
Abstract
Background
Chronic inflammatory bowel disease (IBD) causes significant distress for patients and their families. Data assessing the need of these patients for support and sharing with their partners are scarce. The aim of this study was to assess patients’ views regarding sharing of information with their partners.
Methods
Ambulatory IBD patients treated at the Chaim Sheba Medical Center between January 2011 and January 2013 were asked to complete an anonymous questionnaire. Patients who had a stable partner and completed more than 95% of the questionnaire were included.
Results
Of 134 patients who agreed to complete the questionnaire, 101 met the inclusion criteria, 53 were men (mean age 45±15 years), and 50% had academic education. Only 42% of patients reported that their partner accompanied them to the doctor. However, 93% shared health problems with their partner, 64% would have liked their partner to receive more medical information, and 70% would like their partner to be more involved. The majority (88%) believed that more partner involvement could help them deal better with the disease, and 70% thought that support groups for partners should be established. No association was found between patients’ demographic data and their answers. Patients who felt that partner involvement could help them to deal with the disease tended to share medical information with their partners and wanted them to be more involved in health care decision-making (P<0.001).
Conclusion
Most IBD patients in our study wanted their partner to be more involved with their health problems, and believed that greater partner involvement could help them deal better with their disease. Therefore, more attention should be focused on gaining better cooperation from patients’ families.
Introduction
Crohn’s disease (CD) is a chronic inflammatory disorder that may affect the gastrointestinal tract from the mouth to the anus. Inflammation is transmural, and might therefore be complicated by fistula and abscess formation, perforations, and fibrotic strictures. Ulcerative colitis is another form of inflammatory bowel disease (IBD) that mainly affects the colon, causing abdominal pain, bloody diarrhea, and weight loss. Both diseases may cause significant morbidity and diminished quality of life.Citation1–Citation6 The natural history of IBD is characterized by periods of flare-up with active symptomatic disease and periods of disease remission.Citation7
Psychosocial function has been found to be closely related to quality of life in patients with IBD.Citation8 The disease was shown to have an impact on patients’ psychological functioning even during periods of remission when patients are not suffering from active IBD symptoms.Citation9
Social support was shown to improve patients’ ability to cope with active disease and stress. Family support was reported by patients as being helpful for managing IBD.Citation10–Citation13 Nicholas et alCitation14 found that providing social support to adolescents with IBD had a positive effect on their ability to cope with the disease. Honesty and open communication with families regarding diagnosis, bowel symptoms, and treatment led to more effective coping strategies and adaptation.Citation14
Chronic disease in a family member is known to affect quality of life for the whole family. In a recently published paper, Golics et alCitation15 reported a significant emotional impact in 92% of close family members of patients with chronic disease, a significant effect on daily activities in 91% of family members, and an effect on family relationships in 69% of cases. The study included close family members of patients suffering from a variety of chronic diseases, including Crohn’s disease and colitis. Family members included in the study reported providing active support to patients, including reminding them to take their medication, involvement in hospital appointments, and a sense of not being given enough information on the patient’s condition. A few family members mentioned support groups as a potential way of coping with the disease. Of note, involvement of family members has been shown to be crucial for successful patient care,Citation16 so the family can be provided with appropriate support.
However, actual data assessing patients’ attitudes toward spouse or partner involvement in their disease are scarce. Therefore, the aim of this study was to assess patients’ views on information-sharing with their partners.
Patients and methods
Ambulatory IBD patients treated at the Chaim Sheba Medical Center from January 2011 to January 2013 were asked by a research coordinator to complete an anonymous questionnaire assessing their attitudes toward information-sharing with their partners and its influence on their ability to cope with their disease. Patients were informed that participation in the questionnaire was voluntary. The completed questionnaires were collected by the study coordinator. All patients were aged 18 years and older.
