
Abstract
Objective
Currently, the association between abdominal aortic plaques and coronary artery disease (CAD) has not yet been clarified clearly. The purpose of this study was to determine the prevalence of abdominal aortic plaques by ultrasound imaging and to explore its association with CAD in patients undergoing coronary angiography.
Methods
Between October 2014 and June 2015, a prospective study was conducted in the Department of Cardiology at Guangdong General Hospital, Guangzhou, People’s Republic of China. Ultrasound scanning of the abdominal aortas was performed in 1,667 consecutive patients undergoing coronary angiography. Clinical characteristics and coronary profile were collected from the patients.
Results
Of the 1,667 study patients (male, 68.9%; mean age, 63±11 years) undergoing coronary angiography, 1,268 had CAD. Compared with 399 patients without CAD, 1,268 patients with CAD had higher prevalence of abdominal aortic plaques (37.3% vs 17%, P<0.001). In multivariate analysis, abdominal aortic plaques served as independent factors associated with the presence of CAD (odds ratio =2.08; 95% confidence interval =1.50–2.90; P<0.001). Of the 1,268 patients with CAD, the prevalence of abdominal aortic plaques was 27.0% (98/363) in patients with one-vessel disease, 35.0% (107/306) in patients with two-vessel disease, and 44.7% (268/599) in patients with three-vessel disease. Stepwise increases in the prevalence of abdominal aortic plaque was found depending on the number of stenotic coronary vessels (P<0.001; P-value for trend <0.001). In an ordinal logistic regression model, abdominal aortic plaques served as independent factors associated with the severity of CAD according to the number of stenotic coronary vessels (P<0.001).
Conclusion
The prevalence of abdominal aortic plaques was higher in patients with CAD than in those without CAD. Abdominal aortic plaque was an independent factor associated with the presence and severity of CAD.
Introduction
Atherosclerotic disease is a main cause of severe cardiovascular events, such as myocardial infarction and stroke. As the prevalence of atherosclerosis increases globally due to aging population, identifying atherosclerotic plaques will be of utmost importance for early diagnosis and intervention, which will substantially decrease the health care burden.Citation1
Evidence is available indicating that subclinical atherosclerosis in carotid artery is associated with the presence and severity of coronary artery disease (CAD) and with an increased 10-year risk of cardiovascular events.Citation2–Citation5 The association between thoracic aortic plaques and CAD has been often reported by using transesophageal echocardiography.Citation6,Citation7 Furthermore, researchers found that the extent of thoracic aortic atheroma burden was independently associated with increased long-term mortality in patients following cardiothoracic surgery.Citation8 Although autopsy studies reported plaques in the abdominal aorta to be severe in patients with cardiac catastrophe,Citation9 there are limited studies showing the association between CAD and abdominal aortic plaques. Only a small number of observational studies reported that the prevalence and extents of plaques in abdominal aortas were greater in patients with CAD than in those without CAD by using cardiovascular magnetic resonance (CMR). But they reported that plaques in abdominal aorta were not independent factors for CAD.Citation9–Citation11 Besides, due to lack of large-scale data, the results of these studies may not be convictive. Although CMR was a useful tool for evaluating atherosclerotic plaques in abdominal aortas,Citation12 it is neither cost efficient nor suitable for population-based studies.
The 2014 ESC guidelines recommend that population screening for abdominal aortic aneurysm (AAA) should be performed by abdominal aorta ultrasound in all men >65 years of age.Citation13 Abdominal aorta ultrasound has become a useful tool to not only screen AAA but also evaluate atherosclerotic plaques, which is noninvasive, easy to assess, cost efficient, and could be routinely used in population-based study.Citation1 However, the significance of abdominal aortic plaques detection by ultrasound imaging is not yet definitive.
The association between CAD and abdominal aortic plaques has not yet been clarified clearly. The purpose of the present study was to determine the prevalence of abdominal aortic plaques by ultrasound imaging and to explore its association with CAD in patients undergoing coronary angiography.
Subjects and methods
Study patients
Between October 2014 and June 2015, a prospective study was conducted in the Department of Cardiology at Guangdong General Hospital, Guangzhou, People’s Republic of China. The study was approved by the ethics committees of Guangdong General Hospital. Abdominal aortic ultrasound is a routine examination in patients undergoing coronary angiography in our hospital. As this was an observational study, written informed consent was not required according to the policy of the ethics committees of Guangdong General Hospital. Ultrasound scanning of the abdominal aortas was performed in 1,667 consecutive patients undergoing coronary angiography for suspected or known CAD, or prior to valve surgery. Excluded were patients with aortic diseases, congenital heart disease, infectious diseases, autoimmune diseases, or neoplasma. The clinical characteristics of the patients and their coronary profile were collected prospectively.
