a few centimetres. They can manifest as a single stone, a cluster of concretions, or a disseminated pan-intestinal pattern. It is divided into two categories: primary and secondary.Citation1 Primary enteroliths form in the gastrointestinal tract, usually within an abnormal pouch such as a diverticulum, and are further classified as “true” or “false.” The presence of diverticular disease, altered luminal propagation, and peristaltic function, as well as luminal pH and the microenvironment specific to each segment of the gut, are important factors in developing conditions necessary for stone formation. True primary enteroliths are formed from chemical elements that are already present in the bowel in anatomically compromised areas of stasis, and their composition can vary depending on the location.Citation2 Cholic acid enteroliths require a lower pH and are typically found in the proximal small intestine. Diverticular disease, strictures, and low luminal pH facilitate calculus formation.Citation3 Interestingly, primary enteroliths made of calcium phosphate, calcium oxalate, and calcium carbonate are found in the distal small bowel (terminal ileum) as these salts require alkaline pH to precipitate.Citation4 Diverticular diseases of the intestine predispose to enterolith formation. While duodenal diverticulosis occurs in up to 22% of the adult population, ileo-jejunal diverticular disease is uncommonly present with an estimated prevalence of less than 5%.Citation5 The clinical presentation of enterolithiasis includes abdominal pain, distention, nausea, and vomiting that can be sudden or insidious as a result of the enterolith tumbling through the bowel lumen and giving rise to incomplete but recurrent obstruction.Citation5
Secondary-type enteroliths form outside of the gastrointestinal tract proper and then migrate into the bowel, causing an obstruction. The most common type is a gallstone, which reaches the gastrointestinal tract through a cholecysto-duodenal or cholecysto-jejunal fistula. The resultant gallstone ileus accounts for less than 5% of mechanical small bowel obstructions. It is rare and develops in less than 0.5% of patients with gallbladder calculus. The patients may have nonspecific symptoms initially but later may manifest features of intestinal obstruction. Since in the beginning, the symptoms may be nonspecific and intermittent abdominal pain, and the X-ray investigations may fail to identify the cause of the obstruction, the diagnosis of intestinal obstruction due to a gallstone may be delayed, and sometimes the diagnosis is made during surgery.Citation6 The majority of reported cases of obstruction demonstrate a gallstone larger than 20 mm in diameter. The distal ileum (60%) is the most common site of obstruction, followed by the jejunum (15%), stomach (15%), and colon (5%).Citation7 De novo formation and subsequent transit of an enterolith through the gastrointestinal tract may give rise to colicky pain and intermittent, partial or complete intestinal obstruction.Citation8 Single enteroliths smaller than 2 cm in size should typically pass unnoticed through the small intestine into the colon. In the event that the enterolith is retained, it may grow in size due to additional calcification and growth and may result in bowel obstruction in the future.Citation7
Optimal treatment of enterolithiasis should focus on enterolith removal and correction of underlying pathology to prevent the formation of additional enteroliths in the future.Citation9 During surgery, crushing and milking the stone down to the colon is the least invasive step.Citation10 If this fails, an enterotomy, usually proximal to the obstruction site, will enable the delivery of the enterolith.Citation11 Resection of the involved segment may be considered in more complicated cases.Citation12
Conclusion
Small bowel obstruction due to enteroliths is a rare condition. A CT scan of the abdomen can easily pick up these stones, including the radiolucent ones. Although larger obstructing enteroliths may need surgery, most of the smaller ones are likely to pass down spontaneously. Therefore, every effort should be made for early non-operative management, failing which surgical removal will alleviate symptoms.
Ethics Statement
Written consent for publication was obtained from the patient. This manuscript received Institutional Ethics Committee approval for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
- Gupta NM, Pinjla RK, Talwar BL. Calcific enterolithiasis. Indian J Gastroenterol. 1986;5(1):29–30.
- Gurvits GE, Lan G. Enterolithiasis. World J Gastroenterol. 2014;20(47):17819–17829. doi:10.3748/wjg.v20.i47.17819
- Fallingborg J. Intraluminal pH of the human gastrointestinal tract. Dan Med Bull. 1999;46(3):183–196.
- Paige ML, Ghahremani GG, Brosnan JJ. Laminated radiopaque enteroliths: diagnostic clues to intestinal pathology. Am J Gastroenterol. 1987;82(5):432–437.
- Makris K, Tsiotos GG, Stafyla V, Sakorafas GH. Small intestinal nonmeckelian diverticulosis. J Clin Gastroenterol. 2009;43(3):201–207. doi:10.1097/MCG.0b013e3181919261
- Mulita F, Tchabashvili L, Bousis D, et al. Gallstone ileus: a rare cause of small intestine obstruction. Clin Case Rep. 2021;9(11):e04924. doi:10.1002/ccr3.4924
- Nakao A, Okamoto Y, Sunami M, Fujita T, Tsuji T. The oldest patient with gallstone ileus: report of a case and review of 176 cases in Japan. Kurume Med J. 2008;55(1–2):29–33. doi:10.2739/kurumemedj.55.29
- Jones RP, McWhirter D. Intermittent small bowel obstruction caused by Meckel’s enterolith. Ann R Coll Surg Engl. 2010;92(5):W16–17. doi:10.1308/147870810X12699662980079
- Ihara E, Ochiai T, Yamamoto K, Kabemura T, Harada N. A case of gallstone ileus with a spontaneous evacuation. Am J Gastroenterol. 2002;97(5):1259–1260. doi:10.1111/j.1572-0241.2002.05715.x
- Leow CK, Lau WY. Treatment of small bowel obstruction by jejunal enterolith. Surgery. 1997;122(5):977–978. doi:10.1016/S0039-6060(97)90349-4
- Cartanese C, Campanella G, Milano E, Saccò M. Enterolith causing acute afferent loop syndrome after Billroth II gastrectomy: a case report. G Chir. 2013;34(5–6):164–166. doi:10.11138/gchir/2013.34.5.164
- Shah SR, Bhaduri A, Desai DC, Abraham P, Joshi A. Obstructing enterolith as presenting feature in Crohn’s disease. Indian J Gastroenterol. 2003;22(1):24.