Abstract
Background
The aim of this study was to investigate the link between atrial fibrillation (AF) and dyspepsia, as well as the contribution of dyspepsia to the overall burden of AF.
Methods
The 2008, 2009, and 2010 Japan National Health and Wellness Survey (NHWS) datasets were used in this study. The NHWS is an Internet-based survey administered to the adult population in Japan using a random stratified sampling framework to ensure demographic representativeness. The presence of dyspepsia was compared between those with and without AF. Among those with AF, the effect of dyspepsia on health status, work productivity, and activity impairment was examined, along with health care resource use using multivariable regression modeling and controlling for baseline differences.
Results
Among patients with AF (n = 565), the three most commonly reported comorbidities were hypertension (38.76%), dyspepsia (37.35%), and overactive bladder (28.72%). Patients with AF had 48.59% greater odds of reporting dyspepsia than those without AF (P < 0.05). Patients with dyspepsia used more AF medications (2.05 versus 1.54) and had been diagnosed more recently (9.97 versus 10.58 years). Dyspepsia was associated with significantly worse physical health status (P < 0.05) and significantly more absenteeism, overall work impairment, activity impairment, physician visits, and emergency room visits (all P < 0.05).
Conclusion
Patients with AF in Japan experience a number of comorbidities, with dyspepsia being the most common noncardiovascular comorbidity. Given the prevalence and additional burden of this comorbidity across both humanistic and economic outcomes, the management of dyspepsia among patients with AF should be an area of greater focus.
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia, affecting approximately 0.65% of the Japanese population.Citation1 Its presence is associated with a significant increase in future stroke risk.Citation2 Aside from elevated stroke risk, AF is associated with a substantial burden on both the patient and society. According to previous literature, nearly all domain scores of the Short-Form 36 (a measure of health status) were significantly lower in patients with AF compared with age-matched controls.Citation3,Citation4 In the United States, direct costs ranged from $2000 to $14,200 per patient per year, predominantly because of an increased number of hospitalizations.Citation5 Lastly, patients with AF who remain in the work force also have significantly more sick leave and short-term disability than non-AF controls.Citation6
Although primarily linked to the disease itself, the patient burden can be exacerbated by the presence of comorbidities. Indeed, patients with AF experience a number of concomitant conditions. Although the prevalence of cardiovascular comorbidities among Japanese patients with AF,Citation7–Citation9 as well as the effect of these comorbidities with respect to health-related quality of life, have already been investigated,Citation10 information on other comorbidities is scarce. In the United States, LaMori et al found that 34% of patients with AF also reported experiencing dyspepsia, and that the presence of dyspepsia among patients with AF was associated with a significant decrease in health status and a significant increase in health care resource utilization and work productivity loss.Citation11
Given that the characteristics of Japanese AF patients have been reported to differ from other populations, including a lower body weight and a more dramatic gender split,Citation9 it is important to extend prior research by investigating the prevalence and effect of dyspepsia in Japan rather than extrapolating data from other countries. The objectives of the current study were, firstly, to clarify the link between AF and dyspepsia and, secondly, to understand the attributable burden of dyspepsia among patients with AF in Japan.
Materials and methods
Data source
The current study used data from the 2008, 2009, and 2010 Japan National Health and Wellness Surveys (NHWS, Kantar Health, New York, NY, USA). Details on the Japan NHWS are provided elsewhere.Citation12 In brief, the NHWS is a large, nationally representative, cross-sectional, Internet-based health survey of adults aged 18 years or older. Potential respondents are recruited through a stratified random sampling framework to ensure that the demographic composition is representative of the total Japanese adult population.Citation12 Because it is possible for a respondent to complete the NHWS more than once over this three-year period, a small subset of 2008 respondents also completed the survey in 2009 and 2010. Similarly, a small subset of 2009 respondents also completed the survey in 2010. In these instances, only the most recent data points for each respondent were included. A total of 60,015 unique respondents who completed the 2008, 2009, or 2010 Japan NHWS were included in the analyses.
