
Abstract
Purpose
Osteoporosis is asymptomatic morbidity of the elderly which develops slowly over several years. Osteoporosis diagnosis has typically involved Fracture Risk Assessment (FRAX) followed by dual energy X-ray absorptiometry (DXA) in specialist care. Point-of-care pulse-echo ultrasound (PEUS) was developed to overcome DXA-related access issues and to enable faster fracture prevention treatment (FPT) initiation. The objective of this study was to evaluate the cost-effectiveness of two proposed osteoporosis management (POMs: FRAX→PEUS-if-needed→DXA-if-needed→FPT-if-needed) pathways including PEUS compared with the current osteoporosis management (FRAX→DXA-if-needed→FPT-if-needed).
Materials and methods
Event-based probabilistic cost–utility model with 10-year duration for osteoporosis management was developed. The model consists of a decision tree for the screening, testing, and diagnosis phase and is followed by a Markov model for the estimation of incidence of four fracture types and mortality. Five clinically relevant patient cohorts (potential primary FPT in women aged 75 or 85 years, secondary FPT in women aged 65, 75, or 85 years) were modeled in the Finnish setting. Generic alendronate FPT was used for those diagnosed with osteoporosis, including persistence overtime. Discounted (3%/year) incremental cost-effectiveness ratio was the primary outcome. Discounted quality-adjusted life-years (QALYs), payer costs (year 2016 value) at per patient and population level, and cost-effectiveness acceptability frontiers were modeled as secondary outcomes.
Results
POMs were cost-effective in all patient subgroups with noteworthy mean per patient cost savings of €121/76 (ranges €107–132/52–96) depending on the scope of PEUS result interpretation (test and diagnose/test only, respectively) and negligible differences in QALYs gained in comparison with current osteoporosis management. In the cost-effectiveness acceptability frontiers, POMs had 95%–100% probability of cost-effectiveness with willingness to pay €24,406/QALY gained. The results were robust in sensitivity analyses. Even when assuming a high cost of PEUS (up to €110/test), POMs were cost-effective in all cohorts.
Conclusion
The inclusion of PEUS to osteoporosis management pathway was cost-effective.
Introduction
Osteoporosis is a typically asymptomatic morbidity of the elderly which develops slowly over several years.Citation1–Citation3 Osteoporosis weakens the bones through bone loss after the age of 40 years and increases bone loss after menopause and during the final years of life, making them fragile and more likely to break. Osteoporosis diagnosis often occurs only after a minor fall or sudden impact causes a bone fracture.Citation4–Citation6 Clinically, the World Health Organization defines osteoporosis with reference to bone mineral density. Bone mineral density in adults is usually denoted by its T-score relative to the peak bone mass distribution in healthy women aged 20–40 years, and a T-score ≤−2.5 indicates osteoporosis.Citation7
Osteoporosis is a common illness with a prevalence estimate of 400,000 (around 7.3% of the population in the year 2016)Citation8 in Finland. Each year, ~6,000 first and 1,000 repeat hip fractures and a total of 30,000–40,000 osteoporosis-related fractures occurCitation5 mostly in patients without osteoporosis diagnosis.Citation6 Although the incidences of some fractures have decreased in Finland (potentially due to improved functional ability, osteoporosis management, and other measures),Citation9–Citation12 there is an increase in incidence of some fractures.Citation13–Citation15 The fracture peak may be just emerging in countries such as Finland that had a high birth rate after the second world war, because the incidence of fractures increases exponentially with age.Citation5 Globally, osteoporosis management is a concern in postmenopausal women. Approximately 40% of women and about 14% of men over 50 years of age will have a hip, vertebral or wrist fracture in their remaining lifetime.Citation16–Citation18
Besides the recommendation of adequate dietary calcium and vitamin D intakeCitation5 (211,833 and 6,050 Finns with reimbursement for calcium and vitamin D in the year 2016, respectively), reimbursed fracture prevention treatments (FPTs) in Finland can include hormone replacement therapy (190,194 estrogen, 15,925 testosterone), bisphosphonates (31,549: alendronate [22,028], risedronate [6,310], ibandronate [3,139], clodronate [229], zoledronic acid [54]), denosumab (15,610), strontium ranelate (530), teriparatide (457), and calcitonin (22).Citation19 In osteoporosis management, two types of osteoporotic fracture prevention are distinguished: primary osteoporotic fracture prevention, which aims to prevent any osteoporosis-related fracture, and secondary osteoporotic fracture prevention, which aims to prevent subsequent osteoporosis-related fracture in osteoporotic individuals who have already suffered a fracture.
Osteoporosis testing of high-risk populations is effective. The high-risk populations for the testing include women aged >65 years with other risk factors such as heavy smoking or parental osteoporosis-related fracture; or individuals with fracture due to low-energy impact; comorbidities or pharmacologic therapies increasing osteoporosis risk; incidental observations on X-rays; or unexplained body height loss.Citation5 However, identifying the high risk is difficult, and testing bone mineral density in all is not indicated.Citation7 Recent guidelinesCitation4,Citation5,Citation20,Citation21 and Finnish practiceCitation22 recommend that the 10-year fracture risk, estimated using the proprietary Fracture Risk Assessment (FRAX) tool,Citation23 should be used to screen potential osteoporosis for testing bone mineral density.
The medical need for effective on-site diagnostics is high, because around three-quarters of osteoporosis cases remain undiagnosedCitation24 and many osteoporotic individuals are not identified until they experience fracture. Thus, potentially more than three-quarters of osteoporotic individuals do not receive any FPT. This is no surprise, as osteoporosis testing with the current methods alone is challenging.Citation6
To overcome the limitations of using mostly radiographic, large diagnostic tools which are rarely available in primary care facilities, a novel handheld device based on the pulse-echo ultrasound technology (pulse-echo ultrasonometry or ultrasonography [PEUS], Bindex®; Bone Index Finland, Kuopio, Finland) was developed.Citation25–Citation29 PEUS is used as a point-of-care osteoporosis testing-diagnosis tool after FRAX screening and it can help avoid dual-energy X-ray absorptiometry (DXA) for most postmenopausal women.Citation25,Citation26,Citation29 The bone mineral density estimates obtained using PEUS have correlated very well with those obtained with the DXA methodCitation26,Citation28 and are associated with clinically confirmed fractures in the previous 5 years.Citation25 The DXA has been the gold standard of choice in the bone mineral density-based diagnostics.Citation5,Citation20,Citation21,Citation30
The cost-effectiveness of current care-based conventional osteoporosis management (COM)Citation4,Citation5,Citation7,Citation20–Citation22 and two proposed osteoporosis managements (POM) including FRAX screening, testing, diagnosis, and FPT if needed was modeled. Based on a literature search in the PubMed database, no assessments have been published on the subject matter. Overall, evidence-based health economic evaluations including the screening, testing, diagnosing, and FPT have been rarely conducted.
