
Abstract
Background
Delirium and frailty – both potentially reversible geriatric syndromes – are seldom studied together, although they often occur jointly in older patients discharged from hospitals. This study aimed to explore the relationship between delirium and frailty in older adults discharged from hospitals.
Methods
Of the 221 patients aged >65 years, who were invited to participate, only 114 gave their consent to participate in this study. Delirium was assessed using the confusion assessment method, in which patients were classified dichotomously as delirious or nondelirious according to its algorithm. Frailty was assessed using the Edmonton Frailty Scale, which classifies patients dichotomously as frail or nonfrail. In addition to the sociodemographic characteristics, covariates such as scores from the Mini-Mental State Examination, Instrumental Activities of Daily Living scale, and Cumulative Illness Rating Scale for Geriatrics and details regarding polymedication were collected. A multidimensional linear regression model was used for analysis.
Results
Almost 20% of participants had delirium (n=22), and 76.3% were classified as frail (n=87); 31.5% of the variance in the delirium score was explained by frailty (R2=0.315). Age; polymedication; scores of the Confusion Assessment Method (CAM), instrumental activities of daily living, and Cumulative Illness Rating Scale for Geriatrics; and frailty increased the predictability of the variance of delirium by 32% to 64% (R2=0.64).
Conclusion
Frailty is strongly related to delirium in older patients after discharge from the hospital.
Introduction
Delirium is a mental disorder with an acute onset and fluctuating course, characterized by disturbances of consciousness, orientation, memory, thought, perception, and behavior.Citation1 This syndrome represents a serious problem in acute care hospitals and is associated with decreased functional status, longer periods of time before recovery and discharge, institutionalization, premature mortality, and increased health care costs. The etiology of delirium is considered to be multifactorial, with an occurrence rate as high as 83% in hospitals.Citation2 Multicomponent delirium prevention strategies have been shown in intervention studies to consistently reduce the occurrence of delirium.Citation3 Based on this evidence base, the National Institute for Health and Care Excellence has advocated the adoption of multicomponent delirium prevention interventions into the routine care for older inpatients.Citation4 However, despite successful reductions in incident delirium by about a third, anticipated reductions in mortality or admissions to long-term care have not been conclusively observed.Citation5 One-third of older patients still have undetected and unresolved symptoms of delirium at hospital discharge.Citation6
Frailty is a geriatric condition characterized by diminished strength, endurance, and physiological functions that increase an individual’s vulnerability to adverse outcomes such as falls, sarcopenia, institutionalization, worsened disability, and premature death.Citation7 Frailty was recently defined as a state of increased vulnerability related to a poor level of homeostasis after a stressful event, with a corresponding increased risk of adverse outcomes, including falls, delirium, and disability.Citation7 Frailty has been linked to the development and progression of many age-related diseases and syndromes.Citation8
However, little is known about the relationship of frailty as a precipitating risk factor for specific geriatric syndromes in hospitalized older patients.Citation9 Frailty associated with hospitalization may occur in one-third of older patients and can be triggered even when the illness causing hospitalization is successfully treated.Citation7 Frailty has a considerable influence not only on outpatients’ independence and quality of life but also on their use of health care services.Citation10
Delirium and frailty appear to be distinct clinical geriatric conditions. However, in vulnerable older adults, both syndromes can appear simultaneously in response to a stressor.Citation9 Besides the elevated rates of delirium during hospitalization, studies have reported about the important consequences of frailty among older adults discharged from hospital, including increased dependence as shown on the Instrumental Activities of Daily Living (IADL) scale, weight loss, and cognitive impairment.Citation11 These consequences result from the acute syndrome of delirium itself and are also related to the management of patient care during hospitalization. They can lead to a state of severe frailty at discharge, with a high risk of premature death.Citation12
Delirium has been associated with increased long-term cognitive impairment and acceleration of existing cognitive decline. Furthermore, it may delay physical and cognitive recovery, ultimately resulting in new or increasing frailty and long-term disability and institutionalization. Both frailty and delirium in older patients can affect independent functioning and the ability to live at home.Citation9 A study on older patients who had undergone cardiac surgery and then developed postoperative delirium showed that delirium was associated with an approximately twofold increase in the risk of frailty after 1 month.Citation13 However, few studies have examined the relationship between frailty and delirium among older patients.Citation14,Citation15
Therefore, we hypothesized that delirium and frailty were associated in a sample of older adult patients discharged from a hospital.
