
Abstract
For decades, it was believed that the diameter of gastrointestinal smooth muscle cells is sufficiently narrow, and that the diffusion of calcium across the plasma membrane is sufficient, to support contractile activity. Thus, depolarization-triggered release of intracellular calcium was not believed to be operative in gastrointestinal smooth muscle. However, after the incubation of muscle segments in solutions devoid of calcium and containing the calcium chelator ethylene glycol tetraacetic acid, an alternative electrical event occurred that was distinct from normal slow waves and spikes. Subsequently, it was demonstrated in gastrointestinal smooth muscle segments that membrane depolarization associated with this alternative electrical event triggered rhythmic contractions by release of intracellular calcium. Although this concept of depolarization-triggered calcium release was iconoclastic, it has now been demonstrated in multiple gastrointestinal smooth muscle preparations. On the basis of these observations, we investigated whether a rhythmic electrical and mechanical event would occur in aortic smooth muscle under the same calcium-free conditions. The incubation of aortic segments in a solution with no added calcium plus ethylene glycol tetraacetic acid induced a fast electrical event without corresponding tension changes. On the basis of the frequency of these fast electrical events, we pursued, contrary to what has been established dogma for more than three centuries, the question of whether the smooth muscle wall of the aorta undergoes rhythmic activation during the cardiac cycle. As with depolarization-triggered contractile activity in gastrointestinal smooth muscle, it was “well known” that rhythmic activation of the aorta does not occur in synchrony with the heartbeat. In a series of experiments, however, it was demonstrated that rhythmic contractions occur in the aortic wall in synchrony with the heartbeat and share a common pacemaker with the heart. We conclude that important observations in the vascular system became derivative from those in the gastrointestinal system. The challenging of scientific dogma potentially leads to the expansion of our fundamental knowledge base.
Introduction
Recordings of electrical and mechanical activity in vitro from gastrointestinal smooth muscle segments show rhythmic mechanical activity that is triggered by corresponding rhythmic changes in membrane potential.Citation1–Citation3 The underlying membrane potential changes are usually composed of two events, starting with a slow rhythmic change (often denoted as slow waves), which serves to depolarize the membrane potential to a sufficient level to elicit a second event, which is the spike or action potential (). Although in some gastrointestinal smooth muscles slow waves themselves may trigger contractions,Citation4 the usual physiologic trigger for contractions is considered the spike. The depolarizing phase of the spike is predominantly a result of an influx of calcium.Citation2,Citation5 Considering the narrow diameter of smooth muscle cells, it had been concluded that activator calcium for contractions in gastrointestinal smooth muscle originated from an influx of calcium across the plasma membrane associated with spikes, rather than a release of calcium from intracellular pools.Citation1,Citation5
Figure 1 Voltage profiles of electrical activity in cat small intestinal smooth muscle.
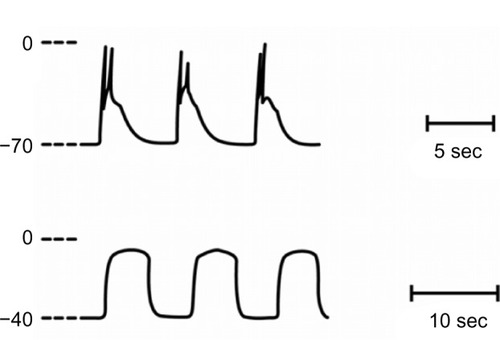
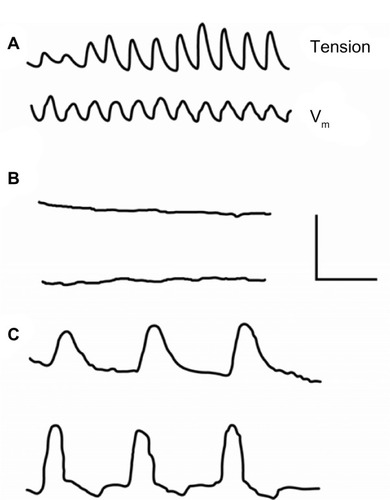
After the incubation of gastrointestinal smooth muscle segments in solutions devoid of calcium and containing the chelating agent ethylene glycol tetraacetic acid (EGTA), normal slow waves and spikes were eliminated, and an alternative rhythmic activity (prolonged potentials) developsCitation6–Citation8 (). Prolonged potentials may persist for hours in calcium-free solutions and have a voltage excursion similar to the spikeCitation3,Citation8 (). In several gastrointestinal and visceral smooth muscle preparations, prolonged potentials trigger rhythmic contractile activityCitation7–Citation10 (). Considering that preparations can be incubated for hours in solutions containing no added calcium plus EGTA, it was concluded that gastrointestinal smooth muscle contains an intracellular calcium pool that is released after membrane depolarization.