Materials and methods
The Patients-Intervention-Comparator-Outcome-Setting-Time-Effects-Perspective-Sensitivity analysis (PICOSTEPS) principle was applied.Citation31,Citation32 PICOSTEPS is in line with a health technology assessment guideline prepared by the Finnish Medicines Agency,Citation33 and Finnish official guidance for the cost-effectiveness analyses attached with pharmaceuticals reimbursement applications submitted to the Finnish Pharmaceuticals Pricing Board.Citation34 Furthermore, PICOSTEPS describes the essential components of evidence-based health economic and outcomes research analytical framework in the order of importance.Citation31
Patients
Five risk cohorts of postmenopausal women were modeled based on clinical rationale: women aged 65 years with secondary osteoporotic fracture prevention, and women aged 75 or 85 years with primary or secondary osteoporotic fracture prevention.Citation5 The other characteristics were: T-score −2.8 (normal distribution, 95% CI −3.1 to −2.5) for osteoporotic and −0.25 (95% CI −1.00 to 0.50) for non-osteoporotic,Citation23 and no parental hip fracture, oral glucocorticoid therapy, rheumatoid arthritis, or alcoholism. The potential events included hip (institutionalized to long-term care after the hip fracture or not institutionalized), vertebral, wrist, and other fractures.
Intervention and comparator
The cost-effectiveness of osteoporosis management pathways () was simulated in the osteoporosis screening–testing–diagnosis model, namely, the POM (FRAX followed by (→) PEUS-if-needed→DXA-if-needed→FPT-if-needed) and COM (FRAX→DXA-if-needed→FPT-if-needed). COM as a comparator was based on its clinical rationale and recommendation in FinlandCitation5 and elsewhere.Citation4,Citation7,Citation20–Citation22,Citation30 POM was included as the intervention based on its resultsCitation25–Citation29 and potential affordability.
Figure 1 Decision tree: POM pathways are on the left-hand side and the COM pathway is on the right-hand side.
Abbreviations: COM, conventional osteoporosis management; DXA, dual-energy X-ray absorptiometry; FRAX, Fracture Risk Assessment; PEUS, pulse-echo ultrasound technology; POM, proposed osteoporosis management; POMA, proposed osteoporosis management pathway A; POMB, proposed osteoporosis management pathway B.
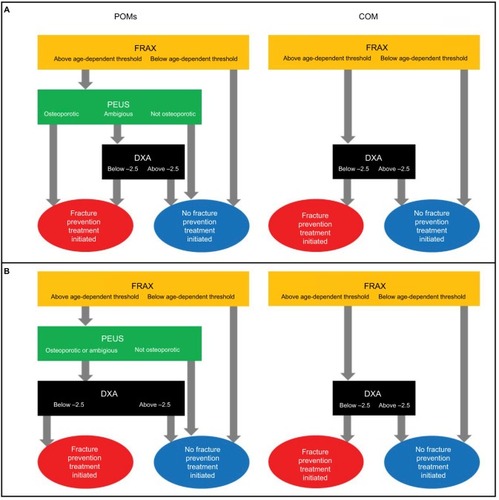
The need for PEUS and/or DXA in the model is based on the age-dependent FRAX,Citation23 which predicts the 10-year fracture risk to help the clinical decision making.Citation5,Citation23 If the 10-year fracture risk exceeded the age-dependent threshold values of 5.9% (age 65–74 years), 11.7% (75–84), or 19.8% (85–) in the FRAX screening, intermediate fracture risk was present and bone mineral density was assessed (i.e., the individual underwent PEUS and/or DXA). If the 10-year fracture risk was below the age-dependent threshold values in the FRAX screening, low fracture risk was present and lifestyle advice and reassurance were given.
Outcome
The key outcome of the analysis was an incremental cost-effectiveness ratio: the difference in simulated costs divided by the difference in simulated effectiveness. Also, the mean costs and effectiveness were presented as secondary outcomes.
Setting
The event-based modeling approach with a clinical decision tree and a Markov extrapolation modelCitation35,Citation36 was selected to capture all relevant data and to simulate (5,000 iterations) the comprehensive osteoporosis management in Finland using Microsoft Excel 2016 with Visual Basic for Applications. A decision tree analysis was done to model the screening–testing–diagnosis process preceding the potential initiation of FPT (). A Markov modeling followed to assess the fractures and FPT (). The event-based modeling strategy was carried out as follows: specify diagnosis and determine initial cohort distribution, define the natural history of the disease (i.e., events and their risks), apply relative risk modifiers (i.e., patient characteristics and treatments), compute costs and effectiveness, and run the simulation model.
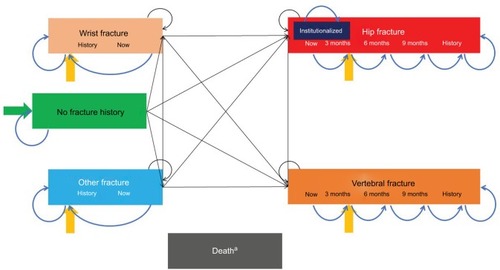
Figure 2 Markov model.
Testing and diagnosis: decision tree model
The osteoporosis screening–testing–diagnosis decision tree model () included COM and POM, and their sensitivity and specificity. FRAX constituted the initial screening tool common to both pathways,Citation23 with a mean accuracy rate of 1.000 (assumed normal 0.975–1.025 95% CI).
In the decision tree, PEUS was calibrated to the 90% sensitivity–specificity threshold in accordance with the International Society for Clinical Densitometry guidelinesCitation37,Citation38 and modeled using Dirichlet distribution (i.e., altogether 10% of PEUS results are false negatives or false positives and have incorrect osteoporosis management). Thus, cost-effectiveness analysis with correct and incorrect treatment pathways was needed to evaluate how much effectiveness is potentially lost when using the POM.
