Abstract
Health care spending has risen steadily in most countries, becoming a concern for decision-makers worldwide. Commentators often point to new medical technology as the key driver for burgeoning expenditures. This paper critically appraises this conjecture, based on an analysis of the existing literature, with the aim of offering a more detailed and considered analysis of this relationship. Several databases were searched to identify relevant literature. Various categories of studies (eg, multivariate and cost-effectiveness analyses) were included to cover different perspectives, methodological approaches, and issues regarding the link between medical technology and costs. Selected articles were reviewed and relevant information was extracted into a standardized template and analyzed for key cross-cutting themes, ie, impact of technology on costs, factors influencing this relationship, and methodological challenges in measuring such linkages. A total of 86 studies were reviewed. The analysis suggests that the relationship between medical technology and spending is complex and often conflicting. Findings were frequently contingent on varying factors, such as the availability of other interventions, patient population, and the methodological approach employed. Moreover, the impact of technology on costs differed across technologies, in that some (eg, cancer drugs, invasive medical devices) had significant financial implications, while others were cost-neutral or cost-saving. In light of these issues, we argue that decision-makers and other commentators should extend their focus beyond costs solely to include consideration of whether medical technology results in better value in health care and broader socioeconomic benefits.
Introduction
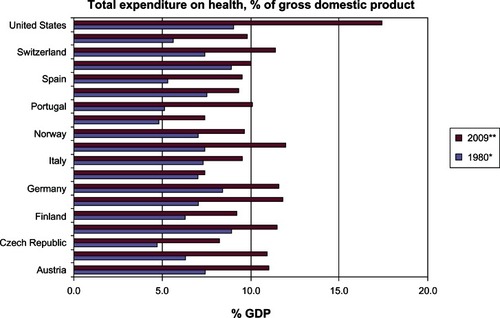
Health care spending has risen at rates greater than gross domestic product in most OECD countries. In 2009, average health spending reached 9.5% of gross domestic product, up from 8.8% in 2008Citation1 (). During the same time period, average per capita spending increased by an average of 3.8% in 2008 and 3.5% in 2009, with public spending on health growing at an even faster rate of 4.8% and 4.1%, respectively.Citation1 For most countries, rising health expenditure is considered an enduring challenge and one that requires a complex balancing act between cost control, affordable and equitable access to beneficial treatments, and support for innovation.
Figure 1 Total expenditure on health as a percentage of gross domestic product (GDP) (1980–2009).
OECD Health Data 2011.Citation1
A number of factors have been identified as contributors to spending growth, including the ageing of populations, increased public demand and expectations, personal income growth, rising prices of physician and hospital services (eg, labor costs), and inefficiencies in the organization and payment of care. For example, the growth in life expectancy has had an obvious yet gradual impact on the demand for health care. Although the use of care depends ultimately on the health status of a person and not necessarily on their age cohort(s), elderly people use health care more often and more intensively than younger populations, with a high proportion of costs garnered at the end of life.Citation2 Longer life spans, in concert with an increase in unhealthy lifestyles, have also contributed to an increased prevalence of disease, particularly chronic conditions such as obesity, diabetes, and cancer. Greater prevalence of chronic conditions are likely to increase spending both through an increase in treated prevalence (ie, number of cases treated) and the cost of treatment (ie, spending per case).
However, analysts often point to advances in medical technology and their diffusion across health systems as the principal driver for burgeoning expenditures.Citation3–Citation10 This paper critically examines this conjecture, based on an analysis of a broad range of existing evidence on the relationship between medical technology diffusion and health expenditure. We strive to focus on medical devices, given the gap in the literature on their role in health expenditures, which has predominantly centered on pharmaceuticals, and because the sector has grown considerably in recent years. Not only are there substantially more medical technologies on the market, but they have grown increasingly sophisticated.
The paper is structured as follows. We first outline the methods used to review the literature, followed by a summary of the available evidence. The paper then discusses the complexities inherent to ascertaining the impact of technology on spending, including some of the methodological challenges associated with demonstrating and quantifying this link. Based on the analysis, we close by arguing that while the impact of medical technology on rising costs is an important concern and area of inquiry, attention should also be focused on exploring whether investments in medical technology result in better value, as measured by therapeutic benefit, cost-effectiveness, and other important outcomes (eg, quality of life, improved productivity) in health care, and under which conditions technologies allow for the most effective and efficient use of available health care resources. We offer some general suggestions for what might be done to support this end.
Materials and methods
A literature review was conducted to explore the current evidence base on the relationship between medical technology and health care expenditures. Unlike previous studies in this area, we considered a wide range of literature to ensure adequate coverage of different methodological approaches and ideological perspectives for assessing this relationship. The categories of literature included in the search and review included general and descriptive analyses, policy analyses, literature reviews, multivariate analyses, cost-effectiveness analyses, and cost impact studies of specific technologies. presents and describes the various study types included in the review.
Table 1 Types of studies included in the review
Key databases, including PubMed, EMBASE, MEDLINE, and EconLit, were searched to identify relevant literature. The search terms employed to identify relevant literature included “technolog* AND (expenditure OR cost) AND (health OR healthcare)”, and “medical AND technolog* AND (expenditure OR cost)”.
To identify relevant cost-effectiveness analyses across all medical technologies would be a considerable task. Therefore, we took advantage of two previously completed systematic reviews of economic evaluations of medical devices in the cardiology and orthopedic sectors, the two most significant markets for therapeutic devices.Citation11 In these reviews, we used the National Health Service Economic Evaluation DatabaseCitation12 for the searches, which contains structured reviews (abstracts) of full economic evaluations of health care treatments and programs. In these two previously conducted studies, we employed the following search terms “cardiology”, “cardiac rhythm management”, “cardiovascular”, “coronary stents”, “cardiac resychronization”, “implantable cardioverter defibrillators”, “orthopaedic”, “hip”, “knee”, “shoulder”, “ankle”, “elbow”, “arthroplasty”, and “joint”.
All the relevant abstracts were reviewed, from both the general literature review and the review of National Health Service Economic Evaluation Database. Duplicate and irrelevant abstracts were identified and eliminated. Selected articles were reviewed according to a data extraction form, developed in Microsoft Excel, to standardize the review and facilitate subsequent analysis of the collated information. The categories of information extraction included: basic bibliographic information; publication year; literature type (eg, descriptive analysis); study aims; technologies studied; study setting; methods employed; outcomes across health, costs/expenditures, and cost-effectiveness; and, stated conclusions and implications of the study. The information extracted was then analyzed for key themes across the domains interest (ie, impact of medical technology on costs or spending and factors influencing this relationship, and the methodological challenges noted in measuring such linkages).
A total of 86 studies were included in the review (Appendix 1). provides a summary of general study details. The majority (52%) of studies were more qualitative in nature (eg, descriptive and policy analyses, literature reviews), followed by cost-effectiveness (40%) and multivariate (24%) analyses. In addition, the bulk of studies were published within the last ten years (77%) and focused on the US (52%). With the exception of cost-effectiveness and cost impact studies examining specific medical devices, most studies (52%) examined medical technology in general, which in some cases included some combination of drugs, devices, diagnostics, or procedures.
Table 2 Characteristics of the reviewed literature
Results
Although technological innovation is of great significance in health careCitation13,Citation14 and has been claimed to be a key driver of health spending, the review highlighted that research measuring the potential contributions of medical technology to rising health care costs has been relatively sparse. One possible reason for this neglect, and the predominant reliance on more descriptive or qualitative analyses among available studies, is that technology itself and its possible implications on health expenditures are insufficiently understood. Other reasons center on the often limited data available to explore this relationship and the complexities of measuring such associations, which we discuss further below.
The available evidence that does exist suggests that, in general, new medical technology is an important determinant in rising health care expenditures. Of the studies reviewed that attempted to quantify this relationship, mainly econometric studies, the overall impact (ie, proportion of the cost increase) ranges from approximately 25% to 75%, averaging at about 50%Citation7,Citation9,Citation10,Citation14–Citation19 ().
Table 3 Contributions of selected factors to growth in health care spending
While much of the quantitative evidence indeed substantiated the cost-increasing effect of new technology overall, the broader spectrum of evidence (eg, cost-effectiveness studies, descriptive analyses) suggests that the relationship between technological advances and health care expenditure is not straightforward or static. Rather, it should be understood as being complex, with a wide range of potential intervening factors that change and shift the dynamic of the association, depending on the particular circumstances.
For example, this relationship often differed across technologies, with some exerting more upward pressure on health care expenditure than others. Of 16 diseases (and subgroups) studied by ScitovskiCitation20 in a case study, new technology decreased costs in eight cases, increased costs in seven, and in one case had neutral effects. The use of “low-tech” technologies such as electrocardiography, laboratory tests, and x-rays stabilized or increased costs at a moderate pace, while the use of complex or sophisticated technologies and procedures such as cesarean section, new treatment modalities for breast cancer, and coronary bypass surgery substantially increased costs. In another case study, Bryan et alCitation21 found that technology that introduces computer-based information networks for imaging archiving increased annual hospital costs by 1.8%. A Congressional Budget OfficeCitation6 review of the available economic literature highlighted particular areas of technology advancement that has been accompanied by more spending, including revascularization for coronary artery disease, diagnostic imaging, and joint replacement.
