
Abstract
Background
Currently approved biologic therapies for moderate-to-severe ulcerative colitis have well-established efficacy. However, many patients fail to respond or lose response, leading to dose escalation or treatment switching.
Objective
We sought to identify real-world evidence on dose escalation and treatment switching and associated clinical and economic outcomes among adults with ulcerative colitis treated with infliximab, adalimumab, golimumab, vedolizumab, ustekinumab, or tofacitinib.
Methods
We conducted a systematic search of Embase, MEDLINE (up to 26 August 2020), and conference proceedings (2017−2020) for studies in adults with ulcerative colitis to assess clinical response and remission, colectomy, adverse events, and economic outcomes related to dose escalation and treatment switching.
Results
In 56 studies, dose escalation and treatment switching involving infliximab and/or adalimumab were most frequently investigated. Rates of clinical response after dose escalation were 20–95% (1.8–36 months), clinical remission rates were 10–94% (1.8–36 months), colectomy rates were 0–33% (12–38 months), and adverse event rates were 0–18%. Treatment switching rates in 21 studies were 4–70% over 3–62 months, with switch due to loss of response rates of 4–35% over 12–62 months (7 studies). Up to 35% of patients underwent colectomy 12−120 weeks after switching, and 13–38% experienced adverse events. Data relating to economic outcomes were limited to tumor necrosis factor inhibitors, but demonstrated increased direct costs associated with both dose escalation and treatment switching.
Conclusion
Dose escalation and treatment switching are common with existing therapies. However, clinical response and remission rates vary, and a proportion of patients fail to achieve optimal clinical and economic outcomes. This highlights the need for more efficacious and durable treatments for patients with moderate-to-severe ulcerative colitis.
Plain Language Summary
Although biologic therapies are effective treatments for patients with moderate-to-severe ulcerative colitis, many fail to respond or lose response over time. These patients may then receive higher doses or more frequent doses of their therapy (called dose escalation) or may switch treatments. We performed a systematic literature review to gather real-world evidence of clinical and economic outcomes for patients who experience dose escalation or treatment switching, including rates of clinical response (improvement in disease activity), clinical remission (little or no disease activity visible endoscopically), colectomy (a surgical procedure to remove all or part of colon), and adverse events, as well as direct healthcare costs. The treatments included in the search were the biologic therapies infliximab, adalimumab, golimumab, vedolizumab, and ustekinumab and the small molecule tofacitinib. We found 56 studies reporting outcomes and treatment patterns for these treatments, with the most data for infliximab and adalimumab. Clinical outcomes varied widely, with rates of clinical response after dose escalation of 20–95%, clinical remission rates of 10–94%, colectomy rates up to 33%, and adverse event rates up to 18%. Between 4% and 35% of patients switched treatments; of these, up to 35% underwent colectomy and 13–38% experienced adverse events. Direct costs were higher after both dose escalation and treatment switching. Since clinical outcomes were so varied and costs were higher for patients experiencing these treatment strategies, the study suggests a need for more effective and durable treatments for patients with moderate-to-severe ulcerative colitis.
Introduction
Ulcerative colitis (UC) is a chronic, relapsing-remitting disease characterized by inflammation of the rectal and colonic mucosa.Citation1 UC is a major form of inflammatory bowel disease (IBD),Citation2 and its worldwide incidence and prevalence are rising.Citation3 The Montreal classification categorizes UC into 3 subgroups defined by disease extent: ulcerative proctitis (rectal involvement only), left-sided or distal UC (inflammation limited to a proportion of the colorectum distal to the splenic flexure), and extensive colitis or pancolitis (involvement extending proximal to the splenic flexure).Citation4 The clinical course of UC is characterized by periods of remission and exacerbation that often require the escalation of doses, switching of treatments, or, ultimately, surgery.Citation5
The updated Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE-II) consensus identifies clinical response as an immediate UC treatment target, clinical remission as an intermediate treatment target, and endoscopic healing as a long-term target; moreover, the statement notes that clinical response and remission are more valuable as therapeutic goals in UC than in Crohn’s disease.Citation6 Improvement in signs and symptoms of UC, histologic healing, and reduction in the risk of adverse long-term outcomes such as colonic dysplasia and colectomy are also reported to be treatment goals of interest.Citation6–9 First-line treatment for mild or moderate UC includes aminosalicylates (5-ASAs), such as sulfasalazine or mesalazine, which are recommended to reduce inflammation.Citation10 5-ASAs are effective for many patients; however, other patients fail to achieve remission on this therapy and may, therefore, require treatment with corticosteroids and, when remission is still not achieved, biologic therapies.Citation11 Moderate-to-severe UC is commonly managed with biologic agents, such as the tumor necrosis factor inhibitor (anti-TNF) therapies infliximab (IFX), adalimumab (ADA), and golimumab (GOL), as well as the integrin α4β7 inhibitor vedolizumab (VDZ) and the interleukin (IL)-12 and IL-23 inhibitor ustekinumab (UST).Citation10,Citation12,Citation13 Pharmacologic therapy options also include an established small molecule, the Janus kinase (JAK) inhibitor tofacitinib (TOF), and newer small molecules, such as the JAK inhibitors upadacitinib and filgotinib, and ozanimod, a sphingosine 1-phosphate receptor modulator. Clinical guidelines on the management of UC recommend treatment with biologic agents or TOF for patients with steroid-dependent active disease, oral steroid-refractory active disease, moderate-to-severe disease, and moderate disease that is refractory to thiopurines.Citation10,Citation12,Citation14
The use of biologics in the treatment of UC has led to improved outcomes, including higher rates of clinical remission and fewer surgeries.Citation15,Citation16 Nonetheless, about one-third of inflammatory bowel disease patients fail to respond to treatment with biologics (primary nonresponse) and 23–46% of patients experience loss of response (LOR) over time (secondary LOR).Citation17–19 In such instances, physicians may consider escalating the dose of the biologic or switching to an alternative treatment.Citation17,Citation18 These approaches have become important tools in the management of UC.Citation20 However, dose escalation and treatment switching may have clinical and safety implications and potential economic consequences. The objective of the study was to identify real-world evidence on dose escalation and treatment switching and associated clinical and economic outcomes among adults with ulcerative colitis treated with IFX, ADA, GOL, VDZ, UST, or TOF.
Materials and Methods
Data Sources and Search Strategies
A systematic literature review (SLR) was conducted to identify studies published in Embase and MEDLINE (via www.embase.com) from database inception up to 26 August 2020. In addition, conference proceedings from meetings of the European Crohn’s and Colitis Organisation, the American College of Gastroenterology, United European Gastroenterology Week, and Digestive Disease Week held from 2017 to 2020 were searched to identify abstracts reporting recent not fully published studies.
