Abstract
Background
An economic evaluation was undertaken in order to assess several therapeutic alternatives (rosuvastatin, atorvastatin, simvastatin, and pravastatin) for the prevention of primary and secondary cardiovascular events in high-risk patients in Greece.
Methods
A probabilistic Markov model with five distinct states provided estimates over a 20-year time span. The relative effectiveness of comparators was based on the literature. The HellenicSCORE risk equation was used to forecast survival. The transition probabilities from acute myocardial infarction or stroke to death were estimated with reference to the Framingham study. In addition, Framingham scores were used to calculate the probability of nonfatal acute myocardial infarction or nonfatal stroke. Costs were estimated from the perspective of sickness funds and included direct medical costs valued in the year 2012. The total treatment cost accounted for the cost of drugs, routine examinations, and resources expended in the management of acute myocardial infarction, stroke, and death. The utility decrements used are those for the Greek population. A supplementary budget impact analysis was also conducted.
Results
The mean discounted quality-adjusted life years in the case of males for the rosuvastatin arm were 10.18 versus 10.04, 9.94, and 9.88 for atorvastatin, simvastatin, and pravastatin, respectively. The mean total cost was €15,392, €16,438, €17,009, and €17,356 for rosuvastatin, atorvastatin, simvastatin, and pravastatin, respectively. Similar results were obtained in the case of females, while all analyses demonstrated a statistically significant difference at the 95% level of significance. The total burden of 100% (single) use of rosuvastatin in a hypothetical cohort of 100 male patients for one year was €1.47 million versus €1.53 million for atorvastatin, €1.57 million for simvastatin, and €1.59 million for pravastatin.
Conclusion
Rosuvastatin may represent an attractive choice compared with likely alternative existing therapies used in the primary and secondary prevention of cardiovascular events by the National Health Service of Greece.
Introduction
According to the World Health Organization, cardiovascular disease (CVD) is the leading cause of morbidity and mortality worldwide.Citation1 The major risk factors associated with CVD, such as tobacco use, alcohol use, hypertension, hypercholesterolemia, obesity, physical inactivity, and unhealthy diet, have a high prevalence across the world.Citation2 In Greece, the prevalence of cardiovascular risk factors is very high, and thus CVD accounts for 45.8% of all deaths in men and women.Citation3–Citation13 Given that the life expectancy of the general population in Greece is 78 years and 83 years of age for males and females, respectively,Citation3 CVD accounts for a considerable amount of life lost due to premature deaths in the country.
Apart from being a major cause of mortality and morbidity, CVD has an economic impact expressed in terms of direct health care costs, informal care costs, and loss of productivity. The total direct and indirect cost of CVD and stroke in the United States for 2010 was estimated at $503.2 billion.Citation14 In Europe, CVD is estimated to cost €169 billion annually, with health care accounting for 62% of all costs.Citation15 In this context, it has been noted that CVD is becoming a negative factor for economic growth in developing countries.Citation16 According to the Agency for Healthcare Research and Quality’s guidelines, many forms of heart disease are largely preventable.Citation17 Controlling conditions such as hypertension, diabetes, and hypercholesterolemia can reduce the risk of heart disease. Statins represent the main class of drugs used in standard practice for reducing serum cholesterol and for preventing ischemic coronary disease.Citation18 Atorvastatin, simvastatin, pravastatin, and rosuvastatin are among the most widely used statins. In particular, rosuvastatin has been shown to be effective in cholesterol reduction and in achieving targets for low-density lipoprotein cholesterol (LDL-C) levels.Citation19–Citation22
Health care resources are scarce in contrast with the increasing needs. Also, given the size of the population using statins, the related expenditure is significant, especially in light of the present fiscal status in most countries. Thus, an economic evaluation was undertaken in order to assess the cost-effectiveness of the therapeutic alternatives (rosuvastatin, atorvastatin, simvastatin, and pravastatin) in the prevention of primary and secondary cardiovascular events in Greece, which is going through a major financial crisis, making this approach to medical decision-making more important than ever before. The present paper presents the results of this economic analysis.