Figure 2 Recording from cat small intestinal muscle segment of mechanical (upper) and electrical (lower) activity in normal solution (A), 7 minutes after change to calcium-free solution (B), and 50 minutes after change to calcium-free solution (C). As shown in (C), prolonged potentials triggered contractions. Electrical recordings were made with pressure electrodes. Calibration bar: A/B, 0.4 mV, 0.8 g, 16 seconds; C, 0.27 mV, 0.13 g, 10 seconds. Reproduced with permission from Mangel AW, Nelson DO, Rabovsky JL, Prosser CL, Connor JA. Depolarization-induced contractile activity of smooth muscle in calcium-free solution. Am J Physiol. 1982;242(1):C36–C40.Citation8
These observations were considered iconoclastic, as it was “well known” that there was no depolarization-sensitive release of intracellular calcium in gastrointestinal smooth muscle. However, this mechanical and electrical activity has now been well described in multiple gastrointestinal and other visceral smooth muscle preparations. Possible explanations for the lack of observing contractile activity in calcium-free solutions by others include observation during the period immediately after changing from normal to calcium-free solutions, as it may take time for plateau potentials to develop, and use of single cells, as there appears to be a minimal geometry needed to observe the activity.Citation9,Citation10
These and other explanations for the failure of some to note contractions in gastrointestinal smooth muscle during incubation in calcium-free solution have recently been described.Citation3
Electrical activity of aortic smooth muscle
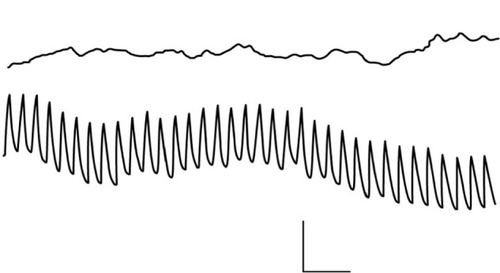
In contrast to gastrointestinal smooth muscle, segments of aortic smooth muscle are generally quiescent both electrically and mechanically in organ baths or show spontaneous contractions at a frequency significantly slower than the cardiac cycle.Citation11,Citation12 When aortic segments are incubated in a similar calcium-free solution with EGTA, a fast rhythmic electrical activity, compared with prolonged potentials, developsCitation13 (). No changes in mechanical activity were associated with these fast electrical events. Thus, experiments conducted with aortic muscle segments in vitro do not support the notion that phasic contractile activity may occur in the large conduit arteries. However, we remained intrigued that the aortic smooth muscle wall has the machinery to generate a rapid electrical event and, therefore, investigated whether the aortic wall in vivo undergoes rhythmic activation in synchrony with the heartbeat.
Figure 3 Recording of electrical activity from a segment of rabbit aorta. In the upper trace, recordings are made in normal solutions containing calcium. In the lower trace, fast rhythmic potentials become apparent after a change to calcium-free solution. Recordings are made with a pressure electrode. Calibration bar: 1 mV, 4 seconds. Reproduced with permission from Mangel A, van Breemen C. Rhythmic electrical activity in rabbit aorta induced by EGTA. J Exp Biol. 1981;90:339–342.Citation13
Arterial smooth muscle activity in vivo
The Windkessel hypothesis states that the smooth muscle walls of large arteries behave as passive elastic tubes, which represents the framework for understanding the behavior of the large arterial vasculature. This notion is perpetuated in current textbooks and a well-done recent review article.Citation14 If this fundamental understanding is incorrect, then the paradigm in which the large conduit arteries is understood is incorrect, potentially opening new avenues to develop additional classes of therapeutics for the treatment of cardiovascular diseases.