Search terms for the SLR were developed in accordance with the PICOS framework (which defines study population, interventions/comparators, outcomes, and study type; see Supplementary Table 1 for the full PICOS statement) and included details on specific aspects of the study question, which was to identify real-world evidence on clinical, safety, and economic outcomes associated with dose escalation and treatment switching with anti-TNF agents, VDZ, UST, and TOF. The exact search terms (including EMTREE terms and free-text search terms) are presented in Supplementary Table 2.
Study Selection
Study eligibility criteria were expressed in terms of the PICOS framework. The population of interest comprised adult UC patients (aged ≥18 years) who were naive to anti-TNF therapy and those who had received prior anti-TNF therapy. Therapies of interest were IFX, ADA, GOL, VDZ, UST, and TOF. Studies considered relevant were those that reported outcomes of interest (Supplementary Table 1) associated with dose escalation and treatment switching for the target therapies.
To assess the eligibility of studies, 2 reviewers independently examined titles and abstracts identified using the search strategy according to the prespecified inclusion/exclusion criteria. The full text of articles that were identified as potentially relevant based on title and abstract were then critically reviewed by 2 reviewers screening independently. At each step, disagreements about any articles were referred to a third reviewer for a consensus. From the eligible studies, the following data were extracted: study design, baseline patient characteristics, and clinical, safety, and economic outcomes related to dose escalation and treatment switching. Clinical outcomes extracted included clinical response, clinical remission, steroid-free clinical remission, avoidance of colectomy, and safety.
Definition of Terms
Dose escalation or optimization of UC therapies can be achieved by increasing the dose or shortening the interval between doses (ie, dose remains at the approved level but is administered more frequently). presents information from the United States FDA-approved Prescribing Information and the European Union EMA-approved Summary of Product Characteristics on the treatments of interest in this review and their regular dosages, which can be escalated or given in a shortened dosing interval in adults with UC.
Table 1 Regular Dosages for Drugs Administered in Patients with UC
Results
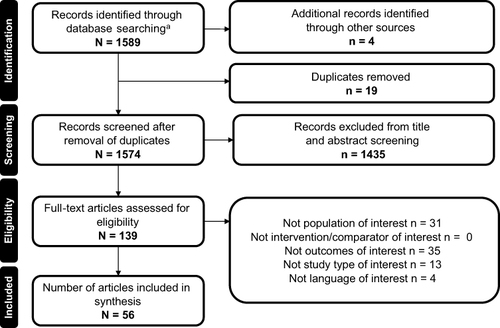
(PRISMA flow diagram) summarizes the identification and selection of 56 included studies (52 full-text articles, 4 conference abstracts). Of the 56 articles and abstracts, 26 reported on dose escalation only, 7 reported on treatment switching only, 22 reported on both dose escalation and treatment switching, and 1 reported on interval lengthening. Characteristics of the included studies are summarized in Supplementary Table 3.Citation21–76
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for publication screening and selection. aEMBASE + Medline.
The following outcomes of interest related to dose escalation were reported for 17 studies (some reported in more than 1 study): clinical response, n=11; clinical remission, n = 11; colectomy, n = 8; adverse events (AEs), n = 6; and economic outcomes, n = 2. The following outcomes related to treatment switching were reported in 12 studies (some reported in more than 1 study): clinical response, n = 6; clinical remission, n = 9; corticosteroid-free remission, n = 5; colectomy, n = 8; AEs, n = 6; and economic outcomes, n = 1. Overall, the majority of the studies were retrospective; the predominance of evidence on dose escalation was reported from 2014 to present, while the evidence of treatment switching was reported more consistently over time (Supplementary Figure 1).
Dose Escalation
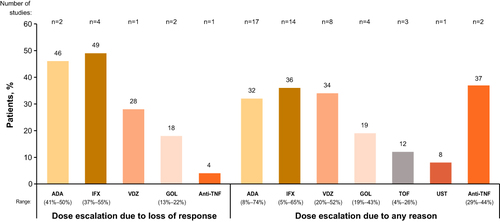
Of the 48 studies reporting dose escalation, 20 reported dose increases only, 14 reported interval shortening, and 14 reported dose escalation via both methods (Supplementary Table 4).Citation21–29,Citation31,Citation32,Citation34–38,Citation40–42,Citation45–52,Citation54,Citation55,Citation57–69,Citation71,Citation72,Citation74–76 One study did not describe the method of dose optimization.Citation24 Follow-up times varied from ≤12 months in 11 studies to >12-≤24 months in 10 studies and >24 months in 8 studies; follow-up times were not reported for the remaining 19 studies. There were 9 reports of dose escalation done to address LOR,Citation31,Citation44,Citation46,Citation63,Citation66–68,Citation75,Citation76 whereas the remaining 39 dose escalations were done for any reason ().Citation22–29,Citation32,Citation34,Citation35,Citation37,Citation38,Citation40–42,Citation45,Citation47–52,Citation55,Citation57–62,Citation64,Citation65,Citation69,Citation71,Citation72,Citation74 The average rate of escalation by dose increase varied greatly, ranging from 80% to 340% relative to the starting dose (Supplementary Table 5).Citation26,Citation29,Citation31,Citation35,Citation36,Citation38,Citation40,Citation46,Citation49,Citation52,Citation57,Citation59,Citation61–63,Citation65–69,Citation75 In studies with follow-up times of ≤12 months, the rate of dose escalation was 11.5–44%, whereas in studies with follow-up times of >12-≤24 months and >24 months, the rate of dose escalation was 8.4–73.5% and 4.9–54.0%, respectively (Supplementary Table 4). The highest mean dose increases reported for IFX were 5–22 mg/kg over 8 weeks (340%),Citation35 100–370 mg/kg over 4 weeks for GOL (270%),Citation35 and 40–112 mg biweekly for ADA (180%).Citation35 Dose escalation by interval shortening alone was reported in 31 studies (Supplementary Table 6);Citation21–23,Citation26–28,Citation31,Citation32,Citation34,Citation36–38,Citation41,Citation44,Citation46,Citation47,Citation49–52,Citation55,Citation58,Citation59,Citation64–68,Citation70,Citation71,Citation74,Citation75 this most commonly occurred with IFX (from 5 mg/kg every 8 to 4 weeks) and ADA (from 40 mg every 2 weeks to once weekly).
Figure 2 Proportion of patients treated with dose escalation due to loss of responseCitation31,Citation44,Citation46,Citation63,Citation66–68,Citation75,Citation76 or any reason.Citation22–29,Citation32,Citation34,Citation35,Citation37,Citation38,Citation40–42,Citation45,Citation47–52,Citation55,Citation57–62,Citation64,Citation65,Citation69,Citation71,Citation72,Citation74 Studies originating in multiple countries and including multiple anti-TNF therapies were counted more than once, giving a total number of references higher than the 48 publications found.