The questionnaire included demographic data (age, sex, educational level, marital status, number of children). Patients who were not married were asked if they had a stable partner. Only patients who had a stable partner (ie, in a committed relationship lasting at least 6 months) were included. Since all our patients were white Caucasians, ethnicity was not assessed. The diagnosis (ie, Crohn’s disease or ulcerative colitis) and disease duration were reviewed. Subjects who had a stable partner were asked about sharing their health problems with their partner, partner involvement in disease management (including doctor’s visits), and their views on partner involvement and how it should be achieved. Only patients who completed more than 95% of the items in the questionnaire were included. The study was approved by the local ethics committee and all patients gave their written informed consent before completing the questionnaire.
Statistical analysis
Mean age according to sex was compared using the Student’s t-test. The chi-squared test and Fisher’s exact test were used for categorical variables, eg, for assessing the relationship between: sex, education, and number of children; sex, education, number of children, and type of answer; and belief that involvement of the partner could help in dealing better with the disease and answers to the other questions. The statistical analysis was performed using IBM® SPSS® Statistics for Windows version 21.0 software (IBM Corporation, Armonk, NY, USA). P<0.05 was considered to be statistically significant.
Results
Of 140 patients approached, 134 agreed to complete the questionnaire. Thirty-three patients were excluded because they did not complete the questionnaire (), leaving 101 participants in the study. Patient demographic characteristics are shown in .
Figure 1 Study design.
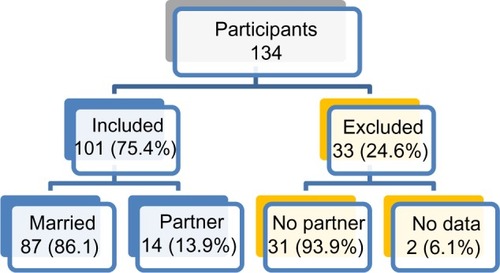
Table 1 Patient characteristics
Only 41 of 96 patients (42%) who answered the relevant question reported that their partner accompanied them to doctor’s appointments. However, 92 of 98 patients (94%) who answered the relevant question stated that they shared and discussed their health problems with their partner. Sixty-one of 96 patients (64%) who answered the relevant question wanted their partner to receive more medical information, and 67 of 96 (70%) who answered the relevant question would like their partner to be more involved. Eighty-four of 96 patients (88%) who answered the relevant question believed that increased partner involvement could help them to cope better with the disease, and 70 of 99 (70%) who answered the relevant question thought that a support group for partners should be established. No association was found between patient demographic data and any of these variables.
Further stratification was performed according to patients’ views regarding the effect of partner involvement on their ability to cope with the disease (). Ninety-nine percent of patients who considered partner involvement to be beneficial shared their health problems with their partner, compared with 58% of patients who did not consider partner involvement to be beneficial (P<0.001). Three quarters of these patients wanted their partner to receive more medical information from the physician about their physical condition, compared with only 8% of the patients who did not perceive partner involvement as beneficial (P<0.001). Similarly, 79% of these patients wanted their partner to be more involved in their health care decisions, compared with 8% of patients who did not consider partners’ involvement as beneficial (P<0.001).
Table 2 Distribution of patients’ answers
Interestingly, most patients who preferred partner involvement were actually not accompanied by the partner to the clinic/doctors’ visits. Only 46% of these patients reported that their partner accompanied them to doctor’s appointments versus 17% of the partners of patients who did not consider partner involvement to be beneficial (P=0.065).
Fifty-eight percent of patients who considered partner involvement to be beneficial for coping with the disease answered “yes” to questions regarding their wish for partner involvement, partners receiving more information from the physician, and whether they shared health problems with the partner ().
Table 3 Stratification of patients’ answers
Discussion
Inflammatory bowel disease can cause considerable suffering and diminished quality of life for both patients and their families. Moreover, disease symptoms, such as chronic diarrhea, chronic abdominal pain, fecal incontinence, soiling, perianal fistula, and fatigue, may cause impairment of body image, fear of sexual intimacy, and social isolation.Citation17–Citation20
Coping with these symptoms requires appropriate strategies. However, the data suggest that patients with IBD often use passive coping strategies, for instance, escape-avoidance behavior,Citation20–Citation23 which in turn may lead to psychological distress and poor adaptation to the disease.Citation24 Social support was shown to be very important for coping with IBD. Sewitch et alCitation25 found that perceived stress in IBD patients may change according to their level of social support. Patients who were satisfied with their social support had lower levels of psychological distress and better disease adjustment. Spouses were also the most frequently reported source of support for patients with other chronic diseases, such as diabetes mellitus,Citation26 interstitial cystitis,Citation27 and breast cancer.Citation28
In our current study, we examined patients’ views and beliefs regarding the sharing of medical information and disease symptoms with their life partner. Our first notable finding is that most patients rate their partners support as important, perceiving it to be instrumental in better coping with the disease. Most of the patients (88%) believed that partner involvement could help them deal better with their disease and 94% reported sharing their health problems with the partner. These high percentages indicate that most IBD patients need to unload the psychological burden of their disease, and feel that their partner is a stable source of support and comfort.