Coronary angiography
Coronary angiography was performed using a standard technique. Obstructive CAD was defined as the existence of astenosis >50% of the lumen diameter of at least one major coronary vessel. The severity of the disease referred to the number of identified stenosed vessels (lumen diameter <50%) [one-, two-, or three-vessel disease]) and was evaluated by two experienced cardiologists, who were blinded to the ultrasound evaluation of the abdominal aortas.Citation3
Assessment of abdominal aortic atherosclerosis
Atherosclerosis of the abdominal aortas was assessed by ultrasound scanning with a ultrasound device equipped with a Philips iE 33 imager with a 3.5/7 MHz multiplane probe. All studies were recorded and were reviewed offline by two independent senior echocardiographers who were blinded to patient demographics as well as to coronary profile. A third expert was advised in case of disagreement, and the majority view was adopted.
Abdominal aortic intimal morphology was graded by a modification of the classification proposed by Pitsavos et al;Citation14 thus, atherosclerotic plaque characteristics and maximum width were graded as follows: grade I, normal intima; grade II, increased intimal echo density without lumen irregularity; grade III, increased intimal echo density with single or multiple well-defined atheromatous plaque ≤3 mm; and grade IV, atheroma >3 mm or mobile or ulcerated plaque. Each patient was characterized on the basis of the most severe identified lesion. Grades III and IV were considered to represent abdominal aortic plaque.Citation15
Evaluation of risk factor variables
The risk factor variables evaluated in the present study included age, sex, smoking, hypertension, diabetes mellitus, chronic kidney disease, triglyceride, total cholesterol, low density lipoprotein-cholesterol (LDL-C), and high density lipoprotein-cholesterol (HDL-C).
Hypertension was defined as present if there was any history of high blood pressure or if the blood pressure measured twice in the hospital exceeded 140 mmHg (systolic) or 90 mmHg (diastolic) or in case of current use of antihypertensive medications.
Diabetes mellitus was defined as present if the patient had a history of diabetes or if the fasting plasma glucose exceeded 7.0 or 11.1 mmol/L 2 hours after a meal or in case of current use of diabetic medications.
Chronic kidney disease was defined as present if the estimated glomerular filtration rate (eGFR) was less than 60 mL/min/1.73m2. The eGFR (expressed as mL/min/1.73 m2) was computed using a prediction formula derived from the Modification of Diet in Renal Disease study:Citation16 eGFR =186 × (serum creatinine−1.154) × (age−0.203) × 0.742 (if female).
Blood samples measured by standard laboratory methods were taken in a fasting state on the morning of the day when angiography was performed.
Statistics
Quantitative data are presented as mean ± standard deviation (SD) and qualitative data are presented as frequencies. Differences between two groups were evaluated by the unpaired t-test for parametric variables and by the chi-square test for categorical variables. A multiple logistic regression analysis was used to elucidate the associations between abdominal aortic plaque and CAD. An ordinal logistic regression analysis was used to elucidate the associations between abdominal aortic plaque and the severity of CAD. A P-value of <0.05 was considered statistically significant. All the statistical analyses were made with the SPSS for Windows software, version 20.0 (IBM Corporation, Armonk, NY, USA).
Results
Prevalence of abdominal aortic plaques in patients with CAD
Of the 1,667 study patients (male, 68.9%; mean age, 63±11 years) undergoing coronary angiography, 1,268 had CAD (>50% stenosis). Compared with 399 patients without CAD, 1,268 patients with CAD had higher prevalence of abdominal aortic plaque (37.3% vs 17%; P<0.001). Other clinical characteristics in patients with and without CAD are displayed in .
Table 1 Clinical characteristics in patients with and without CAD
Factors associated with the presence of CAD
To identify any independent factor associated with the presence of CAD, clinical variables (age, sex, smoking, hypertension, diabetes mellitus, chronic kidney disease, triglyceride, total cholesterol, LDL cholesterol, HDL cholesterol, abdominal aortic plaque) were entered into a multivariate logistic regression model. In multivariate analysis, male sex (odds ratio [OR] =2.45; 95% confidence interval [CI] =1.76–3.41; P<0.001), diabetes mellitus (OR =1.54; 95% CI =1.09–2.17; P=0.014), and abdominal aortic plaque (OR =2.08; 95%CI =1.50–2.90; P<0.001) were independent factors associated with the presence of CAD ().