The majority of studies (25; 52.0%) were conducted in mixed treatment-naïve and treatment-experienced populations, in which the experienced patients had at least 1 previous biologic treatment failure. Six studies (12.5%) included only treatment-naïve patients, while 5 (10.4%) included only treatment-experienced patients and 12 (25.0%) did not report patients’ prior biologic treatment experience.
The most commonly investigated escalations were for doses of IFX and ADA and were done across follow-up times of 12–62 months and 11–32 months, respectively, with doses escalated in 42% and 34% of patients in daily practice (in 18 and 19 studies) (Supplementary Figure 2). TOF and UST had the fewest studies reporting dose escalation. Time to dose escalation ranged from 0.7 to 29 months (Supplementary Table 4) and was mainly reported in studies of IFX (n = 7) and ADA (n = 10), in which the rates of dose escalation were similar.
Clinical Response
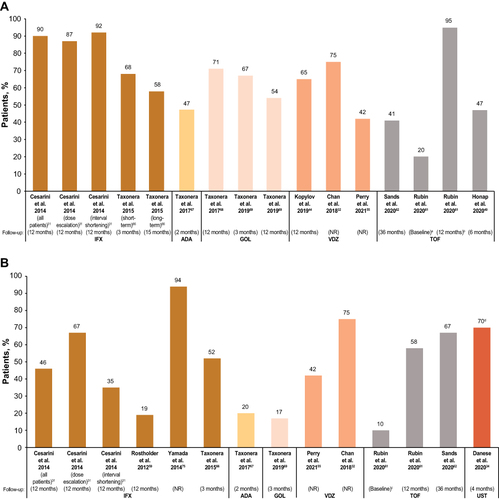
Clinical response after dose escalation was reported in 11 studies,Citation31,Citation32,Citation40,Citation44,Citation55,Citation61,Citation62,Citation66–69 the majority of which (n = 10) comprised populations of both anti-TNF–naïve and anti-TNF−experienced patients (Supplementary Table 7).Citation31,Citation32,Citation40,Citation55,Citation61,Citation62,Citation66–69 The definition of clinical response was consistent across studies as a 3-point decrease in partial Mayo score or as a decrease in partial Mayo score of ≥50% and a final score of ≤2. The rates of short- and long-term (2.8–15 months) clinical response with IFX dose escalation ranged from 58% to 92% (). Short-term (1.8 months) clinical response after ADA dose escalation was reported in 1 study and was achieved by 47% of patients.Citation67 Clinical response after GOL, VDZ, and TOF dose escalations was achieved in 54–71%,Citation68,Citation69 42–75%,Citation32,Citation44,Citation55 and 20–95%Citation40,Citation61,Citation62 of patients, respectively. No study reported clinical response after UST dose escalation.
Figure 3 (A) Rates of clinical responseCitation31,Citation32,Citation40,Citation44,Citation55,Citation61,Citation62,Citation66–69 and (B) clinical remissionCitation31,Citation32,Citation34,Citation55,Citation59,Citation61,Citation62,Citation66,Citation67,Citation69,Citation75 after dose escalation. a20% of patients were in clinical remission at time of dose escalation. bPartial remission; only 20 observed cases for partial remission at 12 months (ie, data missing for 21 of the original 41 patients). c10% of patients were in clinical remission at the time of dose escalation, with such patients who violated protocol being treated with dose escalation at the discretion of the treating physician. dData reported for a subpopulation of patients treated with dose escalation (n=20/40) for whom 16-week follow-up data were available.
Clinical Remission
Clinical remission after dose escalation was reported in 8 studies and 3 abstracts, of which 7 comprised mixed populations of anti-TNF–naïve and anti-TNF–experienced patients (Supplementary Table 8).Citation31,Citation32,Citation34,Citation55,Citation59,Citation61,Citation62,Citation66,Citation67,Citation69,Citation75 The definition of clinical remission was mostly consistent across studies, defined as a Mayo score of 0–2, although in some studies, the definition was an absence of symptoms or a Modified Truelove and Witts Severity Index score of <4. Clinical remission after IFX dose escalation was reported over 12 months in 4 studies, in which the rate ranged from 19% to 94%Citation31,Citation59,Citation66,Citation75 (). Short-term (1.8 months) clinical remission after ADA dose escalation was reported in 1 study and was achieved by 19.7% of patients.Citation67 Clinical remission after GOL, VDZ, TOF, and UST dose escalations was achieved in 16.7%,Citation69 41.7–75.0%,Citation32,Citation55 9.8–57.6%,Citation61,Citation62 and 70.0%Citation34 of patients, respectively.
Colectomy
The need for colectomy for lack of efficacy despite dose escalation was reported in 9 studies (Supplementary Table 9).Citation31,Citation37,Citation59,Citation64,Citation66–69,Citation75 Five of these studies reported on patients undergoing colectomy after IFX dose escalation, with rates ranging from 0% to 33% across 12–38 months.Citation31,Citation37,Citation59,Citation66,Citation75 In 1 study, the colectomy rate at 12 months was 20% after IFX dose escalation and 3.8% after IFX interval shortening.Citation31 Two studies reported rates of colectomy after ADA dose escalation: 10% over 27.6 months in 1 studyCitation64 and 21.0% (16.7% in treatment-naïve patients and 21.9% in treatment-experienced patients) over 17 months in the other study.Citation67 The colectomy rate after GOL dose escalation was reported in 2 studies: 0.0–2.9% over 12 months.Citation68,Citation69 No studies reported colectomy outcomes after VDZ, TOF, or UST dose escalation.
Dose De-Escalation
Dose de-escalation data in patients who had initial dose escalation were reported in 8 studies only for ADA and IFX (Supplementary Table 10).Citation29,Citation31,Citation35,Citation36,Citation50,Citation57,Citation66,Citation67 The overall proportion of patients with dose de-escalation ranged from 17.1% to 80.9%, with mean time to de-escalation of 21 days to 13.6 months.
Adverse Events
Six studies reported AEs associated with dose escalation (Supplementary Figure 3).Citation31,Citation36,Citation61,Citation62,Citation66,Citation75 Regardless of study duration, IFX dose escalation was associated with variable rates of AEs (0.0–18.0%). Treatment discontinuation due to AEs was reported only after dose escalation of IFX, occurring in 8.9% of patients over 24 months.Citation66 The rate of AEs associated with TOF dose escalation was 14.0% over 36 months.Citation62 No safety data were reported for ADA, GOL, VDZ, or UST.
Economic Outcomes
Only 2 studies reported on the costs associated with dose escalation. Black et al (2016) found that ADA dose escalation without subsequent de-escalation was associated with a £1187.00 (8.9%) increase in mean all-cause healthcare costs (defined as any hospital and pharmacy services) over 12 months compared with no escalation; for those patients whose dose was subsequently de-escalated, the increase was £1273.00 (9.5%) (Supplementary Figure 4A).Citation29 Prescription costs accounted for the majority of UC-related healthcare costs for patients whose dose was escalated and those whose dose was not (97% and 96%, respectively). Pöllinger et al (2019) showed that ADA dose escalation without subsequent de-escalation was associated with a €11,160.00 (44.8%) annual increase in direct drug costs (defined as the mean of all ADA prescriptions); for patients who underwent subsequent de-escalation, there was an increase in annual cost of €7808.00 (31.3%) per year (Supplementary Figure 4B).Citation57 No studies reported direct or indirect costs associated with IFX, GOL, VDZ, TOF, or UST.
