Abstract
Background
This article describes the personal, societal, and economic burden attributable to schizophrenia in the People’s Republic of China and highlights the potential for effective outpatient treatment to reduce this burden given recent changes in the Chinese health care system. The importance of effective antipsychotic therapy in reducing the burden of schizophrenia is also examined.
Methods
Published research on the burden, disability, management, and economic costs of schizophrenia in the People’s Republic of China was examined in the context of the larger body of global research. Research written in English or Chinese and published before June 2012 was identified using PubMed, CNKI, and Wanfang Med database searches. The contribution of effective antipsychotic therapy in reducing the risk for relapse and hospitalization and improving patients’ functioning is described.
Results
Schizophrenia imposes a substantial burden on Chinese society, with indirect costs accounting for the majority of the total cost. Functional impairment is high, leading to lost wages and work impairment. In the People’s Republic of China, schizophrenia is the most common diagnosis among hospitalized psychiatric patients. Ongoing changes in the Chinese health care system may reduce some barriers to effective relapse prevention in schizophrenia and potentially reduce hospitalizations. The use of antipsychotics for acute episodes and maintenance treatment has been shown to decrease symptom severity and reduce the risk for relapse and hospitalization. However, discontinuing antipsychotic medication appears common and is a strong predictor of relapse. Cost-effectiveness research in the People’s Republic of China is needed to examine the potential gains from improved outpatient antipsychotic treatment.
Conclusion
Schizophrenia is a very costly mental illness in terms of personal, economic, and societal burden, both in the People’s Republic of China and globally. When treated effectively, patients tend to persist longer with antipsychotic treatment, have fewer costly relapses, and have improved functioning. Further research examining the long-term effects of reducing barriers to effective treatments on the societal burden of schizophrenia in the People’s Republic of China is needed.
Introduction
Schizophrenia is a highly debilitating mental illness that is seen across nearly every culture and is characterized by impaired thinking, feeling, behavior, and functioning.Citation1–Citation3 The World Health Organization ranks schizophrenia among the top ten causes of years lost because of disability.Citation4 Most of the research on schizophrenia has been conducted in Western countries. The purpose of this review is to examine the available literature on the personal, societal, and economic burden attributable to schizophrenia in the People’s Republic of China, in the context of international research in this field, and to highlight the importance of effective antipsychotic therapy and relapse prevention in reducing the burden of schizophrenia in both the acute and maintenance treatment phases.
Diagnosis
The primary symptoms in schizophrenia can be broadly categorized into positive and negative symptoms.Citation1,Citation5,Citation6 Positive symptoms include delusions, hallucinations, disorganized speech, and bizarre behavior; negative symptoms include fat emotions, reduced speech, and reduced goal-driven behavior. Globally, schizophrenia is usually diagnosed using either the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR)Citation1 or the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) criteria.Citation6 In the People’s Republic of China, schizophrenia is diagnosed using the Chinese Classification of Mental Disorders, 3rd Edition, Revised (CCMD-3) criteria.Citation5 Although not identical, diagnostic criteria for schizophrenia within the DSM-IV-TR, ICD-10, and CCMD-3 are largely similar, although CCMD-3 differs in that it requires a loss of insight during the active phase of the illness as well as significant social dysfunction.Citation5 Both the ICD-10 and CCMD-3 require continuous symptoms for at least 1 month, rather than the 6-month duration required by the DSM-IV-TR. Regardless of the diagnostic system, implicit in the symptoms of schizophrenia are deficits in cognition, social functioning, and productive functioning.Citation7,Citation8
Epidemiology
Schizophrenia is found in all societies. A meta-analysis of 85 studies estimated the worldwide prevalence of schizophrenia to be 0.54%.Citation9 In the People’s Republic of China, a recent large-scale study estimated the 1-month prevalence rate at 0.78%, with similar rates found in rural (0.80%) and urban (0.72%) areas.Citation10 Other studies in the People’s Republic of China have reported prevalence estimates ranging approximately from 0.2% to 2.2%.Citation9,Citation11 The prevalence of schizophrenia in the People’s Republic of China appears to be similar to the global prevalence.
Disease management in the People’s Republic of China
When reviewing global research on schizophrenia, which has been primarily generated in Western countries, any cultural, socioeconomic, and treatment modality differences present in the People’s Republic of China need to be considered. The results of the largest schizophrenia observational study to date, the Worldwide-Schizophrenia Outpatient Health Outcomes study, which did not include the People’s Republic of China, revealed the existence of country-level and geographic differences in the course and prognosis of schizophrenia. In general, patients living in less developed regions had a more favorable disease course: continuous remission was lowest in Northern and Southern Europe (45.7%) and highest in North Africa and the Middle East (67.4%); remission followed by a relapse was lowest in North Africa and the Middle East (13.6%); and a persistent symptomatic course was lowest in East Asia (15.1%) and highest in Southern Europe (39.3%).Citation12 These findings parallel a previous study by the World Health Organization.Citation13 The improved outcomes in developing countries may reflect differences in extended family structures, greater social inclusion, reduced stigma, or greater employment in schizophrenia.Citation14 Although the better prognosis in developing countries conclusion may be an oversimplification, a recent review of 23 longitudinal studies in low- to middle-income countries found a large heterogeneity in outcomes from different studies and countries and reported that a lack of treatment was consistently associated with worse outcomes, whereas accessing care was associated with improved outcomes.Citation15 Nevertheless, the variability in outcomes across regions highlights the need to consider the culture, socioeconomics, and treatment methods within a given region or country.