In 1733, Stephen Hales laid the foundation for the current understanding of arterial blood pressure and of the smooth muscle wall acting as a passive elastic tube.Citation14 In 1899, Otto Frank further expanded this theory, denoting it Windkessel.Citation14 Over the years, many of the underlying assumptions of the model have not changed: large arteries are considered passive elastic tubes, serving as reservoirs for blood pumped from the heart.Citation14 The smooth muscle wall of these vessels is assumed to be incapable of quick, rhythmic contractions, especially in light of the fast frequency of the heart rate.
Arterial walls behave as passive elastic tubes
In 1939, Wiggers and WegriaCitation15 recorded changes in thoracic aortic diameter and aortic pressure in anesthetized dogs. The pressure–diameter curves obtained revealed that the diameter was smaller on aortic deflation than it had been at the same pressure during aortic dilation. In other words, after passive distension of the vessel by the pulse wave, an active reduction in diameter occurs. The interpretation of these results was that during the cardiac cycle, “some active change in the vessel wall … more probably a muscular action”Citation15 is occurring. In 1955, RushmerCitation16 measured pressure–circumference relationships in the dog aorta in vivo and observed “consistent differences in the shape of the pressure and circumference curves during the cardiac cycle(s)”.Citation16 Rushmer noted that if passive distension by the pulse wave were responsible for circumference changes, then simultaneous and consistent patterns would be observed. However, because of the observed hysteresis, energy was being exchanged, and the direction of hysteresis was such that energy was being imparted by the aorta to the blood (ie, a contraction).
Nevertheless, Rushmer discounted the possibility that active phasic contractions occur in the smooth muscle wall during the cardiac cycle; instead, he suggested that an inadequate quantity of smooth muscle exists in the vessel wall and that the responsiveness of the vascular smooth muscle is too slow to participate in the cardiac cycle. He concluded that technical artifacts or changes in vessel length during the cardiac cycle erroneously suggest a phasic aortic contraction. Peterson et al,Citation17 in 1960, reported on the mechanical properties of the walls of major arteries in dogs in vivo and concluded that from the analysis of 5,000 pulse cycles, “no evidence has been found to suggest that the arterial wall [undergoes] active contraction synchronous with the cardiac cycle”.Citation17 Furthermore, they conclude that the mechanical properties of vascular smooth muscle are too slow to synchronize with the cardiac cycle.
In a more recent study, Gentile and GrossCitation18 found no evidence of active diameter changes in bypassed aortic segments in synchrony with pulsatile pressure changes in a bypassed tube. The methodology used to record diameter changes in this study was inferior and may account for the lack of diameter changes being observed.
Arterial wall shows rhythmic contractility
In contrast to the studies discussed earlier, on the basis of the fast rhythmic electrical activity observed in aortic muscle segments during incubation in calcium-free solution, Mangel et alCitation19–Citation21 directly measured tension changes in dog and rabbit aorta, femoral artery, and coronary artery in vivo. The initial experimental design involved bypassing the blood flow and recording tension changes in the bypassed segment. In the bypass tube, changes in arterial pressure were recorded. These experiments demonstrated a 1:1 coupling between pulse pressure changes and aortic, coronary, or femoral artery smooth muscle contractions. On the basis of the phasing of the pulse wave with the arterial contractions, these contractions were described as pulse-synchronized contractions (PSCs)Citation21 ().
Figure 4 Simultaneous recording of tension (upper) and blood pressure (lower) from the rabbit aorta in vivo.
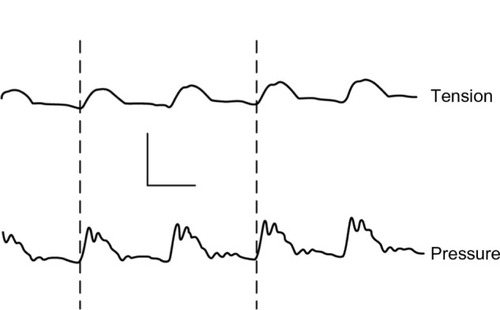
As this direct demonstration of smooth muscle contractions in large conduit arteries in vivo was considered heretical, significant effort was focused on ensuring that these events were not caused by either a movement artifact related to the pulse wave or cardiac contractility. After the local application of the neural blocker tetrodotoxin or the local anesthetic xylocaine, either to the bypassed segment or proximal to it, a block of aortic contractions, without affecting the pulse wave, occurred.Citation20 In addition to the pharmacologic dissociation with tetrodotoxin and xylocaine, several other manipulations were performed. The definitive experiment to eliminate the pulse wave as a source of a movement artifact that could be producing PSCs was to bleed the animals while recording cardiac and aortic contractility.Citation21 After animals were bled, both cardiac muscle contractions and aortic PSCs persisted for some time. Under these circumstances, there was no pulsatile pressure wave, and therefore, distension from the pulse wave could not be responsible for the PSC.