Treatment Switching
Of the 29 studies reporting on treatment switching, 8 reported outcomes for patients with a history of treatment switching (ie, patients had already switched treatments at study outset), with 18–60% of patients switching because of LOR (Supplementary Table 11).Citation25,Citation33,Citation56,Citation64,Citation68,Citation71,Citation73,Citation74 Of the 8 studies, 7 included only patients who had switched treatments and 4 reported the duration of pre-switch therapy, which ranged from 5.0 to 19.2 months.
The remaining 21 studies reported on treatment switches that occurred during the study observation period, for which follow-up periods ranged from 3 to 62 months (Supplementary Table 12).Citation22–24,Citation26,Citation30,Citation37–39,Citation41,Citation43–45,Citation47,Citation48,Citation51,Citation53,Citation54,Citation60,Citation63,Citation67,Citation72 In studies with follow-up periods of 3–12 months, rates of switching among all UC patients who initiated biologic treatment ranged from 6% to 50%.Citation41,Citation44,Citation48,Citation60,Citation63 In studies with follow-up periods of 12–24 months, switching rates ranged from 4% to 70%.Citation30,Citation38,Citation45,Citation47,Citation67,Citation72 Studies with follow-up periods of >24 months reported switching rates of 4–52%.Citation22–24,Citation26,Citation37,Citation51,Citation53
The median time from start of therapy to treatment switch was reported for 2 studies,Citation48,Citation51 ranging from 3.2 to 7.7 months (Supplementary Table 13). Three other studies reported the time to discontinuation of prior (ie, pre-switch) therapy or time to discontinuation due to LOR.Citation25,Citation37,Citation74
The proportion of UC patients who initiated biologic therapy and switched to another biologic specifically because of LOR was reported in 7 studies and ranged from 4% to 35% over follow-up periods of 12–62 months (Supplementary Table 12). No studies reported the median time from LOR to treatment switch.
The most frequently reported switch was from IFX to ADA, reported in 12 studies (Supplementary Figure 5). Six of the studies reported on history of treatment switching, where 100% of patients had switched from IFX to ADA at study outset for any reason.Citation25,Citation33,Citation56,Citation64,Citation67,Citation71 However, the remaining 6 studies reported on treatment switches that occurred during the study observation period, for which the occurrence of a switch from IFX to ADA ranged from 4% to 53%.Citation22,Citation26,Citation30,Citation39,Citation43,Citation48 Other common switches were ADA to IFX (n = 8), ADA to GOL (n = 3), and IFX to VDZ (n = 2).
Clinical Response and Remission
Nine studies reported the rates of clinical remission after a treatment switch, and, of these, 6 also reported data on clinical response (). Notably, the switches reported in 7 of the 9 studies may be considered switching within class (ie, switching between anti-TNF agents), whereas 2 of the studies reported switches between drugs with different mechanisms of action. Studies reported greater proportions of patients achieving clinical remission with increasing time after switch. The proportion of patients who switched treatments and achieved clinical remission ranged from 10% to 73% at follow-up times of <6 months but ranged from 18% to 100% at follow-up times of ≥6 months. Conversely, the proportion of patients reported as showing a clinical response decreased over time. The proportion of patients who switched and achieved clinical remission ranged from 31.6% to 64.7% during follow-up of <6 months (ie, <26 weeks) but ranged from 18.4% to 52.1% during follow-up of >6 months (ie, ≥26 weeks; ). Five studies reported the proportions of patients who achieved corticosteroid-free clinical remission after a treatment switch, ranging from 22% to 79%.Citation25,Citation33,Citation67,Citation68,Citation71
Table 2 Clinical Remission and Clinical Response Following Treatment Switch
Colectomy
The proportion of patients undergoing colectomy after a treatment switch was reported in 8 studies (Supplementary Table 14). Of the 8 studies, 7 were considered studies of switching within classCitation25,Citation33,Citation64,Citation67,Citation68,Citation71 and 1 reported on switches between drugs with different mechanisms of action.Citation51,Citation56 Among the studies of switching within class, the rate of colectomy reached 20% over follow-up periods of 12–120 weeks. Among the treatment switching studies, the proportion of patients who underwent colectomy was up to 35% (at 108 weeks).
Adverse Events
Six studies reported AEs associated with treatment switching (Supplementary Figure 6);Citation25,Citation56,Citation64,Citation71,Citation73,Citation74 4 of these were studies of switching within class, and the remaining 2 reported AEs after switches between drugs with different mechanisms of action (specifically, IFX and VDZ). Overall, AEs occurred in 13–38% of patients who switched treatment. Four of these studies additionally reported the proportion of patients discontinuing treatment because of AEs after a switch, which ranged from 3% to 20%.
Economic Outcomes
One study reported economic outcomes associated with treatment switching. Null et al (2017) found that the mean quarterly total healthcare expenditure was highest for patients who switched from anti-TNFs (n = 399) at US$15,004 (2014 currency) compared with US$9632 for the patients who maintained the same treatment at a stable dose (n = 1253), representing a 55.8% cost increase.Citation48 Most of these costs were accounted for by total anti-TNF–related pharmacy costs (US$9033 vs US$7362, respectively) and by total medical costs (US$5343 vs US$1723, respectively).
Discussion
This SLR captured real-world evidence on the rates of dose escalation and treatment switching and the associated clinical and economic outcomes among UC patients. Overall, our results showed that dose escalation and treatment switching are commonly required among patients receiving biologic therapies for UC and that rates of clinical response or remission vary considerably. The rates of dose escalation of anti-TNFs, VDZ, TOF, and UST in daily practice ranged from 4.0–65.0%, 20.0–52.1%, 4.3–25.6%, and 8.0%, respectively, and the rates of treatment switching in daily practice ranged from 4.0% to 70.0%.