The stigma associated with mental illness can have a pernicious effect on individuals with mental health problems and their families.Citation16 In the People’s Republic of China, the disruptive behaviors of individuals with schizophrenia are considered a serious cultural transgression, and the stigma may extend to the families as well as the affected individual.Citation17,Citation18 The family bears a greater responsibility for managing the individuals with schizophrenia in the People’s Republic of China relative to many Western cultures, in which the primary responsibility often falls on the affected individual or the health care system.Citation19 As a result, in the People’s Republic of China, individuals with schizophrenia and their families may try to hide the disorder for as long as possible, creating potential barriers to receiving and adhering with mental health treatment.Citation17,Citation18
The health care system in the People’s Republic of China has undergone substantial changes during the last 35 years. Beginning in 1978, decreased central government support and significant policy changes led to a decentralized and privatized health care system.Citation19,Citation20 As part of the new market-based economy, hospitals were encouraged to make a profit, and many mental health rehabilitation facilities dependent on government funding were closed or transformed into small-scale psychiatric hospitals.Citation21 These economic reforms resulted in a reduction in the number of community-based and work-rehabilitation centers, particularly in less affluent rural areas, where mental health services became essentially nonexistent. Specialized psychiatric hospitals became the primary treatment setting for patients with psychiatric conditions, and very few community-based psychiatry services existed.Citation18 In 2002, the first National Mental Health Plan was signed. It included stated goals to establish an effective system for mental health care and to strengthen existing mental health services to decrease the burden and disability associated with mental illness. Several programs were initiated, and they have had a significant effect in some regions.Citation21
A mental health reform program, named the 686 Program, received formal support from the Ministry of Finance in 2004. By early 2005, 60 demonstration sites were established, including one urban and one rural site in each of the People’s Republic of China’s 30 provinces. The program screened patients for possible psychosis, subsidized the cost of medications and hospitalizations for the socially disadvantaged, and implemented community action programs that encompassed the best-practice principles from allied health disciplines. By 2009, the program’s coverage had been expanded to include 112 cities and 96.9 million people, or 7.3% of the People’s Republic of China’s 1.33 billion population.Citation21,Citation22
Large changes in the availability of health insurance have also occurred in the last 15 years in the People’s Republic of China. The rapid economic growth experienced within the People’s Republic of China has been concentrated in the urban areas and has contributed to regional disparities.Citation23 Although commercial health insurance schemes that primarily target the more affluent in Chinese society have expanded, the major change has been the introduction of a countrywide health insurance system, known as basic social medical insurance (BSMI). The BSMI has expanded rapidly, driven by the central government’s goal to provide universal health coverage to the entire population of the People’s Republic of China.Citation24 The BSMI consists of three components: the basic social medical insurance for urban employees (initiated in 1998), the basic social medical insurance for urban residents (initialed in 79 cities in 2007), and the New Rural Cooperative Medical Insurance for Rural Residents (established in 2003).Citation24 The tremendous changes in insurance coverage implemented in the last decade have the potential to improve access to effective health care for hundreds of millions of people and to potentially reduce health-related disability in the People’s Republic of China.
Although insurance coverage is now available to most individuals in the People’s Republic of China, specific coverage for schizophrenia and mental health is varied. In some of the wealthier Eastern areas, the mental health service system is being reformed quickly within whole provinces or cities, but in some underdeveloped Western areas, where skills and resources are lacking, the existing national mental health policies have not yet been implemented.Citation21 The implementation of specific mental health policies and services also tends to be more common in Eastern China than Western China and for urban compared with rural residents. More than 30% of the regions have no specific health insurance policies for mental disorders, and where policies do exist, they tend to be appropriately aimed at the reimbursement of outpatient services.Citation25 Without appropriate coverage for outpatient care of patients with schizophrenia, there is a risk for inadvertently incentivizing the overuse of more expensive hospitalization and inpatient services.
Past research has also shown that many patients with schizophrenia in the People’s Republic of China may not always receive needed care. A large-scale epidemiologic study in the People’s Republic of China reported that 27.6% of patients with psychotic disorders never sought treatment.Citation10 Similarly, another study in rural China found that almost one-third of individuals with schizophrenia received no treatment at all, despite 76% of these individuals having marked symptoms.Citation11 The primary reasons reported for the patient not receiving treatment were lack of money (35.3%), uncertainty about the patient’s illness (29.5%), the patient refusing to accept drug treatment (18.6%), and having no relatives to care for the patient (14.7%).Citation26 Perceptions and psychological attributions of schizophrenia as well as issues of availability, access, and affordability of care may represent important barriers to effective treatment in the People’s Republic of China.
Another important barrier in the People’s Republic of China is the limited number of mental health care practitioners and inpatient facilities. In 2004, the People’s Republic of China had 1.99 psychiatric nurses and 1.29 psychiatrists per 100,000 population compared with 6.50 and 13.70, respectively, in the United States and 24.80 and 9.80 in Europe. Similarly, the People’s Republic of China had 1.06 psychiatric beds per 10,000 population compared with 7.70 in the United States and 8.00 in Europe.Citation27 Although there are fewer mental health care practitioners and inpatient facilities in the People’s Republic of China, estimates of the length of stay for a patient with schizophrenia have ranged from 36.8 to 69.9 days,Citation28,Citation29 which is longer than the 7.4 to 11.1 days seen in the United States,Citation30 30.7 days seen in Australia,Citation31 and 35 days seen in Spain,Citation32 but similar to the number of days seen in Finland.Citation33 The longer inpatient stays in the People’s Republic of China may reflect fewer available community-based treatment options.
Disability
The World Health Organization lists schizophrenia in the top eight causes of years lost to disability.Citation4,Citation34 In the People’s Republic of China, schizophrenia was ranked as the 18th most important health problem.Citation18
The functional impairments associated with schizophrenia are sufficiently severe to be apparent in high-level indicators such as unemployment and marriage rates. Globally, the unemployment rate in samples of individuals with schizophrenia has ranged from 10% to 96%, depending on the study method and country, with the majority of estimates being greater than 75%.Citation35–Citation39 In the People’s Republic of China, estimates of the unemployment rate for patients with schizophrenia have ranged from 41.3% to 64.7%.Citation40–Citation43 Although lower than many global estimates for the rate of unemployment in schizophrenia, these rates are substantially higher than the overall unemployment rate in the People’s Republic of China, which is reported to be lower than in most countries.Citation44
Global estimates of marriage rates for patients with schizophrenia have ranged from about 5% to 30%, with most between 15% and 30%.Citation35–Citation37,Citation45–Citation48 In the People’s Republic of China, the rates of marriage for samples of individuals with schizophrenia have ranged from 10.9% to 46.7%.Citation28,Citation40–Citation43 Marriage and employment rates may be slightly higher in the People’s Republic of China than globally, but they remain substantially lower than in populations without schizophrenia because of the strong effect of the disorder on social and productive functioning.
Economic consequences of schizophrenia
Schizophrenia is an expensive disorder and is associated with high levels of direct costs to the health care system and very high levels of indirect costs, primarily because of lost productivity. Direct costs refer to payments that are made, including those for inpatient stays, outpatient services, and medications, whereas indirect costs refer to resources that are lost as a result of the illness, including lost wages of the patient, lost wages of caregivers, and lost years of life. A review of multiple cost-of-illness studies for schizophrenia from around the globe reported that the direct health care costs of treating schizophrenia accounted for between 1.4% and 3.0% of total national health expenditures.Citation49 In the People’s Republic of China, schizophrenia has been reported to contribute 1.3% of the total burden of disease.Citation50
Comparing costs across geographies is challenging, given differences in study methodologies and health care systems. Although few studies have taken a comprehensive view of the cost of schizophrenia across all of the People’s Republic of China, several studies have examined the costs in specific geographic areas.