Nevertheless, questions persisted: Could movement associated with cardiac contractility lead to an artifact by tugging on the aorta? And, therefore, could PSCs result from a movement artifact from the heartbeat? In the next series of experiments,Citation21 the effects of excision of the left atrial appendage on PSCs were evaluated. This maneuver had no effect on PSCs. However, excision of the right atrial appendage caused irreversible abolishment of the PSC. PSCs were eliminated even if cardiac contractions were maintained at a greater-than-baseline amplitude level by direct electrical stimulation. Thus, this series of experiments showed both that PSCs do not result as a consequence of an artifact caused by cardiac contractions and that the pacemaker for PSCs is similar to that for the heart, in the right atrium.
In an elegant series of experiments, Ravi and FahimCitation22 stimulated the sinoatrial nodal region while recording PSCs from cat pulmonary arteries. When stimuli were applied during times when the heart was mechanically refractory, an “ectopic” PSC was produced without a corresponding pulse wave. Thus, in this configuration, PSCs could not be caused by a mechanical artifact from either the pulse wave or cardiac contractions. Furthermore, these experiments also confirmed the pacemaker region for the PSC to be in the right atrial region, helping to ensure coordination with the heartbeat.
A further review of the literature does show significant information in support of the concept of large arteries undergoing rhythmic contractions in phase with the cardiac cycle. Heyman, in a series of papers published from 1955 to 1961,Citation23–Citation26 demonstrated in both human and dog that active participation of the arterial wall occurs during the cardiac cycle. Unfortunately, these papers have previously been largely ignored. Boucek et alCitation27 also made cineangiographic recordings of the ascending aorta in dogs during the cardiac cycle. Their results suggested that the ascending aorta, during the cardiac cycle, undergoes active diameter changes with the heartbeat.
Conclusion
Challenging well-accepted notions in science has led to important discoveries. In gastroenterology, recognition that acid secretion was physiologic versus pharmacologic was not an easy concept to establish. In a similar vein, establishment of the significance of Helicobacter pylori in ulcer foundation was a high hill to climb.
Although depolarization-activated release of calcium in gastrointestinal smooth muscle was not easy to establish, it has now been demonstrated in multiple tissue types. This observation led to experimentation in aortic smooth muscle.
The observations made in vascular smooth muscle should be of interest to those studying the properties and behaviors of gastrointestinal smooth muscle, as smooth muscle is often segmented into visceral (including gastrointestinal) and vascular smooth muscle and studied separately. Findings such as those described here remind the gastrointestinal physiologist that important lessons for the gastrointestinal tract may be learned from vascular smooth muscle, and vice versa.
The hypothesis that the arterial walls of the conduit arteries behave as passive elastic tubes has been well engrained as scientific dogma for more than a century. The bias in favor of this notion was predicated on the belief that the quantity of smooth muscle in the arterial wall was too small to be significant and that the dynamics of vascular smooth muscle contraction were too slow to coincide with the cardiac cycle. It is now clear that the smooth muscle wall of the large arteries appears to undergo a contraction–relaxation cycle in synchrony with the pulse wave. The timing of the events is such that the upstroke of the contraction occurs during systole; hence the term pulse-synchronized contractions. Because of the phasing between the two events, the rhythmic contractions may help to reduce arterial wall stress from pulse pressure waves by limiting vessel wall distension. Understanding of PSCs may lead to the development of new therapeutic interventions in the field of cardiology that never would have been observed had it not been for experimentation in the gastrointestinal tract evaluating depolarization-mediated release of intracellular calcium.