Table 2 Factors associated with the presence of CAD (multiple logistic regression analysis of the 1,667 study patients)
Prevalence of abdominal aortic plaques according to the coronary profile
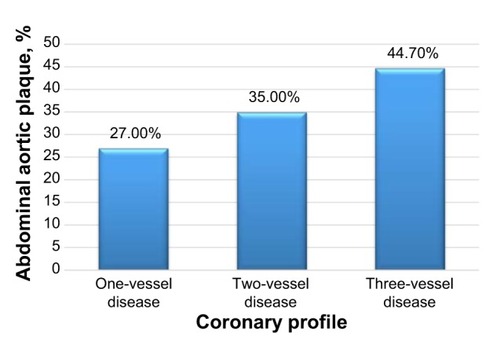
Of the 1,268 patients with CAD, 363 had one-vessel disease, 306 had two-vessel disease, and 599 had three-vessel disease. The prevalence of abdominal aortic plaques was 27.0% (98/363) in patients with one-vessel disease, 35.0% (107/306) in patients with two-vessel disease, and 44.7% (268/599) in patients with three-vessel disease. As shown in , stepwise increases in the prevalence of abdominal aortic plaque were found to depend on the number of stenotic coronary vessels (P<0.001; P-value for trend <0.001).
Figure 1 Prevalence of abdominal aortic plaque according to the coronary profile.
Factors associated with the severity of CAD
To identify any independent factor associated with the severity of CAD according to the number of stenotic coronary vessels, clinical variables (age, sex, smoking, hypertension, diabetes mellitus, chronic kidney disease, triglyceride, total cholesterol, LDL-cholesterol, HDL-cholesterol, and abdominal aortic plaque) were entered into an ordinal logistic regression model. In multivariate analysis, diabetes mellitus, chronic kidney disease, LDL-cholesterol, HDL-cholesterol, and abdominal aortic plaque were the independent factors associated with the severity of CAD ().
Table 3 Factors associated with the severity of CAD (ordinal logistic regression analysis of the 1,268 study patients with CAD)
Discussion
Atherosclerosis is a generalized, progressive disease that may simultaneously affect several arterial trees of the body, such as carotid arteries, femoral arteries, and popliteal arteries.Citation3,Citation17 Subclinical atherosclerosis can be noninvasively identified and analyzed to provide prognostic information beyond that provided by traditional cardiovascular risk factors alone as well as to show the cumulative effect of all risk and susceptibility factors.Citation18 Due to the increasing trend of cardiovascular and cerebrovascular events in many patient populations, the identification and analysis of subclinical atherosclerosis are of utmost importance for the reduction of these severe events.
Carotid atherosclerosis as shown on ultrasound, aortic atherosclerosis detected by ultrasound, and lower extremity atherosclerosis reflected by the ankle-brachial index are validated measures of atherosclerosis that are routinely used in population-based studies because they are relatively cheap, noninvasive, easy to assess, and cost efficient.Citation18–Citation21 Currently, noninvasive imaging modalities for aortic atherosclerotic plaque detection include ultrasound, computed tomography, magnetic resonance imaging, and angiography.Citation1
The association between CAD and thoracic aortic plaques has often been reported by using transesophageal echocardiography.Citation6,Citation7 Several studies indicated that thoracic plaques may be more strongly associated with CAD than carotid or femoral artery plaques detected by ultrasonography and to be associated with cardiovascular events.Citation9,Citation22 Although autopsy study reported plaques in the abdominal aorta, but not in the thoracic aorta, to be severe in patients with cardiac catastrophe,Citation9 there are limited studies showing the association between CAD and abdominal aortic plaques. Kazuhiro Ashida et al reported that the prevalence and extents of plaques in both the thoracic and abdominal aortas were greater in patients with CAD than in those without CAD by using CMR. But they reported that plaque in abdominal aorta was not an independent factor for CAD.Citation9–Citation11 Although CMR was a useful tool for evaluating atherosclerotic plaques in both the thoracic and abdominal aortas,Citation12 it is neither convenient nor cost efficient. In consequence, CMR may not be routinely used in population-based studies for detection of aortic plaques.