Cost of schizophrenia in the People’s Republic of China
Zhai et alCitation50 followed-up 299 patients with schizophrenia from Shandong and Hunan provinces who met DSM-IV diagnostic criteria for 1 year. The patients and their caregivers maintained receipts for all health care services and medications received and completed the Economic Cost Questionnaire every 2 months during the year. The median annual costs in Chinese currency per patient were ¥4370 (approximately US $700) in direct costs and ¥10,081 (approximately US $1600) in indirect costs. Direct costs for those patients who had at least one hospitalization (¥7614) were substantially higher than for those who were not hospitalized (¥1812; P < 0.001). Caregivers bore a substantial part of the indirect costs (¥3600). Although the annual per patient costs are much lower in the People’s Republic of China than in most Western countries, the average net income of a rural resident was only ¥2936 in 2004 (¥9422 disposable income for an urban resident),Citation51 and much of the indirect cost may have fallen on the patient and his or her family.Citation50
In Zhejiang province in 2010, other research examined the direct psychiatric hospital costs for 7684 inpatients. Schizophrenia was the most common diagnosis, making up 3117 of the 7684 discharges. Median total cost for schizophrenia was ¥10,765 per admission or ¥241 per day. Psychiatric medications made up ¥834 of the cost during the hospital admission. Schizophrenia and other psychotic disorders had the longest duration of admission, with an average of 45 days.Citation29
Cost of schizophrenia outside the People’s Republic of China
Administrative claims from the Taiwanese governmental health insurance data in 1999 found that the equivalent of US $112.4 million was spent on care for schizophrenia, which represents 1.2% of the total national health care expenditures. Most of the expenditures (US $84.5 million or 75.2%) were on inpatient care, with US $27.9 million spent on outpatient care, with inpatient and outpatient medication costs of US $28.9 million. On a per patient basis, the average annual direct treatment costs for schizophrenia were US $2144.Citation52 Another study in Taiwan followed up 74 patients treated with risperidone or haloperidol for 1 year beginning during 1999 or 2000. The average annual per patient direct costs were estimated at US $2115, but indirect costs were substantially higher, at US $14,461, primarily because of lost wages for the patient and caregivers.Citation53
Using data from the National Health Insurance in South Korea, the total direct health care costs for schizophrenia during 2005 were estimated at US $418.7 million, with inpatient costs accounting for US $327.7 million (78.3%), outpatient costs being US $77.7 million (18.6%), and medication costs being US $13.3 million (3.2%). The average per patient annual total direct treatment cost was US $2600. Indirect costs were substantially higher, at US $2635.1 million, and were driven primary by lost wages.Citation54
In comparison, the total costs in the United States in 2002 were estimated to be $62.7 billion, with direct health care costs comprising $22.7 billon.Citation55 Hospital and long-term care costs made up 47%, outpatient care 31%, and medications 22.2% of the direct health care costs. The annual per patient direct cost was $15,464.Citation55
The higher indirect costs reported in the People’s Republic of China are consistent with findings from other geographies, although Asian countries appear to have a larger proportion of indirect costs (87% in Taiwan,Citation53 83% in Korea,Citation54 and 63% in IndiaCitation56) than those reported in Western countries (47% to 81%).Citation49 Because of substantial disability, individuals with schizophrenia incur significant indirect costs resulting from lost wages, premature mortality and suicide,Citation49,Citation55 involvement with the criminal justice system,Citation57 and caregiver burden.Citation49,Citation58 In a review of multiple studies from various geographies, the high direct and indirect costs of schizophrenia have been consistently reported.Citation49
Health care resource use
Globally, the use of inpatient facilities is a significant component of the cost of treating schizophrenia.Citation55,Citation59 In a review of cost-of-illness studies for schizophrenia, Knapp et alCitation49 found that hospitalization accounted for between 16.5% and 94% of costs, depending on the country and study methods, with two-thirds of the studies finding that hospitalization accounted for more than 50% of total direct health care costs.
Throughout the world, studies have reported the length of hospitalization for each schizophrenia admission to range from 7.4 to 90 days.Citation30,Citation60–Citation63 In the People’s Republic of China, published estimates of the length of hospitalization for patients with schizophrenia have ranged from 36.8 to 69.9 days, depending on the year and the health insurance status of the patient, with insured patients tending to have longer inpatient stays.Citation28,Citation29 These estimates may not be representative of the current situation or the whole country, given the rapidly changing health care system and regional variations in the People’s Republic of China.
Medications also account for a significant, but substantially lower, proportion (2.0%–13.0% in Western countries) of direct health care costs compared with inpatient and outpatient services.Citation49,Citation59 One study in Zhejiang province reported that the overall cost of hospitalization was ¥10,765 for schizophrenia, with ¥834 for psychiatric medications and ¥719 for nonpsychiatric medication.Citation29 The use of effective antipsychotic medication has been shown to decrease both inpatient and outpatient health care use,Citation49 and low rates of medication adherence have been shown to be associated with higher total inpatient costs.Citation64,Citation65
Treatment goals
The treatment goals for patients with schizophrenia vary, depending on the phase of the illness. During an acute episode, the goals of treatment are to prevent harm, control disturbed behavior, suppress symptoms, attempt to get a rapid return to the best level of functioning, and develop an effective treatment alliance with the patient and family.Citation2,Citation8 Once in the stabilization phase, usually 3–6 months after the acute phase, the primary goals are the consolidation of the therapeutic relationship, reduction of positive symptoms, improvement in cognitive and negative symptoms, improvement of social deficits, promotion of insight and medication adherence, support of developing individual coping strategies, integration of the patient back into their community, and identification of support options to minimize the rate of relapse.Citation3,Citation8 Finally, in the stable phase, the goals become improvement of functioning and recovery, maintaining or improving quality of life, and prevention of relapses.Citation3,Citation8 Therapeutic interventions for schizophrenia include both psychosocial and pharmacological treatments, and the best course of treatment is often a combination of both. In the People’s Republic of China, adding psychosocial interventions to medications has been shown to decrease the risk for medication discontinuation and relapse and to improve quality of life and functioning compared with medication alone.Citation66
Role of antipsychotics
Antipsychotic medications have been the mainstay of the treatment for schizophrenia since their introduction in the 1950s and are recommended for use to treat acute psychotic states as well as maintenance treatment to prevent future relapses.Citation2,Citation8,Citation67,Citation68 Frequently, antipsychotic medications are broadly categorized as being either typical, first-generation antipsychotics (FGAs) or the newer, atypical, second-generation antipsychotics (SGAs). FGAs and SGAs have been thought to differ in terms of treatment effectiveness, tolerability, and adverse event profile.Citation69 The SGAs have been reported to lead to improvements in patient outcomes and a reduced risk for extrapyramidal adverse events compared with FGAs.Citation67,Citation70 However, FGAs and SGAs are heterogeneous groups of medications that have been somewhat arbitrarily grouped together primarily as a result of being developed before or after clozapine.Citation69 In clinical care, SGAs have largely replaced the older FGAs, with risperidone, olanzapine, and quetiapine often being the most commonly prescribed agents.Citation71,Citation72 Research examining antipsychotic use patterns for schizophrenia in the People’s Republic of China also suggests that the SGAs are replacing the FGAs.Citation73 The most commonly used SGAs in the People’s Republic of China appear to be clozapine, risperidone, olanzapine, and quetiapine.Citation74
Relapse
Symptomatic relapse in schizophrenia can be devastating not only to the patients but also to their families. When the patients’ symptoms remain under control, the patients can slowly begin to reintegrate into society; however, when they experience an acute relapse, the setback can be dramatic, often disrupting relationships and employment. Relapse often results in hospitalizationCitation35,Citation63,Citation75 and leads to increases in the use of outpatient services and medication use.Citation75 Relapses tend to increase symptom persistence, disrupt efforts at rehabilitation, and damage relationships, and may lead to greater cognitive decline.Citation76,Citation77
Predictors of relapse
Global treatment guidelines for schizophrenia recommend continuing antipsychotic medications for a minimum or 1 to 2 years after a first-episode patient is stable because this treatment is one of the most efficacious means of relapse prevention.Citation3,Citation8,Citation68 For patients who have had multiple episodes, continuing antipsychotic treatment for a minimum of 5 years and potentially throughout the lifetime is recommended.Citation3,Citation8
A recent meta-analysis of 65 randomized controlled trials found that compared with those taking placebo, patients taking antipsychotic medications were significantly less likely to relapse (relative risk, 0.35) or to be hospitalized (relative risk, 0.38).Citation78 The number needed to treat indicated that during the study periods, for every three patients maintained on an antipsychotic instead of placebo, a single relapse would be prevented.Citation78 The evidence from global studies is strong that antipsychotic maintenance treatment prevents future relapses.
