
Abstract
Objectives
The aim of the study was to evaluate the cost-effectiveness (CE) of treatment with eplerenone versus standard care in adult patients with New York Heart Association class II chronic heart failure and reduced left ventricular ejection fraction from the perspective of the Greek national health care payer.
Methods
A discrete-event model simulating the clinical course and respective outcomes of eplerenone as an add-on to standard therapy versus standard therapy alone based on the pivotal Eplerenone in Mild Patients Hospitalization and SurvIval Study in Heart Failure (EMPHASIS-HF) trial was locally adapted for the Greek setting. Data on medications followed the resource use from eplerenone in mild patients hospitalization and survival study in heart failure and were estimated on a lifetime basis (or until discontinuation). Cost calculations were based on year 2014, event costs (cardiovascular hospitalizations, adverse events, and devices) were sourced from published diagnosis-related groups. A 3% discount rate was applied. In order to test the robustness of the model projections, a range of deterministic and probabilistic sensitivity analyses were carried out.
Results
Over a patient’s lifetime, the addition of eplerenone to standard care compared to standard care alone led to an incremental gain of 1.33 quality-adjusted life-years (QALYs) (6.53 vs 5.20 QALYs, respectively) as well as an increase in the cost of treatment by €2,160; these outcomes produced an incremental CE ratio of €1,624/QALY for the Greek setting. On the basis of probabilistic sensitivity analysis, there was a 100% likelihood of eplerenone being cost-effective versus standard care at a threshold of €3,500/QALY.
Conclusion
This analysis indicates that eplerenone may be a cost-effective option versus standard care accompanied by additional clinical benefits and an added incremental cost at an acceptable, if not low, CE ratio. The results are consistent with the previously published studies on the CE of eplerenone as an add-on therapy to standard care, such as those regarding the health care settings of Spain, the UK, and Australia.
Introduction
Heart failure (HF) represents a major public health issue with a complex pathology and disease management pattern as well as high prevalence.Citation1,Citation2 About 1%–2% of the adult population in developed countries suffer from HF, with this percentage rising to over 10% when it comes to individuals aged 65 years or older.Citation3–Citation6 Although mortality rates have declined in the recent years,Citation7–Citation9 HF-related hospitalizations have substantially increased in the last decade, representing 1%–2% of all hospital admissions and becoming the leading reason for admission in individuals aged 65 years or older.Citation6 Moreover, readmission rates are quite high, ranging between 25% and 30% at 3 months and about 50% at 6 months post-discharge.Citation10,Citation11 Consequently, HF significantly impacts health care budgets internationally, with hospitalization admissions accounting for the most substantial part of this burden.Citation12–Citation14 Apart from the in-hospital part of patient management, the complexity of HF as a clinical problem and the associated comorbidities contributing to the progression of the disease and thus higher hospitalization rates and polypharmacy, lead to a subsequent and continuous increase in expenditures attributed to HF.Citation15–Citation17
A key objective in HF management is, therefore, to alleviate symptoms, reduce the occurrence and need for hospitalizations, and, subsequently, increase survival and improve the patients’ quality of life.Citation5,Citation18,Citation19 Treatment options such as angiotensin-converting enzyme inhibitors and beta blockers, although effective in some aspects of the treatment, have not yet shown the desired outcomes in terms of clinical efficacy.Citation5,Citation18,Citation19 In this light, newer and emerging treatments could play a role in the future of patient management and improved clinical results. Among those, eplerenone, a selective mineralocorticoid-receptor antagonist, also known as an aldosterone antagonist, has been indicated for patients with New York Heart Association (NYHA) class II chronic heart failure (CHF) with reduced left ventricular ejection fraction (LVEF), in addition to standard therapy, on the basis of improved clinical outcomes, that is, reduced cardiovascular (CV) mortality and morbidity, in adult patients with NYHA class II CHF and left ventricular systolic dysfunction (LVEF ≤30%).Citation20,Citation21
The implementation of adequate and sustainable health policies, particularly when considering conditions with significant prevalence and large expenditure such as CHF, seems imperative at a time when health resources are becoming even scarcer and health care systems have to allocate them in the most efficient way. In order to achieve these objectives, economic evaluation methods are indispensable tools in the decision-making process.