The association between CAD and abdominal aortic plaques has not yet been clarified clearly. Ultrasound imaging has become a useful tool for evaluating atherosclerotic plaques in abdominal aortas, which is relatively cheap, noninvasive, easy to assess, and cost efficient. In the present study, we used ultrasound imaging to determine the prevalence of abdominal aortic plaques and to explore its association with CAD in patients undergoing coronary angiography. The prevalence of abdominal aortic plaques was higher in patients with CAD than those without CAD. In multivariate analysis, abdominal aortic plaque was an independent factor associated with the presence of CAD. Stepwise increases in the prevalence of abdominal aortic plaque were found to depend on the number of stenotic coronary vessels. Abdominal aortic plaque was an independent factor associated with the severity of CAD.
In our study, we tried to clarify the association between subclinical arterial wall changes in abdominal aortas and the presence and severity of CAD. According to our results, abdominal aortic plaque was found to be an independent factor associated with the presence and severity of CAD. Although atherosclerosis mainly manifests itself in medium-sized vessels, it is also present in the great vessels, such as the abdominal aorta and the carotidartery.Citation15 The pathway from risk factors to clinical disease is probably through the development of a subclinical state. Therefore, the identification of these subclinical states may provide a very important marker for the effects of risk factors on the cardiovascular system among relatively asymptomatic individuals. The 2014 ESC guidelines on the diagnosis and treatment of aortic diseases recommended that population screening for AAA should be performed by abdominal aorta ultrasound in all men >65 years of age (Class I, Level A).Citation13 Our study found that abdominal aorta ultrasound can not only detect AAA but also abdominal aortic plaque, which was an independent factor associated with the presence and severity of CAD. Researchers found that the extent of thoracic aortic atheroma burden was independently associated with increased long-term mortality in patients following cardiothoracic surgery.Citation8 This is an attractive hypothesis that this relationship is not limited to patients after surgery, but describes general atherosclerotic disease patterns of the aorta, with impact for prevention of cardiovascular events. Identifying abdominal aortic plaques will be of utmost importance for early diagnosis and intervention of CAD, which will reduce severe cardiovascular events in turn.
Limitations
There were several limitations in this study. First, our study population was Chinese patients undergoing angiography, who are generally considered to be a highly selected population at high risk for CAD. Because of this selection bias, our results may not be applicable to the general or other ethnic populations. Therefore, screening for abdominal aortic atherosclerosis in an asymptomatic population is necessary. Second, atherosclerosis varies in severity depending on multiple features that contribute to plaque progression and “stability”. Plaque instability has been confirmed as a main cause of acute coronary syndrome.Citation23 Due to the technical limitations of ultrasound imaging, we cannot assess the stability of abdominal aortic plaque and its association with coronary plaque instability. Recently, researchers have found that targeted fluorescence activatable cell-penetrating peptides (ACPPs) probes distinguished disrupted plaques from stable plaques with high sensitivity and specificity in an animal model. The combination of anatomic, magnetic resonance imaging – derived predictors for disruption and ACPP uptake can further improve the power of identifying high-risk plaques.Citation24 With the recent development in technology, it is possible and necessary to further assess the stability of abdominal aortic plaques and their association with CAD. Third, ultrasound imaging was used to evaluate abdominal aortic plaques, but coronary angiography was used to evaluate coronary atherosclerosis, which cannot visualize plaques, and it only shows lumen characteristics. Our current study cannot elucidate the associations of abdominal aortic plaques with coronary artery plaques. Fourth, atherosclerosis is a systemic disease affecting not only the coronary and carotid arteries but also the thoracic and abdominal aorta and the lower extremities. Our present study focused only on abdominal aortic atherosclerosis and CAD.
Conclusion
In conclusion, the prevalence of abdominal aortic plaques was higher in patients with CAD than those without CAD. Abdominal aortic plaque was an independent factor found to be associated with the presence and severity of CAD.
Author contributions
WL, SL, and JL conceived, designed, and performed the study; analyzed and interpreted data; and drafted the paper. YL, WH, and JC designed the study, analyzed and interpreted data, and drafted the paper.
Acknowledgments
This study was supported by the Guangdong Provincial Public Research and Capacity Building Foundation, People’s Republic of China (No. 2014A020215023) and Science and Technology Program of Guangzhou, People’s Republic of China (No. 201300000180).
Disclosure
The authors report no conflicts of interest in this work.