Materials and methods
Study objective
The aim of the present study was to conduct an economic evaluation comparing rosuvastatin atorvastatin, simvastatin, and pravastatin in the primary and secondary prevention of CVD among high-risk patients in Greece. Dosing in each case is different, and to be able to make reliable comparisons, we used effectiveness data corresponding to the 40 mg dose in each case, which has been shown to achieve at least a 30% reduction in LDL-C levels.Citation27 The model assumes at baseline a mean age of 70 years, systolic blood pressure 140 mmHg, total cholesterol 260 mg/dL, high-density lipoprotein cholesterol (HDL-C) 60 mg/dL, and computes results for nonsmoking males and females.
Perspective of analysis
The perspective of the economic evaluation was that of sickness funds (payers) in Greece. Therefore, only direct health care costs reimbursed by payers were considered. Direct costs are those associated directly with the medical care of patients. Other costs that quantify the remaining nonmedical impact of disease (eg, productivity loss, travelling costs) were not considered in the present analysis.
Economic model
A Markov model was developed based on international experience in this field to assess the clinical and economic implications of using different alternatives for the primary and secondary prevention of events among high-risk patients in Greece ().Citation18 In the model, a population in each arm is simulated during a long period of time. The model comprises different health states in which patients can move over time, and each are associated with different costs and quality of life.
Figure 1 Structure of the model.
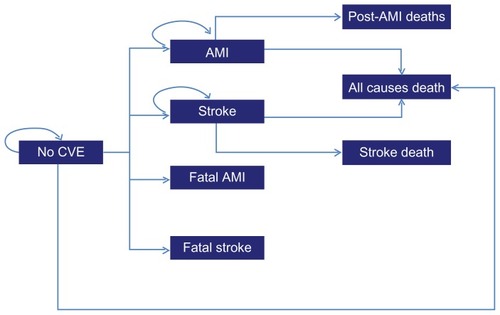
The likelihood of moving between different states is influenced by the effectiveness of each therapy, and hence the cost and quality-adjusted years of life. As illustrated in , patients can transition in year-long model cycles from the initial state of no cardiovascular event to five distinct states, including nonfatal acute myocardial infarction, nonfatal stroke, fatal acute myocardial infarction, fatal stroke, and other-cause death, representing a state in which patients die of causes other than a cardiovascular event. Moreover, patients may die in a subsequent cycle after a nonfatal acute myocardial infarction or stroke due to the fact that their mortality rates are higher.
The SCORE risk equation was calibrated recently in order to calculate the combined 10-year risk reflecting the probability of a patient dying due to acute myocardial infarction or stroke.Citation23 To reflect the local situation, the HellenicSCORE calibration was used in the present analysis.Citation24 The yearly-converted probabilities were adjusted to include the risk of all-cause mortality for Greek patients according to data from the National Statistical Service of Greece.Citation3 Transition probabilities from acute myocardial infarction or stroke to death were estimated based on the Framingham study.Citation25 In addition, Framingham scores were used to calculate the probability that a patient experiences a nonfatal acute myocardial infarction or nonfatal stroke. Thus, all event rates are dependent on patient age, gender, and risk status. The model estimates treatment cost and quality-adjusted life years for alternative treatment options in an identical cohort of 1000 patients in each arm. Annual discount rates of 3.5% were applied for all outcomes, which is common practice in similar studies.Citation26
Efficacy data
Treatment effectiveness was evaluated in the present model on the basis of LDL-C reduction with each of the aforementioned comparators. Data from a meta-analysis were used to assess the LDL-C reduction achieved with different statins.Citation27 Estimates based on 164 placebo-controlled trials indicate that the mean absolute reduction in LDL-C was superior in the case of rosuvastatin (53% for 40 mg, ). It should be noted that although LDL-C remains the primary target of therapy, the risk factors included in the Framingham algorithm are based on total cholesterol rather than LDL-C. However, reductions in total and LDL cholesterol concentrations were highly correlated across trials (r = 0.83), and a bivariate normal distribution was assumed (based on the central limit theorem) in order to convert the mean reduction of LDL-C to a reduction in total cholesterol in a probabilistic manner.Citation27 Moreover, for practical simplicity, HDL-C was considered to be the same before and after treatment, despite the fact that rosuvastatin has been shown to be more efficient in the management of HDL-C levels.Citation28
Table 1 Absolute reduction (mmol/L) and percentage reduction in serum LDL-C concentration according to statin treatmentTable Footnote*
Utilities
Due to lack of appropriate data for the Greek population, utility weights for the nonevent state were set at 1 for all patients. Data regarding utility weights came from a local study which used the EQ-5D and have been presented elsewhere.Citation12 When patients experienced a nonfatal event, such as stroke or acute myocardial infarction, utility decrements for the whole duration of one year (equal to the length of the Markov cycle) were applied. For the second and subsequent years, different utility weights were used ().