The aim of this study was to evaluate the cost-effectiveness (CE) of treatment with eplerenone in adult patients with NYHA class II CHF and reduced LVEF in Greece, from the perspective of a health care system at a time under severe financial constraints and austerity.
Methods
Health economic model
A discrete-event simulation economic model constructed on the basis of the reported outcomes of a pivotal study of eplerenone, the Eplerenone in Mild Patients Hospitalization and SurvIval Study in Heart Failure (EMPHASIS-HF) trial,Citation21 and previously publishedCitation22 was locally adapted for the Greek health care setting.
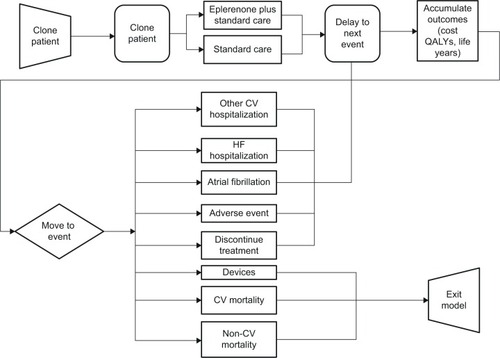
The purpose of the model was to simulate the clinical course and respective outcomes over a patient’s lifetime of two treatment alternatives: eplerenone as per trial protocol, starting dose of 25 mg once daily increased at 4 weeks to 50 mg once daily as an add-on to standard therapy versus standard therapy alone ().
Figure 1 Model structure.
Abbreviations: CV, cardiovascular; HF, heart failure; QALYs, quality-adjusted life-years.
Patient population in the model follows the demographic and clinical characteristics of patients in the EMPHASIS-HF trial,Citation21 that is, all patients were NYHA class II, had a mean age of 69 years, had a mean LVEF of 26%, and 78% of patients were male. Concomitant medication usage was reported at trial enrollment and as per trial protocol, subjects were to remain on the same dosing throughout the trial duration;Citation21 it was therefore assumed that subjects remained on the same pharmacotherapy for their lifetime (85% treated with diuretics, 78% with angiotensin-converting enzyme inhibitors, 19% with angiotensin receptors blockers, 87% with beta blockers, 88% with antithrombotics including antiplatelet or oral anticoagulants, and 63% with lipid-lowering agents).Citation21
illustrates the outline of the model and patient flows/projections.Citation22 In brief, individual times to events are assigned to each simulated patient for each model event. One identical patient is “cloned” and follows each treatment arm. Probabilities of future events are estimated based on risk equations for each event derived from patient-level data from EMPHASIS-HF (time-dependent distributions).Citation21 Thus, treatment efficacy is a factor that influences the occurrence and time of occurrence of a series of events such as HF hospitalization, other CV hospitalization, new-onset atrial fibrillation, implantation of cardiac resynchronization therapy (CRT) or implantable cardioverter defibrillator (ICD) devices, adverse events, discontinuation of eplerenone, CV mortality, and other causes of mortality, all of which were recorded in the EMPHASIS-HF trial. Patients remain in the model until death occurs, or are given an ICD or CRT device. The model accurately projects the within-trial outcomes;Citation22 for the time beyond the trial follow-up period, the model also provides a reasonable approximation of current survival estimates for chronic systolic HF patients, with a mean survival of approximately 8 years in the standard care arm.
The model calculates the resource use associated with treatment: drug costs of active treatment and concomitant medications, disease monitoring and disease-related events. Moreover, based on the clinical outcomes of treatment, health-related quality of life estimations in the form of utilities were also employed as described previouslyCitation22 and also shown in .
Table 1 Inputs for medication, event costs, and utilities used within the model (input values for the base case and sensitivity analysis are shown)
Treatment discontinuations were taken from the EMPHASIS-HF trial, using the proportions of patients discontinuing after each type of event.Citation22 Time to event was based on probabilistic distributions and outcomes were accumulated for 25,000 patients for each arm.