Whether a particular technology increases or decreases costs depends on whether a given technology: substitutes for an existing service; expands the number of treatable conditions, in that it allows providers to treat conditions they previously could not treat or could not treat effectively or aggressively; intensifies level of use of the technology for the same condition; impacts the delivery of care (eg, improves the capacity of the system to treat more patients); broadens the definition of diseases; and extends life, for which each patient bears (or induces) additional years of health care consumption.Citation6,Citation17,Citation22–Citation25
For instance, with regards to increasing the indications and applications of the innovations, the initial use of imaging diagnostics (eg, x-rays, computed tomography, magnetic resonance) was initially targeted to specific organs and functions, but their application has extended to almost every part of the human body, resulting in increased spending.Citation26 Further, some new technologies may allow lower unit costs (ie, treatment becomes cheaper) or cause less discomfort or complications, thereby offering the potential for cost savings. However, these benefits may lead to increased provision of services to persons who, without the new technology, may not have undergone a particular treatment. Therefore, when the cost savings per case are offset by the increased number of procedures, these technologies will result in increased costs in the aggregate, but will almost certainly also increase the total benefits from the care provided. Chernew et alCitation27 found this was the case with regard to introduction of laparoscopic techniques at the beginning of the 1990s in the US. Of course, new technology can also help extend life (in patients with life-threatening or chronic conditions), which may result in higher spending due to extended years of health care utilization. However, in parallel, a given technology may also allow individuals to live those additional years with greater quality of life or in an improved health state, which could bring potential cost-savings and/or broader social benefits.
In contrast, those technologies that have a substitutive effect, thereby reducing treatment with older technology, eg, use of percutaneous transluminal coronary angioplasty (PTCA) and coronary artery bypass grafting (CABG), may facilitate reductions in spending, even if treatment expansion follows.Citation25,Citation26 For example, PTCA outcomes improved through the introduction of coronary stents, leading to reduced occurrence of restenosis, heart attacks, emergency CABG, and mortality. Consequently, the procedures had become highly substitutable with CABG and for patients with severe coronary artery disease. While the growth of PTCA resulted in higher costs, this has been offset over time by the substitution of PTCA for CABG. Therefore, by metrics of costs, the diffusion of some new technologies can increase spending rapidly at first as it treats those who went without, and less rapidly over time as technology substitutes for more expensive existing treatments.Citation28,Citation29
Moreover, the impact of technology on costs varies depending on the circumstances (eg, patient population, placement in treatment pathway) within which a given therapy is used. For example, several cost-effectiveness analyses on drug-eluting stents have demonstrated that use of these devices increased per patient treatment costs compared with standard balloon angioplasty.Citation30–Citation32 However, if used in medium-risk to high-risk patients, drug-eluting stents could be cost-neutralCitation31,Citation32 or even cost-saving.Citation30
There are also organizational, economic, and social considerations that influence the link between new technology and spending and arguably interplay with the aforementioned factors. For example, impacts on costs may be affected by how the technology is administered or impacts the delivery of care, because some innovations may lead to an increased use of medical personnel, material supplies, or training, particularly if they employ a new technique or procedure, while others may reduce staff or time requirements or shift care to less costly settings of care (eg, inpatient to outpatient).Citation33,Citation34 In particular, some technologies may improve the efficiency of care delivery by reducing procedure time, length of stay, or number of hospitalizations, thereby increasing the capacity of the hospital to treat additional patients. Overall costs may rise as a result, but such outlays will likely result in improved health outcomes for a greater number of patients.
Finally, technological advancements may generate consumer demand for care (and, perhaps more intense, costly services, even if not cost-effective), as well as the demand for insurance.Citation17,Citation27,Citation35,Citation36 At the same time, expanding insurance provides increased incentives to develop new technologies.Citation22 Some analysts maintain that such incentives contribute to long-term growth in expenditure, because the development costs of these products must be recouped by industry (leading to higher prices).Citation6 Although much of this evidence originates from the US, Barros and Martinez-GiraltCitation37 also found that payment systems affect the rate of technology adoption and utilization in European systems. National procurement policies and practices may also influence their diffusion into the health system and the costs associated with adoption. For example, use of more centralized purchasing strategies (eg, local or regional procurement consortiums) or value-based purchasing in Europe and elsewhere, where payment is directly linked to the quality and efficiency of a new technology, may reduce spending.Citation38,Citation39
In relation to this point, there are important differences between countries and their respective health systems that influence the adoption and diffusion of new technologies. For instance, technological change often results from incentives in the health care system. Given that incentive structures differ across countries, technology influences spending differently across jurisdictions.Citation40 Lambooij et alCitation41 assert that lower resourced countries encourage diffusion of innovations that enhance efficiency, whereas better resourced jurisdictions encourage diffusion of complex, expensive technologies.
Discussion
The results of our review suggest that medical technology does have a significant role in health care expenditures, albeit a dynamic and complex one. However, there are limitations to the methodological approaches used in the available published literature, which introduce challenges to arriving at a clear assessment of such dynamics. For example, in terms of quantifying this link, the residual approachCitation4,Citation10,Citation17 can yield a reasonable indirect approximation of how medical technology relates to long-term growth in total health expenditure, but it can be sensitive to assumptions regarding the effects of other related factors (eg, personal income, health insurance coverage, technology development) and the dynamics between them.Citation6,Citation18 This frequently leads to an overestimation of the effect of technology on spending. Another common method, ie, the proxy approach,Citation14,Citation15 is only as good as the proxy indicator used to assimilate the impact of technology on spending. The use of time as a proxy measure for technological change, for example, not only captures such changes, but may also encapsulate variations in policy, patient experiences, preference, and expenditures.Citation15
Another method, ie, the case study approach,Citation25,Citation26 is useful to explain the impact of certain medical technologies on health care costs, but there are problems of sampling and it is difficult to generalize to an aggregate or national level.Citation6,Citation19 Consequently, most analysts using this approach have focused on the most significant conditions (eg, prevalent, contributing to high levels of mortality or disability), such as heart disease. These technical issues also characterize cost-effectiveness and cost impact analyses.Citation42–Citation45
In addition to the limitations noted with individual approaches, there are technical issues shared across the various methods. Firstly, the results are frequently based on aggregate level data that are often subject to potential endogeneity and omit variable bias.Citation46 Secondly, as intimated above, several of these methods can depend on relatively simplified models dealing with highly complicated and interrelated parametersCitation16 and can only arrive at conclusions about the collective effect of technology on health care spending, not on the contributions of specific technologies. Different types of technologies (eg, drugs versus medical devices) arguably impact health spending differently, particularly in terms of the associated changes in clinical practice that follow their adoption. For example, a recent studyCitation47 estimated that medical devices account for a relatively small share of national health expenditures (3%–5%), which have risen only slightly over the last 20 years, ie, a trend different from that of pharmaceuticals. Thirdly, across both quantitative and qualitative approaches, capturing the economic (and social) complexities surrounding the use of technology can be challenging, because it generally necessitates a complete understanding of the manner and magnitude of change in the clinical management pathway associated with treatment and follow-up. This process can occur over extended periods of time, and can have varying resource costs that can be both easy and difficult to measure.Citation48
Available studies are often focused on a narrow time window and the specific duration of the life cycle for a technology. Therefore, results from studies with longer or different time periods could vary. For instance, the price of medical technologies generally decreases over time, which would not be captured in shorter-term studies or those that happen to examine a given technology(s) close to initial launch. similarly, technological advances occur simultaneously with changes in other factors that affect health care spending, such as personal income and health financing systems, which make it difficult to identify causality reliably, and exactly how technology itself affects spending growth. Finally, current methods cannot effectively demonstrate the cost impact that would result if availability of technology were reduced or eliminated. In the short-term, cost-savings may be achieved, while limited access to technology may result in higher costs in the long term due to the presence of disease that was not adequately treated owing to reliance on older, less-effective technologies or a complete lack of viable treatment alternatives.
Therefore, while examining the role of medical technology in rising health expenditures is indeed an important area of inquiry, it is largely an incomplete exercise, due to some of the noted methodological issues, and also because most new technological innovations are cost-increasing. Even if a given technology increases costs, it may increase benefits by an even greater amount. In addition, the same technology, applied in different settings, or in different groups of patients, could be cost-effective in some instances and not in others. Consequently, alongside simply examining costs, it is perhaps more productive to assess whether the additional benefits resulting from the use of the technology justify any increase in costs and under which circumstances technologies deliver greater value in health care. That is, are the resulting spending levels reflected in more effective, cost-effective, and higher quality health care?
Several studies from the review indicate that, on average, increases in spending as a result of technological advances have provided reasonable value. For example, Cutler et alCitation49 found that from 1960 to 2000, average life expectancy increased by 7 years, 3.5 years of which were attributable to improvements in health care. Comparing the value of a year of life (anywhere from $50,000 to $200,000) with the finding that each year of increased life expectancy cost about $19,900 in health spending, they conclude that the increased spending, on average, had been a worthwhile investment. similar conclusions were arrived at by Cutler and McClellanCitation25 and Skinner et alCitation50 in examining technological innovation in cardiac care. The former, for example, demonstrated that the use of new technology helped to increase the average coronary patient’s life expectancy by one year (valued at $70,000 per case), while treatment costs increased $10,000 per case (4.2% per year), for a net benefit of $60,000 per case. In addition, as previously discussed, cost-effectiveness analyses of particular medical devices demonstrate value for money (as measured by cost per quality-adjusted life year) and in some limited cases, cost savings.Citation30,Citation31,Citation42,Citation51–Citation53 On a broader level, Fuchs and SoxCitation54 surveyed physician perceptions of the importance of and value brought by various areas of technological innovation, with magnetic resonance imaging and computed tomographic scanning, angiotensin-converting enzyme inhibitors, balloon angioplasty, statins, and mammography all rated highly.