Table 2 Utility weights used in the modelCitation12
Costing methodology
Costs were estimated from the perspective of sickness funds, and included direct medical costs valued in the year 2012. The total cost related to each treatment includes the cost of drugs, the cost of acute myocardial infarction and stroke, routine examinations and visits to practitioners, as well as the cost of the resources consumed for those dying (). The total cost of comparators was calculated by multiplying the number of units of drugs required for 40 mg therapy by the unit price. The cost per pill for comparators was calculated using prices from the price bulletin of January 2012.Citation29 In the case of atorvastatin, the price of its generic was used because this is the prevalent medication. By definition, there was no variation in unit costs, given that unit prices were obtained from the official government gazette and are common to all public hospitals in Greece. The cost of each comparator medication was calculated based on the assumption that patients take one tablet/capsule per day every day throughout the year until they die. Data on resource use for stroke and acute myocardial infarction and reimbursement rates were collected from recently published tariffs. Examinations and procedures performed on an outpatient basis were valued separately. The cost of any outpatient regime was calculated according to the resource utilization proposed by experts. The cost of death was derived from the Greek bibliography, and a 3.5% rate was used in order to express the findings of this study in present values.
Table 3 Cost inputs used in the model
Analyses
The model was set to provide deterministic and probabilistic analyses. The results are used to compute incremental cost-effectiveness ratios and cost-effectiveness acceptability curves. In this light, probability distributions were specified around all of its parameters () and these were used to run simulations in order to derive expected values and intervals. This is important also because cost data are truncated and do not follow normal distributions.Citation30 Given that data are generally not normally distributed, but skewed to the right, bias-corrected uncertainty intervals (UI) were calculated using the percentile method of nonparametric simulation (using 5000 replications). It is important to indicate that given the probabilistic nature of the components (as random variables), cost and survival of comparators could be slightly different and not “fixed” results produced in each experiment.
Table 4 Distributions used in the model for probabilistic analysis
Budget impact analysis
Apart from the cost-effectiveness analysis which compares alternative therapeutic agents in regards to their costs and outcomes, a supplementary budget impact analysis was undertaken to forecast the future economic impact of substitution of rosuvastatin for other comparators. A straightforward way is to assess the economic impact of statin use within a lifetime horizon. Hence the results presented refer to a hypothetical cohort of 100 patients treated exclusively with each therapy in order to make easy extrapolations.
Results
The results indicate that, in the case of males, rosuvastatin was associated with fewer major cardiovascular events (stroke or acute myocardial infarction) per patient. During the duration of analysis, the mean number of events in the rosuvastatin arm was 0.92 per patient relative to 1.46, 1.76, and 1.93 for atorvastatin, simvastatin, and pravastatin, respectively. Similarly, for women, the mean number of major events was 0.61 per patient against 0.92, 1.1, and 1.2 for atorvastatin, simvastatin, and pravastatin, respectively. There were no differences amongst comparators for fatal events in either men or women. The main results are shown in detail in .
Table 5 Markov model results in the baseline population
The mean estimate for discounted quality-adjusted life years in the rosuvastatin arm was 10.18 (95% UI, 10.11–10.23) versus 10.04 (95% UI, 9.96–10.10), 9.94 (95% UI, 9.84–10.02), and 9.88 (95% UI, 9.77–9.96) for atorvastatin, simvastatin, and pravastatin, respectively. The difference in quality-adjusted life years relative to rosuvastatin was 0.14 (95% UI, 0.11–0.17, P < 0.001) for atorvastatin, 0.24 (95% UI, 0.20–0.28, P < 0.001) for simvastatin, and 0.30 (95% UI, 0.25–0.35, P < 0.001) for pravastatin.