References
- LuYWeiJShaoQAssessment of atherosclerotic plaques in the rabbit abdominal aorta with interleukin-8 monoclonal antibody-targeted ultrasound microbubblesMol Biol Rep2013403083309223292075
- Barrett-ConnorELaughlinGAConnorCCoronary artery calcium versus intima-media thickness as a measure of cardiovascular disease among asymptomatic adults (from the Rancho Bernardo Study)Am J Cardiol20079922723117223423
- KafetzakisAKochiadakisGLaliotisAAssociation of subclinical wall changes of carotid, femoral, and popliteal arteries with obstructive coronary artery disease in patients undergoing coronary angiographyChest20051282538254316236920
- BelcaroGNicolaidesANRamaswamiGCarotid and femoral ultrasound morphology screening and cardiovascular events in low risk subjects: a 10-year follow-up study (the CAFES-CAVE study(1))Atherosclerosis200115637938711395035
- KrogerKLehmannNRappaportLCarotid and peripheral atherosclerosis in male marathon runnersMed Sci Sports Exerc2011431142114721200345
- AgmonYKhandheriaBKMeissnerIRelation of coronary artery disease and cerebrovascular disease with atherosclerosis of the thoracic aorta in the general populationAm J Cardiol20028926226711809426
- MatsumuraYTakataJYabeTFurunoTChikamoriTDoiYLAtherosclerotic aortic plaque detected by transesophageal echocardiography: its significance and limitation as a marker for coronary artery disease in the elderlyChest199711281869228361
- KurraVLieberMLSolaSExtent of thoracic aortic atheroma burden and long-term mortality after cardiothoracic surgery: a computed tomography studyJACC Cardiovasc Imaging201031020102920947047
- AshidaKMomiyamaYFayadZAMagnetic resonance evaluation of the associations of thoracic and abdominal aortic plaques with the presence and extent of coronary artery stenosisJ Cardiovasc Magn Reson2007985586118066744
- TaniguchiHMomiyamaYFayadZAIn vivo magnetic resonance evaluation of associations between aortic atherosclerosis and both risk factors and coronary artery disease in patients referred for coronary angiographyAm Heart J200414813714315215803
- MomiyamaYKatoRFayadZAA possible association between coronary plaque instability and complex plaques in abdominal aortaArterioscler Thromb Vasc Biol20062690390916424346
- WorthleySGHelftGFusterVHigh resolution ex vivo magnetic resonance imaging of in situ coronary and aortic atherosclerotic plaque in a porcine modelAtherosclerosis200015032132910856524
- ErbelRAboyansVBoileauC2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC)Eur Heart J2014352873292625173340
- PitsavosCEAggeliKIBarbetseasJDEffects of pravastatin on thoracic aortic atherosclerosis in patients with heterozygous familial hypercholesterolemiaAm J Cardiol199882148414889874052
- KallikazarosIETsioufisCPStefanadisCIPitsavosCEToutouzasPKClosed relation between carotid and ascending aortic atherosclerosis in cardiac patientsCirculation2000102III263III26811082399
- LeveyASBoschJPLewisJBGreeneTRogersNRothDA more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study GroupAnn Intern Med199913046147010075613
- MaranhaoRCLeiteAJDevelopment of anti-atherosclerosis therapy based on the inflammatory and proliferative aspects of the diseaseCurr Pharm Des201521119620425312729
- SillesenHMuntendamPAdourianACarotid plaque burden as a measure of subclinical atherosclerosis: comparison with other tests for subclinical arterial disease in the High Risk Plaque BioImage studyJACC Cardiovasc Imaging2012568168922789936
- SillesenHFalkEWhy not screen for subclinical atherosclerosis?Lancet201137864564621440933
- ErbelRMohlenkampSMoebusSCoronary risk stratification, discrimination, and reclassification improvement based on quantification of subclinical coronary atherosclerosis: the Heinz Nixdorf Recall studyJ Am Coll Cardiol2010561397140620946997
- van der MeerIMBotsMLHofmanADelSAvan der KuipDAWittemanJCPredictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: the Rotterdam StudyCirculation20041091089109414993130
- VargaAGruberNForsterTAtherosclerosis of the descending aorta predicts cardiovascular events: a transesophageal echocardiography studyCardiovasc Ultrasound200422115500685
- FusterVBadimonLBadimonJJChesebroJHThe pathogenesis of coronary artery disease and the acute coronary syndromes (2)N Engl J Med19923263103181728735
- HuaNBaikFPhamTIdentification of high-risk plaques by MRI and fluorescence imaging in a rabbit model of atherothrombosisPLoS One201510e139833