These data are in agreement with those of other studies,Citation10–Citation14,Citation25 that similarly highlight the importance of social support when coping with IBD. Along this line, the majority of patients expressed a desire for their partner to be more involved in their health care decisions, and to receive more information from their physician concerning their disease.
When stratifying the patients according to their answer to the pivotal question concerning their view on whether partner involvement was beneficial in coping with the disease, virtually all of those who believed in partner involvement reported sharing their health problems with the partner, and the majority (80%) wanted the partner to be more involved in their health care decisions and to receive more medical information from the physician. Interestingly, most of the patients who felt that partner’s involvement was beneficial were not accompanied by the partner at medical appointments. Although patients were not asked about this issue specifically, we believe that this did not reflect true patient preferences. More likely, it reflected the daily reality of life for these relatively young patients (mean age 45.36±15.46 years) who arrive on an ambulatory basis and whose partners are often absent because of other commitments.
In contrast with the above, it should be mentioned that a minority of patients did not perceive partner involvement as beneficial, and this subgroup also tended to decline providing more information to their partner. Only 17% of this subgroup (versus 46% in the group with a positive view on partner involvement) were accompanied by their partner to hospital appointments (P=0.065, not statistically significant). Interestingly, even in this group, 58% of patients shared their health problems with their partner, possibly reflecting the fact that they still needed to share and unload their burden with their life partner.
Overall, these observations underscore that IBD experts should be cognizant of the possible positive role of life partners in quality of life for IBD patients. Accordingly, once patient consent has been secured, physicians caring for IBD patients should try to involve their patients’ partners in medical decision-making, share relevant information with them, and encourage them to accompany the patient to the clinic.
Our study has a few limitations. Only patients who agreed to complete a questionnaire were included, which may have introduced selection bias. However, this limitation is inherent in any study using voluntary questionnaires. Second, the results of the questionnaire represent only the opinions of our patient population, which comprised IBD patients in a tertiary center. However, given that we care for a variety of patients with the full spectrum of disease severity, we estimate that their answers can provide a good estimate of patient preferences. Lastly, patients’ partners were not included in the study, and they should probably be included in future studies to elucidate their perceptions on how desirable their involvement is in supporting their partner with IBD.
In conclusion, the present study emphasizes the importance ascribed by IBD patients to social support from their life partner. We believe that physicians should be aware of this and try to involve patients’ families in general, and patients’ partners in particular, in management of the disease. This might include encouragement of partners to attend clinic visits, sharing medical information with them, and accepting them as a major source of support for the patient. Working together with patients’ partners can have a major impact on patients’ ability to cope with the disease, leading to improved quality of life.
Disclosure
The authors report no conflicts of interest in this work.