Before concluding, it is important to note a few limitations to this study. Firstly, while we strove to select and review only studies focused on medical technology, some studies, particularly certain types of econometric studies, looked at technology collectively. Therefore, for those studies, we were unable to distinguish the relative contribution of different types of technology (eg, drugs versus devices) to the proportion of spending attributed to technological innovation. Secondly, we focused our review of cost-effectiveness studies only on selected cardiology and orthopedic devices. Nevertheless, these particular sectors are arguably important markets and those most likely to have a cost impact.
Conclusion
Major technological advances in medical science have allowed health care providers to diagnose and treat illnesses in ways that were previously impossible. In general, such developments have tended to increase health care spending, which has been seen as an important policy concern, especially considering ever-limited health care budgets.
However, examining the link between medical technology and health expenditures is only one part of the picture. In order to understand better the dynamics between innovation and spending, it is important to assess whether and under what circumstances do investments in medical technology result in better value in health care. As Cutler and McClellanCitation25 assert, “it does not necessarily follow that technology change is therefore bad … costs of technology need to be compared with benefits before welfare statements can be made”. Given the current global economic situation, it is ever more important to ensure that we are attaining good value for money from the technologies developed.
To be sure, the question of whether medical technologies result in added value to the health care system is, of course, also difficult to answer. It depends on our ability to determine the value of output from the health services sector, and placing a value on longer or better quality of life is difficult to appraise. As a starting point, much more comparative research is needed to understand better which technologies work best and are most cost-effective, and under what circumstances. Indeed, as previously discussed, some of the cost-increasing effects of technology arise from inappropriate use, where new treatments are offered to patients for whom there is none to little clinical benefit. Current efforts to support comparative effectiveness research in the US and health technology assessment in Europe and elsewhere may help to foster these aims. However, it is important to note that medical technologies introduce unique technical challenges to health technology assessment or comparative effectiveness research, so assessment methods should adequately account for or be developed to accommodate such aspects.Citation55 Moreover, in addressing questions of value, such research should strive, where possible, to assess a broad range of potential benefits beyond clinical or therapeutic benefit, including value for money, higher quality of care, improved quality of life, greater efficiency in care delivery (eg, reduced length of stay, shifting care from inpatient to outpatient settings), and enhanced ability to work or return to work.
If the evidence generated from such research is to have an impact on health care spending, it should be used to inform policy and practice. As such, comparative effectiveness research and health technology assessment should be used to help reward and support the introduction of technologies into practice that confer therapeutic benefit and reasonable value for money, either through use in coverage and payment policies, insurance benefit design, or practice guidelines. Conversely, use of low-value interventions should be disincentivized through disinvestment or limitation on their use. Such strategies should be coupled with a greater emphasis on evidence-based delivery of care (eg, aligning appropriate financial incentives for providers and consumers), which might further reduce expenditure levels if such incentives support greater use of cost-effective services.Citation6 However, in parallel, it will be important to monitor carefully the impact of such policy levers in order to ascertain the best way to control costs without denying the benefits of new innovation. In addition, such measures need to be coupled with other policies and practices to address some of the other drivers of health spending, including initiatives to support healthy aging and improve coordination of care for the chronically ill. Finally, given our ever-limited health care resources, it would be prudent to debate the opportunity costs of funding new (and increasingly expensive) technologies. Even in cases where medical technologies are cost-effective, available resources may be better allocated to other equally or more cost-effective investments outside of the health care sector, such as the environment or education.
Disclosure
The authors report no conflicts of interest in this work.
References
- Organisation for Economic Co-operation and DevelopmentOECD Health Data 2011Paris, FranceOrganisation for Economic Co-operation and Development2011 Available from http://www.oecd.org/health/health-systems/healthataglance2011.htm.
- LubitzJDRileyGFTrends in Medicare payments in the last year of lifeN Engl J Med1993328109210968455667
- Organisation for Economic Co-operation and DevelopmentOECD Health at a Glance: Europe 2010Paris, FranceOrganisation for Economic Co-operation and Development2010
- Organisation for Economic Co-operation and Development Projecting OECD Health and Long Term Care Expenditures: What are the Main Drivers? Organisation for Economic Co-operation and Development Economic Department Working Paper, No 477; 2006. Available from: http://www.oecd.org/tax/public-finance/36085940.pdf. Accessed March 15, 2013.
- Centers for Disease Control and PreventionHealth, United States, 2009 with Special Feature on Medical TechnologyUS Department of Health and Human ServicesHyattsville, MD2009 Available from: http://www.cdc.gov/nchs/data/hus/hus09.pdf. Accessed March 15, 2013.
- Congressional Budget OfficeTechnological Change and The Growth of Health Care Spending. Congressional Budget OfficeWashington, DCCongressional Budget Office2008
- PricewaterhouseCoopersThe Factors Fueling Risking Healthcare Costs Report prepared for the American Association of Health Plans2002 Available from: http://heartland.org/sites/all/modules/custom/heartland_migration/files/pdfs/14621.pdf. Accessed March 15, 2013.
- FuchsVREconomics, values, and health care reformAm Econ Rev199686112410168326
- CutlerDMTechnology, Health Costs, and the NIH, Harvard University and the National Bureau of Economic ResearchPaper prepared for the National Institutes of Health Economics Roundtable on Biomedical ResearchSeptember 1995
- NewhouseJMedical care costs: How much welfare loss?J Econ Perspect1992632110128078
- SorensonCDrummondMThe socio-economic value of orthopaedic devices: Evidence and methodological challengesOrthopedic Research and Reviews201248796
- Centre for Review and DisseminationAbstractors Guide for NHS EEDYork, UKCentre for Review and Dissemination2009 Available from: http://ospguides.ovid.com/OSPguides/cleeddb.htm.
- BerndtERCutlerDMFrankRGGrilichesZNewhouseJPTriplettJEMedical care prices and outputCulyerAJNewhouseJPHandbook of Health Economics, Volume 1AAmsterdam, The NetherlandsElsevier2000
- OkunadeAAMurthyVNRTechnology as a major driver of health care costs: a cointegration analysis of the Newhouse conjectureJ Health Econ20022114715911852912
- Di MatteoLThe macro determinants of health expenditure in the United States and Canada: assessing the impact of income, age distribution and timeHealth Policy200571234215563991
- JonesCIWhy have Health Expenditures as a Share of GDP Risen So Much? National Bureau of Economic Research Working Paper Series, No 93252002 Available from: http://ideas.repec.org/p/nbr/nberwo/9325.html. Accessed March 15, 2013.
- PedenEAFreelandMSA historical analysis of medical spending growth, 1960–1993Health Affairs1995142352477657244
- DybczakKPrzywaraBThe Role of Technology on Health Care Expenditure on the EU European Economy – Economic Paper 400Brussels, BelgiumDirectorate General for Economic and Monetary Affairs, European Commission2010 Available from: http://ec.europa.eu/economy_finance/publications/economic_paper/2010/ecp400_en.htm.
- SmithSDHefflerSKFreelandMSThe Impact of Technological Change on Health Care Cost Increases: An Evaluation of the Literature Health Care Financing Administration Working Paper2000 Available from: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/downloads/tech_2000_0810.pdf.
- ScitovskiAAChanges in the cost of treatment of selected illnesses, 1971–1981Med Care198523134513574087950
- BryanSBuxtonMBrennaEEstimating the impact of a diffuse technology on the running costs of a hospitalInt J Technol Assess200016787798
- WeisbrodBAThe health care quadrilemma: an essay on technological change, insurance, quality of care and cost containmentJ Econ Lit199129523532
- RettigRAMedical innovation duels cost containmentHealth Aff (Millwood)1994137277927162
- FuchsVRHealth care for the elderly: how much? Who will pay for it?Health Aff (Millwood)19991811219926642
- CutlerDMMcClellanMIs technological change in medicine worth it?Health Aff (Millwood)2001201129
- BakerLCManaged care and technology adoption in health care: evidence from magnetic resonance imagingJ Health Econ20012039542111373838
- ChernewMFendrickAMHirthRAManaged care and medical technology: implications for cost growthHealth Aff (Millwood)1997161962069086669
- CutlerDMHuckmanRSTechnological development and medical productivity: the diffusion of angioplasty in New York stateJ Health Econ20032218721712606143
- MartinSRiceNSmithPCDoes health care spending improve health outcomes? Evidence from English programme budgeting dataJ Health Econ20082782684218261812
- GreenbergDRosenfieldKGarciaLAIn-hospital costs of self-expanding nitinol stent implantation vs. balloon angioplasty in the femoropopliteal artery (The VascuCoil Trial)J Vasc Interv Radiol2004151065106915466792
- Von HoutBASerruysPWLemosPAOne-year cost-effectiveness of sirolimus eluting stents compared with bare metal stents in the treatment of single native de novo coronary lesions: an analysis from the Ravel trialHeart20059150751215772214
- BagustAGraysonADPalmerNDPerryRAWalleyTCost-effectiveness of drug eluting coronary artery stenting in a UK setting: cost-utility studyHeart200692687415831599
- BlankJVogelaarISpecifying technical change: a research on the nature of technical change in Dutch hospital industryQ Rev Econ Finance200444448463
- BradleyTBKominskiGFContributions of case mix and intensity change to hospital cost increasesHealth Care Financ Rev19921415116310127449
- MasNSeinfeldJIs managed care restraining the adoption of technology by hospitals?J Health Econ2008271026104518417230
- CutlerDMMcClellanMThe determinants of technological change in heart attack treatment NBER Working Paper No 57511996 Available from: http://ideas.repec.org/p/nbr/nberwo/5751.html. Accessed March 17, 2013.