Nonadherence with antipsychotic medication is one of the strongest predictors of relapse.Citation79 When medications are discontinued, the risk for symptomatic relapse has been shown to increase by nearly five times.Citation80 Similarly, medication nonadherence has been shown to be predictive of increased hospitalization rates.Citation81–Citation84 In the People’s Republic of China, a randomized controlled trial found that relative to continuing treatment with the initial antipsychotic (risperidone) dose, random assignment to dose reduction increased the risk for relapse substantially (odds ratio, 2.9), as did poor adherence with medication.Citation43
Nonadherence may be particularly problematic in the People’s Republic of China when patients and their families do not believe that the patient needs to continue treatment with an antipsychotic medication.Citation26,Citation85 An epidemiologic study identified 510 patients with schizophrenia in rural Xinjin county and found that only 30 (5.9%) were currently taking antipsychotic treatment, 92 (18.0%) underwent inconsistent treatment for less than 2 months, 106 (20.8%) had only used traditional Chinese herbal medicines, and 156 (30.6%) had never received any treatment.Citation11 A more recent observational study followed up 1133 patients treated with antipsychotics and found that 40.5% discontinued the study antipsychotic during the 1-year study.Citation86 Other reviews have reported that most patients did not remain on medication for more than 1 year after their initial hospital admission.Citation18 More research is needed to understand the rates of early medication discontinuation and the factors that lead to early discontinuation of antipsychotic treatment in the People’s Republic of China.
Antipsychotics differ in effectiveness
Global research has found that patients are more likely to continue treatment with some antipsychotics relative to others. Time to discontinuation of an antipsychotic for any cause has become an important marker of the real-world effectiveness of antipsychotics in the treatment of schizophrenia.Citation87 Global research has found that patients will continue taking, and clinicians will continue to prescribe, an antipsychotic if they believe the efficacy of the medication, particularly for positive symptoms, outweighs any tolerability issues.Citation88 A recent review of the comparative effectiveness of atypical antipsychotics for the treatment of schizophrenia found that clozapine was the most effective antipsychotic, followed by olanzapine and then by all other atypical and typical antipsychotics.Citation89 Because of its greater efficacy, clozapine remains the treatment of choice for treatment-resistant patients, despite blood monitoring recommendations because of the potential for agranulocytosis, which can be fatal.Citation8,Citation90 Among other (nonclozapine) atypical antipsychotics, olanzapine has been shown to differ on effectiveness when measured as time to all-cause medication discontinuation.
The National Institute of Mental Health-sponsored Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study found that patients persisted longer with olanzapine than quetiapine or risperidone.Citation91 Similarly, large observational trials in Europe have found patients treated with clozapine and olanzapine remain on their antipsychotic medication for a longer period of time than many other commonly prescribed atypical or typical antipsychotics.Citation33,Citation92,Citation93 The only study specifically examining antipsychotic discontinuation rates in the People’s Republic of China, a prospective observational study, failed to find any significant differences.Citation86 However, the rate of treatment discontinuation at 12 months was high (36.7%–46.9%), and the treatment duration (mean, 8.9 months) was short for all antipsychotics studied. The cost of medications in this study was paid for by the patients or their families, and the authors state that affordability may have been a factor that influenced the results.Citation86
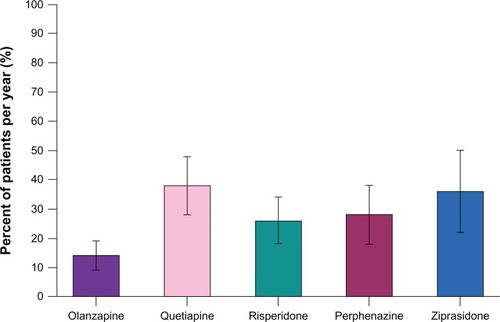
The CATIE study also examined the rates of hospitalization for exacerbations of schizophrenia during the 18-month study.Citation91,Citation94 Similar to the findings on medication discontinuation, the risk for hospitalization was lowest for olanzapine-treated patients and highest among the quetiapine-treated patients ().
Figure 1 Annual hospitalization rates for exacerbation of schizophrenia in CATIE (Phase I).Citation94 Adapted with permission from Psychiatric Services, (Copyright ©2011). American Psychiatric Association. All Rights Reserved.
Abbreviation: CATIE, Clinical Antipsychotic Trials of Intervention Effectiveness.
Similarly, a large, prospective, observational study of patients with schizophrenia treated in usual clinical care in Europe also found that olanzapine provided significantly improved negative, positive, and cognitive symptoms compared with risperidone, quetiapine, oral typicals, and depot typicals.Citation95
Antipsychotic efficacy
In contrast to effectiveness research, which examines health outcomes from treatments when implemented in usual clinical care, efficacy research examines key clinical outcomes such as symptom reduction from protocol-implemented treatment in well controlled studies. A meta-analysis of 150 randomized double-blind controlled trials comparing the efficacy of typical and atypical antipsychotics found better overall efficacy for the atypical antipsychotics on positive and negative symptoms compared with the typical antipsychotics. When specific atypical antipsychotics were compared with typical antipsychotics, greater efficacy was observed for clozapine, olanzapine, amisulpride, and risperidone, but not the other atypical antipsychotics.Citation96 In another meta-analysis of 78 randomized clinical trials comparing the atypical antipsychotics head-to-head, the authors found that the atypicals could not be considered all alike on efficacy, with olanzapine showing significantly greater efficacy than risperidone, quetiapine, aripiprazole, or ziprasidone; clozapine showing significantly greater efficacy than zotepine; and risperidone showing significantly greater efficacy than quetiapine and ziprasidone.Citation97 An examination of longer-term symptomatic relapse rates across studies found that patients taking olanzapine had significantly less risk for relapse compared with those treated with risperidone, quetiapine, ziprasidone, or typical antipsychotics.Citation98 Globally, research has found that the short-term efficacy and longer-term relapse prevention of atypical antipsychotics varies for the different compounds, with greater efficacy reported for clozapine and olanzapine.
