
Abstract
Purpose
Fifteen percent of incident Crohn’s disease (CD) cases are diagnosed at older ages and demonstrate colonic location and inflammatory behavior. Serologic responses to gut microbial antigens are associated with specific phenotypes, and may differ by age at diagnosis. Our aim was to identify an association between age at diagnosis of CD and responses to gut microbial antigens.
Patients and methods
Levels of anti-Saccharomyces cerevisiae antibodies (ASCA) immunoglobulins A and G (IgA and IgG), antibodies to Escherichia coli outer membrane porin-C (anti-Omp-C), antibodies to clostridial flagellin (anti-CBir-1), and perinuclear anti-neutrophil cytoplasmic antibodies (p-ANCA) were compared in patients by age in three diagnosis groups: patients diagnosed at ages of <40, ≥40–59, and ≥60 years. For each antigen, patients with antibody levels in the first, second, third, and fourth quartile were assigned a score of 1, 2, 3, or 4, respectively. Individual scores were added to create a quartile sum score representing cumulative quantitative immune response.
Results
Eighteen, 17, and 12 patients were diagnosed at ages <40, 40–59, and ≥60 years, respectively. The majority (71%) had ileocolonic disease in the youngest group, compared to 36% in the oldest group (P=0.001). Mean ASCA IgA and IgG titers were increased in the youngest age group compared to the older groups (P=0.19 and P=0.13, respectively). Mean quartile sum scores for antibody levels were 7.2±2.8 in those patients diagnosed at ages <40 years, 4.9±2.9 in the 40–59-year-old age group, and 5.6±2.6 in the ≥60-year-old age group (P=0.06).
Conclusion
A trend toward decreased cumulative immune responses to CD-associated gut antigens was observed in CD patients diagnosed at older ages compared to younger patients. Host responses to microbial antigens may be less important in older onset IBD and may contribute to the distinct phenotype in this group.
Introduction
Immune responses to gut flora are thought to play an important role in the multifactorial pathogenic process of Crohn’s disease (CD). Differences in serologic responses to intestinal microbiota have been associated with disease location and behavioral phenotypes, further implicating the interaction between host immunity and enteric antigens in the etiopathogenesis of CD.Citation1 Anti-Saccharomyces cerevisiae antibodies (ASCA) were the first serologic marker identified for CD in the 1980s.Citation2 ASCA immunoglobulins A and G (IgA and IgG), antibodies to Escherichia coli outer membrane porin-C (anti-Omp-C), antibodies to clostridial flagellin (anti-Cbir-1) and to Pseudomonas fluorescens (I2) have been associated with small bowel disease location and complicated (fibrostenotic or perforating) disease behavior.Citation3–Citation9 Post-operative complication risk has also been associated with the presence of anti-CBir-1 and anti- Omp-C.Citation10–Citation13 Perinuclear anti-neutrophil cytoplasmic antibodies (p-ANCA) are common in patients with ulcerative colitis (UC). However, existing literature has demonstrated that CD patients with isolated colonic location and non-stricturing, non-penetrating phenotype are more likely to have positive p-ANCA serology.Citation14
It is estimated that approximately 15% of patients with CD are diagnosed >40 years of age, and that the incidence of inflammatory bowel disease (IBD) diagnosis in this older age group appears to be increasing over time.Citation15 Retrospective studies have demonstrated that patients with older age at diagnosis are less likely to have a complicated disease course, and more often have isolated colonic disease.Citation16,Citation17 Conversely, younger patients are more likely to have complicated disease behavior and small bowel disease location.Citation16 Similar findings were shown in a retrospective analysis, which also evaluated those diagnosed at age 60 and over. Older patients with CD in this study were also less likely to develop complicated disease behavior and were more likely to have isolated colonic disease location.Citation17
In pediatric onset IBD, differences in serologic expression to gut microbial antigens is variable depending on age at diagnosis;Citation14,Citation18 however, little information is available regarding serologic response to gut microbial antigens in older patients with CD. In the current study, we compared the levels of ASCA IgG, ASCA IgA, anti-Omp-C, anti-CBir-1, and p-ANCA by age of diagnosis. We hypothesized that based on the decreased prevalence of small bowel involvement and complicated disease behavior in older CD patients, those diagnosed at age 60 years or older would be less likely to have positive responses to microbial antigens and to have lower quartile scores to the CD-specific antigens than younger CD patients.