Methods and materials
Data were sourced from a prospective clinical trial entitled “Effect estimation of an innovative nursing intervention to improve delirium among home-dwelling older adults,” which was conducted in 2012 and published elsewhere.Citation16 The trial protocol was approved by the cantonal medical ethics committee of Valais, Switzerland (CCVEM 030/11). Written informed consent was obtained from all participants or from their closest relatives if they scored <15 points on the Mini-Mental State Examination (MMSE).Citation17
Participants
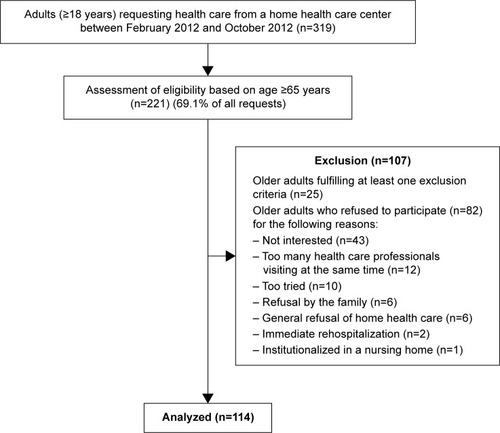
In the original study, a nonprobabilistic sample of 221 eligible participants was contacted within 48 hours of their hospital discharge, in collaboration with a home health care service, in order to request their participation. For different reasons, 107 older adults refused to participate, resulting in a final sample of 114 participants. Patients with a medical prescription for home health care were eligible to participate if they were 1) aged 65 years or older, 2) discharged after hospitalization of at least ≥48 hours, and 3) capable of understanding and answering questions in French. presents the recruitment procedure.
Figure 1 Recruitment of the participants.
Measurements
Assessment of delirium
Delirium was assessed using the validated French version of the Confusion Assessment Method (CAM).Citation18 The CAM is an instrument developed to assist clinicians in identifying patients with delirium. It has been considered suitable for bedside use.Citation19 The psychometric properties of the CAM have been documented as excellent, with 94% sensitivity, 89% specificity, and a Kappa’s inter-rater reliability between 0.70 and 1.00.Citation19 The research nurse or the principal investigator (PI) completed the CAM form based on a structured interview, patient records, and clinical observation of the symptoms/signs described in the CAM. Data were subsequently analyzed categorically by using the CAM algorithm. The inter-rater reliability between the PI and the research nurse (trained in CAM assessment) showed a satisfactory Kappa Cohen’s coefficient of 0.79.Citation20
Assessment of frailty
The frailty status was assessed using the Edmonton Frailty Score (EFS) developed by Rolfson et alCitation21 and been evaluated in a systematic review of de Vries et al.Citation22 This instrument consists of nine domains and eleven items, each scoring 0 points (frailty absent or normal health), 1 point (minor errors or mild/moderate impairment), or 2 points (important errors or severely impaired). The domains include cognitive impairment, autoevaluation of general health status, functional dependency, presence of social support, drug treatments and adherence, nutrition and mood, presence of incontinence, and the “timed up and go (TUG)” test. The TUG tests the basic mobility skills of frail elderly persons. It consists of a measurement of the time in seconds for a person to rise from sitting from a standard arm chair, walk 3 m, turn, walk back to the chair, and sit down. A cutoff score of ≥20 seconds was shown to predict falls in community-dwelling frail elderly people.Citation23
The total score from 0 to 3 points indicates no frailty; 4 or 5 points indicate prefrailty; 6 to 8 points indicates frailty; and 9 to 17 points indicates severe frailty. In order to dichotomize between frail and not frail, a score of 6 points or more was considered as frail. The eleven-item EFS has good psychometric properties and showed an acceptable Cronbach’s alpha of 0.62 in the present study.Citation21 The inter-rater reliability between the PI and the research nurse was excellent (Kappa Cohen’s coefficient =0.85).