In the POM pathway A (POMA, ) of the decision tree, 32.6% of individuals have ambiguous PEUS results (between the 90% sensitivity–specificity calibration thresholds).Citation26 These individuals require and are provided a DXA measurement to verify the diagnosis. A recent real-world study confirmed the proportion of ambiguous PEUS results with the need of sending 32.5% of individuals to DXA investigation after PEUS measurement.Citation29 In POMA, both false positives and negatives occur up to 10% of the patients in total and are modeled accordingly. These results constituted initial cohort distribution for the Markov model in the case of POMA. Thus, in the POMA strategy, PEUS is used for osteoporosis testing and diagnosis,Citation25–Citation29 which is a potentially common strategy in the Finnish public sector based on the clinical and economic rationale.
In the POM pathway B (POMB, ) of the decision tree, both ambiguous and osteoporotic PEUS results require and receive a DXA measurement, which eliminates the false positives. These results constituted the initial cohort distribution for the Markov model in the case of POMB. Thus, in the POMB strategy, PEUS is used for osteoporosis testing only and a positive diagnosis is confirmed with DXA, which can be a potentially common strategy in, for example, the USA.
Bone fractures and prevention: Markov model
The fractures and FPT were modeled with a Markov state transition model. The transitions were determined by clinical outcomes and a hierarchy of fractures was assumed, with hip fractures being more serious than vertebral fractures, which were in turn more serious than wrist and other fractures (). Due to the duration of the fractures and available data, the Markov model had a 3-month cycle. Hip and vertebral fractures were represented as tunnel states because their costs and mortality depended on the time since the fracture. A state was used to model the proportion of individuals who were permanently institutionalized after a hip fracture.
In osteoporosis, the fracture risk can be reduced through FPT. A review of postmenopausal osteoporosis FPTs has been recently published,Citation39 and alendronate once weekly is recommended as the first-line FPT in Finland.Citation5 In addition, generic alendronate is the most affordable FPTCitation40 with a high number of reimbursements in FinlandCitation19 and it is also likely to be a cost-effective FPT.
Time
The modeling was limited to 10 years due to the age of most individuals, potential changes in the FPTs, and limited knowledge regarding the extrapolated effects beyond 10 years (FRAX represents 10-year risk).Citation7,Citation23 Conversions between rates and probabilities were performed using the common transformation methodology.Citation41 The annual discounting rate of effectiveness and costs was 3%.Citation33,Citation34
Effects
The long-term Markov fracture and FPT modeling included hip, vertebra, wrist, and other fractures. Finnish FRAX collaboration data demonstrated the 10-year risk of hip or any fracture in Finland per individual’s age, bone mineral density (T-score), and number of risk factors.Citation7,Citation23 To find osteoporotic fractures, US-based data on the age- and sex-specific relative risk of fracture attributable to osteoporosis were used.Citation42 Relative risk for fracture was increased in individuals with a prior fracture, which could be accounted for by using the FRAX risk lookup, where prior fracture is one of the risk factors.Citation23 The age-dependent results on the fracture rates in the USA were then used to split the Finnish 10-year risk estimate of any fracture into component types of vertebra, wrist, or other fracture and modelled in the Markov model.Citation42 The fracture prevention Markov model concurred with the health states used in earlier evaluations.Citation43 Furthermore, institutionalization risk to long-term facility after hip fracture was modeled based on the Finnish real-world evidence.Citation44
Alendronate 70 mg/week FPT was modeled for osteoporotic individuals. For them, the fracture occurrence was adjusted downward based on the distributional efficacy estimated from a published meta-analysis of FPT.Citation45,Citation46 Suboptimal FPT uptake (adherence) based on 20% adherence at 5 years modified the efficacy through persistence to mimic the real-world situation.Citation47,Citation46 In line with this modeling study, the study included postmenopausal women, naive to bisphosphonates, who received a first prescription of alendronate.Citation47 No rebound was assumed (i.e., FPT effect stops at the time of FPT discontinuation; ).
Table 1 Effect estimates, CI or SEs, and distributions applied
The individuals can die from any health state. The background mortality was modeled based on the year 2016 official Finnish mortality statistics,Citation48 excluding deaths due to osteoporosis (10th revision of the International Statistical Classification of Diseases codes M80 or M81).Citation48,Citation49 The FPT had an indirect effect through fractures to mortality. An elevated mortality relative risk of 4.53 during the first 6 months after the hip or vertebral fracture (1.75 in the subsequent 6 months and 1.78 thereafter) was modeled.Citation50,Citation42 Wrist or other fractures were not considered to increase mortality.
Finally, health-related quality of life was modeled using nationally representative age-, income-, education-, marital status-, and morbidity-adjusted Finnish EuroQol 5-dimensional 3-level scores for women based on a Tobit model,Citation51 and multiplicative health-related quality of life losses associated with the fractures.Citation46,Citation52 The EuroQol 5-dimensional 3-level scores used represent the most suitable health-related quality of life for a postmenopausal woman available for the Finn-ish modeling purposes. Alendronate use was conservatively assumed to be associated with reduction in health-related quality of life ().
Perspective
The analysis included direct costs based on the Finnish guidance,Citation33,Citation34 and applied third-party payer perspective common in the guidance of many European countries.Citation53–Citation62 The analysis included direct health-related costs (e.g., patient co-payments, FPTs, treatments, visits, hospitalizations, traveling)Citation33,Citation34 and excluded taxes, productivity losses (e.g., absenteeism, presenteeism, sickness allowances, pensions), other income transfers, and time costs.
Costs
The Finnish weekly cost of the most affordable generic alendronate 70 mg was €1.70, excluding value-added tax.Citation40 Fracture-associated costs were estimated based on the Finnish resource use in a representative national register study,Citation44 which was valued with the national Finnish unit costsCitation63 according to real values in the year 2016 ().Citation64 The national health care costsCitation63 were converted to year 2016 values using the latest official Finnish Communal Expenses Index for health care.Citation64 Traveling costsCitation65 were converted to 2016 real values using the transportation section of the latest official Finnish Consumer Price Index.Citation66 Due to lack of data, a recursive fracture was considered to have the same costs and consequences as the first fracture.