The mean total cost of rosuvastatin was €11,356 (95% UI, 11,078–11,656); the cost of atorvastatin was €12,453 (95% UI, 12,140–12,787); the cost of simvastatin was €13,059 (95% UI, 12,718–13,423); and the cost of pravastatin was €13,428 (95% UI, 13,068–13,814). Thus, rosuvastatin was cost-saving relative to other therapies, with a mean difference of –€1096 (95% UI, −1211, −984, P < 0.001) relative to atorvastatin −€1703 (95% UI, −1811, −1591, P < 0.001) versus simvastatin, and −€2072 (95% UI, −2181, −1964, P < 0.001) versus pravastatin. These data show that rosuvastatin represents a dominant choice against the other comparators in the case of male patients.
Moreover, in the case of rosuvastatin, the cost of drugs accounted for 53.8% of the total cost, followed by the cost of examinations (14.3%), cost of death (13.3%), cost of stroke (11.1%), and cost of acute myocardial infarction (7.5%). In the atorvastatin arm, the cost of drugs accounted for 46.6% of the total cost, followed by the cost of acute myocardial infarction at 17.1%, the cost of death at 13.7%, and the cost of examinations and stroke at 12.5% and 10.2%, respectively. In the case of simvastatin, the cost of drugs accounted for 45.1% of the total cost, the cost of acute myocardial infarction was 21.6%, followed by the rest of the cost components with smaller percentages. Relatively similar results were obtained in the case of pravastatin.
From the point of view of budget impact, the total burden of 100% (single) use of rosuvastatin in a hypothetical cohort of 100 patients for one year was €1.14 million versus €1.25 million for atorvastatin, €1.30 million for simvastatin, and €1.34 million for pravastatin. Thus, the net saving from the use of rosuvastatin was €109,641 versus atorvastatin, €170,310 versus simvastatin, and €207,190 versus pravastatin.
In the case of females, the mean discounted quality-adjusted life years in the rosuvastatin arm were 10.33 (95% UI, 10.28–10.37) versus 10.26 (95% UI, 10.20–10.30) 10.20 (95% UI, 10.12–10.25), and 10.16 (95% UI, 10.08–10.22) for atorvastatin, simvastatin, and pravastatin, respectively. The difference in quality-adjusted life years for rosuvastatin was 0.08 (95% UI, 0.06–0.09, P < 0.001) versus atorvastatin, 0.13 (95% UI, 0.11–0.16, P < 0.001) versus simvastatin, and 0.17 (95% UI, 0.14–0.20, P < 0.001) versus pravastatin.
The mean total cost in the case of rosuvastatin was €10,678 (95% UI, 10,482–10,885); the cost of atorvastatin was €11,288 (95% UI, 11,071–11,517); the cost of simvastatin was €11,656 (95% UI, 11,415–11,911); and the cost of pravastatin was €11,873 (95% UI, 11,618–12,148). The mean difference in the cost of rosuvastatin was −€610 (95% UI, −1175, −918, P < 0.001) versus atorvastatin −€978 (95% UI, −1044, −913, P < 0.001) versus simvastatin, and −€1195 (95% UI, −1262, −1130, P < 0.001) versus pravastatin. These data indicate that rosuvastatin represents a dominant choice against the other comparators in the case of female patients.
In the case of rosuvastatin, the cost of drugs accounted for 59.2% of the total cost, followed by the cost of examinations at 15.8% and the cost of death at 11.9%. In the atorvastatin arm, the cost of drugs accounted for 54.5% of total cost followed by the cost of examinations (14.5%), the cost of death (12.2%), the cost of acute myocardial infarction (10.2%), and finally the cost of stroke at 8.6%. Similar results were obtained in the case of simvastatin and pravastatin where the cost of drugs accounted for approximately 50% of the total cost of treatment.
