Abstract
Objective
To evaluate the clinical and economic burden of acute coronary syndrome (ACS), a common cardiovascular illness, in the Medicare population.
Methods
Data from the Medicare Current Beneficiary Survey were analyzed. Patients with incident hospitalization for ACS without similar events during the 6 months prior were included. Outcomes evaluated included inpatient mortality, 30-day mortality and readmission, subsequent hospitalization events, and total direct health care costs. Sample population weights were applied, accounting for multistage sampling design to obtain nationally representative estimates for the US Medicare population.
Results
Between March 1, 2002 and December 31, 2006, we identified 795 incident ACS patients (mean age 76 years; 49% male) representing 2,542,211 Medicare beneficiaries. The inpatient mortality rate was 9.71% and the 30-day mortality ranged from 10.96% to 13.93%. The 30-day readmission rate for surviving patients was 18.56% for all causes and 17.90% for cardiovascular disease (CVD)-related diagnoses. The incidence of death since admission was 309 cases per 1000 person–years. Among patients discharged alive, the incidence was 197 for death, 847 for CVD-related admission, and 906 for all-cause admission. During the year when the ACS event occurred, mean annual total direct health care costs per person were US$50,458, with more than half attributable to inpatient hospitalization ($27,609).
Conclusion
In this national representative Medicare population, we found a substantial clinical and economic burden for ACS. These findings suggest a continuing unmet medical need for more effective management of patients with ACS. The continuous burden underscores the importance of development of new interventions and/or strategies to improve long-term outcomes.
Introduction
Acute coronary syndrome (ACS) encompasses both unstable angina (UA) and myocardial infarction (MI), with or without ST-segment elevation (STE) and is currently one of the most common cardiovascular (CV) illnesses in the USA. It can cause significant morbidity and mortality.Citation1 In 2009, close to 1.2 million hospital discharges in the US were associated with an ACS diagnosis.Citation2 Close to 30% of patients had an ACS-hospitalization within 1 year of ACS onset,Citation3 and about 20% of patients hospitalized for ACS had a rehospitalization for ischemic heart diseases within 1 year.Citation3 ACS also has a high economic burden. The projected costs in 2015 for coronary heart disease, most of which consist of costs for ACS, include US$46.8 billion in direct health care costs and $82.8 billion in indirect costs.Citation4
Large prospective registries, such as the Global Registry of Acute Coronary Events (GRACE), have provided valuable information on treatment and practice patterns and outcomes of patients with ACS; however, the outcomes are often only being followed for a relatively short period of time (eg, 6 months).Citation5–Citation8 Several large trials also reported long-term outcomes among ACS patients, but real world data with usual care are still limited.Citation9,Citation10 Retrospective studies using data sources such as medical administrative claims usually allow a longer follow-up but typically lack hard outcomes, such as mortality.
ACS patients could incur significant health care costs because of the use of invasive procedures such as angiography and revascularization. Although these aggressive procedures are performed less frequently among elderly patients,Citation11 ACS could impose a significant burden on the Medicare program because approximately half of ACS patients are older than 65 years of age.Citation8 Several studies have reported the economic burden associated with ACS for commercially-insured populations,Citation3,Citation12–Citation15 but the burden for Medicare beneficiaries has not been examined. Similarly, long-term outcomes for the elderly population have been under-investigated.
The objective of this study was to assess clinical and economic outcomes among Medicare beneficiaries who were hospitalized for ACS. To achieve this goal, this study analyzed data from the Medicare Current Beneficiary Survey (MCBS),Citation16 a nationally representative sample of Medicare beneficiaries. Findings from this study could fill the gaps in knowledge of long-term outcomes of patients with ACS. The economic burden reported could provide a benchmark for consideration when assessing cost-effectiveness across therapies and inform the Medicare program about the potential cost offset associated with strategies to improve the quality of care for these patients.
Methods
Data source
Data from MCBS between 2001 and 2006 were analyzed. The MCBS is a panel survey sponsored by the Centers for Medicare and Medicaid Services with a multistage, stratified sampling design that allows for analysis of a nationally representative sample of all Medicare beneficiaries.Citation16 Each year, a panel of approximately 4000 beneficiaries is recruited and followed for 4 years. In a given year, there are data from four panels of approximately 16,000 beneficiaries available for cross-sectional analysis. MCBS collects a wide variety of data on socioeconomic characteristics and health care resource utilization and costs. Survey responses about health care use are brought together with Medicare Part A and Part B administrative billing claims to provide a complete picture of beneficiaries’ health services use. Three years of complete healthcare utilization data are collected for each panel, which includes Medicare and non-Medicare–reimbursed health care utilization. The medical claims reimbursed by Medicare contain information on dates of service, International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis and procedure codes, and paid amounts.