The Chinese literature on the comparative efficacy of antipsychotics appears similar to the global research. In a randomized, open-label trial of antipsychotic drug-naïve Chinese patients, olanzapine demonstrated significantly greater decreases in schizophrenic symptoms compared with ziprasidone.Citation99 A study comparing risperidone and aripiprazole reported no differences in efficacy,Citation100 and another study showed greater efficacy of risperidone over haloperidol for treatment-resistant patients.Citation101 The research from the People’s Republic of China, although less comprehensive, appears consistent with the global research.
Antipsychotics and tolerability
A meta-analysis using randomized double-blind studies of atypical and typical antipsychotics in the treatment of schizophrenia found that patients treated with atypicals were significantly less likely to need adjunctive treatment for extrapyramidal symptoms but were significantly more likely to gain weight, particularly when treated with clozapine or olanzapine.Citation96,Citation102 Olanzapine treatment has also been associated with significantly higher increases in cholesterol than aripiprazole, risperidone, and ziprasidone and with significantly higher increases in blood glucose than amisulpride, aripiprazole, quetiapine, risperidone, and ziprasidone.Citation102 Risperidone-treated patients have been found to have a significantly higher likelihood for prolactin increases and sexual dysfunction than other atypical antipsychotics.Citation98,Citation103 Studies conducted in the People’s Republic of China have also found significantly reduced extrapyramidal symptoms,Citation86,Citation104 but greater weight gain and greater increases in cholesterol and triglycerides,Citation86,Citation104–Citation106 for olanzapine-treated patients relative to patients treated with risperidone, ziprasidone, or typical antipsychotics. Both global and Chinese studies have found that efficacy and tolerability profiles vary for different antipsychotics. The clinician’s goal is to identify the antipsychotic with the efficacy and tolerability profile best suited to a specific individual with schizophrenia.
Effective management of adverse events may lead to improved outcomes. A recent post hoc analysis from the Chinese subgroup (n = 330) of a multicountry, 6-month, prospective, observational study of outpatients with schizophrenia who were treated with olanzapine compared outcomes for patients who participated or did not participate in a weight control program. Not only did the participants in the weight control program gain less weight but they also had significantly better clinical and functional outcomes: greater improvement in illness severity, higher treatment response rate, shorter time to response, reduced impairment in work activities, and greater improvement in patients’ insight.Citation107,Citation108 This finding supports the clinical experience that participation in a weight control program may help prevent clinically significant weight gain in patients treated with antipsychotics and may also be associated with additional clinical and functional benefits that may help prevent relapse.
Discussion
Schizophrenia imposes a high burden on Chinese society, particularly on the individuals with the disease and their families.Citation50 The Chinese health care system has undergone major changes since 1978, becoming more decentralized and privatized.Citation19–Citation21 At this time, there are initiatives to establish universal health care coverage, and a growing number of individuals are covered by health insurance systems, which can provide some relief from the high direct health care costs of schizophrenia for the patient and family members.Citation21,Citation24 In the recent past, very few community-based psychiatric services have been available, particularly in rural areas, with most services provided by specialty psychiatric hospitals that were primarily located in urban areas.Citation21 In late 2012, the Mental Health Law of the People’s Republic of China was passed. In addition to providing more protection to people suffering from mental illness, including a new protocol for commitment to psychiatric hospitals, the new law supports the expansion of community mental health services.Citation109,Citation110 With the ongoing mental health reforms, there is an opportunity for the development of cost-effective outpatient treatment services that use effective medications to prevent relapses. In terms of direct health care costs, hospitalizations are expensive and often of long duration.Citation29 However, the greatest burden associated with schizophrenia in the People’s Republic of China is a result of indirect costs,Citation50 which include the burden on the caregiver and family and the costs associated with lost productivity, social dysfunction, and premature mortality.
Unfortunately, in the People’s Republic of China, many patients with schizophrenia do not initiate or persist with antipsychotic treatment. Several barriers to receiving antipsychotic treatment exist, including patient and family beliefs about the need for continuing antipsychotics, the cost of the medications to the families, and the limited availability of outpatient services.Citation26 This discordance between actual and recommended practice is a major cause for concern. Research has repeatedly linked antipsychotic discontinuation with greater rates of relapse and hospitalization and with further functional disability.Citation78–Citation80 The burden of the disease could potentially be reduced in the People’s Republic of China if persistence on antipsychotic therapy could be increased.
Improved access to effective treatments in the People’s Republic of China, particularly the combination of family education and antipsychotic treatment, could help reduce the personal, societal, and economic burden of this disease. One study found that adding family-based psychoeducational treatment to antipsychotic medication reduced treatment discontinuation and relapses and increased social functioning, health-related quality of life, and employment rates.Citation66 Recent reviews of antipsychotic efficacy and effectiveness have shown that patients are more likely to persist on therapy with the more effective second-generation antipsychotics for a longer period of time.Citation89,Citation111 Cost-effectiveness research investigating potential gains from improved access to effective antipsychotic treatment of people with schizophrenia in the People’s Republic of China is needed, given the high costs associated with this condition to the individual, the health care system, and society.
Conclusion
Improving access and increasing the levels of persistence with antipsychotic medications in the People’s Republic of China would likely reduce the rate of relapse, improve patient outcomes, and reduce total treatment costs. Several barriers exist to optimum treatment, including the paucity of outpatient psychiatric centers, beliefs about the need for maintenance treatment once acute symptoms are treated, and the relatively high cost of medication to patients and families. Increasing the duration of maintenance treatment, particularly with effective antipsychotics, would likely translate into lower rates of relapse, which is expected to help reduce the personal, societal, and economic burden of schizophrenia in the People’s Republic of China by improving patient outcomes.
Disclosure
The authors report no conflicts of interest in this work. William Montgomery, Li Liu, Haya Ascher-Svanum, Hai Bo Xue, and Tamas Treuer are all full time employees of Eli Lilly and Company or one subsidiaries and minor stockholders in Eli Lilly and Company. Michael Stensland is a full time employee of Agile Outcomes Research Inc, a research firm hired to consult on this work.