References
- LoveJRIrvineEJFedorakRNQuality of life in IBDJ Clin Gastroenterol19921415191556402
- CasellasFArenasJIBaudetJSImpairment of health-related quality of life in patients with inflammatory bowel disease: a Spanish multicenter studyInflamm Bowel Dis20051148849615867589
- RubinGPHunginAPChinnDJQuality of life in patients with established inflammatory bowel disease: a UK general practice surveyAliment Pharmacol Ther20041952953514987321
- CasellasFLópez-VivancosJBadiaXInfluence of inflammatory bowel disease on different dimensions of quality of lifeEur J Gastroenterol Hepatol20011356757211396538
- CanavanCAbramsKRHawthorneBLong-term prognosis in Crohn’s disease: factors that affect quality of lifeAliment Pharmacol Ther20062337738516422997
- HjortswangHJärnerotGCurmanBThe influence of demographic and disease-related factors on health-related quality of life in patients with ulcerative colitisEur J Gastroenterol Hepatol2003151011102012923375
- LatellaGPapiCCrucial steps in the natural history of inflammatory bowel diseaseWorld J Gastroenterol201273790379922876029
- TurnbullGKVallisTMQuality of life in inflammatory bowel disease: the interaction of disease activity with psychosocial functionAm J Gastroenterol199590145014547661168
- LixLMGraffLAWalkerJRLongitudinal study of quality of life and psychological functioning for active, fluctuating, and inactive disease patterns in inflammatory bowel diseaseInflamm Bowel Dis2008141575158418512245
- KarwowskiCAKeljoDSzigethyEStrategies to improve quality of life in adolescents with inflammatory bowel diseaseInflamm Bowel Dis2009151755176419472359
- GraffLAWalkerJRLixLThe relationship of inflammatory bowel disease type and activity to psychological functioning and quality of lifeClin Gastroenterol Hepatol200641491150117162241
- DrossmanDAPatrickDLMitchellCMHealth-related quality of life in inflammatory bowel disease. Functional status and patient worries and concernsDig Dis Sci198934137913862766905
- CasellasFFontanetGBorruelNThe opinion of patients with inflammatory bowel disease on healthcare receivedRev Esp Enferm Dig20049617418415053732
- NicholasDBOtleyASmithCChallenges and strategies of children and adolescents with inflammatory bowel disease: a qualitative examinationHealth Qual Life Outcomes200752817531097
- GolicsCJBasraMKSalekMSFinlayAYThe impact of patients’ chronic disease on family quality of life: an experience from 26 specialtiesInt J Gen Med20131878779824092994
- YoungbloodNMHinesJThe influence of the family’s perception of disability on rehabilitation outcomesRehabil Nurs1992173233261492162
- DrossmanDARingelYPsychological factors in ulcerative colitis and Crohn’s diseaseSartorRSandbornWKirsner’s Inflammatory Bowel Disease6th edPhiladelphia, PA, USAWB Saunders2004
- KieblesJLDoerflerBKeeferLPreliminary evidence supporting a framework of psychological adjustment to inflammatory bowel diseaseInflamm Bowel Dis2010161685169520155849
- CooperJMCollierJJamesVHawkeyCJBeliefs about personal control and self-management in 30–40 year olds living with inflammatory bowel disease: a qualitative studyInt J Nurs Stud2010471500150920646707
- CasatiJTonerBBPsychosocial aspects of inflammatory bowel diseaseBiomed Pharmacother20005438839310989978
- SainsburyAHeatleyRVReview article: psychosocial factors in the quality of life of patients with inflammatory bowel diseaseAliment Pharmacol Ther20052149950815740531
- JonesMPWessingerSCrowellMDCoping strategies and interpersonal support in patients with irritable bowel syndrome and inflammatory bowel diseaseClin Gastroenterol Hepatol2006447448116616353
- GraffLAWalkerJRClaraIStress coping, distress, and health perceptions in inflammatory bowel disease and community controlsAm J Gastroenterol20091042959296919755973
- CraneCMartinMSocial learning, affective state and passive coping in irritable bowel syndrome and inflammatory bowel diseaseGen Hosp Psychiatry200426505814757303
- SewitchMJAbrahamowiczMBittonAPsychological distress, social support, and disease activity in patients with inflammatory bowel diseaseAm J Gastroenterol2001961470147911374685
- AugustKJSorkinDHSupport and influence in the context of diabetes management: do racial/ethnic differences exist?J Health Psychol20111671172121444731
- GintingJVTrippDANickelJCFitzgeraldMPMayerRSpousal support decreases the negative impact of pain on mental quality of life in women with interstitial cystitis/painful bladder syndromeBJU Int201110871371721050362
- NaamanSRadwanKJohnsonSCoping with early breast cancer: couple adjustment processes and couple-based interventionPsychiatry20097232134520070132