Table 2 Fracture costs (€, in the year 2016 real value)
Proprietary FRAX was available free of charge.Citation23 Finnish year 2016 price lists of hospital districts were searched to find the prices of DXA measurements. A price of €268 (incl. visit price) could be a representative input value (i.e., average of most affordable prices per district incl. visit was €297.50), with the lowest (€124.00, probably not feasible) and highest (€476.00) costs. The mean cost of specialist visit and the mean cost of DXA measurement alone would be €313.76 and €67.50, respectively, that is, a total of €381.26. However, for conservative results, €87.00 was used as the base case input for DXA cost. Thus, the total cost of DXA included one primary care doctor visit and travel (€133.26), the DXA test (€87.00, excluding visit) on the official Finnish price lists for communal invoicing, travels (€78.18),Citation65,Citation66 call (€27.88), and statement (€21.45).Citation63,Citation64
The total cost of the PEUS single-site test included primary care nurse visit and travel (€66.77),Citation63–Citation66 call (€27.88) and statement (€21.45),Citation63,Citation64 and PEUS test (€50.00), and the total cost of the DXA specified above for the proportion of individuals undergoing the DXA in POM. The assumed cost of PEUS may overestimate the true PEUS cost to Finnish health care.
Willingness to pay
A complicating factor when interpreting the results of cost-effectiveness analysis in the Finnish setting is the lack of an official willingness-to-pay threshold,Citation67–Citation69 a specific limit for additional investment to an additional quality-adjusted life year (QALY) gained.
In the UK, the most plausible willingness-to-pay threshold in non-end-of-life situations is £20,000Citation60 (€24,406, mean exchange rate €1=£0.81948 in the year 2016),Citation70 or maybe, in some cases, up to £30,000 (€36,609) per QALY gained.Citation60,Citation70 These willingness-to-pay thresholds may also be valid for the screening–testing–diagnosing–osteoporotic fracture prevention if needed process in Finland.Citation67–Citation69
Sensitivity
The robustness of results was tested using one-way and multiway sensitivity analysis scenarios. These included Patient, Setting, and Effects.
The sensitivity of probabilistic analysis was implemented based on distributions, and results were depicted in terms of a cost-effectiveness acceptability frontier.Citation71 The frontier showed the optimal strategies with the highest expected monetary net benefit (pay-off) as a function of willingness to pay.
Results
The average absolute costs saved with POMA vs. COM were €121/patient (1.3%), ranging from €107/patient (75 years old, primary or secondary osteoporotic fracture prevention) to €132/patient (85 years old, secondary osteoporotic fracture prevention). The relative savings with POMA ranged from 1.0%/patient (75 years old, secondary osteoporotic fracture prevention) to 1.7%/patient (65 years old, secondary osteoporotic fracture prevention). The average absolute costs saved with POMB vs. COM were €76/patient (0.8%), ranging from €52/patient (0.5%; 75 years old, secondary osteoporotic fracture prevention) to €96/patient (1.1%; 85 years old, primary osteoporotic fracture prevention), as shown in .
Table 3 Ten-year base case results with 3% per annum discounting: COM pathway vs. POM pathways
In a setting of 40,000 tested women per year, POMA could result in potential annual cost savings of around €4.8 million (range €4.3–5.3 million depending on the patient group). The respective potential annual cost savings with POMB could be €3.0 (€2.1–3.8) million.
Cost-effectiveness
COM resulted in a marginal average QALY gain of 0.001 in comparison with POMA. Due to the negligible QALY gain and additional costs, COM was not cost-effective (the incremental cost-effectiveness ratios range from €60,000 to 308,000/QALY gained) vs. POMA with the common willingness-to-pay threshold values. However, POMB dominated COM, as it resulted in negligible or similar QALY gain with lower costs ().
Sensitivity analyses
Multiple one-way and multiway sensitivity analysis scenarios were used ().
Table 4 Sensitivity analyses presenting incremental cost-effectiveness ratios and their changes: COM pathway vs. POM pathways
For the COM vs. POMA comparison, these sensitivity analyses scenarios included the following:
A. Base case
B. Mean T-score of −3.5 (severe osteoporosis)
C. No discounting
D. Discounting 5%/year
E. 50% initiate FPT
F. 75% initiate FPT
G. 10% adherent to FPT at 5 years
H. 30% adherent to FPT at 5 years
I. No disutility due to FPT
J. DXA cost of €124.00 (the most affordable cost based on the cost review)
K. DXA cost of €381.26 (the expected cost based on the cost review)
L. PEUS test cost assumption of €20.00
M. PEUS test cost assumption of €35.00
N. Institutionalization costs of €154.00/day (elderly home)Citation63
O. Fracture costs decreased by 25%
P. Fracture costs increased by 25%
Q. No travel costs included (direct health care costs only)
R. Travel costs doubled
S. DXA-related travel costs doubled
T. Mean of sensitivity analysis scenarios B–S.
For the COM vs. POMB comparison, the reported sensitivity analysis scenarios included the following:
U. Base case
V. Mean T-score of −3.5 (severe osteoporosis)
W. 30% adherent to FPT at 5 years
X. No travel costs
Y. No disutility due to FPT.
Based on the sensitivity analyses, the results were most sensitive to the large-scale changes in FPT (initiation proportion, disutility), DXA (cost, traveling), and T-score. Yet, POM remained the most cost-effective option and the base case analyses were conservative (i.e., did not benefit POM). For example, the analyses demonstrated that osteoporosis should be detected early and preferably before the first osteoporotic fracture, baseline T-score has significant impact on the cost-effectiveness, FPT should be initiated for osteoporosis and used persistently, DXA travel has the largest impact regarding traveling costs, and any increase in the potentially underestimated DXA-associated costs can significantly decrease the cost-effectiveness of COM.