References
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision4th edArlington, VAAmerican Psychiatric Association2000
- FalkaiPWobrockTLiebermanJGlenthojBGattazWFMöllerHJWFSBP Task Force on Treatment Guidelines for SchizophreniaWorld Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, Part 1: acute treatment of schizophreniaWorld J Biol Psychiatry20056313219116173147
- FalkaiPWobrockTLiebermanJGlenthojBGattazWFMöllerHJWFSBP Task Force on Treatment Guidelines for SchizophreniaWorld Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 2: long-term treatment of schizophreniaWorld J Biol Psychiatry20067154016509050
- MathersCBoermaTFatDMThe Global Burden of Disease: 2004 UpdateGenevaWorld Health Organization2008 Available from: http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdfAccessed November 1, 2012
- Chinese Society of PsychiatryChinese Classification of Mental Disorders3rd edShandong, ChinaShandong Science and Technology Press2001
- World Health OrganizationInternational Statistical Classification of Diseases and Related Health Problems, 10th Revision Version for 2007GenevaWorld Health Organization2007 Available from: http://apps.who.int/classifications/apps/icd/icd10online2007/Accessed September 19, 2012
- LambertMKarowALeuchtSSchimmelmannBGNaberDRemission in schizophrenia: validity, frequency, predictors, and patients’ perspective 5 years laterDialogues Clin Neurosci201012339340720954433
- LehmanAFLiebermanJADixonLBAmerican Psychiatric Association, Steering Committee on Practice GuidelinesPractice guideline for the treatment of patients with schizophrenia, second editionAm J Psychiatry2004161Suppl 215615000267
- SahaSChantDMcGrathJMeta-analyses of the incidence and prevalence of schizophrenia: conceptual and methodological issuesInt J Methods Psychiatr Res2008171556118286464
- PhillipsMRZhangJShiQPrevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001–2005: an epidemiological surveyLancet200937396802041205319524780
- RanMSXiangMZLiSXPrevalence and course of schizophrenia in a Chinese rural areaAust N Z J Psychiatry200337445245712873330
- NovickDHaroJMHongJRegional differences in treatment response and three year course of schizophrenia across the worldJ Psychiatr Res201246785686422575332
- JablenskyASartoriusNErnbergGSchizophrenia: manifestations, incidence and course in different cultures. A World Health Organization ten-country studyPsychol Med Monogr Suppl1992201971565705
- BirchwoodMCochraneRMacmillanFCopestakeSKucharskaJCarrissMThe influence of ethnicity and family structure on relapse in first-episode schizophrenia. A comparison of Asian, Afro-Caribbean, and white patientsBr J Psychiatry19921617837901483164
- CohenAPatelVTharaRGurejeOQuestioning an axiom: better prognosis for schizophrenia in the developing world?Schizophr Bull200834222924417905787
- PhillipsMRPearsonVLiFXuMYangLStigma and expressed emotion: a study of people with schizophrenia and their family members in ChinaBr J Psychiatry200218148849312456518
- YangLHApplication of mental illness stigma theory to Chinese societies: synthesis and new directionsSingapore Med J2007481197798517975685
- PhillipsMRCharacteristics, experience, and treatment of schizophrenia in ChinaDialogues Clin Neurosci20013210911922033637
- ParkLXiaoZWorthJParkJMMental health care in China: recent changes and future challengesHarvard Health Policy Rev2005623545
- BlumenthalDHsiaoWPrivatization and its discontents – the evolving Chinese health care systemN Engl J Med2005353111165117016162889
- LiuJMaHHeYLMental health system in China: history, recent service reform and future challengesWorld Psychiatry201110321021621991281
- China Statistical Yearbook 2010 [homepage on the Internet]National Bureau of Statistics in ChinaBeijing, ChinaChina Statistics Press2010 Available from: http://www.stats.gov.cn/tjsj/ndsj/2010/indexeh.htm8142012
- HungLMRaneSTsaiJShiLAdvancing primary care to promote equitable health: implications for ChinaInt J Equity Health2012111222264309
- DongKMedical insurance system evolution in ChinaChina Economic Review2009204591597
- LiangDWangQYingX[Analysis on status quo of medical insurance policies on mental disorders in China.]China Health Policy Studies2011474650 Chinese. http://d.wanfangdata.com.cn/periodical_zgwszcyj201107010.aspxAccessed May 20, 2013
- RanMXiangMHuangMShanYNatural course of schizophrenia: 2-year follow-up study in a rural Chinese communityBr J Psychiatry2001178215415811157428
- World Health OrganizationMental health atlas 2005 [webpage on the Internet]GenevaWorld Health Organization2005 Available from: http://www.who.int/mental_health/evidence/mhatlas05/en/Accessed November 2, 2012
- PhillipsMRLuSHWangRWEconomic reforms and the acute inpatient care of patients with schizophrenia: the Chinese experienceAm J Psychiatry19971549122812349286181
- YangSLQianMCLuWCost of treating medical conditions in psychiatric inpatients in Zhejiang, ChinaShanghai Archives of Psychiatry2011236329337
- StenslandMWatsonPRGrazierKLAn examination of costs, charges, and payments for inpatient psychiatric treatment in community hospitalsPsychiatr Serv201263766667122588167
- LowLFDraperBHospitalization patterns for psychiatric disorders across the lifespan in Australia from July 1998 to June 2005Psychiatr Serv200960111311619114581
- Saz-ParkinsonZMedelACediel-GarcíaPCastelloteJBouzaCAmateJMTrends on schizophrenia admissions during the deinstitutionalisation process in Spain (1980–2004)Soc Psychiatry Psychiatr Epidemiol201146111095110120972771
- TiihonenJWahlbeckKLönnqvistJEffectiveness of antipsychotic treatments in a nationwide cohort of patients in community care after first hospitalisation due to schizophrenia and schizoaffective disorder: observational follow-up studyBMJ2006333756122416825203
- RösslerWSalizeHJvan OsJRiecher-RösslerASize of burden of schizophrenia and psychotic disordersEur Neuropsychopharmacol200515439940915925493
- AlmondSKnappMFrancoisCToumiMBrughaTRelapse in schizophrenia: costs, clinical outcomes and quality of lifeBr J Psychiatry2004184434635115056580
- AlonsoJCroudaceTBrownJHealth-related quality of life (HRQL) and continuous antipsychotic treatment: 3-year results from the Schizophrenia Health Outcomes (SOHO) studyValue Health200912453654319900255
- CiudadAAlvarezEBobesJSanLPolaviejaPGilaberteIRemission in schizophrenia: results from a 1-year follow-up observational studySchizophr Res20091081–321422219168329
- MarwahaSJohnsonSSchizophrenia and employment – a reviewSoc Psychiatry Psychiatr Epidemiol200439533734915133589