- BarrosPMartinez-GiraltXTechnological Adoption in Health Care CEPR Discussion Papers 75582009 Available from: http://ideas.repec.org/p/unl/unlfep/wp545.html. Accessed March 17, 2013.
- SorensonCKanavosPMedical technology procurement in Europe: a cross-country comparison of current practice and policyHealth Policy2011100435020846739
- ObremskeyWTDailTJahangirAAValue-based purchasing of medical devicesClin Orthop Relat Res20124701054106422033872
- CutlerDMThe lifetime costs and benefits of medical technologyJ Health Econ2007261081110018023900
- LambooijMSEngelfrietPWestertGPDiffusion of innovations in health care: does the structural context determine its direction?Int J Technol Assess201026415420
- MarchLMBarcinillaALCrossMJCosts and outcomes of total hip and knee joint replacement for rheumatoid arthritisClin Rheumatol2008271235124218500442
- MarinelliMSoccettiAPanfoliNde PalmaLCost-effectiveness of cemented versus cementless total hip anthroplasty. A Markov decision analysis based on implant costJ Orthop Traumatol20089232819384477
- BanzKCardiac resynchronization therapy (CRT) in heart failure: a model to assess the economic value of this new medical technologyValue Health2005812813915804321
- Brunner-La RoccaHPKaiserCBernheimACost-effectiveness of drug-eluting stents in patients at high or low risk of major cardiac events in the Basel Stent KostenEff Ektivitäts Trial (BASKET): an 18-month analysisLancet2007370155159
- HayJWHospital cost drivers: an evaluation of 1998–2001 state-level dataAm J Manag Care20039SP13SP2412817612
- DonavanGDKingGEstimates of Medical Device Spending in the United StatesAdvanced Medical Technology Association2011 Available from: www.amsa.org/.../king_paper_medical_device_spending.sflb.ashx
- LuceBRElixhauserAEstimating costs in the economic evaluation of medical technologiesInt J Technol Assess199065775
- CutlerDMRosenABVijanSThe value of medical spending in the United States, 1960–2000N Engl J Med200635592092716943404
- SkinnerJStaigerDTechnology Diffusion and Productivity Growth in Health Care National Bureau of Economic Research Working Paper Series, No 148652009 Available from: http://www.dartmouth.edu/~jskinner/documents/SkinnerStaigerw14865_000.pdf. Accessed March 17, 2013.
- BozicKJMorshedSSilversteinMDRubashHEKahnJGUse of cost-effectiveness analysis to evaluate new technologies in orthopaedics: the case of alternative bearing surfaces in total hip arthroplastyJ Bone Joint Surg Am20068870671416595459
- SinghSSunHAnisAHCost-effectiveness of hip protectors in the prevention of osteoporosis related hip fractures in elderly nursing home residentsJ Rheumatol2004311607161315290742
- Segui-GomezMKeuffelEFrickKDCost and effectiveness of hip protectors among the elderlyInt J Technol Assess2002185566
- FuchsVRSoxHCPhysicians’ views of the relative importance of thirty medical innovationsHealth Aff (Millwood)200120304211558715
- SorensonCTarriconeRSiebertMDrummondMApplying health economics for policy decision making: how much do devices differ from drugs?Europace201113Suppl 2ii54ii5821518751
Appendix 1
Studies reviewed
- AidelsburgerPGrabeinKKlaussVWasemJCost-effectiveness of cardiac resynchronization therapy in combination with an implantable cardioverter defibrillator (CRT-D) for the treatment of chronic heart failure from a German health care system perspectiveClin Res Cardiol200297899717955159 <!--${if: isGetFTREnabled}-->
- BakerLSpetzJManaged Care and Medical Technology Growth National Bureau of Economic Research Working Paper Series, No 68941999 Available from: http://www.nber.org/chapters/c9845.pdf. Accessed March 17, 2013. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 journal Managed+Care+and+Medical+Technology+Growth author%3DL+Baker%26author%3DJ+Spetz 1999 BakerLSpetzJManaged+Care+and+Medical+Technology+GrowthNational+Bureau+of+Economic+Research+Working+Paper+Series%2C+No+68941999Available+from%3A+.+Accessed+March+17%2C+2013. %00empty%00 %00empty%00 %00empty%00 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_2_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DBaker%26rft.aufirst%3DL%26rft.atitle%3DManaged%2520Care%2520and%2520Medical%2520Technology%2520Growth%26rft.date%3D1999 %00empty%00}-->
- BakerLCManaged care and technology adoption in health care: evidence from magnetic resonance imagingJ Health Econ20012039542111373838 <!--${if: isGetFTREnabled}-->
- BakerLBirnbaumHGeppertJMisholDMoyneurEThe relationship between technology availability and health care spendingHealth Aff (Millwood)2003Suppl Web ExclusivesW3-5375115506158 <!--${if: isGetFTREnabled}-->
- BakhaiAStoneGWGrinesCLCost-effectiveness of coronary stenting and abciximab for patients with acute myocardial infarction: results from the CADILLAC (Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications) TrialCirculation20031082857286314610016 <!--${if: isGetFTREnabled}-->
- BanzKCardiac resynchronization therapy (CRT) in heart failure: a model to assess the economic value of this new medical technologyValue Health2005812813915804321 <!--${if: isGetFTREnabled}-->
- BagustAGraysonADPalmerNDPerryRAWalleyTCost-effectiveness of drug eluting coronary artery stenting in a UK setting: cost-utility studyHeart200692687415831599 <!--${if: isGetFTREnabled}-->
- BarrosPMartinez-GiraltXTechnological Adoption in Health Care CEPR Discussion Papers 7558, CEPR. Discussion Papers; 2009. Available from: http://ideas.repec.org/p/unl/unlfep/wp545.html. Accessed March 17, 2013. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 web Technological+Adoption+in+Health+Care author%3DP+Barros%26author%3DX+Martinez-Giralt %00null%00 BarrosPMartinez-GiraltXTechnological+Adoption+in+Health+CareCEPR+Discussion+Papers+7558%2C+CEPR.+Discussion+Papers%3B+2009.+Available+from%3A+.+Accessed+March+17%2C+2013. %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_8_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Dweb%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DBarros%26rft.aufirst%3DP%26rft.atitle%3DTechnological%2520Adoption%2520in%2520Health%2520Care %00empty%00}-->
- BentkoverJDStewertEJIgnaszewskiALepageSLiuPCooperJNew technologies and potential cost savings related to morbidity and mortality reduction in Class III/IV heart failure patients in CanadaInt J Cardiol200388334112659982 <!--${if: isGetFTREnabled}-->
- BodenheimerTHigh and rising health care costs. Part 2: technologic innovationAnn Intern Med200514293293715941701 <!--${if: isGetFTREnabled}-->
- BozicKJMorshedSSilversteinMDRubashHEKahnJGUse of cost-effectiveness analysis to evaluate new technologies in orthopaedics: the case of alternative bearing surfaces in total hip arthroplastyJ Bone Joint Surg Am20068870671416595459 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Use+of+cost-effectiveness+analysis+to+evaluate+new+technologies+in+orthopaedics%3A+the+case+of+alternative+bearing+surfaces+in+total+hip+arthroplasty author%3DKJ+Bozic%26author%3DS+Morshed%26author%3DMD+Silverstein%26author%3DHE+Rubash%26author%3DJG+Kahn 2006 BozicKJMorshedSSilversteinMDRubashHEKahnJGUse+of+cost-effectiveness+analysis+to+evaluate+new+technologies+in+orthopaedics%3A+the+case+of+alternative+bearing+surfaces+in+total+hip+arthroplastyJ+Bone+Joint+Surg+Am20068870671416595459 706-714 J+Bone+Joint+Surg+Am 88 %00null%00 %00empty%00 16595459 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_11_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DBozic%26rft.aufirst%3DKJ%26rft.atitle%3DUse%2520of%2520cost-effectiveness%2520analysis%2520to%2520evaluate%2520new%2520technologies%2520in%2520orthopaedics%253A%2520the%2520case%2520of%2520alternative%2520bearing%2520surfaces%2520in%2520total%2520hip%2520arthroplasty%26rft.jtitle%3DJ%2520Bone%2520Joint%2520Surg%2520Am%26rft.date%3D2006%26rft.volume%3D88%26rft.spage%3D706%26rft.epage%3D714%26rft_id%3Dinfo%3Apmid%2F16595459 %00empty%00}-->