Other variables
Sociodemographic characteristics assessed included age, sex, marital status, and level of education ().
Table 1 Sociodemographic characteristics of participants (n=114)
Cognitive level was assessed using the MMSE by regrouping the seven domains of cognitive functioning.Citation17,Citation24 The eleven-item instrument measures orientation, memory, language, and psychomotor skills. The sum of the scores varies from 0 (severe cognitive impairment) to 30 (no cognitive impairment). A score of <24 points was considered as the cutoff point for cognitive impairment. The MMSE was mostly assessed by the PI, and the instrument presents good psychometric proprieties.Citation25 An excellent inter-rater ratio was obtained between the PI and the research nurse with an intraclass correlation of 0.92.
Functional status was assessed using the Lawton Index of IADL, an assessment considered appropriate for older adults living at home.Citation26,Citation27 The IADL scale assesses independence versus dependence in more complex areas of daily living, such as using the telephone, shopping, preparing meals, cleaning and laundry, using public transport, management of medication and finances, and maintaining a home.Citation28 A score of <16 indicates that the patient is independent, as documented elsewhere.Citation28 Inter-rater reliability was excellent (Kappa Cohen’s coefficient =0.85). Finally, comorbidities were assessed using the Cumulative Illness Rating Scale for Geriatrics (CIRS-G). The CIRS-G scores diseases in 13 organ systems and grades each organ according to severity using explicit rules for classification. Data for CIRS-G scoring were compiled from comprehensive patient interview and chart records. A CIRS-G index of comorbidity of ≥2 implies the presence of moderate and severe illnesses.Citation29 Inter-rater scores between the PI and the research nurse were very high (Pearson’s correlation =0.81). The number of prescribed medications was recorded during patient interviews and through patient records. Participants’ health status and average medication use are presented in .
Table 2 Health status of participating delirious and nondelirious discharged older adults
Data collection
After the participants had given their consent, data were collected during a single home visit within 48 hours of discharge from the hospital. During the home visits, the data collection procedure was standardized to avoid any bias by using an invariable sequence of questions. Data on delirium, frailty, cognition, health status, comorbidities, and medication treatment were collected immediately after consent of the patients at their place they live. It is important to mention that during hospitalization and at hospital discharge, no delirium of frailty assessment was done. A detailed description of the data collection procedure has been published elsewhere.Citation16
Statistical analyses
Sociodemographic and baseline characteristics of subjects with and without frailty were compared using the Student’s t-test for continuous variables and a chi-squared distribution for categorical ones. The odds ratio (OR) of delirium/frailty was calculated using a contingency table in a joint frequency distribution. The association between delirium and frailty was assessed using linear regression, and this association was adjusted for age, cognitive state (MMSE), physical state (IADL), chronic conditions reported (CIRS-G), and polymedication. Collinearity was verified using a matrix correlation and tolerance values.Citation30 All statistical tests were performed using the IBM-Statistical Package for the Social Sciences (IBM-SPSS®), Version 22.Citation31 Statistical significance was set at P=0.05, and all tests were two tailed.
Results
Participant characteristics
No statistically significant differences were found between men and women with regard to being nondelirious or delirious (P=0.612) and their ages (P=0.875; ). Similarly, there were no statistically significant differences with regard to being frail and nonfrail (P=0.560) and their ages (P=0.742; ).
Table 3 Health status among frail and nonfrail discharged older adults
Prevalence of delirium and frailty
Almost one-fifth of the sample (n=20) presented with delirium as measured by the CAM. Almost two-thirds of the frail older adults presented with three or more symptoms of delirium (). Three quarters of participants (n=89) presented with frailty, including 90% of the delirious participants (n=18). The mean frailty score for nondelirious participants was significantly lower than that for delirious participants (P<0.001; ).