Based on the simulations for different base case testing outcomes, the expected additional cost/patient due to the FPT assignment being based on the results of a slightly inaccurate PEUS was small (€35–61 for POMA, average being €46, and €0–22 for POMB, average being €7, over the 10 years; varying by risk group) in comparison with the total costs or cost savings. Based on a face validity assessment scenario with 100% sensitivity–specificity for PEUS, the QALYs were similar for COM and POM, and the expected average cost difference of €165 (average value’s range €162–168 dependent on the patient group) in favor of POM was observed (i.e., POM would be strongly dominant in the case of similar sensitivity–specificity of PEUS and DXA). On the other hand, in an unrealistic extreme sensitivity analysis scenario with 82% sensitivity–specificity threshold for PEUS, the average QALY difference increased with 0.001 between COM and POM in comparison to the COM vs. POMA base case, and the average cost difference decreased to €91 between COM and POM, resulting in €42,604/QALY gained for COM vs. POM.
POMA had 96%–100% probabilities for cost-effectiveness vs. COM at the €24,406 willingness to pay/QALY gained and depending on the patients modeled (). The respective results for POMB were 95%–100%. With the €36,609 willingness to pay/QALY gained, POMA had 82%–99% probabilities for cost-effectiveness. The respective probabilities for POMB were 92%–100%. With the €0 willingness to pay/QALY gained, POMA and POMB had 100% and 97%–100% probabilities for cost-effectiveness, respectively.
Figure 3 Cost-effectiveness acceptability frontiers with sensible willingness-to-pay values of €0–36,609 per quality-adjusted life year gained present high probabilities (82%–100%) of cost-effectiveness for POMA (upper part [A], PEUS is used for the osteoporosis testing and diagnosis) and POMB (lower part [B], patient tested with PEUS).
![Figure 3 Cost-effectiveness acceptability frontiers with sensible willingness-to-pay values of €0–36,609 per quality-adjusted life year gained present high probabilities (82%–100%) of cost-effectiveness for POMA (upper part [A], PEUS is used for the osteoporosis testing and diagnosis) and POMB (lower part [B], patient tested with PEUS).](/cms/asset/8dedf5df-1aa3-4d7b-81ea-36b11857b851/dceo_a_163237_f0003_c.jpg)
Finally, for descriptive purposes, reports the number of simulated fractures based on the treatment allocation and over the maximum time horizon of 10 years (mortality included) for a 75-year-old female without any significant clinical risk factors and with an average T-score of −2.8. Generally, the most frequent fractures include hip and other fractures. Given the incidence and unit cost of fractures, the highest expected cost impact for the first 3 months after a fracture was estimated for hip fractures.
Table 5 Simulated fractures during the maximum time horizon of 10 years for a 75-year-old non-smoking female with no parental hip fracture, no oral glucocorticoid, no rheumatoid arthritis, no alcoholism, and an average T-score of −2.8
Discussion
Recently, the cost-effectiveness of FPTs has been reviewed,Citation39 and the cost-effectiveness of osteoporosis testing and FPT has been debated.Citation30 This study assessed for the first time the incremental cost-effectiveness of two proposed (POMs: FRAX→PEUS-when-needed→DXA-when-needed) vs. conventional (COM: FRAX→DXA-when-needed) osteoporosis management pathways in Finland using generic alendronate FPT for osteoporotic individuals. POMs could result in payer cost savings, regardless of whether PEUS is used for both osteoporosis testing–diagnosing (POMA) or testing only (POMB). POM and the societal perspective appraised in countries such as Sweden would result in additional cost savings, as most of the indirect costs would be associated with the DXA measurement.
The incremental cost-effectiveness ratios of COM vs. POMA were high and POMB dominated COM, which indicated that COM would not be cost-effective in comparison to POMs in the Finnish setting or in most of the European settings. Although COM produced marginally more QALYs (0.001) vs. POMA due to false positives and negatives related to PEUS use, it was far too expensive to achieve reasonable cost-effectiveness. At €24,406 willingness to pay/QALY gained, POM had 95%–100% cost-effectiveness probability.
The osteoporosis management costs were reduced when PEUS was included. The additional cost due to the FPT assignment being based on the PEUS was small in comparison with the total costs. The results were sensitive to the large-scale changes in the FPT, DXA-associated costs, and T-score. However, POMs remained cost-effective vs. COM in the extensive sensitivity analyses.
Based on the explorative analyses, osteoporosis should be detected early and preferably before osteoporotic fracture, T-score has significant impact on the cost-effectiveness, and FPT should be initiated for osteoporosis and used persistently. If 40,000 women were screened per year and FPT was initiated for the osteoporotic, POMA or POMB could easily result in average annual savings of ~€5 or €3 million in the limited social and health care budgets, respectively.
However, evaluation with decision analytical modeling is a simplification of the complex reality. A typical approach is analysis using trial-based efficacy outcomes alone and a demonstration that the intervention may work in optimal and controlled settings. A more difficult and realistic modeling framework was carried out here. As examples, real-world, evidence-based health-related quality of life and persistence, and conservative sensitivity and specificity thresholds for PEUS were used.
Further conservative assumptions were made. For example, DXA measurement was assumed to be 100% accurate, which may not be true due to various human errors, calibration issues or hardware faults. Alendronate FPT was assumed to result in disutility. Sensitivity and specificity of PEUS were accounted for. A partial consequence of this was that especially POMA led to marginally fewer QALYs in comparison with COM. However, the average difference was only 0.001 QALYs (0.03%), which is a negligible difference.
In a larger scope, the PEUSCitation25–Citation29 just recently received a new reimbursement code (0508T: pulse-echo ultrasound bone density measurement resulting in indicator of axial bone mineral density, tibia) from the American Medical Association.Citation72 Considering the previously published evidence on the PEUS method,Citation25,Citation26,Citation29 the American Medical Association reimbursement,Citation72 and the cost-effectiveness results reported here, the use of PEUS as a part of the POM pathway for screening and diagnostics in 65- to 80-year-old postmenopausal Caucasian women is supported.
In addition, access to DXA can be more expensive than assumed here, or even impossible in remote areas. Using an affordable cost of DXA based on the current DXA tests and potentially underestimated traveling costs, PEUS can easily be cost-effective at a cost-per-single-site test of up to around €110 (i.e., 2.2 times the probably overestimated cost used in the base case) in all modeled cohorts. If the costs associated with DXA were higher (e.g., if there is a long distance to the nearest DXA device), an even higher price per PEUS test could be economically justifiable. The Finnish results of POMs with PEUS may underestimate the savings in other countries, but studies in other settings regarding the traveling cost and the optimal location of DXA are needed to confirm such a conclusion.