Measures
Atrial fibrillation
All NHWS respondents were presented with a list of medical comorbidities and asked to select which conditions they had ever experienced (AF was one of these conditions, presented as “atrial fibrillation”, although the specific type of AF the respondents had experienced was not assessed). For the conditions selected, respondents were then asked whether they had been formally diagnosed (“yes” versus “no”). Only respondents who reported having been diagnosed with AF were considered to have AF. No exclusion criteria were applied.
Dyspepsia
The NHWS did not include a direct assessment of dyspepsia. As a result, we used a proxy measure of dyspepsia based on the presence of conditions that share symptoms with, and are often associated with, functional dyspepsia. These conditions included ulcers, abdominal bloating, abdominal pain, gastroesophageal reflux disease (GERD), and heartburn. Patients who self-reported any of those conditions were considered to have dyspepsia. The same approach to assessing dyspepsia has been used in prior research.Citation11
Demographics
Age (18–39, 40–49, 50–59, 60–69, 70 years and older), gender (male versus female), education (college-educated versus less than college-educated), employment (currently employed versus not employed), and annual household income (<¥3,000,000, ¥3,000,000–4,999,999, ¥5,000,000–7,999,999, ≥¥8,000,000, or declined to answer) were included.
Patient characteristics
Smoking (currently a smoker versus former smoker versus never smoked), alcohol use (currently drinking versus not currently drinking), exercise (currently exercising versus not currently exercising), bodyweight (in kilograms), and body mass index (underweight, normal weight, overweight, obese, decline to answer) were assessed for all respondents. The Charlson comorbidity indexCitation13 was calculated based on self-reported comorbidities.
Disease history
Location of AF diagnosis, years diagnosed with AF, AF treatment (neither acetylsalicylic acid [ASA] nor warfarin, ASA without warfarin, ASA and warfarin, warfarin without ASA) and symptom severity were included. The total number of medications taken for AF was also summed and reported.
Health outcomes
The Japanese version of the Medical Outcomes Study 12-Item Short-Form Survey Instrument was used as a generic health status instrument.Citation14,Citation15 Physical component summary and mental component summary scores along with health utilities (SF-6D) were included in the analysis, with higher scores indicating better health status. Physical and mental component summary scores each vary between 0 and 100, with the population mean set at 50. Health utilities vary on a theoretical scale between 0 and 1, with 0 indicating a health state associated with death, and 1 indicating a health state associated with perfect health. The general health version of the Work Productivity and Activity Impairment questionnaire was used to assess absenteeism (the percentage of work time missed because of one’s health in the past seven days), presenteeism (the percentage of impairment experienced while at work in the past seven days because of one’s health), overall work productivity loss (an overall impairment estimate that is a combination of absenteeism and presenteeism), and activity impairment (the percentage of impairment in daily activities because of one’s health in the past seven days).Citation16 Only respondents who reported being full-time, part-time, or self-employed provided data for absenteeism, presenteeism, and overall work impairment. All respondents provided data for activity impairment. The number of physician visits, emergency room visits, and hospitalizations in the previous six months were also reported by all respondents.
Statistical analysis
The prevalence of dyspepsia among those with and without AF was compared using a Chi-square test. The presence of dyspepsia was then predicted from the presence of AF in a logistic regression model controlling for age, gender, education, household income, body mass index, smoking status, exercise behavior, and comorbidities via the Charlson comorbidity index.
Among those with AF only, differences between patients with and without dyspepsia were examined for demographics, patient characteristics, and disease history using Chi-square tests and independent-samples t-tests for categorical and continuous variables, respectively. Adjusted differences between those with and without dyspepsia with regard to health outcomes were assessed using general linear models (for health status) and generalized linear models (for work productivity and health care resource use). The latter models (specifying a negative binomial distribution and a log link function) were used to handle the inherent skewness of those variables correctly. All multivariable regression models controlled for the number of medications and the years diagnosed, because these were the only variables that were significantly different between those with and without dyspepsia and significantly predictive of health outcomes. The a priori cutoff for statistical significance of predictors in the regression model was set at P < 0.05.