Findings on the rate of dose escalation were consistent with those reported in a recent SLR on dose escalation and treatment switching in UC by Gemayel et al (2019).Citation5 However, the rate of treatment switching in daily practice reported in the current SLR was approximately 3-fold greater than that reported by Gemayel et al (range: 1.0% at 6 months to 26.0% at 2 years). This may be explained in part by the emergence of new treatments for UC since the publication of Gemayel et al (data captured 2006–2017) that have increased switching opportunities in daily practice. This SLR also captured a greater number of reasons for switching (LOR, infusion reactions, AEs, patient preferences, and primary nonresponse) compared with Gemayel et al, which reported only LOR and AEs as reasons for treatment switching.Citation5
Similarly, time to dose escalation or treatment switching among UC patients, where reported, ranged between 0.7–29 months and 3.2–7.1 months, respectively. Data on time to dose escalation with GOL, VDZ, and TOF were scarce, possibly owing to the lack of studies assessing dose escalation with these agents. These findings were also consistent with those from Gemayel et al.Citation5 However, the available data from the current study compared with those reported by Gemayel et al demonstrate that time to dose escalation is shorter with GOL (4.7 months) and TOF (1.3 months) than with IFX (up to 29 months), ADA (up to 8.0 months), and VDZ (up to 18.7 months). Further research is needed to understand the factors that influence the time to dose escalation for each drug.
After dose escalation and treatment switching, the proportions of patients achieving clinical response and clinical remission varied greatly. With regard to treatment switching, it is not possible to meaningfully compare the proportions of patients achieving clinical response or remission after switching within a single drug class vs switching between drugs with different mechanisms of action, owing to the small number of studies reporting on switches between drugs with different mechanisms of action.
Considerable proportions of patients were reported to still require colectomy after dose escalation (up to 33% in moderate-to-severe UC patients) or treatment switching (35%). Real-world data on AEs were limited to 6 studies associated with either treatment pattern. AEs were reported to have occurred after dose escalation of IFX and TOF and after switches to ADA, IFX, and VDZ.
A large degree of heterogeneity was observed in the rates of dose escalation and treatment switching across the studies included in this review. Such heterogeneity may stem from the considerable differences noted across the studies in terms of sample size, duration of follow-up, study setting (from single-center to large claims database studies) and region. The noted differences in sample size, follow-up, and study setting may also in part explain the heterogeneity seen in clinical response and remission. Furthermore, most of the evidence was derived from retrospective studies. Hence, it is difficult to draw any conclusion based on any single real-world study by comparing and interpreting the proportion of patients treated with dose escalation or treatment switching across the different therapies and lines of treatments, as well as to make any correlations between the use of prior anti-TNF therapy and the time to dose escalation or treatment switching. However, future meta-analyses of retrospective studies may focus on a quantitative comparison.
Other limitations encountered in this review suggest a need for caution when interpreting the findings. Durations of follow-up were mostly reported as 1–2 years, necessitating longer-term data on the current anti-TNF biologic therapies for UC. There was a lack of data on some clinical outcomes; rates of clinical relapse and hospitalization, the incidence of colorectal cancer, and rates of endoscopic remission after dose escalation and treatment switching could not be compared between treatments.
Data regarding the economic outcomes associated with dose escalation and treatment switching were particularly scarce and limited to direct costs associated with ADA or unspecified anti-TNF therapy; no studies assessed reported indirect costs. However, it should be noted that an analysis of the economic outcomes of dose escalation and treatment switching may be feasible based on the clinical data identified during this SLR. That is, the data regarding levels of dose escalation, types of treatment switch and the clinical outcomes associated with these may be used as the basis for an economic analysis of dose escalation and treatment switching for the drugs included in the scope of this study.
Further research on economic outcomes of real-world UC treatment patterns is warranted by the current or anticipated market entry of biosimilars for IFX and ADA. Biosimilar uptake has been uneven across different regulatory landscapes, which incentivize biosimilar use to varying degrees.Citation77,Citation78 Biosimilar use is generally expected to increase in the coming years, as real-world evidence accrues to suggest that clinical outcomes are comparable between originator and biosimilar products, at lower economic cost.Citation77–80 The degree of cost savings with biosimilars compared with originator products varies, but, through competition with originator products, biosimilar use is expected to drive down prices overall.Citation80,Citation81 With lower acquisition costs, biosimilar dose escalation or treatment switching to a biosimilar would, prima facie, be expected to lower direct costs compared with dose escalation and treatment switching with originators; however, real-world evidence of the economic outcomes associated with these treatment patterns is, as yet, unavailable.
Conclusion
Overall, this SLR demonstrated that dose escalation and treatment switching are commonly required for patients with moderate-to-severe UC in routine clinical practice and are associated with variable clinical response and clinical remission rates. This may be indicative of suboptimal clinical and economic outcomes, underscoring the need for more efficacious and durable treatments for patients with moderate-to-severe UC.
Data Sharing Statement
Bristol Myers Squibb’s policy on data sharing can be found at https://www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Liam Wilson was an employee of Amaris Consulting (Shanghai, China), which conducted the systematic literature review funded by Bristol Myers Squibb (Princeton, NJ, USA). Harpreet Singh was an employee of Amaris Consulting and Tom Tencer was an employee of Bristol Myers Squibb at the time the research was conducted. Jinender Kumar is an employee and/or shareholder of Bristol Myers Squibb (Princeton, NJ, USA). The authors report no other conflicts of interest in this work.
Acknowledgments
The authors thank their colleagues at Amaris Consulting for contributions to this systematic literature review: Idris Watanyar and Matthieu Hugon (study selection), Patricia Ladrón de Guevara (study design), Petya Kodjamanova (data quality checks and inquiries), and Rito Bergemann and Anuja Pandey (study design and data analysis and interpretation). Writing and editorial support were provided by Eleanor Bush, MA, and Diana Arper, MSc, of Peloton Advantage (Parsippany, NJ, USA), an OPEN Health company, funded by Bristol Myers Squibb.