Material and methods
Patients with CD from the University of Maryland, Baltimore IBD Program were eligible to participate from January 2010 to February 2011. The diagnosis of CD was confirmed using standard clinical, endoscopic, radiologic, and histologic criteria.Citation19 Patients with UC, IBD unknown type, or other forms of colitis were excluded. Sera collected from CD patients were tested during a routine clinical visit for the presence of ASCA IgA, ASCA IgG, anti-Omp-C, anti-CBir-1, and p-ANCA using the Prometheus Laboratories Inc. (San Diego, CA, USA) IBD Serology 7 test. A patient was considered positive for a serology marker if the result was above the reference range values. Demographic and clinical data were extracted from an Institutional Review Board (IRB)-approved clinical data repository. The proportion of patents with positive serologic responses to each microbial antigen was compared among the following age-at-diagnosis groups: <40 years, 40–59 years, and ≥60 years of age, using the chi-square test. Mean titers to each microbial antigen were compared among the three groups using the Kruskal–Wallis test. The proportion of patients with positive antibodies to multiple antigens was also compared between groups, using the chi-square test. Scatter plots were generated to compare the distribution of antibody positivity for each CD-specific antigen in the cohort, using the Kruskal–Wallis test. For each CD-specific microbial antigen, patients with detectable antibody levels in the first, second, third, and fourth quartile of distribution were assigned a quartile score of 1, 2, 3, or 4, respectively.Citation8 Individual quartile scores for each microbial antigen were then added to create a sum quartile score for each patient to represent cumulative quantitative immune response toward CD-specific antigens.Citation8 Mean quartiles scores between groups were compared using analysis of variance (ANOVA), as these scores were noted to have a normal distribution. Values below the detectable threshold were not included in the quartile analysis. Statistical analyses were performed using SAS (Cary, NC, USA) statistical analysis software, version 9.2.
Ethical considerations
This study was carried out with the approval of the University of Maryland at Baltimore Human Research Protections Office. At recruitment, all participants gave written informed consent for participation in this study.
Results
Demographics
Forty-seven patients with CD were enrolled. Eighteen, 17, and 12 patients were diagnosed at ages <40 years, between ages 40 and 59 years, and at age 60 years or over, respectively, with ages ranging from 20 to 79 years. Fifty-three percent of the total patient population was female, and 81% was Caucasian. There were no differences in sex, race, smoking status, or extra-intestinal manifestations between the age-at-diagnosis groups (). While no difference was detected in behavioral phenotype between the age-at-diagnosis groups, there was a difference in disease location noted, with 71% of patients <40 years of age at diagnosis demonstrating ileocolonic disease location compared to 36% ileocolonic disease location in patients diagnosed at age 60 years and over (P<0.01). In addition, 47% of patients diagnosed at ages 40–59 years had ileal disease location compared to 0% of patients diagnosed at <40 years of age (P<0.01). In addition, there was a trend detected for perianal involvement in patients diagnosed at age <40 years; however, this trend was not statistically significant (P=0.15).
Table 1 Demographics of participants with CD from the University of Maryland, Baltimore IBD Program by age at diagnosis
ASCA IgA and IgG levels by age at diagnosis
Fifty percent, 18%, and 50% of patients diagnosed at <40 years, 40–59 years, and ≥60 years of age had elevated levels of ASCA IgA (P=0.09; ). The mean titer of ASCA IgA was 44.6±27.7 EU/ml in patients diagnosed <40 years of age, 42.6±23.2 in patients diagnosed at ages 40–59, and 24.0±3.6 in patients diagnosed ≥60 years of age (P=0.19; ). Fifty percent, 18%, and 17% of patients diagnosed at ages <40, 40–59, and ≥60 years had elevated levels for ASCA IgG (P=0.07; ). Similarly, the mean titer of ASCA IgG was elevated at 55.3±24.6 in patients diagnosed at <40 years of age, compared to 36.4±14.8 in patients diagnosed between ages 40 and 59 years, and 33.4±17.7 in patients diagnosed at ≥60 years of age, though not statistically significantly (P=0.13; ).
Figure 1 Distribution of antibody titers to microbial antigens of participants with Crohn’s disease from the University of Maryland, Baltimore IBD Program by age at diagnosis.