- Brunner-La RoccaHPKaiserCBerheimACost-effectiveness of drug-eluting stents in patients at high or low risk of major cardiac events in the Basel Stent KostenEffektivitäts Trial (BASKET): an 18-month analysisLancet2007370155159 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Cost-effectiveness+of+drug-eluting+stents+in+patients+at+high+or+low+risk+of+major+cardiac+events+in+the+Basel+Stent+KostenEffektivit%C3%A4ts+Trial+%28BASKET%29%3A+an+18-month+analysis author%3DHP+Brunner-La+Rocca%26author%3DC+Kaiser%26author%3DA+Berheim 2007 Brunner-La+RoccaHPKaiserCBerheimACost-effectiveness+of+drug-eluting+stents+in+patients+at+high+or+low+risk+of+major+cardiac+events+in+the+Basel+Stent+KostenEffektivit%C3%A4ts+Trial+%28BASKET%29%3A+an+18-month+analysisLancet2007370155159 155-159 Lancet 370 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_12_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DBrunner-La%2520Rocca%26rft.aufirst%3DHP%26rft.atitle%3DCost-effectiveness%2520of%2520drug-eluting%2520stents%2520in%2520patients%2520at%2520high%2520or%2520low%2520risk%2520of%2520major%2520cardiac%2520events%2520in%2520the%2520Basel%2520Stent%2520KostenEffektivit%25C3%25A4ts%2520Trial%2520%2528BASKET%2529%253A%2520an%252018-month%2520analysis%26rft.jtitle%3DLancet%26rft.date%3D2007%26rft.volume%3D370%26rft.spage%3D155%26rft.epage%3D159 %00empty%00}-->
- BryanSBuxtonMBrennaEEstimating the impact of a diffuse technology on the running costs of a hospitalInt J Technol Assess200016787798 <!--${if: isGetFTREnabled}-->
- BusseRExpenditure on health care in the EU: making projections for the future based on the pastEur J Health Econ20012158161 <!--${if: isGetFTREnabled}-->
- CalvertMJFreemantleNYaoGCost-effectiveness of cardiac resynchronization therapy: results from the CARE-HF trialEur Heart J2005262681268816284203 <!--${if: isGetFTREnabled}-->
- CaroJWardAMollerJModelling the health benefits and economic implications of implanting dual-chamber vs single-chamber ventricular pacemakers in the UKEuropace2006844945516690630 <!--${if: isGetFTREnabled}-->
- ChenLHayJWCost-effectiveness of primary implanted cardioverter defibrillator for sudden death prevention in congestive heart failureCardiovasc Drugs Ther20041816117015162078 <!--${if: isGetFTREnabled}-->
- ChernewMHirthRASonnadSSErmannRFenrickAMManaged care, medical technology, and health care cost growth: A review of the evidenceMed Care Res Rev1998552592889727299 <!--${if: isGetFTREnabled}-->
- ChernewMFenrickAMHirthRAManaged care and medical technology: implications for cost growthHealth Aff (Millwood)1997161962069086669 <!--${if: isGetFTREnabled}-->
- ClementeJMarcuelloCMontanesAPueyoFOn the international stability of health care expenditure functions: are government and private functions similar?J Health Econ20042358961315120472 <!--${if: isGetFTREnabled}-->
- CohenDJMurphySABaimDSCost-effectiveness of distal embolic protection for patients undergoing percutaneous intervention of saphenous vein bypass graft (results from the SAFER trial)J Am Coll Cardiol2004441801180815519010 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Cost-effectiveness+of+distal+embolic+protection+for+patients+undergoing+percutaneous+intervention+of+saphenous+vein+bypass+graft+%28results+from+the+SAFER+trial%29 author%3DDJ+Cohen%26author%3DSA+Murphy%26author%3DDS+Baim 2004 CohenDJMurphySABaimDSCost-effectiveness+of+distal+embolic+protection+for+patients+undergoing+percutaneous+intervention+of+saphenous+vein+bypass+graft+%28results+from+the+SAFER+trial%29J+Am+Coll+Cardiol2004441801180815519010 1801-1808 J+Am+Coll+Cardiol 44 %00null%00 %00empty%00 15519010 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_21_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DCohen%26rft.aufirst%3DDJ%26rft.atitle%3DCost-effectiveness%2520of%2520distal%2520embolic%2520protection%2520for%2520patients%2520undergoing%2520percutaneous%2520intervention%2520of%2520saphenous%2520vein%2520bypass%2520graft%2520%2528results%2520from%2520the%2520SAFER%2520trial%2529%26rft.jtitle%3DJ%2520Am%2520Coll%2520Cardiol%26rft.date%3D2004%26rft.volume%3D44%26rft.spage%3D1801%26rft.epage%3D1808%26rft_id%3Dinfo%3Apmid%2F15519010 %00empty%00}-->
- CowieMRMarshallDDrummondMLifetime cost-effectiveness of prophylactic implantation of a cardioverter defibrillator in patients with reduced left ventricular systolic function: results of Markov modelling in a European populationEuropace20091171672619359333 <!--${if: isGetFTREnabled}-->
- CutlerDMHuckmanRSTechnological development and medical productivity: the diffusion of angioplasty in New York stateJ Health Econ20032218721712606143 <!--${if: isGetFTREnabled}-->
- CutlerDMMcClellanMIs technological change in medicine worth it?Health Aff (Millwood)2001201129 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Is+technological+change+in+medicine+worth+it%3F author%3DDM+Cutler%26author%3DM+McClellan 2001 CutlerDMMcClellanMIs+technological+change+in+medicine+worth+it%3FHealth+Aff+%28Millwood%292001201129 11-29 Health+Aff+%28Millwood%29 20 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_24_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DCutler%26rft.aufirst%3DDM%26rft.atitle%3DIs%2520technological%2520change%2520in%2520medicine%2520worth%2520it%253F%26rft.jtitle%3DHealth%2520Aff%2520%2528Millwood%2529%26rft.date%3D2001%26rft.volume%3D20%26rft.spage%3D11%26rft.epage%3D29 %00empty%00}-->
- CutlerDMMcClellanMThe Determinants of Technological Change in Heart Attack Treatment NBER Working Paper No 5751; 1996. Available from: http://ideas.repec.org/p/nbr/nberwo/5751.html. Accessed March 17, 2013. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 web The+Determinants+of+Technological+Change+in+Heart+Attack+Treatment author%3DDM+Cutler%26author%3DM+McClellan %00null%00 CutlerDMMcClellanMThe+Determinants+of+Technological+Change+in+Heart+Attack+TreatmentNBER+Working+Paper+No+5751%3B+1996.+Available+from%3A+.+Accessed+March+17%2C+2013. %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_25_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Dweb%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DCutler%26rft.aufirst%3DDM%26rft.atitle%3DThe%2520Determinants%2520of%2520Technological%2520Change%2520in%2520Heart%2520Attack%2520Treatment %00empty%00}-->
- CutlerDMThe lifetime costs and benefits of medical technologyJ Health Econ2007261081110018023900 <!--${if: isGetFTREnabled}-->
- CutlerDMTechnology, Health Costs, and the NIH, Harvard University and the National Bureau of Economic ResearchPaper prepared for the National Institutes of Health Economics Roundtable on Biomedical ResearchSeptember 1995 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 confproc Technology%2C+Health+Costs%2C+and+the+NIH%2C+Harvard+University+and+the+National+Bureau+of+Economic+Research author%3DDM+Cutler %00null%00 CutlerDMTechnology%2C+Health+Costs%2C+and+the+NIH%2C+Harvard+University+and+the+National+Bureau+of+Economic+ResearchPaper+prepared+for+the+National+Institutes+of+Health+Economics+Roundtable+on+Biomedical+ResearchSeptember+1995 %00empty%00 Paper+prepared+for+the+National+Institutes+of+Health+Economics+Roundtable+on+Biomedical+Research %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_27_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Dproceeding%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DCutler%26rft.aufirst%3DDM%26rft.atitle%3DTechnology%252C%2520Health%2520Costs%252C%2520and%2520the%2520NIH%252C%2520Harvard%2520University%2520and%2520the%2520National%2520Bureau%2520of%2520Economic%2520Research %00empty%00}-->
- Di MatteoLWhat drives provincial health expenditure?Canadian Tax Journal2004521102 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 journal What+drives+provincial+health+expenditure%3F author%3DL+Di+Matteo 2004 Di+MatteoLWhat+drives+provincial+health+expenditure%3FCanadian+Tax+Journal2004521102 1102 Canadian+Tax+Journal 52 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_28_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DDi%2520Matteo%26rft.aufirst%3DL%26rft.atitle%3DWhat%2520drives%2520provincial%2520health%2520expenditure%253F%26rft.jtitle%3DCanadian%2520Tax%2520Journal%26rft.date%3D2004%26rft.volume%3D52%26rft.spage%3D1102 %00empty%00}-->
- Di MatteoLThe macro determinants of health expenditure in the United States and Canada: assessing the impact of income, age distribution and timeHealth Policy200571234215563991 <!--${if: isGetFTREnabled}-->