Additional information
Funding
References
- Ordas I, Eckmann L, Talamini M, Baumgart DC, Sandborn WJ. Ulcerative colitis. Lancet. 2012;380(9853):1606–1619. doi:10.1016/S0140-6736(12)60150-0
- Alatab S, Sepanlou SG, Ikuta K; GBD 2017 Inflammatory Bowel Disease Collaborators. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17–30. doi:10.1016/S2468-1253(19)30333-4
- Du L, Ha C. Epidemiology and pathogenesis of ulcerative colitis. Gastroenterol Clin North Am. 2020;49(4):643–654. doi:10.1016/j.gtc.2020.07.005
- Satsangi J, Silverberg MS, Vermeire S, Colombel JF. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut. 2006;55(6):749–753. doi:10.1136/gut.2005.082909
- Gemayel NC, Rizzello E, Atanasov P, Wirth D, Borsi A. Dose escalation and switching of biologics in ulcerative colitis: a systematic literature review in real-world evidence. Curr Med Res Opin. 2019;35(11):1911–1923. doi:10.1080/03007995.2019.1631058
- Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: an update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) initiative of the International Organization for the Study of IBD (IOIBD): determining therapeutic goals for treat-to-target strategies in IBD. Gastroenterology. 2021;160(5):1570–1583. doi:10.1053/j.gastro.2020.12.031
- Ungaro R, Colombel JF, Lissoos T, Peyrin-Biroulet L. A treat-to-target update in ulcerative colitis: a systematic review. Am J Gastroenterol. 2019;114(6):874–883. doi:10.14309/ajg.0000000000000183
- Peyrin-Biroulet L, Sandborn W, Sands BE, et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): determining therapeutic goals for treat-to-target. Am J Gastroenterol. 2015;110(9):1324–1338. doi:10.1038/ajg.2015.233
- Danese S, Fiocchi C. Ulcerative colitis. N Engl J Med. 2011;365(18):1713–1725. doi:10.1056/NEJMra1102942
- Harbord M, Eliakim R, Bettenworth D, et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 2: current management. J Crohns Colitis. 2017;11(7):769–784. doi:10.1093/ecco-jcc/jjx009
- Burri E, Maillard MH, Schoepfer AM, et al. Treatment algorithm for mild and moderate-to-severe ulcerative colitis: an update. Digestion. 2020;101(Suppl 1):2–15. doi:10.1159/000504092
- Feuerstein JD, Isaacs KL, Schneider Y, Siddique SM, Falck-Ytter Y, Singh S. AGA Clinical Practice Guidelines on the Management of Moderate to Severe Ulcerative Colitis. Gastroenterology. 2020;158(5):1450–1461. doi:10.1053/j.gastro.2020.01.006
- Pantavou K, Yiallourou AI, Piovani D, et al. Efficacy and safety of biologic agents and tofacitinib in moderate-to-severe ulcerative colitis: a systematic overview of meta-analyses. United European Gastroenterol J. 2019;7(10):1285–1303. doi:10.1177/2050640619883566
- Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD. ACG Clinical Guideline: ulcerative colitis in adults. Am J Gastroenterol. 2019;114(3):384–413. doi:10.14309/ajg.0000000000000152
- Tsai L, Ma C, Dulai PS, et al. Contemporary risk of surgery in patients with ulcerative colitis and Crohn’s disease: a meta-analysis of population-based cohorts. Clin Gastroenterol Hepatol. 2021;19(10):2031–2045.e2011. doi:10.1016/j.cgh.2020.10.039
- Amiot A, Peyrin-Biroulet L. Current, new and future biological agents on the horizon for the treatment of inflammatory bowel diseases. Therap Adv Gastroenterol. 2015;8(2):66–82. doi:10.1177/1756283X14558193
- Roda G, Jharap B, Neeraj N, Colombel JF. Loss of response to anti-TNFs: definition, epidemiology, and management. Clin Transl Gastroenterol. 2016;7:e135. doi:10.1038/ctg.2015.63
- Shahwan KT, Kimball AB. Managing the dose escalation of biologics in an era of cost containment: the need for a rational strategy. Int J Womens Dermatol. 2016;2(4):151–153. doi:10.1016/j.ijwd.2016.09.003
- Gisbert JP, Marín AC, McNicholl AG, Chaparro M. Systematic review with meta-analysis: the efficacy of a second anti-TNF in patients with inflammatory bowel disease whose previous anti-TNF treatment has failed. Aliment Pharmacol Ther. 2015;41(7):613–623. doi:10.1111/apt.13083
- Ehrenberg R, Griffith J, Theigs C, McDonald B. Dose escalation assessment among targeted immunomodulators in the management of inflammatory bowel disease. J Manag Care Spec Pharm. 2020;26(6):758–765. doi:10.18553/jmcp.2020.19388
- Afif W, Leighton JA, Hanauer SB, et al. Open-label study of adalimumab in patients with ulcerative colitis including those with prior loss of response or intolerance to infliximab. Inflamm Bowel Dis. 2009;15(9):1302–1307. doi:10.1002/ibd.20924
- Alzafiri R, Holcroft CA, Malolepszy P, Cohen A, Szilagyi A. Infliximab therapy for moderately severe Crohn’s disease and ulcerative colitis: a retrospective comparison over 6 years. Clin Exp Gastroenterol. 2011;4:9–17. doi:10.2147/CEG.S16168
- Amiot A, Serrero M, Peyrin-Biroulet L, et al. Three-year effectiveness and safety of vedolizumab therapy for inflammatory bowel disease: a prospective multi-centre cohort study. Aliment Pharmacol Ther. 2019;50(1):40–53. doi:10.1111/apt.15294
- Armuzzi A, DiBonaventura MD, Tarallo M, et al. Treatment patterns among patients with moderate-to-severe ulcerative colitis in the United States and Europe. PLoS One. 2020;15(1):e0227914. doi:10.1371/journal.pone.0227914
- Baert F, Vande Casteele N, Tops S, et al. Prior response to infliximab and early serum drug concentrations predict effects of adalimumab in ulcerative colitis. Aliment Pharmacol Ther. 2014;40(11–12):1324–1332. doi:10.1111/apt.12968
- Baki E, Zwickel P, Zawierucha A, et al. Real-life outcome of anti-tumor necrosis factor α in the ambulatory treatment of ulcerative colitis. World J Gastroenterol. 2015;21(11):3282–3290. doi:10.3748/wjg.v21.i11.3282
- Bálint A, Farkas K, Palatka K, et al. Efficacy and safety of adalimumab in ulcerative colitis refractory to conventional therapy in routine clinical practice. J Crohns Colitis. 2016;10(1):26–30. doi:10.1093/ecco-jcc/jjv169
- Barberio B, Zingone F, D’Incà R, et al. Infliximab originator, infliximab biosimilar, and adalimumab are more effective in Crohn’s disease than ulcerative colitis: a real-life cohort study. Clin Translat Gastroenterol. 2020;11(5):e00177. doi:10.14309/ctg.0000000000000177
- Black CM, Yu E, McCann E, Kachroo S. Dose escalation and healthcare resource use among ulcerative colitis patients treated with adalimumab in English hospitals: an analysis of real-world data. PLoS One. 2016;11(2):e0149692. doi:10.1371/journal.pone.0149692
- Brady JE, Stott-Miller M, Mu G, Perera S. Treatment patterns and sequencing in patients with inflammatory bowel disease. Clin Ther. 2018;40(9):1509–1521.e1505. doi:10.1016/j.clinthera.2018.07.013
- Cesarini M, Katsanos K, Papamichael K, et al. Dose optimization is effective in ulcerative colitis patients losing response to infliximab: a collaborative multicentre retrospective study. Dig Liver Dis. 2014;46(2):135–139. doi:10.1016/j.dld.2013.10.007
- Chan W, Lynch N, Bampton P, et al. Entyvio lengthen dose-interval study: lengthening vedolizumab dose interval and the risk of clinical relapse in inflammatory bowel disease. Eur J Gastroenterol Hepatol. 2018;30(7):735–740. doi:10.1097/MEG.0000000000001150
- Christensen KR, Steenholdt C, Brynskov J. Clinical outcome of adalimumab therapy in patients with ulcerative colitis previously treated with infliximab: a Danish single-center cohort study. Scand J Gastroenterol. 2015;50(8):1018–1024. doi:10.3109/00365521.2015.1019558
- Danese S, Panaccione R, Peyrin-Biroulet L, et al. Dose adjustment in patients with moderate-to-severe ulcerative colitis: results from the UNIFI maintenance study long-term extension [abstract P448]. J Crohns Colitis. 2020;14(Suppl 1):S403. doi:10.1093/ecco-jcc/jjz203.577
- Dignass A, Waller J, Cappelleri JC, et al. Living with ulcerative colitis in Germany: a retrospective analysis of dose escalation, concomitant treatment use and healthcare costs. J Med Econ. 2020;23(4):415–427. doi:10.1080/13696998.2019.1707210
- Fernández-Salazar L, Barrio J, Muñoz F, et al. Frequency, predictors, and consequences of maintenance infliximab therapy intensification in ulcerative colitis. Rev Esp Enferm Dig. 2015;107(9):527–533.