Measurements of IADL at hospital discharge showed statistically significant differences in dependency: nonfrail participants were less dependent than frail ones (P<0.001), and nondelirious participants were less dependent than delirious ones (P=0.029). Similar statistical differences were observed. With regard to cognitive status, nonfrail participants had a better cognitive status than frail ones (P=0.002), and nondelirious participants had a better cognitive status than delirious ones (P<0.001). Most of the participants had comorbidities and were being prescribed more than four medications. A significant difference was observed in the comorbidity rates and the average number of medications of frail and nonfrail participants (P=0.019), but the difference was not significant between nondelirious and delirious participants (P=0.997; and ).
The high prevalence of frailty among delirious participants reflects the fact that in four of the eleven EFS items – namely cognitive impairment, medication adherence problems, incontinence, and the “timed up and go” test – the scores significantly increased in delirious participants compared to nondelirious participants (P≤0.001, P=0.018, P=0.004, and P=0.041, respectively; ).
Table 4 Distribution of EFS items in delirious and nondelirious discharged older adults
Association between frailty and delirium
The OR of delirium/frailty indicated that frailty was 1.19 times more present (statistically significant) among participants with delirium than among participants without delirium, with a 95% confidence interval (95% CI) of 1.00–1.43. Cognitive status (MMSE) seemed to be a stronger risk factor for delirium than frailty, with an OR of 4.31 (95% CI [1.51–12.28]). Neither IADL (OR 1.13; 95% CI [0.91–1.41]), age (OR 1.12; 95% CI [0.43–2.96]), and CIRS-G (OR 1.04; 95% CI (0.58–1.89]) nor polymedication (OR 1.03; 95% CI [0.34–3.14]) were significant risk factors for delirium.
Linear regression indicated that 32% of the variance in delirium was explained by frailty alone (R2=0.315; P<0.001), thus suggesting that frailty could be strongly associated.Citation32 Being frail explained one-third of the presence of delirium in participants. In a multiple regression model, including age, cognitive and physical state, polymedication, and comorbidities, 64% of the variance in delirium could be explained by these variables (adjusted R2=0.635; P≤0.001; ).
Table 5 Simultaneous multiple regression analysis summary for age, polymedication, frailty, physical and cognitive impairment, and comorbidity
No collinearity was found between frailty scores, CAM scores (T-B Kendall =−0.130; variance inflation factor <10), IADL scores (r=0.44; variance inflation factor <10), and MMSE scores (r=0.45; variance inflation factor <10).Citation33
Discussion
Our results indicate that frailty is strongly associated with delirium in older patients as one-fifth of the participants presented delirium at hospital discharge.Citation2 Nine of ten delirious participants were frail, whereas only three quarters of the nondelirious participants were frail. These findings are consistent with those of other recent studies indicating an elevated prevalence of frailty among discharged older adults with delirium.Citation34,Citation35 However, our study results do not allow to explain this association, and it has recently been mentioned by Teale and Young that the underlying interaction between these two geriatric syndromes is poorly understood.Citation5
Almost all the participants had some functional impairment, and a third of participants presented a significant cognitive impairment at discharge, which corroborates results from other recent studies.Citation36 This highlighted an urgent need for health care owing to a high number of hospitalized older patients presenting several symptoms of frailty. In addition, as already documented elsewhere, discharged older patients face a risk of delirium due to the presence of multifactorial delirium risk factors.Citation37 Some studies have observed a strong relationship between delirium and physical decline, as manifested by an elevated number of hospital-related falls. However, the present study was unable to confirm this relationship, as hospital records concerning adverse events during hospitalization, such as falls and other deleterious events, were incomplete.Citation38 As in other studies, our results showed no association between age and frailty within the cohort.Citation8
In the present study, frailty alone is associated with delirium in more than one-third of cases. In a more complex model – including age, physical and cognitive impairment, polymedication, and polymorbidity – the association of delirium increased, having an impact in up to two-thirds of cases. Thus, cognitive screening alone was more strongly related to delirium than frailty, but cognitive and frailty screening together was even better. These findings confirm that comprehensive geriatric assessment (CGA) and screening for frailty increase early detection of delirium and delirium risks in discharged older adults. Above all, hospitalization itself should be considered as an important delirium and frailty risk factor. Interdisciplinary preventive care strategies focusing on limiting physical and cognitive decline during hospitalization may be effective in averting delirium and frailty and other poor posthospitalization outcomes.Citation39 Health care reforms focusing on building more effective and efficient care models for older inpatients are urgently needed to develop “senior-friendly” hospitals, including specialized geriatric care units.