Results
A total of 565 patients (0.94%) reported a diagnosis of AF. Among these patients, the five most commonly reported comorbidities were hypertension (38.76%), dyspepsia (37.35%), overactive bladder (28.72%), high cholesterol (17.88%), and angina pectoris (16.81%), making dyspepsia the most common non-cardiovascular comorbidity. Among those with AF, the components of dyspepsia included heartburn (15.58%), abdominal pain (12.57%), abdominal bloating (9.03%), GERD (8.67%), and ulcers (8.50%), with 37.16% of patients having at least two of those component conditions.
The prevalence of dyspepsia was significantly higher in those with AF (37.35%) than in the general adult population without AF from NHWS (21.30%; χ2[1] = 85.51, P < 0.0001). Even after adjusting for sociodemographics, health behaviors, and comorbidities, patients with AF had 48.59% greater odds of reporting dyspepsia than those without AF (b = 0.40, odds ratio = 1.49, P < 0.0001, see ).
Table 1 Logistic regression model predicting the presence of dyspepsia
Among those with AF, patients with comorbid dyspepsia were similar to those without AF on all demographic variables (see ). The distributions of age, gender, education, employment, and household income between these two groups were the same (all P > 0.18). Similarly, no differences between those with and without dyspepsia were observed with respect to patient characteristics. Distributions of body mass index, bodyweight, smoking status, alcohol use, and exercise behavior were similar between AF patients with and without dyspepsia (all P > 0.05).
Table 2 Differences in demographic and lifestyle characteristics between AF patients with and without comorbid dyspepsia
However, a few differences were observed with respect to AF-related history. Patients with dyspepsia were more likely to have been diagnosed in a hospital (78.67% versus 70.34%) and less likely to have been diagnosed in a physician’s office (13.74% versus 21.19%, see ). Patients with dyspepsia also reported having been diagnosed more recently (9.97 versus 10.58 years, P = 0.005) and reported using significantly more AF medications (2.05 versus 1.54, P < 0.001).
Table 3 Differences in disease history between AF patients with and without comorbid dyspepsia
Prior to covariate adjustment, the health outcomes of those with AF (without regard to dyspepsia) were compared with those with AF but without dyspepsia, and with those having AF as well as dyspepsia (see ). All health outcomes were worse among those with comorbid dyspepsia, including health status, work productivity loss, activity impairment, and health care resource use.
Table 4 Unadjusted mean level of health outcomes among AF patients with and without comorbid dyspepsia
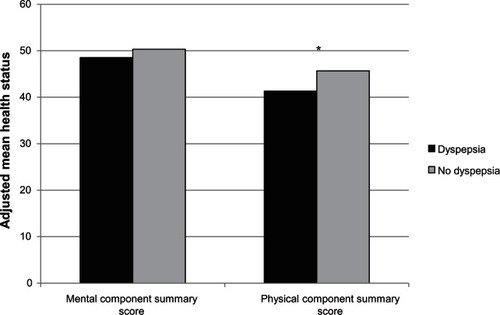
This pattern remained even after controlling for differences in disease history (see ). Patients with dyspepsia reported significantly lower levels of physical component summary scores (41.32 versus 45.66, P < 0.0001) and health state utilities (0.70 versus 0.76, P = 0.008). Although a trend for lower mental component summary scores was found (48.51 versus 50.33, P = 0.09), this difference was not statistically significant.
Figure 1 Adjusted mean health status (as measured by the Short-Form 12 version 2 instrument) between those with and without dyspepsia.
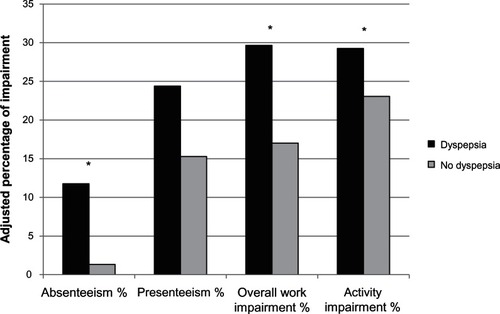
Among those who were employed, a significant effect of dyspepsia on work productivity was also observed (see ). Those with dyspepsia reported significantly more absenteeism (11.77% versus 1.33%, P = 0.003) and overall work impairment, which included both absenteeism and presenteeism (26.65% versus 17.02%, P = 0.045). Although a trend for higher presenteeism was found (24.39% versus 15.28%, P = 0.10), this difference was not statistically significant. Among all patients with AF, not just those employed, patients with dyspepsia reported significantly higher levels of impairment in daily activities (29.27% versus 23.07%, P = 0.036).