Finally, more flexible and agile, economically justifiable methods for screening, detecting, and predicting the course of any important or frequent disease or situation are supported governmentally by the encompassing digitalization of social and health care services as well as by the secondary use of health and social welfare data in Finland. More specifically, the assessment and implementation of digitalized customer-responsive health and social care services including, for example, Omahoito ja Digitaaliset Arvopalvelut (ODA) -digitalized services for primary health and social care,Citation73,Citation74 together with the associated Health Village are under their way. Moreover, the secondary use data lakes covering social and health data have been tested through so-called Isaacus pre-production projects,Citation75,Citation76 and the remote use platforms for the data lakes together with scientist tools are being built to enable knowledge management and research.Citation75 Tools with novel data collecting software such as PEUSCitation25–Citation29 are likely to fit well to this ongoing development.
Conclusion
A significant unmet need for new, safe, and effective osteoporosis diagnosis exists. This cost–utility analysis indicated that FPT should be initiated for osteoporotic patients and used persistently, and that PEUS is a cost-saving method with acceptable results in the osteoporosis testing–diagnosing process or the testing process alone, as POMs can result in cost savings with very similar health outcomes in comparison with COM. POM probably also provides a cost-effective alternative for osteoporosis management in other countries utilizing DXA measurements, but further studies in other settings are needed to confirm this conclusion.
Author contributions
Management (ES, OR), conceptualization (ES, OR, JPK, HK), design (all), data acquisition (ES, OR, JPK, PM), data analysis (ES) and interpretation (all), health economic modeling (ES), initial drafting (ES), and critical revision (all). All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
The study was financially supported by Bone Index Finland Ltd, Kuopio, Finland. ESiOR Oy (Kuopio, Finland) carries out studies, statistical analysis, consultancy, education, reporting, and health economic evaluations for several pharmaceutical, food industry, diagnostics and device companies, hospitals, consultancies, and academic institutions, including the producers and marketers of FPTs. ESiOR received financial support for the study from Bone Index Finland Ltd. The financial supporter (Bone Index Finland Ltd, Kuopio, Finland) participated in the identification, design, conduct, and reporting of the analysis.
Disclosure
ES, PM, or TH did not receive any direct financial support as individuals. HK works as an invited member of the national Käypä Hoito care guidance working group for osteoporosis. HK has received consultancy fees and lecture payments from Amgen Ltd and Eli Lilly ltd, and is a partner of Bone Index. ES, PM, and TH are employees of ESiOR Oy, Kuopio, Finland. ES and TH are also partners and directors of ESiOR. OR and JPK are employees and partners of Bone Index. Bone Index is the manufacturer and marketer of PEUS (Bindex®). The authors report no other conflicts of interest in this work.
References
- NelsonHDHelfandMWoolfSHAllanJDScreening for postmenopausal osteoporosis: a review of the evidence for the U.S. Preventive Services Task ForceAnn Intern Med200213752954112230356
- NelsonHDHaneyEMChouRScreening for Osteoporosis: Systematic Review to Update the 2002 U.S. Preventive Services Task Force Recommendation [Internet]Rockville (MD)Agency for Healthcare Research and Quality (US)20107 Report No. 10-05145-EF-1
- AlhavaEEpidemiology of osteoporosis in FinlandDuodecim20041202149215015560447
- NHS ChoicesOsteoporosis. NHS; [updated June 20, 2016; cited January 19, 2018] Available from: http://www.nhs.uk/Conditions/Osteoporosis/Pages/Introduction.aspxAccessed January 19, 2018
- Osteoporoosi (online) [Osteoporosis]Suomalaisen Lääkäriseuran Duodecimin, Suomen Endokrinologiyhdistyksen ja Suomen Gynekologiyhdistyksen asettama työryhmä [Working Group by Finnish Medical Society Duodecim, Finnish Society for Endocrinology and Finnish Society for Gynaegology] [updated February 14, 2018; cited February 15, 2018]HelsinkiSuomalainen Lääkäriseura Duodecim Available from: http://www.kaypahoito.fiAccessed February 15, 2018
- SundRHonkanenRJohanssonHEvaluation of the FRAX model for hip fracture predictions in the population-based Kuopio Osteoporosis Risk Factor and Prevention Study (OSTPRE)Calcif Tissue Int201495394524792689
- World Health OrganizationAssessment of fracture risk and its application to screening for postmenopausal osteoporosisTechnical report series 843GenevaWHO1994
- Suomen virallinen tilasto (SVT) [webpage on the Internet]Väestörakenne [verkkojulkaisu] [Population Structure]; [updated September 22, 2017; cited January 19, 2018]HelsinkiTilastokeskus Available from: http://www.stat.fi/til/vaerak/index.htmlAccessed January 19, 2018
- KannusPNiemiSParkkariJSievänenHDeclining incidence of fall-induced ankle fractures in elderly adults: finnish statistics between 1970 and 2014Arch Orthop Trauma Surg20161361243124627443166
- KannusPNiemiSSievänenHParkkariJContinuous decline in incidence of distal humeral fracture of older women in FinlandAging Clin Exp Res20172946747127251667
- KannusPParkkariJNiemiSSievänenHLow-trauma knee fractures in older Finnish women between 1970 and 2013Aging Clin Exp Res20162866566826403684
- KorhonenNNiemiSParkkariJSievänenHPalvanenMKannusPContinuous decline in incidence of hip fracture: nationwide statistics from Finland between 1970 and 2010Osteoporos Int201324159960323108781
- KannusPParkkariJNiemiSSievänenHLow-trauma pelvic fractures in elderly finns in 1970–2013Calcif Tissue Int20159757758026319676