Although the delirium rate among our participants was consistent with other studies, the prevalence of frailty was less easy to compare.Citation35 The challenges of detecting delirium in patients after hospital discharge are well described, in contrast to frailty where prevalence is more dependent on the measurement scale.Citation40 In the present study, delirium detection and frailty assessment were combined within clinical assessment and routinely collected data; they could be determined for all patients, regardless of their cognitive or functional abilities, thus increasing their potential utility in the clinical setting. The presence of both frailty and delirium confer a particularly poor prognosis, such as dependency, institutionalization, or even premature death.Citation15,Citation41 However, as delirium and frailty are both viewed as modifiable geriatric syndromes and given the current trend for moving health care out of the hospital into the home, this raises important questions about patient care management.Citation7 Nevertheless, there are links between delirium and frailty.Citation42,Citation43 Although frailty is a chronic condition and delirium is a more acute condition, the unavoidable question of a common pathophysiological mechanism persists. Frailty and delirium may be different clinical expressions of a shared vulnerability to stress in older adults, and future research should determine whether this vulnerability is age related, pathological, genetic, environmental, or most likely, a combination of all of these factors.Citation44 Besides the fact that both syndromes represent significant sources of morbidity and mortality for older adults, both of them are multifactorial, with risk factors and potentially causative mechanisms (eg, inflammation, atherosclerosis, and poor nutrition) that overlap.Citation7 Although there are proven measures for preventing delirium, evidence regarding interventions to improve outcomes following delirium remains uncertain.Citation2,Citation39 Similarly, while complex interventions such as education, optimized nutrition, and exercise have been suggested for delaying or preventing frailty, there is as yet no evidence that such interventions can mitigate these outcomes in frail older inpatients.Citation45,Citation46 Whether multicomponent, nonpharmacological, interdisciplinary interventions are effective in preventing frailty and delirium in hospitalized older adult patients should be the focus of further inquiry. Further research on a larger group of discharged older adults is also required.
Finally, this study has both strengths and limitations. The first strength was the comprehensive geriatric assessment approach used, involving patient records, clinical and CAM assessment after discharge, and optimized delirium detection and frailty assessment. Another strength was that all the participants were accurately screened for their health status and frailty indicators, and they were discriminated by the presence of delirious or nondelirious symptoms.
In addition to the relatively small sample group, it seems important to mention the limiting factor that data were collected at a single hospital site, and thus generalization of these results needs caution. Furthermore, comprehensive geriatric assessment data from the emergency department was incomplete, and therefore we could not make a precise interpretation of participants’ mental status at hospital admission. Another limitation of the study concerns the correctional nature of the data. Using the EFS did impose some methodological limits to the study, as the most widely used screening tool to assess frailty is that proposed by Fried et al.Citation47 This requires the presence of at least three of the five following criteria: weight loss, exhaustion, weak grip strength, slow walking speed, and low physical activity. However, exhausted older inpatients, once discharged, are often unable to complete these performance-based tests, and thus many of the participants in the present study could not have been assessed using such physical testing.