- Fernández-Salazar L, Muñoz F, Barrio J, et al. Infliximab in ulcerative colitis: real-life analysis of factors predicting treatment discontinuation due to lack of response or colectomy: ECIA (ACAD Colitis and Infliximab Study). Scand J Gastroenterol. 2016;51(2):186–195. doi:10.3109/00365521.2015.1070900
- Harper JW, Sinanan MN, Zisman TL. Increased body mass index is associated with earlier time to loss of response to infliximab in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2013;19(10):2118–2124. doi:10.1097/MIB.0b013e31829cf401
- Hiroz P, Vavricka SR, Fournier N, et al. Analysis of TNF-antagonist switch over time and associated risk factors in the Swiss Inflammatory Bowel Disease Cohort. Scand J Gastroenterol. 2014;49(10):1207–1218. doi:10.3109/00365521.2014.946082
- Honap S, Chee D, Chapman TP, et al. Real-world effectiveness of tofacitinib for moderate to severe ulcerative colitis: a multicentre UK experience. J Crohns Colitis. 2020;14(10):1385–1393. doi:10.1093/ecco-jcc/jjaa075
- Hussey M, Mc Garrigle R, Kennedy U, et al. Long-term assessment of clinical response to adalimumab therapy in refractory ulcerative colitis. Eur J Gastroenterol Hepatol. 2016;28(2):217–221. doi:10.1097/MEG.0000000000000515
- Iborra M, Pérez-Gisbert J, Bosca-Watts MM, et al. Effectiveness of adalimumab for the treatment of ulcerative colitis in clinical practice: comparison between anti-tumour necrosis factor-naïve and non-naïve patients. J Gastroenterol. 2017;52(7):788–799. doi:10.1007/s00535-016-1274-1
- Jung YS, Han M, Park S, Cheon JH. Biologic use patterns and predictors for non-persistence and switching of biologics in patients with inflammatory bowel disease: a nationwide population-based study. Dig Dis Sci. 2020;65(5):1436–1444. doi:10.1007/s10620-019-05867-1
- Kopylov U, Avni-Biron I, Ron Y, et al. Effectiveness and safety of vedolizumab for maintenance treatment in inflammatory bowel disease-The Israeli real world experience. Dig Liver Dis. 2019;51(1):68–74. doi:10.1016/j.dld.2018.07.040
- Lindsay JO, Armuzzi A, Gisbert JP, et al. Indicators of suboptimal tumor necrosis factor antagonist therapy in inflammatory bowel disease. Dig Liver Dis. 2017;49(10):1086–1091. doi:10.1016/j.dld.2017.07.010
- Ma C, Huang V, Fedorak DK, et al. Outpatient ulcerative colitis primary anti-TNF responders receiving adalimumab or infliximab maintenance therapy have similar rates of secondary loss of response. J Clin Gastroenterol. 2015;49(8):675–682. doi:10.1097/MCG.0000000000000265
- McDermott E, Murphy S, Keegan D, O’Donoghue D, Mulcahy H, Doherty G. Efficacy of adalimumab as a long term maintenance therapy in ulcerative colitis. J Crohns Colitis. 2013;7(2):150–153. doi:10.1016/j.crohns.2012.03.016
- Null KD, Xu Y, Pasquale MK, et al. Ulcerative colitis treatment patterns and cost of care. Value Health. 2017;20(6):752–761. doi:10.1016/j.jval.2017.02.005
- O’Donnell S, Stempak JM, Steinhart AH, Silverberg MS. Higher rates of dose optimisation for infliximab responders in ulcerative colitis than in Crohn’s disease. J Crohns Colitis. 2015;9(10):830–836. doi:10.1093/ecco-jcc/jjv115
- Olivares D, Alba C, Pérez I, Roales V, Rey E, Taxonera C. Differences in the need for adalimumab dose optimization between Crohn’s disease and ulcerative colitis. Rev Esp Enferm Dig. 2019;111(11):846–851. doi:10.17235/reed.2019.6148/2018
- Ollech JE, Dwadasi S, Rai V, et al. Efficacy and safety of induction therapy with calcineurin inhibitors followed by vedolizumab maintenance in 71 patients with severe steroid-refractory ulcerative colitis. Aliment Pharmacol Ther. 2020;51(6):637–643. doi:10.1111/apt.15616
- Oussalah A, Chevaux JB, Fay R, Sandborn WJ, Bigard MA, Peyrin-Biroulet L. Predictors of infliximab failure after azathioprine withdrawal in Crohn’s disease treated with combination therapy. Am J Gastroenterol. 2010;105(5):1142–1149. doi:10.1038/ajg.2010.158
- Papamichael K, Rivals-Lerebours O, Billiet T, et al. Long-term outcome of patients with ulcerative colitis and primary non-response to infliximab. J Crohns Colitis. 2016;10(9):1015–1023. doi:10.1093/ecco-jcc/jjw067
- Patel H, Lissoos T, Rubin DT. Indicators of suboptimal biologic therapy over time in patients with ulcerative colitis and Crohn’s disease in the United States. PLoS One. 2017;12(4):e0175099. doi:10.1371/journal.pone.0175099
- Perry C, Fischer K, Elmoursi A, et al. Vedolizumab dose escalation improves therapeutic response in a subset of patients with ulcerative colitis. Dig Dis Sci. 2021;66(6):2051–2058. doi:10.1007/s10620-020-06486-x
- Peyrin-Biroulet L, Laclotte C, Roblin X, Bigard MA. Adalimumab induction therapy for ulcerative colitis with intolerance or lost response to infliximab: an open-label study. World J Gastroenterol. 2007;13(16):2328–2332. doi:10.3748/wjg.v13.i16.2328
- Pöllinger B, Schmidt W, Seiffert A, Imhoff H, Emmert M. Costs of dose escalation among ulcerative colitis patients treated with adalimumab in Germany. Eur J Health Econ. 2019;20(2):195–203. doi:10.1007/s10198-017-0953-z
- Reinglas J, Gonczi L, Verdon C, et al. Low rate of drug discontinuation, frequent need for dose adjustment, and no association with development of new arthralgia in patients treated with vedolizumab: results from a tertiary referral IBD center. Dig Dis Sci. 2020;65(7):2046–2053. doi:10.1007/s10620-019-05982-z
- Rostholder E, Ahmed A, Cheifetz AS, Moss AC. Outcomes after escalation of infliximab therapy in ambulatory patients with moderately active ulcerative colitis. Aliment Pharmacol Ther. 2012;35(5):562–567. doi:10.1111/j.1365-2036.2011.04986.x