Acknowledgments
Funds for conduct of this work were provided by RTI Health Solutions, of which Ms Marion and Dr Mangel are employees.
Disclosures
The authors report no conflicts of interest in this work.
References
- BozlerEThe relation of the action potentials to mechanical activity in intestinal muscleAm J Physiol194614649650120992033
- ProsserCLMangelAWMechanisms of spike and slow wave pacemaker activity in smooth musclesCarpenterDCellular PacemakersNew YorkJohn Wiley & Sons1982273301
- EvansEDMangelAWDepolarization-stimulated contractility of gastrointestinal smooth muscle in calcium-free solution: a reviewISRN Gastroenterol2011201169252821991526
- SandersKMExcitation-contraction coupling without Ca2+ action potentials in small intestineAm J Physiol19832445C356C3616846525
- ProsserCLBortoffAElectrical activity of intestinal muscle under in vitro conditionsHandbook of PhysiologyWashington, DCAmerican Physiological Society196820252050
- ProsserCLKreulenDLWeigelRJYauWProlonged potentials in gastrointestinal muscles induced by calcium chelationAm J Physiol19772331C19C24406797
- MangelAWNelsonDOConnorJAProsserCLContractions of cat small intestinal smooth muscle in calcium-free solutionNature19792815732582583114862
- MangelAWNelsonDORabovskyJLProsserCLConnorJADepolarization-induced contractile activity of smooth muscle in calcium-free solutionAm J Physiol19822421C36C407058877
- MangelAWMangelCPSandersKMModulation of intestinal electrical and mechanical activity by calciumINSERM Symposia Series: Ca Regulations in Smooth Muscle1984124111118
- MangelAWVoltage and receptor mediated contractile activity of colonic smooth muscle in calcium-free solutionEur J Pharmacol198410211651686479214
- FurchgottRFBhadrakomSReactions of strips of rabbit aorta to epinephrine, isopropylarterenol, sodium nitrite and other drugsJ Pharmacol Exp Ther1953108212914313062084
- HayashidaNOkuiKFukudaYMechanism of spontaneous rhythmic contraction in isolated rat large arteryJpn J Physiol19863647837943784152
- MangelAvan BreemenCRhythmic electrical activity in rabbit aorta induced by EGTAJ Exp Biol1981903393426787163
- WesterhofNLankhaarJWWesterhofBEThe arterial WindkesselMed Biol Eng Comput200947213114118543011
- WiggersCJWegriaRActive changes in size and distensibility of the aorta during acute hypertensionAm J Physiol19381243603611
- RushmerRFPressure-circumference relations in the aortaAm J Physiol1955183354554913283074
- PetersonLHJensenREParnellJMechanical properties of arteries in vivoCirc Res19608622639
- GentileBJGrossDRViscoelastic behavior of the thoracic aorta of dogs and rabbitsCirc Res19855656906953873295
- MangelAvan BreemenCFahimMLoutzenhiserRMeasurement of in vivo mechanical activity and extracellular Ca45 exchange in arterial smooth muscleBevanJAVascular Neuroeffector Mechanisms1983347351
- MangelAFahimMvan BreemenCRhythmic contractile activity of the in vivo rabbit aortaNature198128957996926947464936
- MangelAFahimMvan BreemenCControl of vascular contractility by the cardiac pacemakerScience19822154540162716297071582
- RaviKFahimMRhythmic contractile activity of the pulmonary artery studied in vivo in catsJ Auton Nerv Syst198718133373819314
- HeymanFMovements of the arterial wall connected with auricular systole seen in cases of atrioventricular heart blockActa Med Scand19551522919613258159
- HeymanFComparison of intraarterially and extra-arterially recorded pulse waves in man and dogActa Med Scand1957157650351013434797
- HeymanFExtra- and intra-arterial records of pulse waves and locally introduced pressure wavesActa Med Scand1959163647347513660760
- HeymanFThe arterial pulse as recorded longitudinally, radially and intra-arterially on the femoral artery of dogsActa Med Scand1961170778113714069
- BoucekRJTakashitaRFojacoRFunctional anatomy of the ascending aorta and the coronary ostia (dog)Am J Anat196411427328214131860