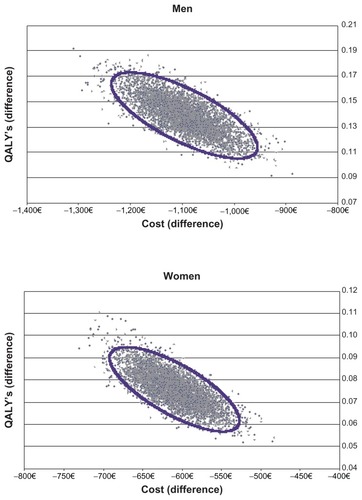
The total burden of 100% (single) use of rosuvastatin in a hypothetical cohort of 100 patients was €1.07 million versus €1.13 million for atorvastatin, €1.17 million for simvastatin, and €1.19 million for pravastatin. Thus, the net saving with rosuvastatin was €61,011 versus atorvastatin, €97,802 versus simvastatin, and €119,511 versus pravastatin. These are significant when the total numbers of patients are taken into consideration. Finally, presents a probabilistic analysis against generic atorvastatin which is the least costly option, and it is clear that rosuvastatin maintains its dominance in most cases.
Figure 2 Scatter plots of rosuvastatin against atorvastatin for both genders.
Discussion
Understanding the relative benefits and costs of alternative treatment strategies for the primary and secondary prevention of cardiovascular events in high-risk patients is important in order to ensure that patients receive an acceptable level of care while effectively managing health care resources. Since the benefits of statins have been widely acknowledged by general practitioners, their use has become a part of standard clinical practice.
Nonetheless, it is paramount to consider the cost relative to the clinical benefits associated with alternative therapy options for high-risk patients in Greece. In the present study, a comparison of rosuvastatin and its main comparators (atorvastatin, simvastatin, pravastatin) was undertaken using a Markov probabilistic model. The statins selected cover almost the entire market in Greece, and the comparison took place assuming an average dose of 40 mg per day for each comparator for reliability purposes.
The analysis here showed that rosuvastatin is an attractive choice against the other aforementioned statins because it is associated with lower cost and slightly greater effectiveness. Furthermore, rosuvastatin represents a potentially cost-saving option from a budget impact point of view in the Greek National Health Service setting. Probabilistic analysis showed that the results hold true in favor of rosuvastatin for both genders at a 95% level of significance. A scatter plot () in the case of rosuvastatin against atorvastatin, as the most prominent comparator, shows that the entire sample of 5000 replications falls into the southwest quadrant, which indicates that rosuvastatin is a slightly less costly and more effective choice. Similar results were obtained in the case of other comparisons.
The results of the current study are in agreement with those reported in the literature.Citation18,Citation31–Citation36 In all the referenced cases, rosuvastatin was a dominant or cost-effective choice under different assumptions regarding doses, the perspective of analysis, and the characteristics of the population involved. From a clinical perspective, that is due to the fact that rosuvastatin represents an advanced therapy from a pharmacological and clinical point of view relative to the other agents in this class, possesses a greater number of binding interactions with 3-hydroxy-3-methylglutaryl coenzyme A reductase, and has the longest terminal half-life among the statins.Citation37 From an economic perspective, because rosuvastatin has a higher capacity to reduce LDL-C in relation to other statins, it minimizes the frequency of costly events, such as stroke and acute myocardial infarction.
Any model is, by necessity, a simplification of the process it tries to simulate, so it was necessary to make assumptions when constructing the model. Cardiovascular disease is quite a complex situation and the probability of experiencing or avoiding an event is subject to variability. CVD risk is affected by several risk factors, including comorbidities, demographic characteristics, dietary habits, treatment switches amongst statins, and dose titrations. In this light, the analysis was limited to high-risk patients who were nonsmokers with a mean age of 70 years. In addition, quality of life with regard to patient age (in the case of no event) was ignored in the present analysis. Utility decrements for the rest of the states were set equal for all comparators to avoid possible bias. The event rates used take into consideration the risk profile of patients and the model was based on widely accepted data.
The model assumed that a patient would be treated for the whole duration of interest from the start to the end of the model or death. Hence, no switching between treatments was allowed. The reason for this was the lack of appropriate data to populate this type of complex management. Furthermore, the analysis used suffers from drawbacks and limitations that are common in studies using similar methodologies. It does not represent experimental research, but instead is based on a model populated with data reported in the literature and on various assumptions, so may suffer from biases. Standard recommendations were followed to limit possible sources of bias. Thus, a systematic review and assessment of the evidence was performed and stochastic analysis was used to draw robust conclusions. This methodology and the modeling approach represent a reasonable substitute for direct real-life comparisons between these treatments. The model allows a relative risk to be applied to each year of risk of cardiovascular events for men and women separately. The assumptions in the model were extracted from the literature and were designed to be easily tested.