Model inputs
The analysis adopts the perspective of a third-party payer, the largest social security fund in Greece and, thus, calculates only direct resource use and costs (inpatient and outpatient). With regards to cost inputs, prices and diagnosis-related group tariffs were sourced from publicly available sources,Citation23,Citation24 or published literatureCitation25 (). Data on medications follow the resource use from the EMPHASIS-HF, and are estimated on a lifetime basis (or until discontinuation).Citation21 Event costs (sourced from published diagnosis-related groups) represent the acute phase (in case of hospitalization) and do not contain follow-up costs. Model structure and inputs on resource use were verified by two clinical experts from the Greek health care setting. The costs for events (CV hospitalizations, adverse events, and devices) were based upon the proportion of patients experiencing each of those events in the EMPHASIS-HF trial. Cost of devices refers to the cost of medical procedure for the application of the device as well as the cost of the device itself. Due to nonavailability of a reliable estimate, the cost of death was not included in the model as a conservative assumption. Cost calculations were based on year 2014,Citation23,Citation24 and a 3% discount rate was applied.
Utility values were taken from published literature and, specifically, calculated using the utility formula from Göhler et alCitation26 using the baseline characteristics of the patients within the EMPHASIS-HF trial. The occurrence of events was accompanied by a decrement, proportional to the severity of the event.Citation27–Citation29 The utility values used within the model are summarized in .
The remaining life span and quality of life for patients receiving ICD or CRT devices were calculated using the hazard ratios (compared to standard care treatment as within the placebo arm of the trial) provided previously.Citation30
Sensitivity analysis
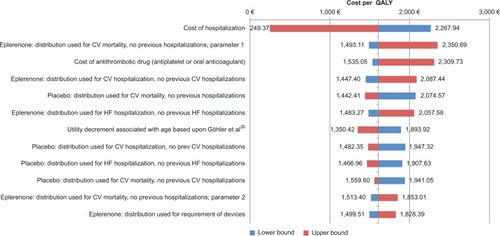
Where possible, information on uncertainty was obtained from the publication used for model inputs or directly from clinical trial data.Citation21,Citation22 Costs were modeled using a gamma distribution, utilities, and proportions using a beta distribution. Uniform distributions were used where maximum and minimum values were given within the literature and the applicability of a mean value within the range was uncertain. Upper and lower bound limits of inputs as well as type of distribution used in the sensitivity analysis are shown in . In order to test the robustness of the model projections, a range of deterministic sensitivity analyses was carried out by varying a number of scenario parameters within their likely range (95% confidence intervals) ().
Figure 2 Tornado diagram of deterministic sensitivity analysis.
In addition to the above, a probabilistic sensitivity analysis (PSA) was also performed. In the PSA, inputs for times to events, costs, and utility values were assigned a probability distribution and were stochastically varied. Outcomes were produced via a Monte Carlo simulation method with 100 iterations.
Results
presents the discounted results of the analysis. Over a patient’s lifetime, the addition of eplerenone to standard care versus standard care alone led to an incremental gain of 1.33 quality-adjusted life-years (QALYs) (6.53 vs 5.20 QALYs, respectively) as well as an increase in the cost of treatment by €2,160. These outcomes produced an incremental cost-effectiveness ratio (ICER) of €1,624/QALY for the Greek setting.
Table 2 Base case results from the discrete event simulation model (discounted)
shows a breakdown of the costs for each treatment arm for the Greek setting based on the model adaptation. The main differences in costs between treatment strategies are seen in the costs associated with HF hospitalizations, which are lower in the case of eplerenone; the costs of devices; and the cost of pharmacotherapy; this may be partly due to the extended life expectancy of those receiving eplerenone versus standard therapy (8.18 vs 6.52 life years, discounted).
Table 3 Cost results from the discrete event simulation model (€, discounted)
The results of the deterministic sensitivity analyses are presented in . It can be seen from the Tornado plots that the most sensitive model parameters are, in particular, the cost of HF-related hospitalization, as well as the distributional parameters for CV mortality when no previous hospitalizations have been experienced, and the cost of antithrombotic drug used (antiplatelet or oral anticoagulant). Nevertheless, the model seemed robust in its predictions and the results remained favorable for eplerenone in the analysis undertaken.