Figure 2 Adjusted percentage of impairment between those with and without dyspepsia.
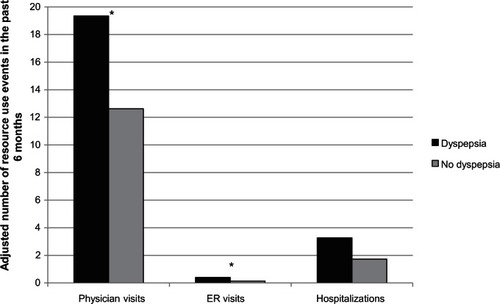
The presence of dyspepsia was also associated with direct cost drivers (see ). Indeed, patients with dyspepsia reported significantly more physician visits (19.35 versus 12.62, P = 0.0003) and significantly more emergency room visits (0.40 versus 0.14, P = 0.008) in the past six months than those without dyspepsia. Although the number of hospitalizations was higher (3.27 versus 1.73, P = 0.13), this difference was not statistically significant between the two groups.
Figure 3 Adjusted number of health care resource use events in the past six months between those with and without dyspepsia.
Discussion
As reported previously,Citation9 patients with AF in Japan suffer from a number of comorbidities, with cardiovascular, urological, and gastrointestinal conditions each being reported by more than one third of AF patients. Our results demonstrate that, when looking at individual conditions, dyspepsia is the most common non-cardiovascular comorbidity, reported by 37.35% of AF patients. Indeed, it is significantly more likely that patients with AF will have dyspepsia compared with patients without AF. It is difficult to compare these point estimates with previous reports, because few studies have assessed the Japanese population, and definitions of dyspepsia vary considerably. However, these statistics do largely coincide with prior research. For example, Mahadeva et al reported that 24.3% of the general population of Kuala Lumpur suffered from dyspepsia (defined as upper abdominal discomfort occurring for at least three weeks in the previous 12 months) compared with 21.3% of the general population in NHWS.Citation17 Prior research from the West has suggested that GERD symptoms occur in 20%–25% of those with dyspepsia (regardless of AF status) which is higher than what was observed in our study (15.28% for heartburn and 8% for GERD).Citation18–Citation20 However, Mahadeva et al found that these symptoms were far less common for dyspepsia among Southeast Asian populations than those from the West, suggesting that our lower estimates may be in the range of what would be expected in a Japanese population.Citation21
Although prior studies have not examined the link between AF and dyspepsia specifically, our findings are consistent with the literature examining the link between AF and GERD,Citation22–Citation24 a condition frequently associated with functional dyspepsia and sharing commonalities with the symptom experience (eg, epigastric pain/burning).Citation25 Kunz et al have found GERD to be a risk factor for AF,Citation22 and other studies have shown GERD to have a potential role in the pathogenesis of paroxysmal AF.Citation23,Citation24
Interestingly, few demographic and patient history differences were observed between those with and without dyspepsia, making it difficult to anticipate patients who may be more susceptible to this condition. The presence of dyspepsia was indifferent to gender, age, bodyweight, overall comorbidity profile, and health risk behaviors, such as smoking and alcohol use. These results suggest that dyspepsia is not restricted to any particular subgroup of patients with AF. However, the relationship with number of medications and presence of dyspepsia suggests that this comorbidity is preventable in certain cases. It is also possible, as discussed in prior studies, that cardiovascular comorbidities could be a contributing factor in the presence of dyspepsia.Citation25,Citation26 Further research is necessary to uncover the true mechanisms of the relationship between AF and dyspepsia.