- PerlickDARosenheckRAKaczynskiRBinghamSCollinsJAssociation of symptomatology and cognitive deficits to functional capacity in schizophreniaSchizophr Res2008991–319219917851042
- YeungFKChanSHClinical characteristics and objective living conditions in relation to quality of life among community-based individuals of schizophrenia in Hong KongQual Life Res20061591459146916957873
- XiangYTWengYZLeungCMTangWKUngvariGSQuality of life of Chinese schizophrenia outpatients in Hong Kong: relationship to sociodemographic factors and symptomatologyAust N Z J Psychiatry200741544244917464737
- XiangYTWangCYWangYSocio-demographic and clinical determinants of quality of life in Chinese patients with schizophrenia: a prospective studyQual Life Res201019331732220135234
- XiangYTWangCYWengYZPredictors of relapse in Chinese schizophrenia patients: a prospective, multi-center studySoc Psychiatry Psychiatr Epidemiol201146121325133021046070
- GilesJParkAZhangJWhat is China’s true unemployment rate?China Economic Review2005162149170
- AdvokatCDixonDSchneiderJComatyJEJrComparison of risperidone and olanzapine as used under “real-world” conditions in a state psychiatric hospitalProg Neuropsychopharmacol Biol Psychiatry200428348749515093956
- Ascher-SvanumHNyhuisAWFariesDEKinonBJBakerRWShekharAClinical, functional, and economic ramifications of early nonresponse to antipsychotics in the naturalistic treatment of schizophreniaSchizophr Bull20083461163117118156640
- HaroJMEdgellETFrewerPAlonsoJJonesPBSOHO Study GroupThe European Schizophrenia Outpatient Health Outcomes Study: baseline findings across country and treatmentActa Psychiatr Scand Suppl200341671512755849
- Silva de LimaMde Jesus MariJBreierAMaria CostaAPondé de SenaEHotopfMQuality of life in schizophrenia: a multicenter, randomized, naturalistic, controlled trial comparing olanzapine to first-generation antipsychoticsJ Clin Psychiatry200566783183816013897
- KnappMMangaloreRSimonJThe global costs of schizophreniaSchizophr Bull200430227929315279046
- ZhaiJGZhaoJPChenJDAn investigation on economic costs of schizophrenia in two medical establishments in Hunan and ShandongChinese Journal of Psychiatry20074014144
- China Statistics Press[National Economic and Social Development Statistics Bulletin 2004.] China Statistics http://www.stats.gov.cn/tjgb/ndtjgb/qgndtjgb/t20050228_402231854.htm5202013 Chinese
- LangHCSuTPThe cost of schizophrenia treatment in TaiwanPsychiatr Serv200455892893015292543
- LeeIHChenPSYangYKThe functionality and economic costs of outpatients with schizophrenia in TaiwanPsychiatry Res2008158330631518243334
- ChangSMChoSJJeonHJEconomic burden of schizophrenia in South KoreaJ Korean Med Sci200823216717518436996
- WuEQBirnbaumHGShiLThe economic burden of schizophrenia in the United States in 2002J Clin Psychiatry20056691122112916187769
- GroverSAvasthiAChakrabartiSBhansaliAKulharaPCost of care of schizophrenia: a study of Indian out-patient attendersActa Psychiatr Scand20051121546315952946
- Ascher-SvanumHNyhuisAWFariesDEBallDEKinonBJInvolvement in the US criminal justice system and cost implications for persons treated for schizophreniaBMC Psychiatry2010101120109170
- AwadAGVorugantiLNPThe burden of schizophrenia on caregivers: a reviewPharmacoeconomics200826214916218198934
- GarattiniLBarbuiCClementeRCornagoDParazziniFStudy Group SCOREDirect costs of schizophrenia and related disorders in Italian community mental health services: a multicenter, prospective 1-year follow up studySchizophr Bull200430229530215279047
- Ascher-SvanumHZhuBFariesDErnstFRA comparison of olanzapine and risperidone on the risk of psychiatric hospitalization in the naturalistic treatment of patients with schizophreniaAnn Gen Hosp Psychiatry2004311115175112
- DaltioCSMariJJFerrazMBDirect medical costs associated with schizophrenia relapses in health care services in the city of São PauloRev de Saude Publica20114511423
- GauSSChungCHGauCSA pharmacoeconomic analysis of atypical antipsychotics and haloperidol in first-episode schizophrenic patients in TaiwanJ Clin Psychopharmacol200828327127818480683
- WeidenPJOlfsonMCost of relapse in schizophreniaSchizophr Bull19952134194297481573
- EaddyMGroggALocklearJAssessment of compliance with antipsychotic treatment and resource utilization in a Medicaid populationClin Ther200527226327215811492
- KnappMKingDPugnerKLapuertaPNon-adherence to antipsychotic medication regimens: associations with resource use and costsBr J Psychiatry2004184650951615172945
- GuoXZhaiJLiuZEffect of antipsychotic medication alone vs combined with psychosocial intervention on outcomes of early-stage schizophrenia: a randomized, 1-year studyArch Gen Psychiatry201067989590420819983
- BuchananRWKreyenbuhlJKellyDLSchizophrenia Patient Outcomes Research Team (PORT)The 2009 schizophrenia PORT psychopharmacological treatment recommendations and summary statementsSchizophr Bull2010361719319955390
- National Collaborating Centre for Mental HealthSchizophrenia: The NICE Guideline on Core Interventions in the Treatment and Management of Schizophrenia in Adults in Primary and Secondary Care (Updated edition)Leicester, UKThe British Psychological Society and the Royal College of Psychiatrists2010 Available from: http://www.nice.org.uk/nicemedia/live/11786/43607/43607.pdfAccessed September 18, 2012
- LeuchtSKisslingWDavisJMSecond-generation antipsychotics for schizophrenia: can we resolve the conflict?Psychol Med200939101591160219335931
- DossenbachMErolAel Mahfoud KessaciMIC-SOHO Study GroupEffectiveness of antipsychotic treatments for schizophrenia: interim 6-month analysis from a prospective observational study (IC-SOHO) comparing olanzapine, quetiapine, risperidone, and haloperidolJ Clin Psychiatry200465331232115096069
- PrahPPetersenINazarethIWaltersKOsbornDNational changes in oral antipsychotic treatment for people with schizophrenia in primary care between 1998 and 2007 in the United KingdomPharmacoepidemiol Drug Saf201221216116921858898
- WeinbrennerSAssionHJStargardtTBusseRJuckelGGerickeCADrug prescription patterns in schizophrenia outpatients: analysis of data from a German health insurance fundPharmacopsychiatry2009422667119308881
- AnFRXiangYTWangCYChange of psychotropic drug prescription for schizophrenia in a psychiatric institution in Beijing, China between 1999 and 2008Int J Clin Pharmacol Ther201048427027420353748
- ChongMYTanCHFujiiSAntipsychotic drug prescription for schizophrenia in East Asia: rationale for changePsychiatry Clin Neurosci2004581616714678459
- Ascher-SvanumHZhuBFariesDEThe cost of relapse and the predictors of relapse in the treatment of schizophreniaBMC Psychiatry201010220059765