Study sample selection
ACS patients were selected from the MCBS based on one or more Medicare Part A inpatient admission claims with an associated diagnosis of ACS (ICD-9-CM: 410.xx [except 410.x2], 411.1x, 411.8x) between March 1, 2002 and December 31, 2006. We chose to conduct this analysis from the period after March 1, 2002, the date of the approval of clopidogrel, which became the standard of care, to reflect the current burden with all available evidence-based medical therapies. The date of first admission for this ACS event was denoted as the index date. We selected further incident cases by requiring patients to have a 6-month period with no ACS events prior to the index date. Furthermore, beneficiaries must have been in the database for at least 6 months before the index date.
Patient characteristics
Baseline demographic and socioeconomic characteristics including age, gender, race, census region, employment status, education status, income, marital status, and living arrangements were assessed. Common CV-related comorbidities, including atrial fibrillation, heart failure, hypertension, coronary arterial diseases, and hyperlipidemia were identified based on Medicare claims during the 6 months before the index date.
Study outcomes
Several clinical outcomes were identified from the index date until loss of follow-up (up to 2.5 years). Mortality was ascertained from hospital discharge status (actual date available) or from the survey data (reported monthly). All-cause rehospitalizations were identified based on Medicare Part A claims. Other hospitalization events, including MI, ischemic stroke, CV diseases (CVD), and major bleeding events were also examined ().
Inpatient mortality was determined based on the discharge status of the index ACS event. Because the exact date of death was not available for all patients, mortality between 30 days and 60 days was examined to provide a range for 30-day mortality. Thirty-day readmission was examined by assessing Medicare Part A claims within 30 days of the discharge date of the index ACS event for both all-cause and CVD-related readmissions, based on hospital claims with an associated diagnosis.
Annual health care costs, including both Medicare and non-Medicare reimbursed services, were summarized for the calendar year when the incident ACS event occurred. Costs combined plan-paid and beneficiaries’ out-of-pocket payments. Total health care costs and costs by settings – including inpatient hospital, medical provider, short-term facility, long-term facility, outpatient hospital, prescribed medicine, home health, dental, and hospice – were reported.
Analysis
Descriptive results were reported for each of the patient characteristics using means and standard errors (SE) for continuous variables and proportions for categorical variables. A Kaplan–Meier curve was plotted for the time to the occurrence of death since admission. The incidence rates of subsequent events of MI, ischemic stroke, CVD, major bleeding events, all-cause readmission, and death were calculated as the number of new cases divided by person–time at risk and reported as number of cases per 1000 person–years. The incidence of death was estimated from all of the ACS cases identified, and the incidence of subsequent events and death was estimated among those cases where patients were discharged alive from the hospital. Inpatient mortality was reported based on all of the ACS cases identified, and 30-day mortality was reported based on ACS cases having at least 30 days of follow-up. Thirty-day readmission rates were estimated among those cases where patients were discharged alive from the hospital and had at least 30 days of follow-up. Finally, the mean and SE of health care costs were summarized. Sample population weights were applied, accounting for multistage sampling design to obtain nationally representative estimates for the US Medicare population.
Results
Patient characteristics
This study identified 795 incident ACS patients, which can be extrapolated to 2,542,211 Medicare beneficiaries with ACS over 58 months between March 1, 2002 and December 31, 2006. These patients had a mean age of 76.1 years, with 49.2% being male, and the majority (86.1%) being white (). More than two-thirds of patients (70.4%) lived in metropolitan areas and 42.3% of patients were from the Southern (US) region. Only 8% of these patients were currently employed, and 67.2% had income levels below $25,000. Two-thirds (62.4%) of patients had a high school education or higher. Approximately 50% of patients were married, while 38.9% were widowed. During the 6 months prior to the index admission, 67.9% of patients had hypertension, 47.4% had hyperlipidemia, 40.4% had coronary artery disease, 22.9% had heart failure, and 13.1% had atrial fibrillation ().
Figure 1 Comorbid conditions during 6 months before admission for acute coronary syndrome.