The results have to be considered strictly in the Greek setting and on the basis of resources and drug prices. If any of the underlying parameters change, so may the results and the conclusions of the analysis. Finally, we confined the analysis to sickness funds and not society overall. A broader analysis could be the goal of research in the future.
Conclusion
Rosuvastatin may represent an attractive option compared with the most likely alternative existing therapies used in the primary and secondary prevention of cardiovascular events in the National Health Service of Greece.
Disclosure
This study was funded by Astra Zeneca, Greece.
References
- World Health OrganizationGlobal atlas on cardiovascular disease prevention and control2011 Available from: http://www.who.int/cardiovascular_diseases/en/Accessed April 23, 2012
- MackayJMensahGAtlas of Heart Disease and StrokeGeneva, SwitzerlandWorld Health Organization2004
- Hellenic Statistical AuthorityConcise Statistical Yearbook2009 Available from: http://www.statistics.grAccessed April 23, 2012Greek
- PitsavosCMiliasGAPanagiotakosDBXenakiDPanagopoulosGStefanadisCPrevalence of self-reported hypertension and its relation to dietary habits in adults; a nutrition and health survey in GreeceBMC Public Health2006620616904009
- EfstratopoulosADVoyakiSMBaltasAAPrevalence awareness treatment and control of hypertension in Hellas Greece: the Hypertension Study in General Practice in Hellas (HYPERTENSHELL) national studyAm J Hypertens2006191536016461191
- AthyrosVGGanotakisESBathianakiMAwareness treatment and control of the metabolic syndrome and its components: a multicentre Greek studyHellenic J Cardiol200546638038616422124
- SarafidisPALasaridisAGousopoulosSPrevalence, awareness, treatment and control of hypertension in employees of factories of Northern Greece: the Naoussa studyJ Hum Hypertens200418962362915029221
- PsaltopoulouTOrfanosPNaskaALenasDTrichopoulosDTrichopoulouAPrevalence awareness treatment and control of hypertension in a general population sample of 26913 adults in the Greek EPIC studyInt J Epidemiol20043361345135215218014
- PanagiotakosDBPitsavosCChrysohoouCSkoumasJStefanadisCStatus and management of blood lipids in Greek adults and their relation to socio-demographic lifestyle and dietary factors: the ATTICA Study. Blood lipids distribution in GreeceAtherosclerosis2004173235336115064113
- GikasASotiropoulosAPanagiotakosDPeppasTSklirosEPappasSPrevalence and associated risk factors of self-reported diabetes mellitus in a sample of adult urban population in Greece: MEDICAL Exit Poll Research in Salamis (Medical Express 2002)BMC Public Health20044215028111
- PanagiotakosDBPitsavosCHChrysohoouCStatus and management of hypertension in Greece: role of the adoption of a Mediterranean diet: the ATTICA studyJ Hypertens20032181483148912872041
- ManiadakisNKourlabaGFragoulakisVSelf-reported prevalence of atherothrombosis in a general population sample of adults in Greece; a telephone surveyBMC Cardiovasc Disord2011111621492471
- LakattaEGAge-associated cardiovascular changes in health: impact on cardiovascular disease in older personsHeart Fail Rev200271294911790921
- Lloyd-JonesDAdamsRJBrownTMAmerican Heart AssociationExecutive summary: heart disease and stroke statisticsCirculation2010121794895420177011
- LealJLuengo-FernandezRGrayAPetersenSRaynerMEconomic burden of cardiovascular diseases in the enlarged European UnionEur Heart J200627131610161916495286
- SuhrckeMUrbanDAre cardiovascular diseases bad for economic growth?Health Econ201019121478149619998332
- Guideline Summary [webpage on the Internet]Rockville, MDAgency for Healthcare Reseach and Quality Available from: http://www.guideline.gov/content.aspx?id=33603&search=cardiovascular#Section420Accessed April 23, 2012