- AmmingerGPEdwardsJBrewerWJHarriganSMcGorryPDDuration of untreated psychosis and cognitive deterioration in first-episode schizophreniaSchizophr Res200254322323011950547
- LiebermanJAPerkinsDBelgerAThe early stages of schizophrenia: speculations on pathogenesis, pathophysiology, and therapeutic approachesBiol Psychiatry2001501188489711743943
- LeuchtSTardyMKomossaKHeresSKisslingWDavisJMMaintenance treatment with antipsychotic drugs for schizophreniaCochrane Database Syst Rev20125CD00801622592725
- Ayuso-GutiérrezJLdel Río VegaJMFactors influencing relapse in the long-term course of schizophreniaSchizophr Res1997282–31992069468354
- RobinsonDWoernerMGAlvirJMPredictors of relapse following response from a first episode of schizophrenia or schizoaffective disorderArch Gen Psychiatry199956324124710078501
- GilmerTPDolderCRLacroJPAdherence to treatment with antipsychotic medication and health care costs among Medicaid beneficiaries with schizophreniaAm J Psychiatry2004161469269915056516
- LawMRSoumeraiSBRoss-DegnanDAdamsASA longitudinal study of medication nonadherence and hospitalization risk in schizophreniaJ Clin Psychiatry2008691475318312037
- WeidenPJKozmaCGroggALocklearJPartial compliance and risk of rehospitalization among California Medicaid patients with schizophreniaPsychiatr Serv200455888689115292538
- SvarstadBLShiremanTISweeneyJKUsing drug claims data to assess the relationship of medication adherence with hospitalization and costsPsychiatr Serv200152680581111376229
- PhillipsMRLiYStroupTSXinLCauses of schizophrenia reported by patients’ family members in ChinaBr J Psychiatry2000177202510945083
- GuoXFangMZhaiJEffectiveness of maintenance treatments with atypical and typical antipsychotics in stable schizophrenia with early stage: 1-year naturalistic studyPsychopharmacology (Berl)2011216447548421369751
- StroupTSMcEvoyJPSwartzMSThe National Institute of Mental Health Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) project: schizophrenia trial design and protocol developmentSchizophr Bull2003291153112908658
- Ascher-SvanumHNyhuisAWStaufferVReasons for discontinuation and continuation of antipsychotics in the treatment of schizophrenia from patient and clinician perspectivesCurr Med Res Opin201026102403241020812791
- AttardATaylorDMComparative effectiveness of atypical antipsychotics in schizophrenia: what have real-world trials taught us?CNS Drugs201226649150822668246
- LahdelmaLAppelbergBClozapine-induced agranulocytosis in Finland, 1982–2007: long-term monitoring of patients is still warrantedJ Clin Psychiatry201273683784222480452
- LiebermanJAStroupTSMcEvoyJPClinical Antipsychotic Trials of Intervention Effectiveness (CATIE) InvestigatorsEffectiveness of antipsychotic drugs in patients with chronic schizophreniaN Engl J Med2005353121209122316172203
- TiihonenJHaukkaJTaylorMHaddadPMPatelMXKorhonenPA nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophreniaAm J Psychiatry2011168660360921362741
- HaroJMSuarezDNovickDBrownJUsallJNaberDSOHO Study GroupThree-year antipsychotic effectiveness in the outpatient care of schizophrenia: observational versus randomized studies resultsEur Neuropsychopharmacol200717423524417137759
- OlfsonMAscher-SvanumHFariesDEMarcusSCPredicting psychiatric hospital admission among adults with schizophreniaPsychiatr Serv201162101138114521969639
- HaroJMEdgellETNovickDSOHO advisory boardEffectiveness of antipsychotic treatment for schizophrenia: 6-month results of the Pan-European Schizophrenia Outpatient Health Outcomes (SOHO) studyActa Psychiatr Scand2005111322023115701107
- LeuchtSCorvesCArbterDEngelRRLiCDavisJMSecond-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysisLancet20093739657314119058842
- LeuchtSKomossaKRummel-KlugeCA meta-analysis of head-to-head comparisons of second-generation antipsychotics in the treatment of schizophreniaAm J Psychiatry2009166215216319015230
- GlickIDCorrellCUAltamuraACMid-term and long-term efficacy and effectiveness of antipsychotic medications for schizophrenia: a data-driven, personalized clinical approachJ Clin Psychiatry201172121616162722244023
- WuXLWangJHHuSHTaoJSerum prolactin levels and the acute-phase efficacy in drug-naïve schizophrenia treated with ziprasidone and olanzapine (translated version)East Asian Arch Psychiatry201222171122447799
- ChanHYLinWWLinSKefficacy and safety of aripiprazole in the acute treatment of schizophrenia in Chinese patients with risperidone as an active control: a randomized trialJ Clin Psychiatry2007681293617284127
- ZhangXYZhouDFCaoLYZhangPYWuGYShenYCRisperidone versus haloperidol in the treatment of acute exacerbations of chronic inpatients with schizophrenia: a randomized double-blind studyInt Clin Psychopharmacol200116632533011712620
- Rummel-KlugeCKomossaKSchwarzSHead-to-head comparisons of metabolic side effects of second generation antipsychotics in the treatment of schizophrenia: a systematic review and meta-analysisSchizophr Res20101232–322523320692814
- KomossaKRummel-KlugeCSchwarzSRisperidone versus other atypical antipsychotics for schizophreniaCochrane Database Syst Rev20111CD00662621249678
- LiYMZhaoJPOuJJWuRREfficacy and tolerability of ziprasidone vs olanzapine in naive first-episode schizophrenia: a 6-week, randomized, open-label, flexible-dose studyPharmacopsychiatry201245517718122290206
- LeeELeungCMWongEAtypical antipsychotics and weight gain in Chinese patients: a comparison of olanzapine and risperidoneJ Clin Psychiatry200465686486615291666
- LeeEChowLYLeungCMMetabolic profile of first and second generation antipsychotics among Chinese patientsPsychiatry Res2011185345645820554016
- AngQTangJZhaoJFactors associated with weight gain during six-month olanzapine therapyChinese Journal of Psychiatry201144316
- MontgomeryWTreuerTYeWDoes participation in a weight control program also improve clinical and functional outcomes for Chinese patients with schizophrenia treated with olanzapine?Proceedings of the 5th ISPOR Asia Pacific ConferenceSeptember 2–4, 2012Taipei, Taiwan http://www.valueinhealthjournal.com/article/S1098-3015%2812%2902106-7/abstractAccessed May 20, 2013
- ChenHHPhillipsMRChengHTranslated and annotated version of China’s new Mental Health LawShanghai Archives of Psychiatry2012246305321
- HvistendahlMWorld’s biggest health care system goes under the knifeScience2013339611950550723371991
- Soares-WeiserKBéchard-EvansLLawsonAHDavisJAscher-SvanumHTime to all-cause treatment discontinuation of olanzapine compared to other antipsychotics in the treatment of schizophrenia: a systematic review and meta-analysisEur Neuropsychopharmacol201323211812522633617