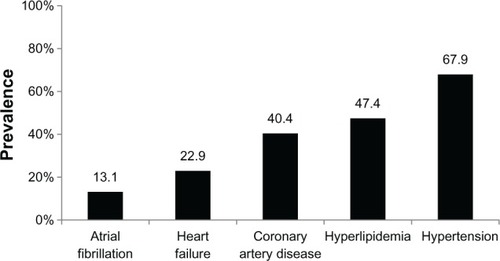
Table 1 Demographic and socioeconomic characteristics
Short-term clinical outcomes
The inpatient mortality rate of our study sample was 9.71% (95% confidence interval [CI]: 7.91%–11.50%; ). Because the vital status was available only on a monthly basis for some patients, 30-day mortality was estimated to be between 10.96% and 13.93%. Among those who survived, the 30-day readmission rate was 18.56% (95% CI: 15.39%–21.72%) for all-cause readmission and 17.90% (95% CI: 14.83%–20.98%) for CVD-related readmission.
Table 2 Mortality and readmission rates
Long-term clinical outcomes
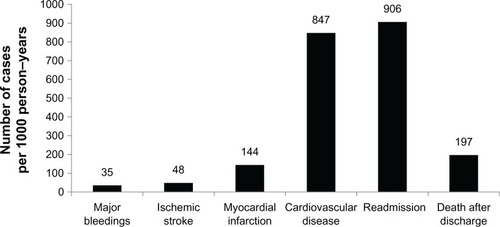
The median follow-up was 227 days, ranging from 1 day (for those who died right after being admitted) to 908 days. shows the Kaplan–Meier curve for survival probability from the time of admission of ACS patients. The same outcome when presented using incidence rate represents 309 deaths per 1000 person–years. Incidence rates of subsequent death and hospitalization for those discharged alive are presented in . If 1000 patients were followed for 1 year, 197 patients died. The incidence rate for all-cause readmission was 906 per 1000 person–years, with CVD being the most common reason (incidence rate = 847 per 1000 person–years). The incidence rates for major bleeding events, ischemic stroke, and MI were 35, 48, and 144 cases per 1000 person–years, respectively.
Figure 2 Kaplan–Meier curve for survival probability from the time of admission of patients with acute coronary syndrome.
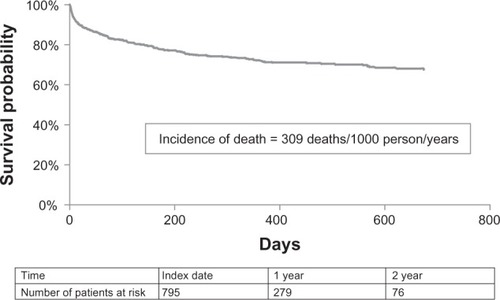
Figure 3 Weighted incident rates of patients discharged alive.
Economic outcomes
The mean annual total direct health care costs per person were $50,458 (SE = 1460; ). When we assessed costs by setting, $27,609 (SE = $1039) was incurred at the inpatient hospital (including index hospitalization), $9313 (SE = $396) was paid to medical providers, $3188 (SE = $324) was used for a short-term facility, $3131 (SE = $387) was used for a long-term facility, $2993 (SE = $269) went to outpatient hospitals, and $2554 (SE = $102) was used for prescribed medicine. These patients spent lesser amounts on services such as home health ($1275; SE = $132), dental care ($208; SE = $31), and hospice ($189; SE = $52).
Table 3 Annual health care costs (US$)
Discussion
This study analyzed claims from MCBS to examine the clinical and economic burden of ACS on Medicare beneficiaries. Using these nationally representative data, we assessed 795 incident ACS patients, representing 2.5 million Medicare beneficiaries accrued over 58 months, which extrapolates to approximately 523,000 new cases annually. Our study population had similar characteristics to those being reported in the prospective registries. The GRACE registry reported that two-thirds of ACS patients were male. This proportion decreased with age,Citation11,Citation12 which explains the lower proportion of males (49.2%) in our study sample. Compared with data from the GRACE registry reported for the elderly population (stratified by 65–74 years, 75–84 years, and ≥85 years), our reported rates of comorbidities, such as atrial fibrillation (13.1% versus 8.9%–19.5% in GRACE), heart failure (22.9% versus 11.9%–27.1% in GRACE), hyperlipidemia (47.4% versus 23.0%–48.1% in GRACE), and hypertension (67.9% versus 64.4%–67.8% in GRACE), were within the same range.Citation11
Our study showed that these ACS patients had a high short-term burden of inpatient mortality, 30-day mortality, and readmission. Nearly 1 in 10 patients died during their index hospital admission, and almost 1 in 5 were rehospitalized within 30 days of discharge. These data are higher than the inpatient mortality rate from the GRACE registry (4.6% in STEMI and 2.2% in non-STEMI), most likely due to age difference (mean age 76 years in our study and 65 years in GRACE registry).Citation17 When compared to the age-stratified inpatient mortality from GRACE (5.5% for those ACS patients aged 65–74 years, 9.3% for those aged 75–84 years, and 18.4 for those aged ≥ 85 years), our data are comparable.Citation11 Retrospective studies assessing the short-term outcomes of Medicare ACS patients are limited. There were a few studies for acute MI, reporting a 30-day mortality rate of 16%.Citation18–Citation20 A lower rate of 30-day mortality ranging between about 11% and 14% is anticipated, because ACS also includes UA, for which the mortality rate is lower.Citation8 The 30-day hospital readmission rate found in this study (18.56%) is also comparable to the rate (19.9%) reported for acute MI among Medicare beneficiaries.Citation18
The GRACE registry reported short-term outcomes such as 6-month mortality, but data on long-term outcome for ACS patients are limited, especially for the elderly population.Citation17 One GRACE registry study in New Zealand reported mortality rate of 1143 ACS patients (mean age = 65 years) to be 12.1% at 6 months, 14.8% at 1 year, 18.7% at 2 years, 25.0% at 3 years, and 39.2% at 4 years.Citation21 With data up to 2.5 years for each beneficiary in this Medicare population, we found that the burden remained high. If 1000 ACS patients who were discharged alive were followed for 1 year, 906 patients would be readmitted and 197 patients would die. Most patients were readmitted for CVD-related reasons. Such a high clinical burden also translates into a high financial burden on the Medicare program.