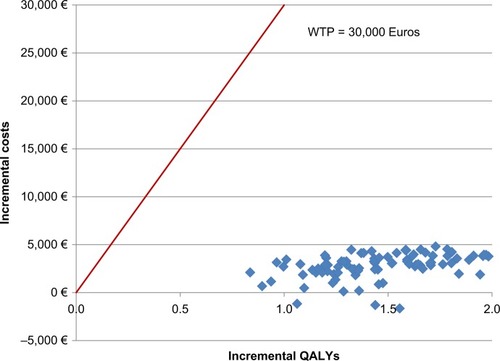
Similarly, probabilistic analyses conducted imply robustness of the model (). The probabilistic iterations of the model demonstrate that, in all cases, eplerenone provides a QALY benefit over standard care (overall mean ICER of €1,896). The ICERs are well below an acceptability threshold range of £20,000–£30,000/QALY gained (based on the upper and lower acceptability thresholds used in the National Institute for Health and Care Excellence guidance for economic evaluationsCitation31), although no explicit criterion of willingness to pay exists for Greece and much debate exists globally around CE threshold policy.Citation32,Citation33
Figure 3 Scatter plot of incremental quality-adjusted life expectancy and lifetime costs for eplerenone vs placebo (the red line represents the threshold of WTP at €30,000).
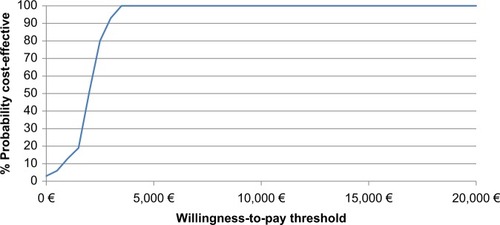
As shown in , eplerenone was a cost-effective treatment choice compared to standard care in 100% of the iterations for any threshold over €3,500/QALY gained.
Figure 4 Cost-effectiveness acceptability curve for eplerenone vs standard care.
Discussion
This analysis aimed at evaluating the clinicoeconomic value of adding eplerenone to the standard therapy of adult patients with NYHA class II HF and reduced LVEF in a setting characterized by severe constraints and deep austerity and contractionary measures. The results of the evaluation indicate that under the present analysis, eplerenone represents a cost-effective option vs standard care accompanied by additional clinical benefit and an added incremental cost at an acceptable, if not low, cost-effectiveness ratio. The core results proved to be rather robust to a series of one-way sensitivity analyses. On the basis of a PSA approach, there was a 100% likelihood of eplerenone being cost-effective versus standard care at a threshold of €3,500/QALY.
The present results are consistent with the previously published studies on the CE of eplerenone as an add-on therapy to standard care, such as those regarding the health care settings of Spain,Citation22 the UK,Citation22 and Australia,Citation34 on the basis of clinical efficacy data from the EMPHASIS-HF trial and, also, for the US,Citation35 France,Citation36 Switzerland,Citation37 and the NetherlandsCitation38 based on clinical efficacy data from the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) trialCitation39 referring to a different study population than the one used in this analysis – namely patients with HF after recent myocardial infarction.
As with any study of this kind, the present one is subject to some limitations that should be acknowledged. First of all, a limitation arises from the fact that the study population, for reasons of consistency and ability to compare the results at an international level, follows the characteristics of the population of the EMPHASIS-HF trial. This could suggest that a discrepancy of the characteristics of the study population and the actual population of Greek HF patients could exist. However, the multicenter nature of the trial with Greek patients also enrolled and the fact that the characteristics of the patients enrolled in EMPHASIS-HF are not dissimilar to typical well-treated patients seen in hospital practice (inpatient or outpatient) across EuropeCitation1,Citation40 could suggest that those discrepancies are not to a notable extent. Moreover, the results of the extensive sensitivity analysis suggest that even if there were notable differences, they would produce a rather negligible effect on the main tendency of outcomes (favorable CE).
Another limitation of the analysis stems from the fact that it is performed using a third-party payer perspective, that is, the perspective of social insurance. A third-party payer perspective does not include costs to society, mainly the productivity losses as a result of the disease and the costs of informal care. The latter could constitute an important cost variable, especially for patients whose daily activities are severely impaired by the CV events associated with HF. Inclusion of such costs typically favors the treatment that averts most clinical events, compared to alternatives, whereas exclusion of societal costs constitutes a conservative approach for the most efficacious alternative (in this case, eplerenone).
Finally, as the EMPHASIS-HF trial was stopped early, due to the evidence of early benefit in the eplerenone-treated arm compared to the standard of care population, there could be some uncertainty regarding the long-term outcomes of eplerenone in the available clinical data. This uncertainty in the clinical data has, however, been included within the modeling approach used and examined within both probabilistic and deterministic sensitivity analyses and has also been discussed and addressed in other economic evaluations of eplerenone that source their efficacy data from EMPHASIS-HF (indicatively, Lee et alCitation22).