- Rubin DT, Mody R, Davis KL, Wang CC. Real-world assessment of therapy changes, suboptimal treatment and associated costs in patients with ulcerative colitis or Crohn’s disease. Aliment Pharmacol Ther. 2014;39(10):1143–1155. doi:10.1111/apt.12727
- Rubin DT, Dubinsky MC, Panés J, et al. Efficacy of tofacitinib dose escalation to 10 mg BID in patients with UC after completing maintenance therapy in remission and losing response: data from OCTAVE open-label, long-term extension study [abstract DOP75]. J Crohns Colitis. 2020;14(Suppl 1):S112–S113. doi:10.1093/ecco-jcc/jjz203.114
- Sands BE, Moss AC, Armuzzi A, et al. Efficacy and safety of escalation to tofacitinib 10 mg Bid for patients with UC following loss of response on 5 mg BID maintenance therapy: results from OCTAVE open-label, long-term extension study [abstract DOP73]. J Crohns Colitis. 2020;14(Suppl 1):S110–S111. doi:10.1093/ecco-jcc/jjz203.112
- Stefanovic S, Detrez I, Compernolle G, et al. Endoscopic remission can be predicted by golimumab concentrations in patients with ulcerative colitis treated with the changed label. Eur J Gastroenterol Hepatol. 2021;33(1):54–61. doi:10.1097/MEG.0000000000001843
- Taxonera C, Estellés J, Fernández-Blanco I, et al. Adalimumab induction and maintenance therapy for patients with ulcerative colitis previously treated with infliximab. Aliment Pharmacol Ther. 2011;33(3):340–348. doi:10.1111/j.1365-2036.2010.04531.x
- Taxonera C, Olivares D, Mendoza JL, Díaz-Rubio M, Rey E. Need for infliximab dose intensification in Crohn’s disease and ulcerative colitis. World J Gastroenterol. 2014;20(27):9170–9177. doi:10.3748/wjg.v20.i27.9170
- Taxonera C, Barreiro-de Acosta M, Calvo M, et al. Infliximab dose escalation as an effective strategy for managing secondary loss of response in ulcerative colitis. Dig Dis Sci. 2015;60(10):3075–3084. doi:10.1007/s10620-015-3735-4
- Taxonera C, Iglesias E, Muñoz F, et al. Adalimumab maintenance treatment in ulcerative colitis: outcomes by prior anti-TNF use and efficacy of dose escalation. Dig Dis Sci. 2017;62(2):481–490. doi:10.1007/s10620-016-4398-5
- Taxonera C, Rodríguez C, Bertoletti F, et al. Clinical outcomes of golimumab as first, second or third anti-TNF agent in patients with moderate-to-severe ulcerative colitis. Inflamm Bowel Dis. 2017;23(8):1394–1402. doi:10.1097/MIB.0000000000001144
- Taxonera C, Iborra M, Bosca-Watts MM, et al. Early dose optimization of golimumab induces late response and long-term clinical benefit in moderately to severely active ulcerative colitis. Curr Med Res Opin. 2019;35(7):1297–1304. doi:10.1080/03007995.2019.1579557
- Torres P, Cañete F, Núñez L, et al. Spacing the administration interval of anti-TNF agents: a valid strategy for patients with inflammatory bowel disease? Dig Dis Sci. 2020;65(7):2036–2043. doi:10.1007/s10620-019-06010-w
- Tursi A, Elisei W, Picchio M, et al. Effectiveness of adalimumab for ambulatory ulcerative colitis patients after failure of infliximab treatment: a first “real-life” experience in primary gastroenterology centers in Italy. Ann Gastroenterol. 2014;27(4):369–373.
- Tursi A, Elisei W, Faggiani R, et al. Effectiveness and safety of adalimumab to treat outpatient ulcerative colitis: a real-life multicenter, observational study in primary inflammatory bowel disease centers. Medicine. 2018;97(34):e11897. doi:10.1097/MD.0000000000011897
- Viola A, Pugliese D, Renna S, et al. Outcome in ulcerative colitis after switch from adalimumab/golimumab to infliximab: a multicenter retrospective study. Dig Liver Dis. 2019;51(4):510–515. doi:10.1016/j.dld.2018.10.013
- Wang Y, Wang J, Pekow J, et al. Outcome of elective switching to vedolizumab in inflammatory bowel disease patients under tumor necrosis factor antagonist-maintained clinical remission. J Gastroenterol Hepatol. 2019;34(12):2090–2095. doi:10.1111/jgh.14751
- Yamada S, Yoshino T, Matsuura M, et al. Long-term efficacy of infliximab for refractory ulcerative colitis: results from a single center experience. BMC Gastroenterol. 2014;14:80. doi:10.1186/1471-230X-14-80
- Yamamoto-Furusho JK, Al Harbi O, Armuzzi A, et al. Incidence of suboptimal response to tumor necrosis factor antagonist therapy in inflammatory bowel disease in newly industrialised countries: the EXPLORE study. Dig Liver Dis. 2020;52(8):869–877. doi:10.1016/j.dld.2020.05.031
- Rémuzat C, Dorey J, Cristeau O, Ionescu D, Radière G, Toumi M. Key drivers for market penetration of biosimilars in Europe. J Market Access Health Policy. 2017;5(1):1272308. doi:10.1080/20016689.2016.1272308
- Bhat S, Limdi JK, Cross RK, Farraye FA. does similarity breed contempt? A review of the use of biosimilars in inflammatory bowel disease. Dig Dis Sci. 2021;66(8):2513–2532. doi:10.1007/s10620-021-07114-y
- Danese S, Bonovas S, Peyrin-Biroulet L. Biosimilars in IBD: from theory to practice. Nat Rev Gastroenterol Hepatol. 2017;14(1):22–31. doi:10.1038/nrgastro.2016.155
- Park SH, Park JC, Lukas M, Kolar M, Loftus EV. Biosimilars: concept, current status, and future perspectives in inflammatory bowel diseases. Intest Res. 2020;18(1):34–44. doi:10.5217/ir.2019.09147
- San-Juan-Rodriguez A, Gellad WF, Good CB, Hernandez I. Trends in list prices, net prices, and discounts for originator biologics facing biosimilar competition. JAMA Netw Open. 2019;2(12):e1917379. doi:10.1001/jamanetworkopen.2019.17379