Past studies have reported the economic burden associated with ACS in commercially-insured populations aged 18–64 years, with estimated annual direct medical costs ranging from $32,345 to $54,821 per patient.Citation3,Citation15 Approximately 50%–60% of the costs related to ACS are due to rehospitalization.Citation3,Citation15 Our study reported that the annual total health care cost for Medicare ACS patients was $50,458. Because the MCBS captures health care costs on a calendar-year basis, the estimated cost does not necessarily represent all costs incurred after the occurrence of ACS events. This might underestimate the burden. Although this figure includes Medicare and non-Medicare expenditures, the majority of these services, especially inpatient services, were paid by Medicare. Similar to the findings from commercially insured populations, more than half of this cost was attributable to inpatient hospitalization ($27,609).
This study demonstrates that ACS is associated with a high economic and clinical burden to Medicare beneficiaries. Hospital cost was the biggest cost driver – partly due to advances in invasive strategies such as percutaneous coronary intervention,Citation22 and also the risk of rehospitalization. During the 58 months when the Medicare beneficiaries, who were newly hospitalized for ACS, were identified these 795 patients incurred $8.3 million in total health care expenditure annually. This sum extrapolates to $26.5 billion to the Medicare program per year. Future research should focus on understanding the cost drivers of ACS patients to identify and implement effective strategies to improve the quality of care and generate cost savings.
Several limitations from this study need to be recognized. ACS patients were identified based on ICD-9-CM diagnosis codes from Medicare claims and we have no access to the medical chart to confirm diagnosis via biomarkers or electrocardiogram. As with any survey, self-reported data are subject to recall bias. Although MCBS collects data on health care utilization whether reimbursed by Medicare or not, diagnoses were captured only from Medicare Part A and Part B claims. Therefore, medical conditions treated with medical services that were covered completely by other insurers or paid solely out of pocket could not be identified. Similarly, major outcomes that may not have been identified could potentially lead to an underestimation of the burden. The date of death was reported as the last day of the month if it could not be identified based on the discharge status of Medicare Part A claims. Hence, the risk of mortality could potentially be underestimated. Since the exact 30-day mortality could not be estimated, a range for this measure was provided instead.
Conclusion
In this nationally representative Medicare population, we found a substantial clinical and economic burden for ACS. These findings suggest a continuing unmet medical need for more effective management of patients with ACS. The continuous burden of ACS underscores the importance of the development of new interventions and/or strategies to improve long-term outcomes.
Acknowledgments
The authors would like to acknowledge Chameleon Communications International, who provided editorial support with funding from Janssen Scientific Affairs, LLC.
Supplementary materials
Table S1 Diagnosis codes used to identify outcomes
Disclosure
This research was funded by Janssen Scientific Affairs, LLC. SC, LB, and MS are employees of United BioSource Corporation, a consulting company that has received research grants from Janssen Scientific Affairs; CC and JS are employees of Janssen Scientific Affairs, LLC (a J&J company) and are shareholders of J&J. The authors have no other conflicts of interest to declare.