In an era of scarce resources and ever-increasing health care needs, rational allocation of resources is an absolute necessity. In this decision-making process, CE analysis can be a useful tool in an attempt to quantify both the clinical benefits as well as the costs associated with each treatment option. Based on this line of thought, the present analysis aimed to evaluate the costs and effects of the addition of a newer treatment option for patients with NYHA class II chronic HF to the current standard of care and concluded that this intervention is a cost-effective option within the Greek context.
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank Becky Pennington for her original work on developing the economic model, as well as John Vincent and Katharina Lins for their valuable comments on improving the manuscript.
Disclosure
DL is an employee of BresMed and was a paid consultant to Pfizer in connection with the sensitivity analysis and development of this manuscript. AB and GS are employees of Pfizer Hellas. The authors report no other conflicts of interest in this work.
References
- ClelandJGSwedbergKFollathFThe EuroHeart Failure survey programme – a survey on the quality of care among patients with heart failure in Europe. Part 1: patient characteristics and diagnosisEur Heart J200324544246312633546
- HeidenreichPAAlbertNMAllenLAForecasting the impact of heart failure in the United States: a policy statement from the American Heart AssociationCirc Heart Fail20136360661923616602
- AzadNLemayGManagement of chronic heart failure in the older populationJ Geriatr Cardiol201411432933725593582
- MasoudiFAHavranekEPKrumholzHMThe burden of chronic congestive heart failure in older persons: magnitude and implications for policy and researchHeart Fail Rev20027191611790919
- McMurrayJJAdamopoulosSAnkerSDESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the task force for the diagnosis and treatment of acute and chronic heart failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESCEur J Heart Fail201214880386922828712
- ZannadFAgrinierNAllaFHeart failure burden and therapyEuropace200911Suppl 5v1v919861384
- CowieMRWoodDACoatsAJThompsonSGSureshVPoole-WilsonPASuttonGCSurvival of patients with a new diagnosis of heart failure: a population based studyHeart200083550551010768897
- HobbsFDRoalfeAKDavisRCDaviesMKHareRMidlands Research Practices Consortium (MidReC)Prognosis of all-cause heart failure and borderline left ventricular systolic dysfunction: 5 year mortality follow-up of the Echocardiographic Heart of England Screening Study (ECHOES)Eur Heart J20072891128113417459902
- Richard HobbsFDClinical burden and health service challenges of chronic heart failureBr J Gen Pract20106057761161520822695
- FilippatosGFarmakisDBistolaVKaravidasAMebazaaAMaggioniAPParissisJTTemporal trends in epidemiology, clinical presentation and management of acute heart failure: results from the Greek cohorts of the Acute Heart Failure Global Registry of Standard Treatment and the European Society of Cardiology-Heart Failure pilot surveyEur Heart J Acute Cardiovasc Care Epub201434
- GiamouzisGKalogeropoulosAGeorgiopoulouVHospitalization epidemic in patients with heart failure: risk factors, risk prediction, knowledge gaps, and future directionsJ Card Fail2011171547521187265
- AmbrosyAPFonarowGCButlerJThe global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registriesJ Am Coll Cardiol201463121123113324491689
- LeeWCChavezYEBakerTLuceBREconomic burden of heart failure: a summary of recent literatureHeart Lung200433636237115597290
- StewartSJenkinsABuchanSMcGuireACapewellSMcMurrayJJThe current cost of heart failure to the National Health Service in the UKEur J Heart Fail20024336137112034163
- ChongVHSinghJParryHSaundersJChowdhuryFManciniDMLangCCManagement of non-cardiac comorbidities in chronic heart failureCardiovasc Ther201533530031526108139
- CookCColeGAsariaPJabbourRFrancisDPThe annual global economic burden of heart failureInt J Cardiol2014171336837624398230
- LangCCManciniDMNon-cardiac comorbidities in chronic heart failureHeart200793666567116488925
- GandhiPUPinneySManagement of chronic heart failure: biomarkers, monitors, and disease management programsAnn Glob Health2014801465424751564
- WilliamsRPOakeshottPDiagnosis and management of chronic heart failureBMJ2014348g142924523371
- National Organization for MedicinesSummary of Product Characteristics: Inspra 50mg/tabGreece2015 Available from: http://services.eof.gr/drugsearch/block/resource/Mjk1MTU5OTIy/SPC_2650002_3.pdfAccessed May 10, 2015
- ZannadFMcMurrayJJKrumHEplerenone in patients with systolic heart failure and mild symptomsN Engl J Med20113641112121073363
- LeeDWilsonKAkehurstRCost-effectiveness of eplerenone in patients with systolic heart failure and mild symptomsHeart2014100211681168724993605
- Official Government Gazette of Greece, Issue B, Number 946, March 27, 2012. [Diagnostic Related Groups].