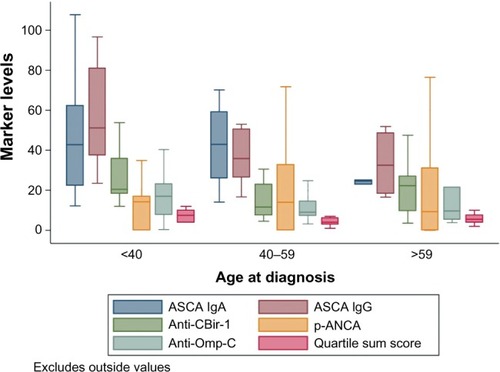
Table 2 Positive serologic responses to each CD-specific antigen by age at diagnosis of participants with CD from the University of Maryland, Baltimore IBD Program
Anti-Omp-C antibody levels by age at diagnosis
Fifty percent, 18%, and 33% of patients aged <40 years, 40–59 years, and ≥60 years at diagnosis had abnormal anti-Omp-C levels (P=0.16; ). There was also no difference in mean titers to anti-Omp-C between the three different age-at-diagnosis groups (P=0.69; ).
Anti-CBir-1 antibody levels by age at diagnosis
Forty-four percent, 29%, and 50% of patients <40, 40–59, and ≥60 years of age at diagnosis had abnormal anti-CBir-1 levels (P=0.49; ). There was also no difference in mean titers to anti-CBir-1 between the three different age-at-diagnosis groups (P=0.09; ).
IBD-specific p-ANCA levels by age at diagnosis
Twenty-eight percent, 24%, and 42% of participants in the youngest, middle, and oldest age-at-diagnosis groups had an abnormal p-ANCA level (P=0.56; ). There was also no difference in mean titers of p-ANCA between age groups (P=0.96; ).
Serologic response to multiple enteric antigens by age at diagnosis
Overall, 81%, 45%, 30%, and 13% of all patients had an abnormal response to at least one, at least two, at least three, and at least four microbial antigens, respectively. The proportion of patients with an abnormal response to any microbial antigen overall did not differ between age-at-diagnosis groups (P=0.19; ).
Table 3 Positive serologic response to microbial antigens of participants with Crohn’s disease from the University of Maryland, Baltimore IBD Program by age at diagnosis
Mean quartile scores to enteric antigens by age at diagnosis
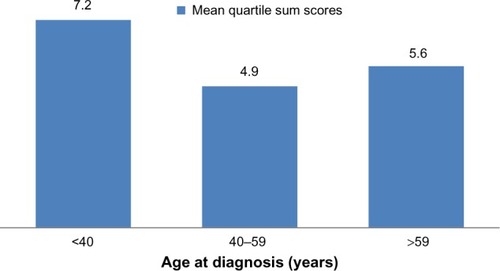
Mean quartile sum scores for antibody levels were higher in the youngest age-at-diagnosis group: 7.2±2.8 in those patients diagnosed at <40 years of age, 4.9±2.9 in those diagnosed between ages 40 and 59 years, and 5.6±2.6 in those diagnosed at age 60 years or over (P=0.06; ).
Figure 2 Mean quartile sum scores to all antigens of participants with Crohn’s disease from the University of Maryland, Baltimore IBD Program by age at diagnosis.
Discussion
In this tertiary referral population of patients with CD, we found a trend toward increased proportion of patients diagnosed at <40 years of age with positive ASCA IgA and ASCA IgG antibodies, compared to those diagnosed at 40 years and older, although this trend did not reach statistical significance. Further, we noted a trend toward higher titers of ASCA IgA, ASCA IgG, and overall quartile scores for all CD-associated antibodies in younger patients, compared to older patients with CD.
Studies in adults have shown that in CD, age is associated with disease location and behavior.Citation16,Citation17,Citation20,Citation21 Information on serologic responses to gut microbial antigens by age at diagnosis is lacking in adults. However, differential serologic responses to microbial gut antigens have been evaluated in pediatric CD populations.Citation18,Citation22–Citation24 Markowitz et al compared the presence of ASCA IgA and IgG, anti-Omp-C antibody, anti-CBir-1 antibody, and IBD-associated p-ANCA among children diagnosed with CD at #7 years of age and between 8 and 15 years of age.Citation14 Children diagnosed between 8 and 15 years of age were more likely to have elevated ASCA IgA and IgG compared to patients diagnosed at 7 years or younger. Conversely, children diagnosed at 7 years or younger were more likely to have elevated anti-CBir-1 antibody responses. Interestingly, there were also differences noted in the distribution of disease location in these children. Children diagnosed at 7 years or younger were more likely to have isolated colonic disease, whereas children diagnosed between 8 and 15 years of age were more likely to have ileocolonic disease location. These results suggest an alternate genetic and environmental pathophysiologic process as the etiology of CD at extremes of age.