- DybczakKPrzywaraBThe Role of Technology on Health Care Expenditure on the EU European Economy – Economic Paper 400Brussels, BelgiumDirectorate General for Economic and Monetary Affairs, European Commission2010 Available from: http://ec.europa.eu/economy_finance/publications/economic_paper/2010/ecp400_en.htm. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 book The+Role+of+Technology+on+Health+Care+Expenditure+on+the+EU+European+Economy+%E2%80%93+Economic+Paper+400 author%3DK+Dybczak%26author%3DB+Przywara 2010 DybczakKPrzywaraBThe+Role+of+Technology+on+Health+Care+Expenditure+on+the+EU+European+Economy+%E2%80%93+Economic+Paper+400Brussels%2C+BelgiumDirectorate+General+for+Economic+and+Monetary+Affairs%2C+European+Commission2010Available+from%3A+. %00empty%00 %00null%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_30_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Dbook%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DDybczak%26rft.aufirst%3DK%26rft.btitle%3DThe%2520Role%2520of%2520Technology%2520on%2520Health%2520Care%2520Expenditure%2520on%2520the%2520EU%2520European%2520Economy%2520%25E2%2580%2593%2520Economic%2520Paper%2520400%26rft.pub%3DDirectorate%2520General%2520for%2520Economic%2520and%2520Monetary%2520Affairs%252C%2520European%2520Commission%26rft.date%3D2010 %00empty%00}-->
- EkmanMSjogrenIJamesSCost-effectiveness of the Taxus paclitaxel-eluting stent in the Swedish healthcare systemScand Cardiovasc J200640172416448993 <!--${if: isGetFTREnabled}-->
- FilionKBRoyAMBaboushkinETRinfretSEisenbergMJCost-effectiveness of drug-eluting stents including the economic impact of late stent thrombosisAm J Cardiol200610333834419166686 <!--${if: isGetFTREnabled}-->
- FuchsVRHealth care for the elderly: how much? Who will pay for it?Health Aff (Millwood)19991811219926642 <!--${if: isGetFTREnabled}-->
- FuchsVRSoxHRPhysicians’ views of the relative importance of thirty medical innovationsHealth Aff (Millwood)200120304211558715 <!--${if: isGetFTREnabled}-->
- GandjourAWeylanEJCost-effectiveness of preventing fractures by hip protectors in elderly institutionalized patients in GermanyValue Health2008111088109519602215 <!--${if: isGetFTREnabled}-->
- GivonUGinsbergGMHoroszowskiHShemerJCost-utility analysis of total hip anthroplasties. Technology assessment of surgical procedures by mailed questionnairesInt J Technol Assess199814735742 <!--${if: isGetFTREnabled}-->
- GoetghebeurMMForrestSHayJWUnderstanding the underlying drivers of inpatient cost growth: a literature reviewAm J Manag Care20039Spec No 1SP3SP1212817611 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Understanding+the+underlying+drivers+of+inpatient+cost+growth%3A+a+literature+review author%3DMM+Goetghebeur%26author%3DS+Forrest%26author%3DJW+Hay 2003 GoetghebeurMMForrestSHayJWUnderstanding+the+underlying+drivers+of+inpatient+cost+growth%3A+a+literature+reviewAm+J+Manag+Care20039Spec+No+1SP3SP1212817611 SP3-SP12 Am+J+Manag+Care 9 Spec+No+1 %00empty%00 12817611 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_37_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DGoetghebeur%26rft.aufirst%3DMM%26rft.atitle%3DUnderstanding%2520the%2520underlying%2520drivers%2520of%2520inpatient%2520cost%2520growth%253A%2520a%2520literature%2520review%26rft.jtitle%3DAm%2520J%2520Manag%2520Care%26rft.date%3D2003%26rft.volume%3D9%26rft.issue%3DSpec%2520No%25201%26rft.spage%3DSP3%26rft.epage%3DSP12%26rft_id%3Dinfo%3Apmid%2F12817611 %00empty%00}-->
- GoyenMDebatinJHealthcare costs for new technologiesEur J Nucl Med Mol Imaging200936139143 <!--${if: isGetFTREnabled}-->
- GreenbergDRosenfieldKGarciaLAIn-hospital costs of self-expanding Nitinol Stent Implantation vs. Balloon Angioplasty in the Femoropopliteal Artery (The VascuCoil Trial)J Vasc Interv Radiol2004151065106915466792 <!--${if: isGetFTREnabled}-->
- GrignonMAging, Health and Aggregate Medical Care Spending in France Department of Economics Working Papers 2005–05McMaster University2005 Available from: http://www.econbiz.de/en/search/detailed-view/doc/all/Aging,%20Health%20and%20Aggregate%20Medical%20Care%20Spending%20in%20France/10005635244/?no_cache=1. Accessed March 17, 2013. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 book %00empty%00 author%3DM+Grignon 2005 GrignonMAging%2C+Health+and+Aggregate+Medical+Care+Spending+in+FranceDepartment+of+Economics+Working+Papers+2005%E2%80%9305McMaster+University2005Available+from%3A+.+Accessed+March+17%2C+2013. %00empty%00 %00null%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_40_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Dbook%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DGrignon%26rft.aufirst%3DM%26rft.atitle%3DAging%252C%2520Health%2520and%2520Aggregate%2520Medical%2520Care%2520Spending%2520in%2520France%26rft.pub%3DMcMaster%2520University%26rft.date%3D2005 %00empty%00}-->
- HallREJonesCIThe Value of Life and the Rise in Health Spending National Bureau of Economic Research Working Paper Series, No 107372004 Available from: http://qje.oxfordjournals.org/content/122/1/39.short. Accessed March 17, 2013. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 journal The+Value+of+Life+and+the+Rise+in+Health+Spending author%3DRE+Hall%26author%3DCI+Jones 2004 HallREJonesCIThe+Value+of+Life+and+the+Rise+in+Health+SpendingNational+Bureau+of+Economic+Research+Working+Paper+Series%2C+No+107372004Available+from%3A+.+Accessed+March+17%2C+2013. %00empty%00 %00empty%00 %00empty%00 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_41_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DHall%26rft.aufirst%3DRE%26rft.atitle%3DThe%2520Value%2520of%2520Life%2520and%2520the%2520Rise%2520in%2520Health%2520Spending%26rft.date%3D2004 %00empty%00}-->
- HayJWHospital cost drivers: an evaluation of 1998–2001 state-level dataAm J Manag Care20039SP13SP2412817612 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Hospital+cost+drivers%3A+an+evaluation+of+1998%E2%80%932001+state-level+data author%3DJW+Hay 2003 HayJWHospital+cost+drivers%3A+an+evaluation+of+1998%E2%80%932001+state-level+dataAm+J+Manag+Care20039SP13SP2412817612 SP13-SP24 Am+J+Manag+Care 9 %00null%00 %00empty%00 12817612 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_42_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DHay%26rft.aufirst%3DJW%26rft.atitle%3DHospital%2520cost%2520drivers%253A%2520an%2520evaluation%2520of%25201998%25E2%2580%25932001%2520state-level%2520data%26rft.jtitle%3DAm%2520J%2520Manag%2520Care%26rft.date%3D2003%26rft.volume%3D9%26rft.spage%3DSP13%26rft.epage%3DSP24%26rft_id%3Dinfo%3Apmid%2F12817612 %00empty%00}-->
- HillmanBJGovernment health policy and the diffusion of new medical devicesHealth Serv Res1986216817113818311 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Government+health+policy+and+the+diffusion+of+new+medical+devices author%3DBJ+Hillman 1986 HillmanBJGovernment+health+policy+and+the+diffusion+of+new+medical+devicesHealth+Serv+Res1986216817113818311 681-711 Health+Serv+Res 21 %00null%00 %00empty%00 3818311 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_43_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DHillman%26rft.aufirst%3DBJ%26rft.atitle%3DGovernment%2520health%2520policy%2520and%2520the%2520diffusion%2520of%2520new%2520medical%2520devices%26rft.jtitle%3DHealth%2520Serv%2520Res%26rft.date%3D1986%26rft.volume%3D21%26rft.spage%3D681%26rft.epage%3D711%26rft_id%3Dinfo%3Apmid%2F3818311 %00empty%00}-->
- HolahanJDorAZuckermanSUnderstanding the recent growth in Medicare physician expendituresJAMA1990263165816612106592 <!--${if: isGetFTREnabled}-->
- HonkanenLAMushlinAILachsMSchackmanBRCan hip protector use cost effectively prevent fractures in community-dwelling geriatric populations?J Am Geriatr Soc2006541658166517087691 <!--${if: isGetFTREnabled}-->
- HuberMOroszeEHealth expenditure trends in OECD countries, 1990–2001Health Care Financ Rev20032512214997690 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed<!--${googleScholarLinkReplacer: %00empty%00 journal Health+expenditure+trends+in+OECD+countries%2C+1990%E2%80%932001 author%3DM+Huber%26author%3DE+Orosze 2003 HuberMOroszeEHealth+expenditure+trends+in+OECD+countries%2C+1990%E2%80%932001Health+Care+Financ+Rev20032512214997690 1-22 Health+Care+Financ+Rev 25 %00null%00 %00empty%00 14997690 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_46_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DHuber%26rft.aufirst%3DM%26rft.atitle%3DHealth%2520expenditure%2520trends%2520in%2520OECD%2520countries%252C%25201990%25E2%2580%25932001%26rft.jtitle%3DHealth%2520Care%2520Financ%2520Rev%26rft.date%3D2003%26rft.volume%3D25%26rft.spage%3D1%26rft.epage%3D22%26rft_id%3Dinfo%3Apmid%2F14997690 %00empty%00}-->