The syndromes of delirium and frailty are highly associated in discharged older adults. However, currently, detecting their delirium remains problematic for several reasons. On the other hand, assessing frailty, either through systematic CGA or by using specific frailty-detection tools, gives health care professionals the opportunity to improve the effectiveness of primary prevention strategies for delirium, by promptly ascertaining which discharged older adults are at a high risk of presenting with that syndrome.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
We thank the patients and their families for their participation in this study. This work would not have been possible without the input of Ms Ariane Kapps, a Master of Science student who helped to develop the intervention, as well as that of all the participating nurses of the Home Health Care Service of Valais. The authors also thank Ms Sylvana Gerber for her contribution to successful data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders, Fifth EditionWashington DCAmerican Psychiatric Publishing2013
- InouyeSKWestendorpRGSaczynskiJSDelirium in elderly peopleLancet2014383992091192223992774
- Holroyd-LeducJMKhandwalaFSinkKMHow can delirium best be prevented and managed in older patients in hospital?CMAJ2010182546547019687107
- HoltRYoungJHeseltineDEffectiveness of a multi-component intervention to reduce delirium incidence in elderly care wardsAge Ageing201342672172723978407
- TealeEAYoungJRMulticomponent delirium prevention interventions: not as effective as NICE suggest?Age and Ageing201544691591726316509
- McAvayGJVan NessPHBogardusSTJrOlder adults discharged from the hospital with delirium: 1-year outcomesJ Am Geriatr Soc20065481245125016913993
- CleggAYoungJIliffeSRikkertMORockwoodKFrailty in elderly peopleLancet2013381986875276223395245
- SantangeloATestaiMMaugeriDDelirium is marker of frailty? Study in a population over 90-year old recovered in a Sicilian RSAEur Psychiatry201025588
- QuinlanNMarcantonioERInouyeSKGillTMKamholzBRudolphJLVulnerability: the crossroads of frailty and deliriumJ Am Geriatr Soc201159suppl 2S262S26822091571
- Abellan Van KanGVellasBIs the mini nutritional assessment an appropriate tool to assess frailty in older adults?J Nutr Health Aging201115315916121369660
- BuurmanBMHoogerduijnJGvan GemertEAde HaanRJSchuurmansMJde RooijSEClinical characteristics and outcomes of hospitalized older patients with distinct risk profiles for functional decline: a prospective cohort studyPLoS One201271e2962122238628
- CleggAYoungJThe frailty syndromeClin Med20111117275
- LeungJMTsaiTLSandsLPBrief report: preoperative frailty in older surgical patients is associated with early postoperative deliriumAnesth Analg201111251199120121372278
- PolRAvan LeeuwenBLVisserLIzaksGJvan den DungenJJAMTielliuIFJStandardised frailty indicator as predictor for postoperative delirium after vascular surgery: a prospective cohort studyEur J Vasc Endovasc Surg201142682483021810543
- LeungJMTsaiTLSandsLPPreoperative frailty in older surgical patients is associated with early postoperative deliriumAnesth Analg201111251199120121372278
- VerlooHGouletCMorinDvon GuntenAEffect estimation of an innovative nursing intervention to improve delirium among home-dwelling older adults: a randomized controlled pilot trialDement Geriatr Cogn Dis Extra20155117619026034489
- FolsteinMFFolsteinSEMcHughPR“Mini-mental state”. A practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res19751231891981202204
- LaplanteJColeMGMcCuskerJSinghSOuimetMAConfusion assessment method. Validation of a French-language versionPerspect Infirm200531122017312661
- WeiLAFearingMASternbergEJInouyeSKThe confusion assessment method: a systematic review of current usageJ Am Geriatr Soc200856582383018384586
- HairJKJBlackWCBabinBJAndersonREMultivariate Data Analysis: A Global Perspective7th edBostonPearson Education Inc2010
- RolfsonDBMajumdarSRTsuyukiRTTahirARockwoodKValidity and reliability of the Edmonton Frail ScaleAge Ageing2006652652916757522