- KorhonenNKannusPNiemiSParkkariJSievänenHRapid increase in fall-induced cervical spine injuries among older Finnish adults between 1970 and 2011Age Ageing20144356757124865165
- KannusPNiemiSPalvanenMSievänenHParkkariJJärvinenMRising incidence of low-trauma fractures of the calcaneus and foot among Finnish older adultsJ Gerontol A Biol Sci Med Sci20086364264518559641
- EnsrudKEPalermoLBlackDMHip and calcaneal bone loss increase with advancing age: longitudinal results from the study of osteoporotic fracturesJ Bone Miner Res199510177817878592956
- JonesGNguyenTSambrookPKellyPJEismanJAProgressive loss of bone in the femoral neck in elderly people: longitudinal findings from the Dubbo osteoporosis epidemiology studyBrit Med J19943096916957950520
- RiggsBLMeltonLJIIIInvolutional osteoporosisN Engl J Med1986314167616863520321
- KelastoLääkekorvausten saajat ja reseptitiedot 2016 [Reimbursement Receivers and Prescriptions 2015]HelsinkiKansaneläkelaitos2018
- CompstonJCooperACooperCNational Osteoporosis Guideline Group (NOGG)UK clinical guideline for the prevention and treatment of osteoporosisArch Osteoporos2017124328425085
- NOGG2017Clinical guideline for the prevention and treatment of osteoporosis [updated 2017 March; cited January 19, 2018]. Available from: https://www.shef.ac.uk/NOGG/NOGG%20Guideline%202017.pdfAccessed January 19, 2018
- KrögerHFRAX fracture risk calculator in the diagnostics and treatment of osteoporosisDuodecim20131291149115223819200
- FRAXFracture Risk Assessment ToolFinland [updated na; cited January 19, 2018]. Available from: http://www.shef.ac.uk/FRAX/tool.aspxAccessed January 19, 2018
- NguyenTVCenterJREismanJAOsteoporosis: underrated, underdiagnosed and undertreatedMed J Aust2004180S18S2214984358
- SchousboeJTRiekkinenOKarjalainenJPrediction of hip osteoporosis by DXA using a novel pulse-echo ultrasound deviceOsteoporos Int201728859327492435
- KarjalainenJPRiekkinenOTöyräsJJurvelinJSKrögerHNew method for point-of-care osteoporosis screening and diagnosticsOsteoporos Int20162797197726556741
- BehrensMFelserSMau-MoellerAThe Bindex® ultrasound device: reliability of cortical bone thickness measures and their relationship to regional bone mineral densityPhysiol Meas2016371528154027511629
- KarjalainenJPRiekkinenOTöyräsJMulti-site bone ultrasound measurements in elderly women with and without previous hip fracturesOsteoporos Int2012231287129521656263
- KarjalainenJPRiekkinenOKrögerHPulse-echo ultrasound method for detection of post-menopausal women with osteoporotic BMDOsteoporos Int Epub2018219
- BlainHMasudTDargent-MolinaPEUGMS Falls and Fracture Interest Group; International Association of Gerontology and Geriatrics for the European Region (IAGG-ER); European Union of Medical Specialists (EUMS); Fragility Fracture Network (FFN); European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO), and; International Osteoporosis Foundation (IOF)A comprehensive fracture prevention strategy in older adults: the European Union Geriatric Medicine Society (EUGMS) statementAging Clin Exp Res20162879780327299902
- SoiniEJoutsenoJSumelahtiMLCost-utility of first-line disease-modifying treatments for relapsing-remitting multiple sclerosisClin Ther20173953755728209373
- SoiniEBiologisten lääkkeiden kustannusvaikuttavuus nivelpsoriaasin hoidossa [Cost-Effectiveness of Biologic Treatments in Joint Psoriasis]. Käypä hoito [Current Care Criteria]: Lisätietoa [Additional information] [updated March 1, 2017; cited January 19, 2018]. Available from: http://www.kaypahoito.fi/web/kh/suositukset/suositus?id=nix02465&suositusid=hoi50062Accessed January 19, 2018
- Fimean suositus lääkkeiden hoidollisen ja taloudellisen arvon arvioin-nista [Fimea recommendation for the assessment of the therapeutic and economic value of pharmaceuticals]KuopioFimea kehittää, arvioi ja informoi -julkaisusarja [Serial Publication Fimea Develops, Assesses and Informs]22012
- Terveystalousselvityksen selvityksen laatiminen lääkevalmisteen korvattavuus- ja tukkuhintahakemukseen [Composing health economic evaluation for the pricing and reimbursement application]3112017HelsinkiLääkkeiden hintalautakunta2017
- BriggsAClaxtonCSculpherMDecision Modelling for Health Economic EvaluationOxfordOxford University Press2008
- SoiniEHallinenTBrignoneMCost-utility analysis of vortioxetine versus agomelatine, bupropion SR, sertraline and venlafaxine XR after treatment switch in major depressive disorder in FinlandExpert Rev Pharmacoecon Outcomes Res20171729330227680105
- HansDBShepherdJASchwartzENPeripheral dual-energy X-ray absorptiometry in the management of osteoporosis: the 2007 ISCD Official PositionsJ Clin Densitom20081118820618442759
- KriegMABarkmannRGonnelliSQuantitative ultrasound in the management of osteoporosis: the 2007 ISCD Official PositionsJ Clin Densitom20081116318718442758
- HiligsmannMEversSMBen SedrineWA systematic review of cost-effectiveness analyses of drugs for postmenopausal osteoporosisPharmacoeconomics20153320522425377850
- Lääkehaku [Drug search]HelsinkiKansaneläkelaitos2018
- FleurenceRLHollenbeakCSRates and probabilities in economic modelling: transformation, translation and appropriate applicationPharmacoEconomics2007253617192114
- HiligsmannMMcGowanBBennettKBarryMReginsterJYThe clinical and economic burden of poor adherence and persistence with osteoporosis medications in IrelandValue Health20121560461222867768
- NayakSRobertsMSGreenspanSLCost-effectiveness of different screening strategies for osteoporosis in postmenopausal womenAnn Intern Med201115575176122147714
- SundRJuntunenMLüthjePPERFECT − Lonkkamurtuma [PERFECT – Hip fracture]HelsinkiSTAKESin työpapereita [STAKES working papers]200818131
- StevensonMJonesMLDe NigrisEA systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosisHealth Technol Assess200591160
- HiligsmannMEthgenOBruyèreODevelopment and validation of a Markov microsimulation model for the economic evaluation of treatments in osteoporosisValue Health20091268769619508659