- JonesCIWhy have Health Expenditures as a Share of GDP Risen So Much? National Bureau of Economic Research Working Paper Series, No 9325; 2002. Available from: http://www.stanford.edu/~chadj/health300.pdf. Accessed March 17, 2013. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 journal Why+have+Health+Expenditures+as+a+Share+of+GDP+Risen+So+Much%3F author%3DCI+Jones %00null%00 JonesCIWhy+have+Health+Expenditures+as+a+Share+of+GDP+Risen+So+Much%3FNational+Bureau+of+Economic+Research+Working+Paper+Series%2C+No+9325%3B+2002.+Available+from%3A+.+Accessed+March+17%2C+2013. %00empty%00 %00empty%00 %00empty%00 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_47_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DJones%26rft.aufirst%3DCI%26rft.atitle%3DWhy%2520have%2520Health%2520Expenditures%2520as%2520a%2520Share%2520of%2520GDP%2520Risen%2520So%2520Much%253F %00empty%00}-->
- KaiserCBrunner-La RoccaHPBuserPTIncremental cost-effectiveness of drug-eluting stents compared with a third-generation bare-metal stent in a real-world setting: randomised Basel Stent Kosten Effekivitats Trial (BASKET)Lancet200536692192916154019 <!--${if: isGetFTREnabled}-->
- KoenigLSiegelJMDobsonAHearleKHoSRudowitzRDrivers of healthcare expenditures associated with physician servicesAm J Manag Care20039Spec No 1SP34SP4212817614 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Drivers+of+healthcare+expenditures+associated+with+physician+services author%3DL+Koenig%26author%3DJM+Siegel%26author%3DA+Dobson%26author%3DK+Hearle%26author%3DS+Ho%26author%3DR+Rudowitz 2003 KoenigLSiegelJMDobsonAHearleKHoSRudowitzRDrivers+of+healthcare+expenditures+associated+with+physician+servicesAm+J+Manag+Care20039Spec+No+1SP34SP4212817614 SP34-SP42 Am+J+Manag+Care 9 Spec+No+1 %00empty%00 12817614 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_49_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DKoenig%26rft.aufirst%3DL%26rft.atitle%3DDrivers%2520of%2520healthcare%2520expenditures%2520associated%2520with%2520physician%2520services%26rft.jtitle%3DAm%2520J%2520Manag%2520Care%26rft.date%3D2003%26rft.volume%3D9%26rft.issue%3DSpec%2520No%25201%26rft.spage%3DSP34%26rft.epage%3DSP42%26rft_id%3Dinfo%3Apmid%2F12817614 %00empty%00}-->
- KuukasjarviPRasanenPMalmivaaraAAronenPSintonenHEconomic evaluation of drug-eluting stents: a systematic literature review and model-based cost-utility analysisInt J Technol Assess200723473479 <!--${if: isGetFTREnabled}-->
- LordSJHowardKAllenFA systematic review and economic analysis of drug-eluting coronary stents available in AustraliaMed J Aust200518346447116274347 <!--${if: isGetFTREnabled}-->
- MarchLMBarcinillaALCrossMJCosts and outcomes of total hip and knee joint replacement for rheumatoid arthritisClin Rheumatol2008271235124218500442 <!--${if: isGetFTREnabled}-->
- MarinelliMSoccettiAPanfoliNde PalmaLCost-effectiveness of cemented versus cementless total hip anthroplasty. A Markov decision analysis based on implant costJ Orthop Traumatol20089232819384477 <!--${if: isGetFTREnabled}-->
- MartinSRiceNSmithPCDoes health care spending improve health outcomes? Evidence from English programme budgeting dataJ Health Econ20082782684218261812 <!--${if: isGetFTREnabled}-->
- MasNSeinfieldJIs managed care restraining the adoption of technology by hospitals?J Health Econ2008271026104518417230 <!--${if: isGetFTREnabled}-->
- MattijsSLamboojiPEWestertGPDiffusion of innovations in health care: does the structural context determine its direction?Int J Technol Assess201026415420 <!--${if: isGetFTREnabled}-->
- McClellanMNewhouseJPThe marginal cost-effectiveness of medical technology: a panel instrumental-variables approachJ Econom1997773964 <!--${if: isGetFTREnabled}-->
- McKenzieLValeLStearnsSMetal on metal hip resurfacing arthroplasty. An economic analysisEur J Health Econ2003412212915609179 <!--${if: isGetFTREnabled}-->
- MittonCRRoseMSKohmanMLSheldonRSCost-utility analysis of pacemakers for the treatment of vasovagal syncopeAm J Cardiol1999841356135910614807 <!--${if: isGetFTREnabled}-->
- NicholGKaulPHusztiECost-effectiveness of cardiac resynchronization therapy in patients with symptomatic heart failureAnn Intern Med200414134335115353425 <!--${if: isGetFTREnabled}-->
- NewhouseJMedical care costs: how much welfare loss?J Econ Perspect1992632110128078 <!--${if: isGetFTREnabled}-->
- NeytMThiryNRameekersDVan BrabandtHCost-effectiveness of implantable cardioverter defibrillators for primary prevention in a Belgian contextAppl Health Econ Health Policy20086678018774871 <!--${if: isGetFTREnabled}-->
- OkunadeAAMurthyVNRTechnology as a major driver of health care costs: a cointegration analysis of the Newhouse conjectureJ Health Econ20022114715911852912 <!--${if: isGetFTREnabled}-->
- Oliveira MartinsJDe La MaisonneuveCThe Drivers of Public Expenditure on Health and Long-Term Care: An Integrated Approach2006 Available from: http://ssrn.com/abstract=917782. Accessed March 17, 2013. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 journal The+Drivers+of+Public+Expenditure+on+Health+and+Long-Term+Care%3A+An+Integrated+Approach author%3DJ+Oliveira+Martins%26author%3DC+De+La+Maisonneuve 2006 Oliveira+MartinsJDe+La+MaisonneuveCThe+Drivers+of+Public+Expenditure+on+Health+and+Long-Term+Care%3A+An+Integrated+Approach2006Available+from%3A+.+Accessed+March+17%2C+2013. %00empty%00 %00empty%00 %00empty%00 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_64_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DOliveira%2520Martins%26rft.aufirst%3DJ%26rft.atitle%3DThe%2520Drivers%2520of%2520Public%2520Expenditure%2520on%2520Health%2520and%2520Long-Term%2520Care%253A%2520An%2520Integrated%2520Approach%26rft.date%3D2006 %00empty%00}-->
- OwensDKSandersGDHarrisRACost-effectiveness of implantable cardioverter defibrillators relative to amiodarone for prevention of sudden cardiac deathAnn Intern Med19971261128992917 <!--${if: isGetFTREnabled}-->
- PackerCSimpsonSStevensAInternational diffusion of new health technologies: a ten-country analysis of six health technologiesInt J Technol Assess200622419428 <!--${if: isGetFTREnabled}-->
- PammolliFRiccaboniMOglialoroCMedical Devices Competitiveness and Impact on Public Health ExpenditureBruxelles, BelgiumEnterprise Directorate-General, European Commission2005 Available from: http://ideas.repec.org/p/pra/mprapa/16021.html. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 book Medical+Devices+Competitiveness+and+Impact+on+Public+Health+Expenditure author%3DF+Pammolli%26author%3DM+Riccaboni%26author%3DC+Oglialoro 2005 PammolliFRiccaboniMOglialoroCMedical+Devices+Competitiveness+and+Impact+on+Public+Health+ExpenditureBruxelles%2C+BelgiumEnterprise+Directorate-General%2C+European+Commission2005Available+from%3A+. %00empty%00 %00null%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_67_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Dbook%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DPammolli%26rft.aufirst%3DF%26rft.btitle%3DMedical%2520Devices%2520Competitiveness%2520and%2520Impact%2520on%2520Public%2520Health%2520Expenditure%26rft.pub%3DEnterprise%2520Directorate-General%252C%2520European%2520Commission%26rft.date%3D2005 %00empty%00}-->
- PedenEAFreelandMSA historical analysis of medical spending growth, 1960–1993Health Aff (Millwood)1995142352477657244 <!--${if: isGetFTREnabled}-->
- PedenEAFreelandMSInsurance effects on US medical spending (1960–1993)Health Econ199876716879890329 <!--${if: isGetFTREnabled}-->
- PricewaterhouseCoopersThe Factors Fueling Risking Healthcare Costs Report prepared for the American Association of Health Plans2002 Available from: http://heartland.org/sites/all/modules/custom/heartland_migration/files/pdfs/14621.pdf. Accessed March 15, 2013. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 journal The+Factors+Fueling+Risking+Healthcare+Costs %00empty%00 2002 PricewaterhouseCoopersThe+Factors+Fueling+Risking+Healthcare+CostsReport+prepared+for+the+American+Association+of+Health+Plans2002Available+from%3A+.+Accessed+March+15%2C+2013. %00empty%00 %00empty%00 %00empty%00 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_70_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aucorp%3DPricewaterhouseCoopers%26rft.atitle%3DThe%2520Factors%2520Fueling%2520Risking%2520Healthcare%2520Costs%26rft.date%3D2002 %00empty%00}-->