- AraujoDVBahiaLSouzaCPRPavãoALBCost-effectiveness and budget impact analysis of rosuvastatin and atorvastatin for LDL-cholesterol and cardiovascular events lowering within the SUS* scenarioInt J Atheroscler200723189194
- AsztalosBFLe MaulfFDallalGEComparison of the effects of high doses of rosuvastatin versus atorvastatin on the subpopulations of high-density lipoproteinsAm J Cardiol200799568168517317371
- BullanoMFKamatSWertzDAEffectiveness of rosuvastatin versus atorvastatin in reducing lipid levels and achieving low-density-lipoprotein cholesterol goals in a usual care settingAm J Health Syst Pharm200764327628417244877
- JonesPHHunninghakeDBFerdinandKCEffects of rosuvastatin versus atorvastatin simvastatin and pravastatin on non-high-density lipoprotein cholesterol apolipoproteins and lipid ratios in patients with hypercholesterolemia: additional results from the STELLAR trialClin Ther20042691388139915531001
- MotskoSPRussmannSMingEESinghVPVendiolaRMJonesJKEffectiveness of rosuvastatin compared to other statins for the prevention of cardiovascular events – a cohort study in 395,039 patients from clinical practicePharmacoepidemiol Drug Saf200918121214122219780020
- ConroyRMPyoralaKFitzgeraldAPEstimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE projectEur Heart J20032411987100312788299
- PanagiotakosDBFitzgeraldAPPitsavosCPipilisAGrahamIStefanadisCStatistical modelling of 10-year fatal cardiovascular disease risk in Greece: the HellenicSCORE (a calibration of the ESC SCORE project)Hellenic J Cardiol2007482556317489342
- Framingham Heart StudyHard coronary heart disease (10-year risk) Available from: http://www.framinghamheartstudy.org/risk/hrdcoronary.htmlAccessed April 23, 2012
- ManiadakisNKaitelidouDSiskouOEconomic evaluation of treatment strategies for patients suffering acute myocardial infarction in GreeceHellenic J Cardiol200546321222115981557
- LawMRWaldNJRudnickaARQuantifying effect of statins on low density lipoprotein cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysisBMJ20033267404142312829554
- JonesPKafonekSLauroraIHunninghakeDComparative dose efficacy study of atorvastatin versus simvastatin pravastatin lovastatin and fluvastatin in patients with hypercholesterolemia (the CURVES study)Am J Cardiol19988155825879514454
- The Ministry for Health and Social SolidarityPrice bulletin Available from: http://www.yyka.gov.gr/articles/times-farmakwn/deltia-timwnMinistry of Health2012Accessed April 23, 2012Greek
- BriggsAProbabilistic analysis of cost-effectiveness models: statistical representation of parameter uncertaintyValue Health2005811215841888
- BennerJSSmithTWKlingmanDCost-effectiveness of rosuvastatin compared with other statins from a managed care perspectiveValue Health20058661862816283862
- PalmerSJBradyAJRatcliffeAEThe cost-effectiveness of a new statin (rosuvastatin) in the UK NHSInt J Clin Pract200357979280014686571
- OhsfeldtRLGandhiSKFoxKMStacyTAMcKenneyJMEffectiveness and cost-effectiveness of rosuvastatin atorvastatin and simvastatin among high-risk patients in usual clinical practiceAm J Manag Care200612Suppl 15S412S42317112329
- PintoCGCarragetaMOMiguelLSCost-effectiveness of rosuvastatin in the prevention of ischemic heart disease in PortugalValue Health200811215415918380628
- Costa-ScharplatzMRamanathanKFrialTBeamerBGandhiSCost-effectiveness analysis of rosuvastatin versus atorvastatin simvastatin and pravastatin from a Canadian health system perspectiveClin Ther20083071345135718691996
- OhsfeldtRLGandhiSKSmolenLJCost effectiveness of rosuvastatin in patients at risk of cardiovascular disease based on findings from the JUPITER trialJ Med Econ201013342843720662625
- RosensonRSRosuvastatin: a new inhibitor of HMG-coA reductase for the treatment of dyslipidemiaExpert Rev Cardiovasc Ther20031449550515030249