References
- KolanskyDMAcute coronary syndromes: morbidity, mortality, and pharmacoeconomic burdenAm J Manag Care200915Suppl 2S36S4119355807
- RogerVLGoASLloyd-JonesDMAmerican Heart Association Statistics Committee and Stroke Statistics SubcommitteeHeart disease and stroke statistics–2012 update: a report from the American Heart AssociationCirculation2012125e2e22022179539
- MenzinJWygantGHauchOJackelJFriedmanMOne-year costs of ischemic heart disease among patients with acute coronary syndromes: findings from a multi-employer claims databaseCurr Med Res Opin20082446146818194592
- HeidenreichPATrogdonJGKhavjouOAAmerican Heart Association Advocacy Coordinating CommitteeStroke CouncilCouncil on Cardiovascular Radiology and InterventionCouncil on Clinical CardiologyCouncil on Epidemiology and PreventionCouncil on ArteriosclerosisThrombosis and Vascular BiologyCouncil on CardiopulmonaryCritical CarePerioperative and ResuscitationCouncil on Cardiovascular NursingCouncil on the Kidney in Cardiovascular DiseaseCouncil on Cardiovascular Surgery and AnesthesiaInterdisciplinary Council on Quality of Care and Outcomes ResearchForecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart AssociationCirculation201112393394421262990
- FoxKAGoodmanSGKleinWManagement of acute coronary syndromes. Variations in practice and outcome; findings from the Global Registry of Acute Coronary Events (GRACE)Eur Heart J2002231177118912127920
- FoxKAEagleKAGoreJMStegPGAndersonFAGRACE and GRACE2 InvestigatorsThe Global Registry of Acute Coronary Events, 1999 to 2009–GRACEHeart2010961095110120511625
- Grace InvestigatorsRationale and design of the GRACE (Global Registry of Acute Coronary Events) Project: a multinational registry of patients hospitalized with acute coronary syndromesAm Heart J200114119019911174331
- StegPGGoldbergRJGoreJMGRACE InvestigatorsBaseline characteristics, management practices, and in-hospital outcomes of patients hospitalized with acute coronary syndromes in the Global Registry of Acute Coronary Events (GRACE)Am J Cardiol20029035836312161222
- MarschnerICColquhounDSimesRJLong-Term Intervention with Pravastatin in Ischemic Disease (LIPID) studyLong-term risk stratification for survivors of acute coronary syndromes. Results from the Long-term Intervention with Pravastatin in Ischemic Disease (LIPID) Study. LIPID study investigatorsJ Am Coll Cardiol200138566311451296
- LahoudRHoweMKrishnanSMZachariasSJacksonEAEffect of use of combination evidence-based medical therapy after acute coronary syndromes on long-term outcomesAm J Cardiol201210915916422011560
- AvezumAMakdisseMSpencerFGRACE InvestigatorsImpact of age on management and outcome of acute coronary syndrome: observations from the Global Registry of Acute Coronary Events (GRACE)Am Heart J2005149677315660036
- BerensonKOgbonnayaACascianoREconomic consequences of ACS-related rehospitalizations in the USCurr Med Res Opin20102632933619968457
- EtemadLRMcCollamPLTotal first-year costs of acute coronary syndrome in a managed care settingJ Manag Care Pharm20051130030615871640
- ZhaoZWingetMEconomic burden of illness of acute coronary syndromes: medical and productivity costsBMC Health Services Research2011111921199575
- JohnstonSSCurkendallSMakenbaevaDThe direct and indirect cost burden of acute coronary syndromeJ Occup Environ Med2011532721187788
- AdlerGSA profile of the Medicare Current Beneficiary SurveyHealth Care Financ Rev19941515316310138483
- FoxKAStegPGEagleKAGRACE investigatorsDecline in rates of death and heart failure in acute coronary syndromes, 1999–2006JAMA20072971892190017473299
- BernheimSMGradyJNLinZNational patterns of risk-standardized mortality and readmission for acute myocardial infarction and heart failure. Update on publicly reported outcomes measures based on the 2010 releaseCirc Cardiovasc Qual Outcomes2010345946720736442
- BradleyEHHerrinJCurryLVariation in hospital mortality rates for patients with acute myocardial infarctionAm J Cardiol20101061108111220920648
- FihnSDVaughan-SarrazinMLowyEDeclining mortality following acute myocardial infarction in the Department of Veterans Affairs Health Care SystemBMC Cardiovasc Disord200994419719849
- TangEWWongCKHerbisonPGlobal Registry of Acute Coronary Events (GRACE) hospital discharge risk score accurately predicts long-term mortality post acute coronary syndromeAm Heart J2007153293517174633
- WrightRSAndersonJLAdamsCD2011 ACCF/AHA Focused Update of the Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction (Updating the 2007 Guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice GuidelinesCirculation20111232022206021444889