- de VriesNMStaalJBvan RavensbergCDHobbelenJSMOlde RikkertMGMNijhuis-van der SandenMWGOutcome instruments to measure frailty: a systematic reviewAgeing Res Rev201110110411420850567
- PodsiadloDRichardsonSThe timed up & go: a test of basic functional mobility for frail elderly personsJ Am Geriatr Soc1991391421481991946
- DerouesnéCPoitreneauJHugonotLKalafatMDuboisBLaurentBLe mini-mental state examination (MMSE): un outil pratique pour l’évaluation de l’état cognitif des patients par le clinicien, version française consensuelle. [Mini mental state Exam: a practical tool for clinicians to assess the cognitive state of patients, French consensual version]La Presse Médicale1999282111411148 French10399508
- NaugleRIKawczakKLimitations of the mini-mental state examinationCleve Clin J Med19895632772812743549
- LawtonMPBrodyEMAssessment of older people: self-maintaining and instrumental activities of daily livingGerontologist1969931791865349366
- BuurmanBMvan MunsterBCKorevaarJCde HaanRJde RooijSEVariability in measuring (instrumental) activities of daily living functioning and functional decline in hospitalized older medical patients: a systematic reviewJ Clin Epidemiol201164661962721074969
- Barberger-GateauPCommengesDGagnonMLetenneurLSauvelCDartiguesJFInstrumental activities of daily living as a screening tool for cognitive impairment and dementia in elderly community dwellersJ Am Geriatr Soc19924011112911341401698
- MillerMDParadisCFHouckPRRating chronic medical illness burden in geropsychiatric practice and research: application of the Cumulative Illness Rating ScalePsychiatry Res19924132372481594710
- TabachnickBGFidellLSUsing Multivariate Statistics6th edBostonPearson Education Inc2013
- IBM-SPSSStatistical Package for Social SciencesSomer, NYIBM Corporation2011
- CohenJStatistical Power and Analysis for the Behavioral Sciences2nd edHillsdale, NYLawrence ERdbaum Associates1988
- MasonCHPerreaultWDJrCollinearity, power, and interpretation of multiple regression analysisJ Market Res1991283268280
- EelesEMPPeelNMWhiteSVO’MahonyMSBayerAJBhatRFrailty and illness severity in relation to delirium in older inpatientsAustralas J Ageing20133228
- JoostenEDemuynckMDetroyerEMilisenKPrevalence of frailty and its ability to predict in hospital delirium, falls, and 6-month mortality in hospitalized older patientsBMC Geriatr201414124393272
- HoogerduijnJGBuurmanBMKorevaarJCGrobbeeDEde RooijSESchuurmansMJThe prediction of functional decline in older hospitalised patientsAge Ageing201241338138722378613
- CovinskyKEPierluissiEJohnstonCBHospitalization-associated disability: “she was probably able to ambulate, but I’m not sure”J Am Med Assoc20113061117821793
- WitloxJEurelingsLSMde JongheJFMKalisvaartKJEikelenboomPvan GoolWADelirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysisJ Am Med Assoc20103044443451
- CameronIFairhallNGillLLockwoodKLangronCAggarCDeveloping interventions of frailtyAdv Geriatr20152015845356
- CleggAWestbyMYoungJBUnder-reporting of delirium in the NHSAge Ageing201140228328621169280
- EelesEMPWhiteSVO’MahonySMBayerAJHubbardREThe impact of frailty and delirium on mortality in older inpatientsAge Ageing201241341241622391613
- AndrewMKLe capital social et la santé des personnes âgées. [Social capital and healthy aging]Retraite et Société200546132145 French
- AgostiniJVZhangYInouyeSKUse of a computer-based reminder to improve sedative-hypnotic prescribing in older hospitalized patientsJ Am Geriatr Soc2007551434817233684
- BergmanHFerrucciLGuralnikJMHoganDBHummelSKarunananthanSFrailty: an emerging research and clinical paradigm – issues and controversiesJ Gerontol A Biol Sci Med Sci200762773173717634320
- OoMTTenchevaAKhalidNChanYPHoSFAssessing frailty in the acute medical admission of elderly patientsJ R Coll Physicians Edinb201343430130824350311
- TurnerGCleggABest practice guidelines for the management of frailty: a British Geriatrics Society, age UK and Royal College of General Practitioners reportAge Ageing201443674474725336440
- FriedLPTangenCMWalstonJNewmanABHirschCGottdienerJFrailty in older adults: evidence for a phenotypeJ Gerontol A Biol Sci Med Sci2001563M146M15611253156