- RabendaVMertensRFabriVRichyFGathonHJReginsterJYAdherence to bisphosphonates therapy and hip fracture risk in osteoporotic womenOsteroporos Int200819811818
- Suomen virallinen tilasto (SVT) [webpage on the Internet]Kuolleet [Mortality] [updated April 28, 2017; cited January 19, 2018]HelsinkiTilastokeskus Available from: http://www.stat.fi/til/kuol/index.htmlAccessed January 19, 2018
- Suomen virallinen tilasto (SVT) [webpage on the Internet]Kuolemansyyt [Causes of death] [updated December 29, 2017; cited January 19, 2018;]HelsinkiTilastokeskus Available from: http://www.stat.fi/til/ksyyt/index.htmlAccessed January 19, 2018
- HaentjensPMagazinerJColón-EmericCSMeta-analysis: excess mortality after hip fracture among older women and menAnn Intern Med201015238039020231569
- SaarniSIHärkänenTSintonenHThe impact of 29 chronic conditions on health-related quality of life: a general population survey in Finland using 15D and EQ-5DQual Life Res2006151403141416960751
- HiligsmannMEthgrenORichyFReginsterJYUtility values associated with osteoporotic fracture: a systematic review of the literatureCalcif Tissue Int20088228829218404243
- Baltic guideline for economic evaluation of pharmaceuticals (pharmacoeconomic analysis) [updated August 8, 2002; cited January 19, 2018;]. Available from: https://www.ispor.org/PEguidelines/source/Baltic-PE-guideline.pdfAccessed January 19, 2018
- Belgian Health Care Knowledge CentreBelgian Guidelines for Economic Evaluations and Budget Impact Analyses2nd edBrusselsBelgian Health Care Knowledge Centre (KCE)2012
- Collège des Économistes de la SantéFrench Guidelines for the Economic Evaluation of Health Care TechnologiesParisCollège des Économistes de la Santé2004190
- College voor zorgverzekeringen Guidelines for pharmacoeconomic research, updated versionDiemenCollege voor zorgverzekeringen2006114
- Health Information and Quality AuthorityGuidelines for the Economic Evaluation of Health Technologies in IrelandCorkHealth Information and Quality Authority2010175
- Institut für Pharmaökonomische ForschungGuidelines on health economic evaluation Vienna: Institut für Pharmaökonomische Forschung2006111
- López-BastidaJOlivaJAntoñanzasFSpanish recommendations on economic evaluation of health technologiesEur J Health Econ20101151352020405159
- National Institute for Health and Care ExcellenceGuide to the Methods of Technology Appraisal 2013LondonNational Institute for Health and Care Excellence2013
- Norwegian Medicines AgencyGuidelines on How to Conduct Pharmacoeconomic AnalysesNorwegian Medicines Agency2012127
- Scottish Medicines ConsortiumGuidance to Manufacturers for Completion of New Product Assessment FormScottish Medicines Consortium2007
- KapiainenSVäisänenAHaulaTTerveyden- ja sosiaalihuollon yksik-kökustannukset Suomessa vuonna 2011 [Health and Social Care Costs in Year 2011 in Finland]HelsinkiTerveyden ja hyvinvoinnin laitos2014
- Suomen virallinen tilasto (SVT) [webpage on the Internet]Julkisten menojen hintaindeksi [Public Expenditure Cost Index] [updated October 27, 2017; cited January 19, 2018]HelsinkiTilastokeskus Available from: http://www.stat.fi/til/jmhi/index.htmlAccessed January 19, 2018
- HujanenTKapiainenSTuominenUPekurinenMTerveydenhuollon yksikkökustannukset Suomessa vuonna 2006 [Health Care Unit Costs in Year 2006 in Finland]HelsinkiStakesin Työpapereita2008
- Suomen virallinen tilasto (SVT) [webpage on the Internet]Kuluttaja-hintaindeksi [Consumer Price Index] [updated January 15, 2018; cited January 19, 2018]HelsinkiTilastokeskus Available from: http://www.stat.fi/til/khi/index.htmlAccessed January 19, 2018
- SoiniEJHallinenTSokkaALSaarinenKCost-utility of first-line actinic keratosis treatments in FinlandAdv Ther20153245547626006101
- SoiniEKukkonenJMyllykangasMRyynänenOPContingent valuation of eight new treatments: What is the clinician’s and politician’s willingness to pay?Open Complement Med J20124111
- SoiniEKroonisen lymfaattisen leukemian hoidon kustannusvaikuttavuus Suomessa ja sen uudet tulkinnat: Kliininen kustannushyöty ja vaikuttavuusinvestoiminen [Cost Effectiveness of Chronic Lymphatic Leukaemia and Its New Interpretations: Clinical Cost Benefit and Impact Investment]BestPractice Onkologia / Hematologia201653032
- Bank of FinlandAverage Annual Exchange Courses in Year 2016HelsinkiBank of Finland2017
- BartonGRBriggsAHFenwickEAOptimal cost-effectiveness decisions: the role of the cost-effectiveness acceptability curve (CEAC), the cost-effectiveness acceptability frontier (CEAF), and the expected value of perfection information (EVPI)Value Health20081188689718489513
- American Medical AssociationCPT® Category III Codes [updated December 21, 2017; cited January 19, 2018]. Available from: https://www.ama-assn.org/sites/default/files/media-browser/public/cpt/cpt-category3-codes-descriptors.pdfAccessed January 19, 2018
- Prime Minister’s OfficeFinland, A Land of Solutions. Mid-Term Review. Government Action Plan 2017–2019FinlandGovernment Publications72017
- VäätäinenSSoiniEArvonenSVirtual hospital 2.0 – modelled cost-benefit assessment: towards potential economic efficiency with digitalization and customer-responsive serviceseHealth 2018, The 23rd Finnish National Conference on Telemedecine and eHealth, The 23rd ISfTeH International Conference37March 15, 2018Helsinki/Stockholm/HelsinkiFinnish Society of Telemedicine and eHealth
- SoiniEHallinenTKekoniAEfficient secondary use of representative social and health care data in Finland: Isaacus data lake, analytics and knowledge management pre-production projectValue Health201720A777
- HallinenTSoiniEKekoniAIsaacus pre-production project: child protection process and placement decisioneHealth 2018, The 23rd Finnish National Conference on Telemedecine and eHealth, The 23rd ISfTeH International Conference64March 15, 2018Helsinki/Stockholm/HelsinkiFinnish Society of Telemedicine and eHealth