Although AF itself can pose a burden on the patient and society,Citation3–Citation6 our results suggest that a significant part of this burden is due to dyspepsia. Indeed, patients with dyspepsia reported significantly worse health status and significantly more work impairment, primarily due to absenteeism. More health care resource use was also observed, primarily due to physician visits and emergency room visits. Collectively, these findings suggest that the presence of dyspepsia not only poses significant societal costs by affecting patients’ daily functioning and work productivity, but also incurs great health care costs through its direct management or exacerbation of other conditions. These results have important clinical implications, in that although many factors should be considered when managing patients with AF, dyspepsia should not be overlooked.
Limitations
Several limitations of this research should be noted. The primary one is the definition of dyspepsia, which was determined using a proxy measure because direct assessment was not available in the NHWS data. Although the conditions used as part of the definition share symptoms with dyspepsia, and are often linked with the condition, it is possible that patients with these symptoms did not experience true dyspepsia and patients without these conditions did experience true dyspepsia. However, given the large number of patients (nearly 40%) with at least two of these conditions, the relationship between our proxy measure and actual dyspepsia is likely to be very strong.
It should also be emphasized that all data from the NHWS were self-reported and no clinical verification of diagnoses or treatments were available. This could have introduced additional measurement error because patients may have mistakenly reported a diagnosis of AF and those without AF may have been undiagnosed. Related to this point, it should be noted that our prevalence of AF (0.94%) was higher than that reported in the literature (0.65%).Citation1 The reason for this discrepancy is unclear, but it could be that it was more common to mistakenly report a diagnosis of AF than for those without AF to be undiagnosed. Future research would be necessary.
Because of the cross-sectional and observational nature of this study, the relationship between dyspepsia and health outcomes may not be causal. For example, some studies have suggested a link between depression and dyspepsia (although the causality of this relationship is also in question), which may explain some of the additional variability observed in the current study. No data on the type of AF (eg, paroxysmal) were available, which may have hidden underlying heterogeneity across AF subgroups.
Lastly, our findings may not be generalizable to the AF population in Japan. It is possible that the sample of patients with AF in the current study differs from the general AF population in Japan. The NHWS is nationally representative of the Japanese population with respect to age and gender, and the demographic characteristics of the sample of AF patients match those of prior publications.Citation1,Citation7,Citation8,Citation10 However, the extent to which those who decided to participate in the NHWS survey differ from the overall population of patients with AF is unknown.
Conclusion
In Japan, patients with AF experience a number of comorbidities, with dyspepsia being the most common non-cardiovascular comorbidity. Few factors were associated with the presence of dyspepsia, making the prediction of its appearance challenging. However, the number of medications was associated with its presence, suggesting it could be a function of treatment for AF. Regardless of the specific cause, patients with AF and dyspepsia reported significantly worse health outcomes than patients with AF and without dyspepsia, emphasizing that the management of dyspepsia among patients with AF should be a greater area of focus.
Acknowledgment
The authors thank Jan-Samuel Wagner, a consultant to Kantar Health, for his assistance with the literature review.
Disclosure
The NHWS is fielded by Kantar Health. Bayer Yakuhin Ltd, purchased access to the NHWS data and funded the analysis and preparation of this manuscript. YK is a paid consultant to Bayer Yakuhin Ltd, for critical discussions on the study analysis, study interpretation, and clinical insights. MD is an employee of Kantar Health. BR and ECYW are employees of Bayer Yakuhin Ltd; KI and J-BB were employees of Bayer Yakuhin Ltd at the time of the study.