In our present study, a trend toward higher titers of ASCA IgA and IgG was noted among patients diagnosed at <40 years of age. Positivity for ASCA has been associated with small bowel disease location and complicated behavioral phenotypes including stricturing and perforating disease.Citation25–Citation27 Complicated CD phenotypes are also more often seen in patients diagnosed at younger ages; therefore, these trends are not surprising. Prior epidemiologic studies comparing younger and older CD patients point to an alternate pathway for the development of CD in older patients.Citation25–Citation27 The lower prevalence of ASCA in this older population may point to a pathogenic process that does not typically involve the small bowel or result in complicated phenotypes. Conversely, it is possible that the development of IBD in older patients is in fact due to dysregulated immune responses to gut microbiota that are not yet identified and not on the IBD 7 test. Analyzing the potential differences in gut microflora in CD patients with younger and older ages at diagnosis would help to further elucidate the meaning of our observed serologic responses.
Our present study was limited by small sample size, particularly in the oldest age-at-diagnosis group. This small sample size may have impaired our ability to detect differences in responses to other microbial antigens in the IBD 7 test. It may have also limited detection of a “dose–response” correlation between increasing age and decreasing IBD serology titers. Further, when interpreting our results, one must consider the role of immune senescence and how it may impact the IBD 7 test analysis. Currently, there are no studies that elucidate the possible effect of immune senescence on the sensitivity and specificity of the IBD 7 serologic test. This natural decline in the production of naïve, antigen-specific lymphocytes and T cell dysregulation with aging may be the underlying explanation for the reduced ASCA level seen in older patients.Citation28 The most accurate method to clarify the role of ASCA in the etiopathogenesis of CD in the elderly would be to follow this patient cohort (particularly the youngest age-at-diagnosis group) in a long-term, prospective study where serologic analyses are performed at regular intervals and assessed for declines over time. Given the understanding that ASCA positivity does not correlate with disease duration or activity,Citation29 a decline over time in this serologic response would suggest an effect of immune senescence. While medical therapy data was not included in the present analysis, there is currently no evidence in the literature to suggest that medical therapy impacts detection of serologic markers in IBD.
Conclusion
To the best of our knowledge, this is the first study to focus on serologic responses to gut microflora in young, middle-aged, and older adults with CD. It also addresses the clinically relevant question of whether CD-specific serologic testing is beneficial in patients diagnosed at older ages.
In summary, our present study demonstrated an increased proportion of patients diagnosed with CD at <40 years of age with a positive ASCA compared to patients diagnosed at older ages. This finding is congruent with studies that have shown that patients with CD diagnosed at older ages are less likely to develop complicated CD, given that positive ASCA has been associated with complicated CD.Citation25–Citation27 Our findings also suggest that the same disease may have differing etiopathogenesis depending on the age at diagnosis. Further research is needed to identify differences in bacterial populations in different age-at-diagnosis groups and how these changes, if present, affect the pathogenesis of CD. In addition, clinicians should be aware that CD diagnosed in older ages may represent a distinct phenotype, one in which serologic responses to microbial antigens are less common.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
This work was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), number T32 DK067872 Research Training in Gastroenterology Grant. Laboratory testing and specimen delivery was funded by Prometheus Laboratories Inc.
Disclosure
The authors report no conflicts of interest in this work.