- RettigRAMedical innovation duels cost containmentHealth Aff (Millwood)1994137277927162 <!--${if: isGetFTREnabled}-->
- SandersGDHlatkyMAOwensDKCost-effectiveness of implantable cardioverter defibrillatorsN Engl J Med20053531471148016207849 <!--${if: isGetFTREnabled}-->
- SandersGDHlatkyMAEveryNRPotential cost-effectiveness of prophylactic use of the implantable cardiovascular defibrillator or amiodarone after myocardial infarctionAnn Intern Med200113587088311712877 <!--${if: isGetFTREnabled}-->
- SandersGDHlatkyMAOwensDKSpecial report: cost-effectiveness of implantable cardioverter defibrillators in a MADIT-II populationTechnology Evaluation Center Assessment Program Report2004193 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 journal Special+report%3A+cost-effectiveness+of+implantable+cardioverter+defibrillators+in+a+MADIT-II+population author%3DGD+Sanders%26author%3DMA+Hlatky%26author%3DDK+Owens 2004 SandersGDHlatkyMAOwensDKSpecial+report%3A+cost-effectiveness+of+implantable+cardioverter+defibrillators+in+a+MADIT-II+populationTechnology+Evaluation+Center+Assessment+Program+Report2004193 %00empty%00 Technology+Evaluation+Center+Assessment+Program+Report 19 3 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_74_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DSanders%26rft.aufirst%3DGD%26rft.atitle%3DSpecial%2520report%253A%2520cost-effectiveness%2520of%2520implantable%2520cardioverter%2520defibrillators%2520in%2520a%2520MADIT-II%2520population%26rft.jtitle%3DTechnology%2520Evaluation%2520Center%2520Assessment%2520Program%2520Report%26rft.date%3D2004%26rft.volume%3D19%26rft.issue%3D3 %00empty%00}-->
- SharplesLDDryerMCaffertyFCost-effectiveness of ventricular assist device use in the United Kingdom: Results from the evaluation of Ventricular Assist Device Programme in the UK (EVAD-UK)J Heart Lung Transplant2006251336134317097498 <!--${if: isGetFTREnabled}-->
- SchreyoggJBaumlerMBusseRBalancing adoption and affordability of medical devices in EuropeHealth Policy20099221822419410326 <!--${if: isGetFTREnabled}-->
- Segui-GomezMKeuffelEFrickKDCost and effectiveness of hip protectors among the elderlyInt J Technol Assess2002185566 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Cost+and+effectiveness+of+hip+protectors+among+the+elderly author%3DM+Segui-Gomez%26author%3DE+Keuffel%26author%3DKD+Frick 2002 Segui-GomezMKeuffelEFrickKDCost+and+effectiveness+of+hip+protectors+among+the+elderlyInt+J+Technol+Assess2002185566 55-66 Int+J+Technol+Assess 18 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_77_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DSegui-Gomez%26rft.aufirst%3DM%26rft.atitle%3DCost%2520and%2520effectiveness%2520of%2520hip%2520protectors%2520among%2520the%2520elderly%26rft.jtitle%3DInt%2520J%2520Technol%2520Assess%26rft.date%3D2002%26rft.volume%3D18%26rft.spage%3D55%26rft.epage%3D66 %00empty%00}-->
- ShriveFMMannsBJGalbraithPDEconomic evaluation of sirolimus-eluting stentsCan Med Assoc J200517234535115684117 <!--${if: isGetFTREnabled}-->
- SinghSSunHAnisAHCost-effectiveness of hip protectors in the prevention of osteoporosis related hip fractures in elderly nursing home residentsJ Rheumatol2004311607161315290742 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->PubMed Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal Cost-effectiveness+of+hip+protectors+in+the+prevention+of+osteoporosis+related+hip+fractures+in+elderly+nursing+home+residents author%3DS+Singh%26author%3DH+Sun%26author%3DAH+Anis 2004 SinghSSunHAnisAHCost-effectiveness+of+hip+protectors+in+the+prevention+of+osteoporosis+related+hip+fractures+in+elderly+nursing+home+residentsJ+Rheumatol2004311607161315290742 1607-1613 J+Rheumatol 31 %00null%00 %00empty%00 15290742 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_79_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DSingh%26rft.aufirst%3DS%26rft.atitle%3DCost-effectiveness%2520of%2520hip%2520protectors%2520in%2520the%2520prevention%2520of%2520osteoporosis%2520related%2520hip%2520fractures%2520in%2520elderly%2520nursing%2520home%2520residents%26rft.jtitle%3DJ%2520Rheumatol%26rft.date%3D2004%26rft.volume%3D31%26rft.spage%3D1607%26rft.epage%3D1613%26rft_id%3Dinfo%3Apmid%2F15290742 %00empty%00}-->
- SkinnerJStaigerDTechnology Diffusion and Productivity Growth in Health Care National Bureau of Economic Research Working Paper Series, No 14865; 2009. Available from: http://www.dartmouth.edu/~jskinner/documents/SkinnerStaigerw14865_000.pdf. Accessed March 17, 2013. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 journal Technology+Diffusion+and+Productivity+Growth+in+Health+Care author%3DJ+Skinner%26author%3DD+Staiger %00null%00 SkinnerJStaigerDTechnology+Diffusion+and+Productivity+Growth+in+Health+CareNational+Bureau+of+Economic+Research+Working+Paper+Series%2C+No+14865%3B+2009.+Available+from%3A+.+Accessed+March+17%2C+2013. %00empty%00 %00empty%00 %00empty%00 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_80_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DSkinner%26rft.aufirst%3DJ%26rft.atitle%3DTechnology%2520Diffusion%2520and%2520Productivity%2520Growth%2520in%2520Health%2520Care %00empty%00}-->
- SmithSDHefflerSKFreelandMSThe Impact of Technological Change on Health Care Cost Increases: An Evaluation of the Literature Health Care Financing Administration Working Paper; 2000. Available from: http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/downloads/tech_2000_0810.pdf. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 journal The+Impact+of+Technological+Change+on+Health+Care+Cost+Increases%3A+An+Evaluation+of+the+Literature author%3DSD+Smith%26author%3DSK+Heffler%26author%3DMS+Freeland %00null%00 SmithSDHefflerSKFreelandMSThe+Impact+of+Technological+Change+on+Health+Care+Cost+Increases%3A+An+Evaluation+of+the+LiteratureHealth+Care+Financing+Administration+Working+Paper%3B+2000.+Available+from%3A+. %00empty%00 %00empty%00 %00empty%00 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_81_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DSmith%26rft.aufirst%3DSD%26rft.atitle%3DThe%2520Impact%2520of%2520Technological%2520Change%2520on%2520Health%2520Care%2520Cost%2520Increases%253A%2520An%2520Evaluation%2520of%2520the%2520Literature %00empty%00}-->
- Von HoutBASerruysPWLemosPAOne-year cost-effectiveness of sirolimus eluting stents compared with bare metal stents in the treatment of single native de novo coronary lesions: an analysis from the Ravel trialHeart20059150751215772214 <!--${if: isGetFTREnabled}-->
- WeisbrodBAThe health care quadrilemma: an essay on technological change, insurance, quality of care and cost containmentJ Econ Lit199129523532 <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}-->Web of Science ®<!--${googleScholarLinkReplacer: %00empty%00 journal The+health+care+quadrilemma%3A+an+essay+on+technological+change%2C+insurance%2C+quality+of+care+and+cost+containment author%3DBA+Weisbrod 1991 WeisbrodBAThe+health+care+quadrilemma%3A+an+essay+on+technological+change%2C+insurance%2C+quality+of+care+and+cost+containmentJ+Econ+Lit199129523532 523-532 J+Econ+Lit 29 %00null%00 %00empty%00 %00empty%00 %00null%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_3_1_2_2_83_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Darticle%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DWeisbrod%26rft.aufirst%3DBA%26rft.atitle%3DThe%2520health%2520care%2520quadrilemma%253A%2520an%2520essay%2520on%2520technological%2520change%252C%2520insurance%252C%2520quality%2520of%2520care%2520and%2520cost%2520containment%26rft.jtitle%3DJ%2520Econ%2520Lit%26rft.date%3D1991%26rft.volume%3D29%26rft.spage%3D523%26rft.epage%3D532 %00empty%00}-->
- YaoGFreemantleNCalvertMJThe long-term cost-effectiveness of cardiac resynchronization therapy with or without an implantable cardioverter defibrillatorEur Heart J200728425117110403 <!--${if: isGetFTREnabled}-->
- YockCABoothroydDBOwensDKGarberAMHlatkyMACost-effectiveness of bypass surgery vs stenting in patients with multivessel coronary artery diseaseAm J Med200311538238914553874 <!--${if: isGetFTREnabled}-->
- YouJJWooADennisTKLife expectancy gains and cost-effectiveness of implantable cardioverter defibrillators for the primary prevention of sudden cardiac death in patients with hypertrophic cardiomyopathyAm Heart J200714589990717967596 <!--${if: isGetFTREnabled}-->