- Official Government Gazette of Greece, Issue B, Number 2336, August 29, 2014. [Positive list of reimbursed medicines].
- ParissisJAthanasakisKFarmakisDDeterminants of the direct cost of heart failure hospitalization in a public tertiary hospitalInt J Cardiol2015180464925438208
- GöhlerAGeislerBPManneJMUtility estimates for decision-analytic modeling in chronic heart failure – health states based on New York Heart Association classes and number of rehospitalizationsValue Health200912118518718647251
- BergJLindgrenPNieuwlaatRBouinOCrijnsHFactors determining utility measured with the EQ-5D in patients with atrial fibrillationQual Life Res201019338139020108048
- MowattGValeLPerezJSystematic review of the effectiveness and cost-effectiveness, and economic evaluation, of home versus hospital or satellite unit haemodialysis for people with end-stage renal failureHealth Technol Assess2003721174
- SullivanPWSlejkoJFSculpherMJGhushchyanVCatalogue of EQ-5D scores for the United KingdomMed Decis Making201131680080421422468
- FoxMMealingSAndersonRDeanJSteinKPriceATaylorRSThe clinical effectiveness and cost-effectiveness of cardiac resynchronisation (biventricular pacing) for heart failure: systematic review and economic modelHealth Technol Assess20071147iiiivix248
- NICEGuide to the Methods of Technology Appraisal 2014 Available from: http://www.nice.org.uk/article/pmg9/resources/non-guidance-guide-to-the-methods-of-technology-appraisal-2013-pdf2013Accessed May 10, 2015
- EichlerHGKongSXGerthWCMavrosPJonssonBUse of cost-effectiveness analysis in health-care resource allocation decision-making: how are cost-effectiveness thresholds expected to emerge?Value Health20047551852815367247
- NimdetKChaiyakunaprukNVichansavakulKNgorsurachesSA systematic review of studies eliciting willingness-to-pay per quality-adjusted life year: does it justify CE threshold?PLoS One2015104e012276025855971
- AdemiZPasupathiKKrumHLiewDCost effectiveness of eplerenone in patients with chronic heart failureAm J Cardiovasc Drugs201414320921624610254
- ZhangZMahoneyEMKolmPSpertusJCaroJWillkeRWeintraubWSCost effectiveness of eplerenone in patients with heart failure after acute myocardial infarction who were taking both ACE inhibitors and beta-blockers: subanalysis of the EPHESUSAm J Cardiovasc Drugs2010101556320104935
- de PouvourvilleGSolesseABeillatMCost-effectiveness analysis of aldosterone blockade with eplerenone in patients with heart failure after acute myocardial infarction in the French context: the EPHESUS studyArch Cardiovasc Dis2008101951552119041835
- SzucsTDHolmMVSchwenkglenksMZhangZWeintraubWSBurnierMErnePCost-effectiveness of eplerenone in patients with left ventricular dysfunction after myocardial infarction – an analysis of the EPHESUS study from a Swiss perspectiveCardiovasc Drugs Ther200620319320416775667
- van GenugtenMLWeintraubWSZhangZVoorsAACost-effectiveness of eplerenone plus standard treatment compared with standard treatment in patients with myocardial infarction complicated by left ventricular systolic dysfunction and heart failure in the NetherlandsNeth Heart J2005131139340025696430
- PittBRemmeWZannadFEplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarctionN Engl J Med2003348141309132112668699
- NICORNational Heart Failure Audit Available from: http://www.hqip.org.uk/assets/NCAPOP-Library/Heart-Failure-Audit-Report-NICOR-2010-2011.pdf2012Accessed May 10, 2015