References
- InoueHFujikiAOrigasaHPrevalence of atrial fibrillation in the general population of Japan: an analysis based on periodic health examinationInt J Cardiol200913710210718691774
- LipGYTseHFManagement of atrial fibrillationLancet200737060461817707756
- van den BergMPHassinkRJTuinenburgAEQuality of life in patients with paroxysmal atrial fibrillation and its predictors: importance of the autonomic nervous systemEur Heart J20012224725311161936
- KangYBahlerRHealth-related quality of life in patients newly diagnosed with atrial fibrillationEur J Cardiovasc Nurs20043717615053890
- WolowaczSESamuelMBrennanVKJasso-MosquedaJGVan GelderICThe cost of illness of atrial fibrillation: a systematic review of the recent literatureEuropace2011131375138521757483
- RohrbackerNJKleinmanNLWhiteSAMarchJLReynoldsMRThe burden of atrial fibrillation and other cardiac arrhythmias in an employed population: associated costs, absences, and objective productivity lossJ Occup Environ Med20105238339120357675
- SuzukiSYamashitaTOtsukaTTreatment strategy and clinical outcome in Japanese patients with atrial fibrillationHeart Vessels20092428729319626402
- NakataniYMizumakiKNishidaKAnticoagulation control quality affects the D-dimer levels of atrial fibrillation patientsCirc J20127631732122185714
- BriereJBRossiBIwamotoKStankusADiBonabenturaMDPatient Characteristics and Comorbidities of Patients with Atrial Fibrillation in JapanValue in Health201215A113
- AlonsoJFerrerMGandekBIQOLA Project GroupHealth-related quality of life associated with chronic conditions in eight countries: results from the International Quality of Life Assessment (IQOLA) projectQual Life Res20041328329815085901
- LaMoriJCModySHGrossHJDyspepsia and disease burden among patients with atrial fibrillationCrit Pathw Cardiol201211141922337216
- LiuGGDiBonaventuraMDYuanYThe burden of illness for patients with viral hepatitis C: evidence from a national survey in JapanValue Health201215S65S7122265070
- CharlsonMEPompeiPAlesKLMacKenzieCRA new method of classifying prognostic comorbidity in longitudinal studies: development and validationJ Chronic Dis1987403733833558716
- FukuharaSBitoSGreenJHsiaoAKurokawaKTranslation, adaptation, and validation of the SF-36 Health Survey for use in JapanJ Clin Epidemiol199851103710449817121
- FukuharaSWareJEJrKosinskiMWadaSGandekBPsychometric and clinical tests of validity of the Japanese SF-36 Health SurveyJ Clin Epidemiol199851104510539817122
- ReillyMCZbrozekASDukesEMThe validity and reproducibility of a work productivity and activity impairment instrumentPharmacoeconomics1993435336510146874
- MahadevaSYadavHRampalSEverettSMGohKLEthnic variation, epidemiological factors and quality of life impairment associated with dyspepsia in urban MalaysiaAliment Pharmacol Ther2010311141115120175766
- MalfertheinerPCurrent concepts in dyspepsia: a world perspectiveEur J Gastroenterol Hepatol199911Suppl 1S25S2910443909
- JonesRHLydeardSEHobbsFDDyspepsia in England and ScotlandGut1990314014052338264
- TalleyNJZinsmeisterARSchleckCDMeltonLJDyspepsia and dyspepsia subgroups: a population-based studyGastroenterology1992102125912681551533
- MahadevaSRamanMCFordACGastro-oesophageal reflux is more prevalent in Western dyspeptics: a prospective comparison of British and South-East Asian patients with dyspepsiaAliment Pharmacol Ther2005211483149015948816
- KunzJSHemannBEdwin AtwoodJJacksonJWuTHammCIs there a link between gastroesophageal reflux disease and atrial fibrillation?Clin Cardiol20093258458719911354
- GersonLBFridayKTriadafilopoulosGPotential relationship between gastroesophageal reflux disease and atrial arrhythmiasJ Clin Gastroenterol20064082883217016140
- WeiglMGschwantlerMGattererEFinstererJStöllbergerCReflux esophagitis in the pathogenesis of paroxysmal atrial fibrillation: results of a pilot studySouth Med J2003961128113214632362
- MahadevaSYadavHRampalSGohKLRisk factors associated with dyspepsia in a rural Asian population and its impact on quality of lifeAm J Gastroenterol20101090491220179699
- Wildner-ChristensenMHansenJMDe MuckadellOBRisk factors for dyspepsia in a general population: non-steroidal anti-inflammatory drugs, cigarette smoking and unemployment are more important than Helicobacter pylori infectionScand J Gastroenterol20064114915416484119