References
- SartorRBMicrobial influences in inflammatory bowel diseasesGastroenterology2008134257759418242222
- MainJMcKenzieHYeamanGRAntibody to Saccharomyces cerevisiae (bakers’ yeast) in Crohn’s diseaseBMJ19882976656110511063143445
- PappMAltorjayIDotanNHungarian IBD Study GroupNew serological markers for inflammatory bowel disease are associated with earlier age at onset, complicated disease behavior, risk for surgery, and NOD2/CARD15 genotype in a Hungarian IBD cohortAm J Gastroenterol2008103366568118047543
- TarganSRLandersCJYangHAntibodies to CBir1 flagellin define a unique response that is associated independently with complicated Crohn’s diseaseGastroenterology200512872020202815940634
- ArnottIDLandersCJNimmoEJSeroreactivity to microbial components in Crohn’s disease is associated with disease severity and progression, but not NOD2/CARD15 genotypeAm J Gastroenterol200499122376238415571586
- DassopoulosTFrangakisCCruz-CorreaMAntibodies to saccharomyces cerevisiae in Crohn’s disease: higher titers are associated with a greater frequency of mutant NOD2/CARD15 alleles and with a higher probability of complicated diseaseInflamm Bowel Dis200713214315117206688
- SuttonCLKimJYamaneAIdentification of a novel bacterial sequence associated with Crohn’s diseaseGastroenterology20001191233110889151
- MowWSVasiliauskasEALinYCAssociation of antibody responses to microbial antigens and complications of small bowel Crohn’s diseaseGastroenterology2004126241442414762777
- LandersCJCohavyOMisraRSelected loss of tolerance evidenced by Crohn’s disease-associated immune responses to auto- and microbial antigensGastroenterology2002123368969912198693
- CoukosJAHowardLAWeinbergJMBeckerJMStucchiAFFarrayeFAASCA IgG and CBir antibodies are associated with the development of Crohn’s disease and fistulae following ileal pouch-anal anastomosisDig Dis Sci20125761544155322311367
- FleshnerPIppolitiADubinskyMBoth preoperative perinuclear antineutrophil cytoplasmic antibody and anti-CBir1 expression in ulcerative colitis patients influence pouchitis development after ileal pouch-anal anastomosisClin Gastroenterol Hepatol20086556156818378498
- HuiTLandersCVasiliauskasESerologic responses in indeterminate colitis patients before ileal pouch-anal anastomosis may determine those at risk for continuous pouch inflammationDis Colon Rectum20054861254126215868228
- PapadakisKAYangHIppolitiAAnti-flagellin (CBir1) phenotypic and genetic Crohn’s disease associationsInflamm Bowel Dis200713552453017260364
- MarkowitzJKugathasanSDubinskyMAge of diagnosis influences serologic responses in children with Crohn’s disease: a possible clue to etiology?Inflamm Bowel Dis200915571471919107777
- LapidusABernellOHellersGPerssonPGLofbergRIncidence of Crohn’s disease in Stockholm County 1955–1989Gut19974144804869391246
- PolitoJM2ndChildsBMellitsEDTokayerAZHarrisMLBaylessTMCrohn’s disease: influence of age at diagnosis on site and clinical type of diseaseGastroenterology199611135805868780560
- QuezadaSMSteinbergerEKCrossRKAssociation of age at diagnosis and Crohn’s disease phenotypeAge Ageing201342110210622918090
- DesirBAmreDKLuSEUtility of serum antibodies in determining clinical course in pediatric Crohn’s diseaseClin Gastroenterol Hepatol20042213914615017619
- Lennard-JonesJEClassification of inflammatory bowel diseaseScand J Gastroenterol Suppl198917026 discussion 16–192617184
- HeresbachDAlexandreJLBretagneJFABERMADCrohn’s disease in the over-60 age group: a population based studyEur J Gastroenterol Hepatol200416765766415201578
- LakatosPLDavidGPandurTIBD in the elderly population: results from a population-based study in Western Hungary, 1977–2008J Crohns Colitis20115151321272797
- DubinskyMCLinYCDutridgeDWestern Regional Pediatric IBD Research AllianceSerum immune responses predict rapid disease progression among children with Crohn’s disease: immune responses predict disease progressionAm J Gastroenterol2006101236036716454844
- GuptaNBostromAGKirschnerBSPresentation and disease course in early- compared to later-onset pediatric Crohn’s diseaseAm J Gastroenterol200810382092209818796101
- PaulTBirnbaumAPalDKDistinct phenotype of early childhood inflammatory bowel diseaseJ Clin Gastroenterol200640758358616917397
- WalkerLJAldhousMCDrummondHEAnti-Saccharomyces cerevisiae antibodies (ASCA) in Crohn’s disease are associated with disease severity but not NOD2/CARD15 mutationsClin Exp Immunol2004135349049615008984
- ForcioneDGRosenMJKisielJBSandsBEAnti-Saccharomyces cerevisiae antibody (ASCA) positivity is associated with increased risk for early surgery in Crohn’s diseaseGut20045381117112215247177
- SmithBRArnottIDDrummondHENimmoERSatsangiJDisease location, anti-Saccharomyces cerevisiae antibody, and NOD2/CARD15 genotype influence the progression of disease behavior in Crohn’s diseaseInflamm Bowel Dis200410552152815472511
- HakimFTGressREImmunosenescence: deficits in adaptive immunity in the elderlyTissue Antigens200770317918917661905
- SeiboldFWeberPKleinRBergPAWiedmannKHClinical significance of antibodies against neutrophils in patients with inflammatory bowel disease and primary sclerosing cholangitisGut19923356576621612483